National Guidance for Child Protection in Scotland 2021 - updated 2023
This guidance describes the responsibilities and expectations for all involved in protecting children and will support the care and protection of children.
Part of
Part 4: Specific Support Needs and Concerns
- Introduction
- Poverty
- When services find it hard to engage
- Disabled children
- Parents with learning disabilities
- Impact of mental health or health problems on children
- Children and young people experiencing mental health problems
- Suicide and self-harm
- Neglect and emotional abuse
- Domestic abuse
- Parental alcohol and drugs use
- Physical abuse, equal protection and restraint
- Severe obesity
- Child sexual abuse
- Child sexual exploitation
- Internet-enabled sexual offending
- Harmful sexual behaviour by children
- Online safety
- Online challenges and hoaxes
- Under-age sexual activity
- Bullying
- Hate crime
- Serious harmful behaviour by children
- Risk of terrorism
- Complex investigations
- Female genital mutilation
- Honour-based abuse and forced marriage
- Fabricated or induced illness
- Death of a child
- Community
- Cultural and faith communities
- Defence community
- Child protection in emergencies
- Non-recent abuse
- Child protection themes
Link to Appendix with References and Sources of Help for Specific Support Needs and Concerns
Introduction
4.1 Part 2B described common themes in multi-agency assessment. Part 3 defined steps in child protection. Part 4 covers specific areas of concern; and also factors that may intersect with these concerns and so may require specific attention and support. There are common threads connecting practice. The GIRFEC approach encourages consideration of the child's experience and perspective, within and beyond the family. The Promise encourages a focus on support for those relationships that are key to emotional safety and resilience. "When children talk about wanting to be safe, they talk about having relationships that are real, loving and consistent."
Poverty
4.2 Article 27.3 of the UNCRC requires public authorities to assist parents and others responsible for the child as necessary in providing the conditions necessary for the child's development. The Scottish Government has made tackling child poverty a national mission and is committed to working together with partners across the public, third and private sectors in order to tackle poverty and improve outcomes for families. Action to tackle child poverty is set out in Best Start, Bright Futures, the second Tackling Child Poverty Delivery Plan for the period 2022-26..
4.3 Most families experiencing poverty provide safe and loving homes and practitioners should be careful not to stigmatise families through highlighting the impact of poverty in families. However, poverty can cause as well as accelerate neglect and the risk of other harms. Consideration of the impact of poverty on children is a core consideration in child protection assessment and family support. Recent research indicates the disproportionate number of children placed apart from their families within the poorest neighbourhoods in Scotland. There is a growing interest in undertaking Social Needs Screening (also known as Poverty Screening) into the response of all disciplines who encounter children in need of support (Alderman, 2018; Bhavna Singichetti, 2019; Bywaters et al., 2017). The anti-poverty practice framework for social work in Northern Ireland and the British Association of Social Workers (BASW) anti-poverty practice guide for social work (2019) have been strongly influenced by this research.
4.4 Intersection. Poverty intersects with other stressors upon families, including disability, mental health problems, ill health, poor housing, barriers to employment, poor literacy skills, learning disabilities and racial discrimination. As noted in The Promise, "Poverty is a mediating factor among various factors that increase the risk of child abuse and neglect" (p17). Practitioners need to be alert to the corrosive impact of poverty upon the physical and mental wellbeing of parents, carers, children and young people. Community-level poverty can also limit the capacity for members of the community to provide informal social support. Poverty is frequently entrenched across generations and severely limits children's life chances and prospects. There are interactions between poverty and other challenges in dispersed Scottish rural and island communities that are of specific concern within social work (Turbett 2019). The emotional and economic isolation of rural victims of domestic abuse has been highlighted by English research (NRCN 2019). Poverty alone must never be a reason for removal of children from the care of their family.
4.5 Local authorities' safeguarding of children encompasses support for migrant families who have no recourse to public funds. These families face a high risk of poverty and destitution. Guidance on migrant rights and entitlements can be found at http://www.migrationscotland.org.uk/migrants-rights-entitlements/social-services%E2%80%99-support-introduction.
4.6 Analysis. Individual practitioners may have little influence on structural inequalities. However, in each situation, multi-agency planning to protect children should seek to maximise income and access appropriate resources for the family in order to address the distinctive context and relevance of deprivation. In this process, the My World Triangle prompts practical consideration of material barriers to wellbeing for each child. This should also prompt consideration of those instances when material affluence can mask emotional neglect and abuse (Bernard 2019).
4.7 Strategic direction. The Child Poverty (Scotland) Act 2017 sets out statutory targets to help tackle and reduce child poverty, which should be met in the financial year beginning 1 April 2030. Local authorities have duties under the Community Empowerment (Scotland) Act 2015, the Children and Young People (Scotland) Act 2014 and the broader social policy framework of the Scottish Government, to improve the health and wellbeing of children living in poverty. Actions to prevent and mitigate child poverty at the local level are likely to have both a direct and indirect impact on child wellbeing, safety and protection. The Scottish Government published the second Tackling Child Poverty Delivery Plan, Best Start, Bright Futures, in March 2022 setting out wide ranging and ambitious action to provide immediate support to families and to break the cycle of poverty in Scotland. Practitioners must be alert to the fact that economic pressures facing households to meet the cost of basic essentials, including food and energy can intensify the impacts of poverty. There is a need to ensure connection between local poverty analysis and planning with national strategy and policy (McKendrick, 2018). This includes, for example, ensuring that families access financial support available to them including the Scottish Child Payment, Best Start Grants and Best Start Foods delivered by Social Security Scotland. The Independent Care Review has stressed that: "There must be significant, on-going and persistent commitment to ending poverty and mitigating its impacts for Scotland's children, families and communities."
Resources and References - Poverty
When services find it hard to engage
4.8 Terms. 'Resistance' and 'disguised compliance', usually meaning disguised non-compliance or non-effective compliance, are terms sometimes used when services find it hard to engage with families. Such terms imply that the location of responsibility for this block lies with children and families.
4.9 'Non-engagement' covers a spectrum of failures that are all a product of interaction. The tone of engagement and painful previous experience of services may both play a part.
4.10 Inclusive protection and support of children also involves engaging with the risks and strengths presented by fathers and/or the men that are most significant to the child's safety and wellbeing. This component of protection and support is sometimes absent.
4.11 Non-engagement on the part of service users may take the form of aggression, manipulation, concealment, superficiality, blaming and 'splitting' professionals, inaction or selective action. Children who experience frequent changes of address within such a pattern may be at increased risk.
4.12 Effective child protection is a constant search for 'meeting points'. This is likely to depend on appreciation of the feelings and context of avoidant or oppositional communications. These might include fear, distrust, exhaustion, shock, isolation, intoxication, anxiety, depression, stigma, denial, blame, shame, deflection, trauma, attachment history, incapacity or confusion. Some will have had traumatic experience of being coerced and controlled. Others may already have had a child removed.
4.13 Developing a shared sense of purpose in relation to what needs to change for the safety of a child involves offering choices, respecting proven positives and anticipating difficulties together. Collaboration may also involve some degree of structured coercion, as far as necessary in each situation. This is not inconsistent with work 'in relationship', step by achievable step. Widening the circle should be considered - engaging others who can be partner in relation to the child's safety plan.
4.14 Development of a working alliance does not include condoning harmful behaviour or conditions. Deviation from a Child Protection Plan must be explored in detail and addressed in practical terms.
4.15 Co-operation is no assurance of readiness to change, of capacity to change, or of change in the child's experience. Co-operation can only be gauged by evidence of change in those behaviours defined as a necessary focus for the sake of the child's safety.
4.16 Failures in engagement are interactive - a shared responsibility. Persistent failure in engagement can contribute to significant harm as indicated in the triennial analysis of Significant Case Reviews (Care Inspectorate 2019). When children are subject to compulsory measures, the Principal Reporter must be informed if services cannot gain access. More urgent steps may be taken if necessary, especially if babies and other very young children are involved.
4.17 Effective co-operation can fail at any point, sometimes rapidly. Anticipation of and planning for predictable cycles of stress response is a necessary part of child protection planning. With most complex and interactive risks, progress is unlikely to be linear.
4.18 Encouraging hope promotes collaborative goal-setting. Unrealistic goal-setting without sufficient continuity of support will erode the potential to sustain safety. Motivational interviewing (Forrester et al 2012) may provide skills and concepts for approaching resistance, so long as a focus is kept on the child's welfare and safety. Honesty, transparency, curiosity and caution are steps on the road to effective alliance.
4.19 Solution-focused and strengths-based approaches may be optimal. This should be backed by careful recording, multi-agency assessment and chronology in order to gauge progress and guard against drift in planning.
4.20 Practitioners encounter hostility and aggression. Sometimes this can be anticipated in the location and planning of some meetings. Sometimes it is necessary to withdraw to minimise risk. In all such situations practitioners should be supported and supervised to ensure retention of focus on the child's safety needs, and to support the wellbeing and safety of staff.
Resources and References - When services find it hard to engage
Protection of disabled children
4.21 Disabled children are children first and foremost. Each child has unique potential. Their needs must be considered in the context of a holistic assessment of the child and the intersecting strengths and risks in their world. The term 'Disabled children' is used in this Guidance and in Scottish Government policy documents to reflect a social model of disability (p7. A Fairer Scotland for Disabled People). It is the right of individuals, families and groups to use terms which feel acceptable to them, such as 'children with disabilities'.
4.22 'Disabled children' is a broad term which may be applied to children with a broad range of physical, emotional, developmental, learning, communication and healthcare needs. The term is applicable when these needs have a substantial and long-term impact on a child's ability to engage fully in normal day-to-day activities. Some children (and some adults) are affected by disabilities and developmental delays that have never been assessed or diagnosed.
4.23 Most parents of disabled children provide safe and loving homes. Their expertise, commitment, willingness to work in partnership, motivation and hope are potentially strong protective factors.
4.24 However, children with communication impairments, behavioural disorders, learning disabilities and sensory impairments may be additionally vulnerable to abuse and neglect.
4.25 Disabled children have an equal right to be safe. Structures, processes and attitudes may open or close doors to safety. Effective protection requires extra preparation and consideration of the impact of any disability for a child within child protection processes.
4.26 The experience of each child must be central. Their voice and feelings must be heard when people make decisions that involve them. Some disabled children require specific assistance and communication support so that they can share their experience and participate. This must be provided. Some children have profound difficulties in communicating their experience and require special consideration to ensure attunement to their experience, and attention to ensure their wellbeing and safety. Principles of inclusive communication apply.
4.27 Rights and support: Disabled children and children affected by the disability of another family member are entitled to support as a child 'in need' as defined in section 93(4) of the Children (Scotland) Act 1995 for the purpose of meeting requirements under Part 2 of that Act to safeguard and promote their welfare etc. The Equality Act 2010, the UNCRC (Articles 2 and 23) and the United Nations Convention on the Rights of Persons with Disabilities help to reinforce and promote the rights of disabled children.
4.28 Protecting disabled children is a shared responsibility for all involved, requiring close collaboration between education and health as well as specialist practitioners, those leading child protection investigation, and parents or carers and advocacy services, as relevant in each situation.
4.29 Incidence of abuse of disabled children is likely to be under-reported. Some people may find it hard to believe that disabled children are at risk of abuse.
4.30 Invisibility of abuse is more likely when children are afraid, isolated or do not understand what is happening, and also when those around are not responsive to their distress. Distressed reactions do not necessarily relate to disability. Direct communication with children is essential when there are concerns. Supportive relationships with practitioners who know the child are protective.
4.31 Interacting factors: Risks which may be accentuated by some disabilities can combine with unrelated factors. Interacting factors may include:
- a child's dependency on support for communication, mobility, manual handling, intimate care, feeding and/or invasive health procedures
- a child's understanding of abusive behaviour and ability to resist
- availability of sex education and support for understanding
- a child's experience of asserting choice
- availability of a trusted person within or outside the family
- availability of advocacy and communication
- fear of abusers, of rejection or blame
- additional vulnerability to online abuse
- attachment history, including significant losses, disruptions and trauma
- neglectful or abusive responses to the child relating to parent or carer needs or cultural attitudes
4.32 Harm may be accentuated by many intersecting contextual factors, including the impact of poverty and housing insecurity; lack of support for parents who have learning disabilities or physical or mental health problems; domestic abuse; parental substance use; family isolation from positive community relationships or professional support; immigration status anxieties; insecurities in relation to leave to remain in the country, access to funds and housing; and abusive, coercive control within the family or care setting.
4.33 Barriers to effective protection can occur at any stage in support and child protection processes:
- when nobody listens to the child and those who know the child best
- if the child's communications and reactions are not understood
- when there is a lack of curiosity, competence and confidence in exploring reasons for distress or signs of maltreatment
- when there is a lack of practitioner awareness of the impact of neglect
- when there are delays or fragmentation in the assessment and sharing of information, or the co-ordination and planning of assessment and support
4.34 Some disabled children may behave harmfully to others. In some situations, a limited understanding (e.g. of boundaries) and reduced self-control may play a part in the interaction of reasons for this.
4.35 Training about the susceptibility of disabled children to abuse is essential in order to build confidence and awareness among those working with children. This includes staff such as bus drivers, care assistants, escorts and personal assistants.
4.36 All staff working with disabled children must have an awareness of child protection processes as described in Part 3 of this Guidance. They must understand and know how to respond when a child may be showing or telling about abuse. This entails a supportive approach which protects everyone closely involved - for example by considering siblings' needs and experience.
4.37 Some roles and tasks require provision of additional training, guidance and supervision. For example, practitioners involved in a child protection investigation will need additional guidance and training in relation to indicators of concern; consideration of a child's wishes, feelings, support and communication needs; and investigative interviewing, as appropriate. There is a need for guidance and training for practitioners working with people with learning disabilities in the field of sexual health and relationships.
4.38 Care assistants who are employed directly by parents and carers may have variable knowledge, skill and training. Access to clear local guidance on self-directed support and safe practice in contracting services is an essential component of preventative strategy that goes beyond the scope of Child Protection Guidance. Guidance on the Disclosure (Scotland) Act 2020, when implemented, will be of relevance.
4.39 Significant transitions require assessment and must be planned in good time, together with parents and carers, in accordance with applicable local procedures. These are phases of heightened and predictable vulnerability, as children move between services or life stages. Disabled children and young adults must be provided with appropriately adapted learning methods and resources so that they can help to keep themselves safe as they grow up. A practice insight on this topic has been drafted to illustrate and explain key practice considerations, offer a resource, prompt reflection and signpost selected sources. It can be found in the Practice Insights supporting document alongside this Guidance.
4.40 Child Protection Committees should be confident that there are local procedures which encompass disabled children. Local procedures should outline the interface of child and adult protection processes in local systems as indicated above. The Third Sector has a significant role with disabled children. Local procedures must describe how child protection concerns are progressed by statutory agencies in partnership.
4.41 Robust assessment and data recording processes support improvement in child protection assessment and planning. For example, when a child has a disability, the type and, if relevant, the severity of that disability should be recorded, along with the implications for the child's support and communication needs. A practice insight on this topic has been drafted to illustrate and explain key practice considerations, offer a resource, prompt reflection and signpost selected sources. It can be found in the Practice Insights supporting document alongside this Guidance.
Resources and References - Disabled children
Parents with learning disabilities
4.42 People with learning disabilities are all individuals with unique needs, strengths and potential. A learning disability affects a person's development, can be significant, and will be lifelong. This means that a person with a learning disability may need help to understand information, learn skills and live a fulfilling life. Some people with learning disabilities also have specific healthcare needs and require support to communicate. Some people and organisations prefer the broader term 'learning difficulties'. Societal attitudes, service structures and resources impact on the extent to which a learning disability becomes a barrier for people living a fulfilling life. A rights-based approach applies to support for parents with learning disabilities (UN Convention on the Rights of Persons with Disabilities).
4.43 Provisional national statistics indicate there are 23,446 adults with learning disabilities known to local authorities across Scotland. It has been estimated that there may be 5,000 parents in Scotland with learning disabilities. The Scottish Learning Disabilities Observatory is developing a national data picture.
4.44 An estimated 40-60% of parents with a learning disability do not live with their children. The children of parents with a learning disability are more likely than any other group of children to be removed from their parents' care. This is often due to the context of risk. For example, parents with a learning disability are often confused by services and disproportionately affected by poverty, social isolation, stress, mental health problems, low literacy and communication difficulties.
4.45 Contextual factors can interact with systemic factors including lack of:
- strategic leadership
- worker expertise and understanding
- inter-disciplinary co-operation
- sufficient, tailored and sustained support
4.46 Late recognition of risk and episodic child protection in crisis is neither fair nor effective. By contrast, effective child protection addresses need early and entails assessment, support and planning which:
- has a focus on the child's needs in connection with the needs of each parent and the strengths and gaps within the family network
- ensures that parents understand and are involved with what is happening, the reasons for meetings, accessible information, and involvement of advocacy as required
- includes targeted specialist assessment and co-ordinated, multi-disciplinary support plans
- looks ahead to long-term needs and different situations, including predictable life transitions
- is flexible, including a range of assessment methods and support services, some of which are 'at home' and can be adjusted to changing needs
- is step-by-step, applying appropriate assessment tools and support in order to grow parenting skills on an on-going basis. Some specific, pre-birth considerations are included in the section on pre-birth support
4.47 A practice insight on this topic has been drafted to illustrate and explain key practice considerations, offer a resource, prompt reflection and signpost selected sources. It can be found in the Practice Insights supporting document alongside this Guidance.
Resources and References - Parents with learning disabilities
Impact of mental health or health problems on children
4.48 Poor parental health (for both mothers and fathers, both mental and physical) can be a contributor to mental health problems in children and young people. The stigma associated with mental health problems means that many families are reluctant to access services because of a fear about what will happen next. Parents and carers may worry about being judged, and that they will be deemed incapable of caring for their children.
4.49 Parental use of alcohol and/or drugs can play a dynamic and reciprocal part in the causes and consequences of mental ill health. Early trauma and current domestic abuse can reinforce a cumulative cycle of harm in which individuals are known to child protection systems. Safety is likely to depend on persistent support for parents with complex interacting difficulties, especially if they disengage or disguise their own struggles when risks to children are rising.
4.50 Child protection assessment should consider the emotional accessibility and reliability of parents or carers. Child Protection Plans should aim to support these qualities.
4.51 Children are affected when a parent is unable to anticipate or prioritise his or her needs, and by a parent's distress, disturbance, delusions and lack of insight. Children may also be deeply affected when separated from a parent who is ill. In many instances the COVID-19 pandemic has magnified this stress and protective planning in these circumstances includes maintenance of connections for the child's wellbeing. Article 9 of the UNCRC outlines requirements of public authorities when a child is lawfully separated from parents, in their best interests. Article 9.3 requires public authorities to respect the right of the child who is separated from one or both parents to maintain personal relations and direct contact with both parents on a regular basis, except if it is contrary to the child's best interests.
4.52 Some children take on premature caring responsibilities due to parental illness. Child protection in this context requires compassionate recognition of parental experience in this dynamic, while remaining focused on the child's needs. Whenever safely possible, widening the circle of support and building on family strengths may be key to sustained protective planning.
4.53 Where adult mental health services, community learning disability services and specialist Third Sector supports are involved, children's safety must be considered in planning support for parents. Where information sharing is necessary, this is a two way process between adult and children's services.
4.54 The COVID-19 pandemic has accentuated the need for planned support for those families who are experiencing significant adversity, including infant developmental difficulties, parental substance misuse, domestic abuse and trauma (Scottish Government 2020). This support is crucial in the perinatal period - from conception to one year after a baby is born (Perinatal and infant mental health | NHS Education for Scotland).
4.55 Child protection processes often increase feelings of anxiety, stigma and isolation. The tone of engagement can accelerate or defuse risk of harm and self-harm. Recognition of the parent's experience is a starting point.
Resources and References - Mental health
Children and young people experiencing mental health problems
4.56 Children can experience a range of mental health problems, from depression and anxiety through to psychosis. While most will recover, many are left with unresolved difficulties or undiagnosed illnesses that can follow them into adult life. Parents and carers may be bewildered or frightened by their child's behaviour, or concerned that they are the cause of such behaviour. Child protection may be a component of the service response to children and young people experiencing mental health problems. Local training and policy should reflect the need for awareness of these issues.
4.57 Every child's needs and circumstances are unique to that individual and there tend not to be single causal connections. However, factors which make it more likely a child will experience mental health problems include:
- experience of neglect and abuse
- long-term physical illness
- insecurities in primary attachments
- domestic abuse
- problematic drug or alcohol use and offending
- bereavement and separation
- experiences of bullying, discrimination, isolation and exclusion
- living in poverty or being homeless
- premature and overwhelming caring responsibilities
- experience of long-term struggle in educational settings
4.58 A small number of children with mental health problems may pose risks to themselves and others. For some, their vulnerability, suggestibility and risk levels may be heightened as a result of their mental ill health. For others, a need to control, coupled with lack of insight into or regard for the feelings and needs of others, may lead to them preying on the vulnerabilities of other children. Co-ordinated inter-agency work, and close collaboration with parents or carers, is essential to mitigate risks for these children and for others.
4.59 Mental and emotional wellbeing should be addressed, applying the same principles of early intervention and prevention that underlie the GIRFEC approach to supporting a child's whole wellbeing. A range of services should be available locally to supplement specialist support that CAMHS can provide. This should include counselling services in schools, and community wellbeing service support for children, young people and their families. Lead professionals should be aware of the range of potential services in their areas and will work in collaboration with professionals in these services where required and appropriate.
4.60 Practitioners involved in child protection must be trauma-informed in their approach. Early recognition of and response to the impact of trauma is required, alongside a collaborative response between adult and children's services when a multi-agency plan is needed to protect a child from significant harm. The national trauma framework and training plan is relevant across professional sectors:
4.61 Transitions between placements; schools; child and adult services; stages of recovery and phases of relationship are all zones in which insecurities surface. They require anticipatory and follow-up planning if there is a child at risk of significant harm. Children who have been through criminal justice processes, are looked after, have learning disabilities, identify as LGBT and live in low-income households are all among groups that have a much greater probability of experiencing mental health problems (Audit Scotland 2018). For these reasons, child protection assessment and support planning should consider what we can do to recognise and respond with care to an apparent intersection of vulnerabilities.
4.62 Children who experience adversity and trauma are, in adulthood, more likely to become parents at a young age, experience poor mental health, use substances, have contact with the criminal justice system, and experience poor physical health. For some young people, mental health problems will severely limit their capacity to participate actively in everyday life, and will continue to affect them into adulthood. Some may go on to develop severe difficulties, including personality disorders, and display behaviour that challenges families and services (Mental Welfare Commission 2019).
4.63 Unaccompanied asylum-seeking children may be particularly vulnerable to mental health problems. They may have experienced traumatic events before arrival. Some will have been trafficked, and some will have on-going fears relating to this, in addition to insecurities about the future. Many will have no awareness of the support available to them, making it difficult for them to access services. Therefore any child protection planning should fit within a co-ordinated, relational and holistic approach, with access to independent advocacy as appropriate.
4.64 Third Sector and community support is critical. Recommendations made by the Children and Young People's Mental Health Taskforce (Scottish Government 2019) encapsulate a whole-system approach to addressing mental ill health.
Resources and References - Mental health
Suicide and self-harm affecting children
4.65 Suicide is an act of deliberate self-harm which results in death. Self-harm refers to self-poisoning or self-injury, irrespective of the apparent purpose of the act. Self-harm is generally a way of coping with overwhelming emotional distress. Many people self-harm where there is no suicidal intent. However, those who self-harm can be at a higher risk of suicide. Self-harm may combine with other expressions of distress and disturbance. If there are concerns that abuse or neglect are associated with self-harm, child protection processes apply.
4.66 Suicidal thoughts in children may be triggered by an event. However they are usually caused by an accumulation and interaction of vulnerabilities and experiences. This may include response to technology assisted information and communication. Suicidal thoughts and self-harming behaviour are more common among children who have been impacted by neglect, abuse, disrupted attachment, rejection, alienation, traumatic separation and loss. Children will also need support when they are impacted by the mental ill health, self-harm or suicide of others.
4.67 Parents, carers and peers may be the first to become aware of risk or distress. Frontline workers in health, education, social care, the police, the voluntary sector and the prison service need to be alert to circumstances where individuals may be at heightened risk, and should maintain awareness of what to do to support young adults. Every Life Matters is the Scottish Government Suicide Prevention Action Plan 2018.
4.68 A trauma-informed initial response can often significantly reduce risk and feelings of pain, isolation and despair. Depending on the immediate urgency of the situation and the capacity, mental and physical state of the person, in almost all instances it will be effective to take time to:
- take the threat of harm seriously and listen calmly
- recognise expressed feelings, showing warmth and empathy
- raise awareness that the person has some control, options and possibilities for a way forward, one step at a time
- ensure there is more than one person who can be responsive when emotional support is next urgently needed
4.69 In complex situations, preventative responses are likely to involve prompt multi-agency assessment. This may involve collaboration between children and adult services, and support for family or carers as well as for the child. Awareness of online risks and triggers may be critical for young people whose relationships and emotional fluctuations may be vectored through digital media.
Resources and References - Suicide and self-harm
Responding to neglect and emotional abuse
4.70 As noted in the definition in Part 1, neglect can arise in the context of systemic stressors, especially poverty. This does not imply that where there is poverty in a family there is neglect. On the contrary, when concerns are raised about neglect it is essential to ascertain the extent to which poverty is an underlying problem. Practitioners may need to consider the interaction of a range of structural stressors impacting upon parents, carers and children. Within the national practice model, the 'My Wider World' side of the My World Triangle prompts analysis of these factors Neglect covers a broad range of potentially co-existent physical and emotional maltreatment. This includes harm caused pre-birth for example due to parental alcohol and drug use or paternal violence. The causes and effects of neglect filter in to all the other sections in Part 4 of this Guidance.
4.71 Articles 9,19 and 39 of the UNCRC are of key relevance in relation to the duties of States Parties in relation to protection, prevention, support and recovery from neglect. The focus on preventative support in Statutory Guidance on Part 12 of the Children and Young People (Scotland) Act 2014 is relevant when children are at risk of becoming looked after. The Promise states: "Where children are safe in their families and feel loved they must stay - and families must be given support together to nurture that love and overcome the difficulties which get in the way."
4.72 Criminal offences currently termed 'cruelty' towards children under 16 years by persons with charge or care of, or parental responsibilities for that child are defined under section 12 of the Children and Young Persons (Scotland) Act 1937. These offences are currently subject to consultation and review. These offences include the wilful ill-treatment, neglect, abandonment or exposure to this, in a manner likely to cause unnecessary suffering or injury to health (including mental health).
4.73 Emotional abuse and neglect are the most commonly recorded concerns leading to the placing of children on the child protection register. Children may experience neglect and other forms of abuse at the same time. "Lack of parental care" was the most common ground for referral to the Scottish Children's Reporter Administration. (SCRA 2018). The average age for such referrals was 6 years. Practitioners will be aware of the urgency and need of a supportive response when very young children are involved. See also the section on pre-birth assessment and support below. Teenage neglect is less often recognised.
4.74 Single incidents of extreme neglect can be significantly harmful. However, neglect and emotional abuse are usually associated with the term 'persistent'. This refers to a pattern, which may be either continuous or intermittent, which has either caused or is likely to cause significant harm. For example, neglect may involve lack of physical care, including care for health and safety and including online and in the digital environment. It may also include unreliability or unavailability of emotional care, and lack of developmental care. It may further include neglect of educational, medical, dental care and nutritional needs (see section on obesity below). Unmet needs can impact on children's wellbeing regardless of the level of parent or carer intent. Comprehensive assessment of unmet needs and analysis of impact on wellbeing is essential, again guided by the My World Triangle.
4.75 Emotional abuse includes parental behaviour or exposure to adult behaviour that evokes fear, humiliation, distress, despair and a closing down of self-expression. This can cause immediate and long-term harm, because of the traumatic impact, the impact on development and how a child learns to feel about themselves, their relationships and the world. Extreme overprotection can also impair development. The effect of these harms are complicated when parents place all the responsibility for troubled or frozen behaviour on to the child.
4.76 Practitioners must be able to describe the interactions of concern. There must be a basis for the belief that these will be harmful. Descriptions in plain language are more useful than non-specific general terms like 'emotional abuse'.
4.77 A proportionate response to concerns requires an awareness of healthy development at each age and stage, and contrasting indicators associated with the need for support. For example, it is necessary to be curious about the reasons for:
- abnormally quiet and unresponsive infants with signs of developmental delay
- pre-school children who show abnormally frequent and persistent aggression and frustration; or who may be withdrawn, watchful and avoidant of parents or carers; or indiscriminate in their affections with strangers
- primary school age children who show an abnormally poor attention span, lacking an ability to be absorbed in play either alone or especially with others, who lack confidence and self-esteem and show unusual impulsivity and sharp mood swings, or an abnormal lack of concentration, confidence and/or social skills
- children in secondary school who show an abnormal lack of self-confidence, who lack trust in others, are self-isolating or have difficulty sustaining friendships, who steal, bully others, run away, or who show signs of eating disorders, self-harm or depression
4.78 Signs of concern may be physical, emotional, behavioural, educational or relational. Some concerns are visible. However, there are neglected children who are abnormally quiet and compliant and become invisible. The experience and impact of neglect is individual to that child, just as the intersection of causes is distinctive in each situation. Practitioners who are involved in assessment, planning and support must try to understand the quality of daily life experience and relationships of the child and their parents. That may take time.
4.79 Domestic abuse, parental alcohol and drug use, isolation, poverty, chronic or acute health problems and severe housing stress are common examples of factors that can contribute to conditions and interactions that cause harm. Some cultural groups may experience disproportionate deprivation. They are also more likely to experience confusion and disempowerment within statutory decision-making systems (Henderson, Kurlus, SCRA 2017). In all situations, respect for culture and recognition of the context of harmful interaction promotes the likelihood of effective engagement.
4.80 Affluence and achievement can also be isolating, and sometimes mask emotional neglect. It may take much longer to recognise what is absent. Developing a supportive working relationship with articulate, well-resourced and high-achieving families requires a confidence in role, skill, sensitivity and honesty, as well as keeping the child's experience as the central focus.
4.81 Persistent neglect can have a lifelong impact, and may be associated with the onset of physical and mental health problems, suicidal behaviour, eating disorders and obesity, alcohol and substance abuse, aggression, violence and criminal behaviour, high-risk sexual behaviour and homelessness. These are not inevitable consequences. Many parents who have experienced chronic neglect find ways forward and succeed in sustaining safe and loving care for their children. Some struggle to recall feelings associated with past trauma or deprivation.
4.82 The effects of neglect and emotional maltreatment may emerge in troubled or depressed teenage behaviour. Neglect may cause an increased vulnerability to exploitation, harmful and self-harming behaviour in teenage years. These patterns can contribute to neglect in the next generation. Young parents who have been neglected are more likely to need additional support to tune in to and build secure attachment with their own children. Parenting challenges tend to expose past hurts. Practitioners should seek to understand what lies behind neglectful behaviour and build on positive skills and relationships in order to increase safety and resilience through stressful times.
4.83 Protection of children from harm depends on early, inter-agency support in collaboration with parents, before the urgency of risk of significant harm draws children in to child protection systems. Uncertainties about definitions and thresholds can delay recognition and support.
4.84 Early signs of neglect must be taken seriously. Provision of early help can defuse the need for child protection processes. An inter-agency referral discussion becomes necessary when there is reason to believe the impact of neglect or emotional abuse could lead to significant harm.
4.85 The impact of neglect and/or emotional abuse upon a child will be affected by how early maltreatment occurred, the severity and type of maltreatment, the response of the child (which may include shame, anger and self-blame), the nature of relationships within which neglect occurred, and any steps taken to safeguard, protect or support the child during neglectful phases.
4.86 A comprehensive health assessment is recommended as part of a multi-agency assessment for all children where chronic neglect is a concern. Assessment and planning must be co-ordinated, collaborative and practical, addressing specific risks and the way risks interact. Plans should also be clear about the transfer of professional responsibilities at times of transition.
4.87 A structured framework for assessment of neglect is recommended in order to improve the quality and consistency of assessment. Practitioners who are confident about their use are more likely to promote purposeful, step-by-step working relationships with parents. The Graded Care Profile (GCP) (Srivastava 1997) has been adapted and used since 2009. Version 2 of this framework has been evaluated (NSPCC 2018) and adaptations are being tested in some parts of Scotland.
4.88 Strength-based approaches and a systematic, structured approach to assessment can be applied together. At all junctures in assessment, planning and support, the aim is to find a meeting point and shared understanding about what needs to change to keep the child safe and well, and how this will be achieved within a timescale that is right for the children involved. This clarity is essential in the context of compulsory measures. CPCScotland published Child Neglect in Scotland: Understanding Causes and Supporting Families' in October 2021. This is a framework setting out guiding principles for working with children and young people who may be experiencing neglect, and supporting local areas to ensure that local Integrated Children's Service and Child Protection Committee plans incorporate appropriate actions to prevent, reduce and manage the impact of neglect on children and families.
4.89 The concept of capacity to change may promote transparency of goals, methods, shared responsibilities and timescales. Advocacy and Third Sector supports may play a key part in motivational support and work for change.
4.90 When children have experienced chronic neglect, they may not be used to adults being or becoming predictable, kind and nurturing. They can be distrustful and anxious, and may behave in ways that seem rejecting or angry. This is demanding for parents or carers seeking to offer a secure base and a safe home. To prevent secondary harmful cycles occurring when children are accommodated, carers and children may need additional support in understanding and response to these dynamics.
4.91 When children have had to be removed from parental care in cases of neglect, effective child protection leads into careful assessment of reunification and transitional support needs. For example, NSPCC resources designed for use within English legislation offer guidance (NSPCC 2015). (Reunification: An evidence-informed framework for return home practice.) Progress is rarely linear and final. Any good plan should include sufficient continuity of, or access to support for predictable and unpredictable crises.
4.92 A practice insight on this topic has been drafted to illustrate and explain key practice considerations, offer a resource, prompt reflection and signpost selected sources. It can be found in the Practice Insights supporting document alongside this Guidance.
Resources and References - Neglect and emotional abuse
Domestic abuse
4.93 This section has a focus on child protection response. Further detail is provided in appended links to practice insights.
4.94 Definition. Domestic abuse is any form of physical, verbal, sexual, psychological or financial abuse which might amount to criminal conduct and which takes place within the context of a relationship. The relationship may be between partners (married, cohabiting, in a civil partnership or otherwise), or ex-partners. The abuse may be committed in the
4.95 home or elsewhere, including online. Domestic abuse includes degrading, threatening and humiliating behaviour predominantly by men and predominantly towards women. It is a gendered crime and is underpinned by attitudes and inequalities between men and women that continue to be prevalent in society. It may be committed in the home or elsewhere; and may include online activity. There is significant evidence of links between domestic abuse and emotional, physical and sexual abuse of children, and children themselves can experience domestic abuse as 'coercive control' of the whole family environment, not just of their mother.
4.96 Prevalence. There were 60,641 domestic abuse incidents known to Police Scotland in 2018-19. This was a 2% rise from 2017-18. In 2018-19, 2,673 children were referred to the Reporter under section 67(1)(f) of the Children's Hearings (Scotland) Act 2011, due to a "close connection with a person who has carried out domestic abuse" (SCRA 2019). This does not include children referred on other grounds who may also have experienced domestic abuse. For the estimated 2,668 children on the child protection register at 31 July 2018, there were 6,830 concerns relating to domestic abuse at the case conferences at which they were registered.
4.97 Violence against women and girls refers to a range of actions that harm, or cause suffering and indignity to, women and children. These include but are not limited to physical, sexual and psychological violence in the family, general community or in institutions. This includes domestic abuse, rape, incest and child sexual abuse; sexual harassment and intimidation at work, online, at home or in public; commercial sexual exploitation including prostitution, pornography and trafficking; and so called 'honour-based' violence, including dowry-related violence, female genital mutilation, forced and child marriages, and 'honour' crimes. The Scottish Government's definition of violence against women and girls is based on the United Nations Declaration on the Elimination of Violence Against Women (Equally Safe: national strategy). Article 19 of the UNCRC requires public authorities to take all appropriate measures in relation to protection of children from all forms physical and mental violence, injury or abuse etc.
4.98 Offence. The criminal offence of Domestic Abuse is detailed in sections 1 and 2 of the Domestic Abuse (Scotland) Act 2018. Offences cover behaviour likely to cause a partner or ex-partner to suffer physical or psychological harm (including fear, alarm and distress). This can range from behaviour that is violent, threatening or intimidating or has effects such as dependency, isolation from friends or family, controlling, depriving or restricting freedom of action or which is frightening, humiliating, degrading or punishing.
4.99 Statutory aggravation of the offence in relation to a child is provided for at section 5 of the 2018 Act. This includes where a child sees, hears, or is present during or is likely to be adversely affected by the offence of domestic abuse. There does not have to be evidence that the child is aware, understands or has been adversely affected by the domestic abuse and a single source of evidence is sufficient for the offence to be aggravated.
4.100 Emotional and psychological harm. Children are harmed by experiencing behaviour that is, intimidating and degrading, threatening, exposing of intimate information, or accusing and blaming. Coercive and controlling behaviour is also harmful. Examples of coercive and controlling behaviour include when the child and non-abusive parent are isolated from friends and family, or when abusers cut off the non-abusive parent's access to a phone or a bank account. Chronic trauma can disrupt attachment, achievement, concentration and wider relationships. The traumatic impact of domestic abuse is often masked, and emerges indirectly in anxious or troubled behaviours in teenage years. As highlighted throughout this Guidance, a trauma-informed approach is required by all involved practitioners (NES 2019).
4.101 Abuse between young people. Young people may experience abuse and coercive control in their own relationships outside of the family home. As within adult domestic abuse, this can include physical, sexual and emotional abuse. This is often unrecognised, and victims may choose not to disclose it. Social media and digital technology may be used to perpetrate the abuse.
4.102 Response. Members of the public or non-statutory services concerned for the safety of a child or parent should contact Police Scotland or social work. As far as possible, taking into account the urgency of the situation, this should be in collaboration with the non-abusing parent/carer. On all occasions when children are present during an incident that requires the police to attend, officers in attendance will consider all information, including previous incidents, to assess whether there is a child wellbeing or protection concern. Information about the incident will be considered for sharing by Divisional Concern Hubs with appropriate statutory and non-statutory agencies who have support, wellbeing or health responsibilities, or who provide domestic abuse advocacy services (COPFS 2019).
4.103 The Domestic Abuse (Protection) (Scotland) Act 2021, once implemented, will introduce a power for Police Scotland and the courts to issue Domestic Abuse Protection Notices and Orders as short-term, emergency protection for persons experiencing domestic abuse.
4.104 The child protection response by statutory agencies will depend on professional judgement about the risk of harm and the urgency of the circumstances. Domestic abuse is always a wellbeing concern. It may be a child protection concern if there is evidence that significant harm has occurred or may occur. Professional judgement involves consideration of key factors such as the child's experience, needs and voice (and those of other children affected); the non-abusing parent's views, choices, strengths and abilities to use available supports; the presence of other complicating factors such as parental alcohol and drug use; and the abuser's pattern of coercive control.
4.105 Only where professional judgement indicates the likelihood of risk of significant harm will an IRD be triggered as outlined in Part 3 of this Guidance.
4.106 In some cases the risk from the perpetrator is very high. Multi-agency planning and partnership with the non-abusive parent must protect the child. It can be difficult to achieve safe collaboration with a non-abusing parent/carer if they deny, or do not recognise, the risk posed by the perpetrator towards the child.
4.107 GP and hospital services must be alert to the needs of victims of abuse, and especially those who are pregnant and have mental health, drug and alcohol difficulties. Domestic abuse may begin during pregnancy.
4.108 Third Sector organisations, such as Scottish Women's Aid, play an essential role in developing and providing services for women and children. A National Domestic Abuse and Forced Marriage Helpline is open 24/7, 365 days a year. This is available for professionals seeking advice, as well as for individuals who are at risk of or experiencing domestic abuse.
4.109 Disclosure Scheme for Domestic Abuse Scotland (DSDAS) aims to provide a way of sharing information about a partner's abusive past with a potential victim. It gives people at risk of domestic abuse the information needed to make an informed decision on whether to continue the relationship. Disclosures are only made where it is lawful, proportionate and necessary to do so.
4.110 Sex Offender Community Disclosure Scheme (Keeping Children Safe) was introduced across Scotland in 2011 and is managed by Police Scotland. The scheme enables parents, carers, guardians, or any other person who is concerned about a person's access to a child to apply, albeit only the parent, carer or guardian can be given information under the Scheme (Information on how to submit an application for the Sex Offender Community Disclosure Scheme. - Police Scotland).
4.111 In cases where Police Scotland believes that an individual poses a risk to the child concerned, discussions will also take place with partner agencies, and steps agreed and progressed to ensure the child's safety.
4.112 Police Scotland provides governance and co-ordination for the scheme to ensure it is publicised widely and embedded in national police training.
4.113 Multi-Agency Risk Assessment Conferences (MARAC) are local meetings where representatives from statutory and non-statutory agencies meet to discuss individuals at high risk of serious harm or murder as a result of domestic abuse. A referral to a MARAC should be considered at the point this risk is identified. MARACs can play a vital role in terms of safety planning for victims of domestic abuse and their children. Safelives, a UK-wide domestic abuse charity, has developed a suite of resources to help ensure that each MARAC keeps as many victims of domestic abuse as possible safe (Home | Safelives).
4.113 Multi-Agency Tasking and Co-Ordination (MATAC) is a Police Scotland-led and chaired initiative to identify and manage the most harmful domestic abuse perpetrators. MATAC aims to effectively tackle offending by domestic abuse perpetrators who present the greatest risk of harm. It does this through:
- effective partnership working to identify those domestic abuse perpetrators who present the greatest risk of harm
- multi-agency information sharing to support intelligence development and proactive enforcement action against identified perpetrators
- using tasking and co-ordination to proactively investigate identified perpetrators, using relevant and legitimate tactics
4.114 Where MARAC or MATAC processes identify children at risk, consideration should be given to referring the children for IRD. Where a risk or a potential risk of significant harm to children is identified during a MARAC or MATAC conference then an IRD should be held without delay.
Systematic responses
Safe and Together
4.115 The Safe and Together Model is based on partnering with domestic abuse survivors and intervening with domestic abuse perpetrators in order to ensure the safety and wellbeing of children. The Safe and Together approach includes principles and elements essential to safe practice. These are to:
- keep the child safe with the non-abusive parent
- form a supportive partnership with the non-abusive parent
- hold the abusive parent accountable for their abuse
4.116 Within this approach, practitioners from statutory and non-statutory agencies work collaboratively and reach consensus to ensure the safety and wellbeing of children living with domestic abuse (Humphreys, Healey and Mandel 2018). Practitioners will:
- locate responsibility for the abuse with the perpetrator and recognise their abuse is a parenting choice
- get as much information about fathering and father's parenting choices as about mothering and find out about the pattern of abuse and how this affects choices available to the non-abusing parent
- explore the perpetrator's pattern of coercive control to identify all forms of abuse and control in both current and previous relationships, rather than outlining singular incidents of physical violence
- assess how abuse has harmed the child, including descriptions of direct physical, emotional and sexual abuse from the perpetrator to the child, as well as the way in which the domestic abuse has harmed them
- assess wider wellbeing impact upon the child
- define how the non-abusing parent has promoted the safety, wellbeing, stability and nurture of their children
- assess the interaction of other factors like substance abuse, mental health, culture, and how other socio-economic factors are considered and addressed
4.117 The Caledonian System is implemented in many Scottish local authorities (2019). This is an integrated approach to address men's domestic abuse and to improve the lives of women, children and men. It does this by working with men convicted of domestic abuse-related offences on a programme to reduce their re-offending while offering integrated services to women and children. The Men's Service uses a challenging but trauma-sensitive approach with cognitive behavioural techniques to encourage men to recognise their abuse and take responsibility for themselves and their relationship with their ex/partners and children. The Women's and Children's Services support women and children and advocate for their rights. Men will be referred to the programme if they have been convicted of offences involving domestic abuse.
Learning from lived experience: bridges to safety
4.118 The following features of practice have been associated with safer practice by those consulted in review of this Guidance.
- finding a safe way to talk to non-abusing parent in private (away from perpetrator)
- ensuring children's experience and views are given due weight in decision-making, especially about contact
- recognising positive steps to protect the child
- responding early within universal services, including early referral to specialist domestic abuse services
- applying training, experience and supervision that generates an informed understanding of the dynamics of domestic abuse
- supporting the non-abusing parent, which in turn supports the child
- understanding when a non-abusing parent's ability to effectively parent has been compromised by the perpetrator's abuse, and providing support accordingly
- recognising and integrating protective factors in safety planning
- supporting children in finding an advocate who they trust
- being clear about confidentiality, and explaining to children and women what information will and will not be shared about them, why and with whom
- being aware of the consequences of sharing information with perpetrators, and taking heed of women's and children's fear of reprisal from a perpetrator, especially following separation
4.119 Child abduction in the context of domestic abuse. Section 6 of the Child Abduction Act 1984 creates a criminal offence in Scotland for a person connected with a child under 16 to take or send the child out of the UK without appropriate consent where there is a UK court order in place awarding custody of the child to any person or which makes the child a ward of court or where there is a UK court order in place prohibiting the child's removal.
4.120 Where no such court order is in place, the parent or person with rights of custody can use civil law under the 1980 Hague Convention on the Civil Aspects of International Child Abduction to seek return of the child, or access rights. Where the country to which the child has been abducted is not a party to the Hague Convention, advice should be sought from the Foreign and Commonwealth Office (FCO).
4.121 A practice insight on this topic has been drafted to illustrate and explain key practice considerations, offer a resource, prompt reflection and signpost selected sources. It can be found in the Practice Insights supporting document alongside this Guidance.
Resources and References - Domestic abuse
Children and families affected by alcohol and drug use
Guidance on neglect, domestic abuse and pre-birth child protection are adjacent in this section and closely inter-related.
4.122 Public, child and family health. Parental alcohol and drug use is a significant public health problem present in all income groups, cultures and areas of Scotland. Directly and indirectly, it contributes to the abuse and neglect of thousands of children and can cause harm through various forms of loss, through imprisonment, illness, disturbed and broken relationships and death. Parental alcohol and drug use overlaps and intersects with domestic abuse, neglect, emotional abuse and parental mental ill health as dominant reasons for child protection registration and the need for children to be looked after. There is a strong link between problem drug and alcohol use, deprivation, and trauma. In this context compassion, understanding and workforce resilience are essential within effective child protection.
4.123 Prevalence. The availability, relative cheapness and social acceptability of alcohol make it the substance with most widespread impact. Alcohol-related deaths are twice as high in Scotland as the rest of the UK. Over the last ten years, drug-related deaths have risen in Scotland and are the highest in Europe. Opioids are implicated in most drug-related deaths. The Psychoactive Substances Act 2016 creates a blanket ban on the production, distribution, sale and supply of psychoactive substances in the UK (which is underpinned by criminal offences and civil sanctions). However, novel psychoactive substances are still a growing cause of harm. NHS Scotland estimates 55,800 to 58,900 individuals had substance use problems in 2015-16. Of these, 71% were male, concentrated in the 15-24 age bracket. Drug problems in people aged over 35 is now a growing issue.
4.124 Significant harm is not an inevitable consequence of parental alcohol and drug use. The probability of significant harm will relate to the extent to which each child's needs (as considered within the context of the My World Triangle) are met, blocked or disrupted by the causes, cycle, circumstances and consequences of seeking, paying for, using and experiencing substances by the parent(s). The significance and urgency of the impact will depend on factors to do with the drug, the pattern, the parents, the child, and the multi-dimensional impact upon safety, health, nurture and, by chronic interaction, to all aspects of wellbeing. Every drug-related concern about a child has a distinct context, history and degree of urgency.
4.125 Harm may be multi-dimensional, affecting physical and mental health and development, relationships, behaviour, identity and survival. The effects of parental alcohol or drug use on a developing foetus depends on the substance, when it is taken during pregnancy and the pattern of use. Foetal Alcohol Spectrum Disorder (FASD) is the leading known worldwide preventable cause of neurodevelopmental disorder, with maternal use of alcohol during pregnancy leading to learning and behavioural difficulties. Neonatal abstinence syndrome (NAS) is defined by clinical signs of withdrawal from heroin and other opiates, cocaine and benzodiazepines. Children with NAS sometimes require drug treatment for withdrawal and hospitalisation. If parental substance use takes priority over the needs of the child, parents risk being inconsistent or emotionally unavailable, leading to insecure attachment, and learning and cognitive delays in the child which can have lifelong impact. Where child protection concerns in pregnancy include the use of alcohol or drugs, this must form a focus for multi-agency support.
4.126 It is essential to consider and take steps to safeguard children from harm caused by access to substances in the home.
4.127 Children affected by parental alcohol and drug use may experience neglect, feelings of fear, blame, abandonment, anger and shame. Children who may not be recognised as Young Carers may have to care for children, or for adults. Secrecy and denial are recurrent features within families affected by alcohol and drug use. Divisions occur within families where there is pressure to contain knowledge of substance use. Children's potential to experience and develop trusting, secure relationships are compromised. Many parents feel marginalised outside the home, and inside the home they do not know how to acknowledge or discuss their substance issues with their children. Stigma accompanying parental alcohol and drug use affects children, locks in secrecy and remains a barrier to connection with universal services, treatment and support.
4.128 Child protection approach. Although specialist assessment and support may be required, key elements of the general approach to assessment, and of the steps indicated in parts 2b and 3 of this Guidance, apply.
4.129 Parents value clear, consistent and honest messages about their progress when delivered in the context of trusted relationships and intensive support. Parents need holistic help that takes into account damaging early-life experiences (Dawe et al (2018). Parenting and fatherhood-focused interventions should be considered within substance abuse treatment programmes, unless there are compelling (e.g. child safety) reasons not to do so. Child protection planning should not be exclusively reliant on maternal change and responsibility. Aims, methods, steps, choices, expectations and lines of communication should be crystal clear to all involved, especially parents and children. Components will be tailored to needs and resources. 'Parents Under Pressure' is an example of an intensive, modular, community-based programme which has been subject to robust evaluation (Barlow et al 2018).
4.130 Capacity to change and decision-making. It may be very difficult to predict parenting capacity with confidence. When assessment relates to the risk of significant harm, the assessment should include an evaluation of capacity to change within a timescale that will meet the child's needs. A combination of practices may be required to support safe decision-making and to offset the risk of selective attention to information confirming previous judgements. This combination may include the use of approved, structured risk assessment tools, careful assessment of family functioning, and involvement of families in shared decision-making around the nature and focus of Child Protection Plans.
4.131 Professional judgement about the likelihood of significant harm involves multi-agency consideration of the interaction, accumulation, immediacy and likely continuity of risks and strengths in each situation. Parental needs may obscure the child's needs. Drug use may bring on mental health disorders in a reciprocal and cyclical manner. Mental disorders can also lead to drug use, possibly as a means of 'self-medication'. Parents experiencing anxiety or depression may rely on alcohol, tobacco, and other drugs to temporarily alleviate their symptoms. Both drug use disorders and other mental illnesses are influenced by overlapping factors such as genetic vulnerabilities, early trauma, or the current experience of domestic abuse.
4.132 Connected child protection. Follow-up support is required for parents who have involuntarily lost their children through child protection and permanence processes, in order to anticipate and prevent a repeat cycle of risk, separation and loss.
4.133 Policy, strategy and local process. The Scottish Government aims to make stronger links with housing, education and justice to focus recovery from parental alcohol and drug use and support beyond health. The national approaches to alcohol and drug harms are outlined in Rights, Respect and Recovery (Scottish Government 2018) and the Alcohol Framework (Scottish Government 2018). Article 33 of the UNCRC addresses the wider impact on children of harmful drug use, requiring public authorities to take all appropriate measures, including legislative, administrative, social and educational measures, to protect children from the illicit use of narcotic drugs and psychotropic substances as defined in the relevant international treaties, and to prevent the use of children in the illicit production and trafficking of such substances. The section below on Child Criminal Exploitation is also relevant.
4.134 The Framework to Reduce the Use of and Harm from Alcohol and Drugs (Scottish Government/COSLA 2019) describes the roles of Alcohol and Drug Partnerships and governance within integration authorities. Audit Scotland (2019) has reported on the efficacy of current approaches. Child Protection Committees, Adult Protection Committees and Chief Officers must work together to ensure local procedures, services and assessment frameworks are in place, that transitional protocols are in place for vulnerable young adults, and that there are evaluative mechanisms to ensure an understanding of how well services are working locally in relation to child protection response in this context.
4.135 Substances, policy and law. While non-specialists should not be expected to know or judge compound details, a broad sense of the landscape may be helpful. Introductory training tools and graphics may be accessed at (Adley/UK Drugwatch 2017). A recent Scottish Parliament research briefing summarises legislation and policy (Davies 2017).
Resources and References - Parental alcohol and drug use
Physical abuse, equal protection, and restraint
4.136 Article 19 of the UNCRC requires public authorities to take all appropriate legislative, administrative, social and educational measures to protect children from all forms of physical or mental violence, injury or abuse.
4.137 Physical abuse is the causing of physical harm to a child or young person. Although there is a distinction between inflicted and non-inflicted physical harm, some accidents may be attributed to neglect and lack of supervision. This might include exposing a child to parental alcohol and drug use or domestic abuse, which may constitute an "aggravation by reason of involving a child" under section 5 of the Domestic Abuse (Scotland) Act 2018, for the purpose of the domestic abuse offence in section 1(1) of that Act.
4.138 In addition to the common law of assault, section 12 of the Children and Young Persons (Scotland) Act 1937 contains provisions dealing with the treatment of children and young people by persons of 16 years or over who have parental responsibilities in relation to them or who have charge or care of them. That section makes it an offence for such persons to treat that child with cruelty (described as wilful assault, ill-treatment, neglect, abandoning, exposing, or causing or procuring such treatment in a way which is likely to cause unnecessary suffering or injury to health).
4.139 Professional guidelines and evidence reviews are available about assessment of suspected physical maltreatment, including, for example: suspicious bruising; human bite marks; burns and scalds; fractures; inter-cranial injuries; abusive head injuries and facial or mouth injury.
4.140 Concerns are heightened if there is no explanation for the injuries, explanations shift during assessment, explanations do not fit the injuries, or there are unreasonable delays in seeking treatment. In relation to fractures, no one fracture in isolation is specific for physical abuse. The younger the child, the greater the likelihood of that a fracture is related to abuse. The majority of abused children with fractures are less than 18 months old, whereas most accidental fractures occur in children over five years. Bruising is the most common presenting feature of physical abuse in children. Accidental bruising increases with increased mobility. The presence of bruising in infants who are not independently mobile, including those who are not yet crawling or walking independently, requires thorough investigation, as it is extremely rare for a non-mobile infant to sustain accidental bruising.
4.141 In some instances, despite medical examination, there will be continuing uncertainty about explanations for injuries.
4.142 The need for and nature of any immediate action will relate to considerations including:
- the child's presentation and apparent fears
- significance of the injuries
- attitude of responsible adults to the injuries
- likelihood of contact with a person who may have caused the injuries
- contextual information including previous recorded concerns
- availability of a safe and responsive parent or carer
Equal protection
4.143 The Children (Equal Protection from Assault) (Scotland) Act 2019 ('the 2019 Act') removed the previous common law defence of 'reasonable chastisement'. If a parent or carer physically punishes their child they can be prosecuted for assault. (Section 16 of the Standards in Scotland's Schools etc. Act 2000 effectively ended the use of corporal punishment in schools.) There is a growing body of international evidence showing that physical punishment of children can lead to long-term negative outcomes.
4.144 Physical punishment or physical discipline can take many forms, including (but not limited to) smacking, skelping, spanking and slapping. It is not an offence to restrain a child to protect him/her, or others, from harm. However, as indicated below, restraint can be used in a way that is harmful.
4.145 Awareness and support. Under section 2 of the 2019 Act, the Scottish Ministers must take appropriate steps to promote public awareness and understanding about the effect of the Act. Public facing material has been placed on-line: see, for example, Parent Club. Both statutory and Third Sector agencies have a crucial and collaborative role in raising awareness of the reasons for and consequences of the law; and in promoting access to assistance for parents and carers who need support in managing children's behaviour and accessing wider sources of support, for example, via the Family Support Directory (or local equivalent); and through helplines such as Children 1st Parentline.
4.146 Police Scotland. The Lord Advocate has issued guidelines to the Chief Constable of Police Scotland on the investigation and reporting of allegations of assaults by parents or carers on children. Those guidelines and prosecutorial policy support a proportionate response to allegations of assaults on children by parents and carers. When appropriate, that response may include the use of recorded police warnings, diversion and other alternatives from prosecution.
4.147 Reporting concerns. Anyone who sees a person physically punishing/assaulting their child can:
- call the police on 101
- contact local authority social work
- call Crimestoppers on 0800 555 111 (anonymously) who will report to police
- as has always been the case, call 999 if a child or young person is in immediate danger
Prompts in paragraphs 3.1-3.6 may be useful for persons calling social work or police.
4.148 Child protection. Statutory agencies will progress an inter-agency referral discussion if there are concerns about significant harm or the risk of significant harm to a child. Part 3 of this Guidance outlines relevant considerations and steps in child protection processes. Part 2B outlines principles in multi-agency assessment.
4.149 Assessment and support. When concerns fall short of the significant harm threshold, this must not stop the provision of proportionate co-ordinated support. General guidance and advice (such as hints and tips on coping with being a parent and Ready Steady Baby) are valuable preventative resources. However concerns relating to physical punishment of a child require assessment and proportionate response. This may include targeted and/or intensive support. All responses must be carefully recorded. Practitioners should be alert to any pattern of concern and the wider context of this incident.
4.150 Cultural competence. There may be some variation in personal, family, community or cultural attitudes to parenting, for example in relation to reasonable discipline. Sensitivity is essential alongside practitioners' central focus on a child's needs for protection from harm; and the needs of a family for support to reduce stress and associated risk.
4.151 A practice insight on this topic has been drafted to illustrate and explain key practice considerations, offer a resource, prompt reflection and signpost selected sources. It can be found in the Practice Insights supporting document alongside this Guidance.
4.152 Referral to the Reporter. Where there is an apparent need for compulsory measures, consideration should be given to referral to the Reporter.
Restraint
4.153 'Restraint' may be defined as an act carried outwith the purpose of restricting an individual's movement, liberty and/or freedom to act independently. This may or may not involve the use of force. Restraint is to be distinguished from punishment in that it is for the purposes of protection, not discipline. Restraint does not require the use of physical force, or resistance by the person being restrained, and may include indirect acts of interference, for example removing someone's walking frame to prevent them moving around (Equalities and Human Rights Commission 2019).
4.154 Restraint usually involves a parent, carer or professional making physical contact with a child, although there may be examples of indirect restraint for people with disabilities or young children which prevent access or egress. Restraint, if used inappropriately, excessively or harmfully, could result in a charge of assault being brought.
4.155 Use of restraint carries risks and can be extremely damaging to children and young people. It may, however, be the only realistic response in some situations and as a last resort (for example, to prevent a child running into a busy road or to prevent a violent act against another person). Adults should do everything they can to understand the child before using restraint, especially if the child is upset or frightened. Restraint should never hurt a child, and it should only ever happen for the shortest time possible. Restraint should never be used as punishment, or as a way to make someone 'behave'.
4.156 Additional vulnerabilities. Children with communication difficulties, learning disabilities, autistic spectrum conditions and mental health difficulties are especially vulnerable to inappropriate use of restraint in education, health and social care settings. Wherever possible use of restraint should be avoided. Agency protocols must support proactive, preventative, non-restrictive responses to distressed and challenging behaviour. This begins with forming an understanding of the needs behind the behaviours, and forming strategies with each individual child to protect their safety and rights, and those of others involved.
4.157 The Health and Social Care Standards (2017). Children receiving services through the NHS, as well as services registered with the Care Inspectorate and Healthcare Improvement Scotland, should be able to expect that while they will be kept safe and protected from avoidable harm, any intervention that he/she experiences is safe and effective. This requires appropriate staff training and development, supervision and support.
4.158 Recording. Any use of restraint and/or seclusion (variously defined in Scotland but by which is meant shutting a child somewhere alone and not allowing them to leave), should also be recorded as one critical way of ensuring that practice is rights-compliant and appropriately monitored and scrutinised.
4.159 The physical and psychological impact of restraint must be considered. Physical restraint provokes strong feelings and children may be left physically or emotionally hurt. Even if a child has not directly experienced restraint, they may be scared that it will happen in future or have been upset by seeing others restrained.
4.160 To avoid a breach of a child's rights, any use of restraint must be lawful, necessary and proportionate. The key question for everyone involved with children and young people who express distressed behaviour should be: "What is in the best interests of the child and/or those around them in view of the risks presented?"
Resources and References - Physical abuse, equal protection and restraint
When obesity is a cause for escalating concerns about risk of harm
4.161 Severe obesity is not an automatic flag for child protection concerns. However NHS Scotland Standards (2019) have been developed in recognition of the complexity of the condition and in view of some situations in which significant harm or death may result from neglectful circumstances. Article 19 of the UNCRC requires public authorities to take all appropriate measures to protect and support children while in the care of parents and others, from a broad spectrum of harm including negligent treatment.
4.162 A child's health condition and sustained recovery is likely to be influenced by a complex interaction of factors such as physical, emotional and cognitive abilities, environmental, familial and social issues. Professional curiosity is necessary and practitioners should be alert to the possibility of neglect and need for support due to an interaction of such factors.
4.163 If efforts by health services to provide information, guidance and support have been unsuccessful due to avoidance, hostility, denial, inability or unwillingness to follow essential clinical advice to prevent harm, these would be strong indications of the need to escalate concern. It will be essential to understand and address the barriers to teamwork around the child's or young person's needs, without delay.
Resources and References - Obesity
Child sexual abuse
4.164 Definition. Child sexual abuse (CSA) is an act that involves a child in any activity for the sexual gratification of another person. Sexual abuse involves forcing or enticing a child to take part in sexual activities, whether or not the child is aware of what is happening. A child under age 16 cannot consent to sexual activity at all, so it cannot be claimed that the child consented or assented to such activity. Generally, the position for children aged 16/17 will depend on whether there is consent or a reasonable belief of consent. Some sexual offences, such as sexual abuse of trust (section 42 of the Sexual Offences (Scotland) Act 2009) apply up to age 18 irrespective of consent. The offences of taking or possession of indecent photographs of children (sections 52 and 52A of the Civic Government (Scotland) Act 1982) apply up to age 18, with certain defences related to those in established relationships where the child is reasonably believed to be 16 or over.
4.165 Sexual abuse may involve physical contact, including penetrative or non-penetrative acts. They may include non-contact activities, such as involving children in looking at, or in the production of, indecent images, or in watching sexual activities, using sexual language towards a child, or encouraging children to behave in sexually inappropriate ways. Children who experience sexual abuse may experience multiple forms of abuse and neglect within and beyond the family.
4.166 For those who may be victims of sexual offences aged 16-17 and who are at risk of significant harm, child protection procedures should be considered, and must be applied when there is concern about sexual exploitation or trafficking.
4.167 Article 19 of the UNCRC sets out requirements on public authorities to take appropriate protective measures. These include appropriate legislative, administrative, social and educational measures to protect the child from sexual abuse; support for the child and for those who have the care of the child; as well as forms of prevention, identification, reporting, referral, investigation, treatment and follow-up.
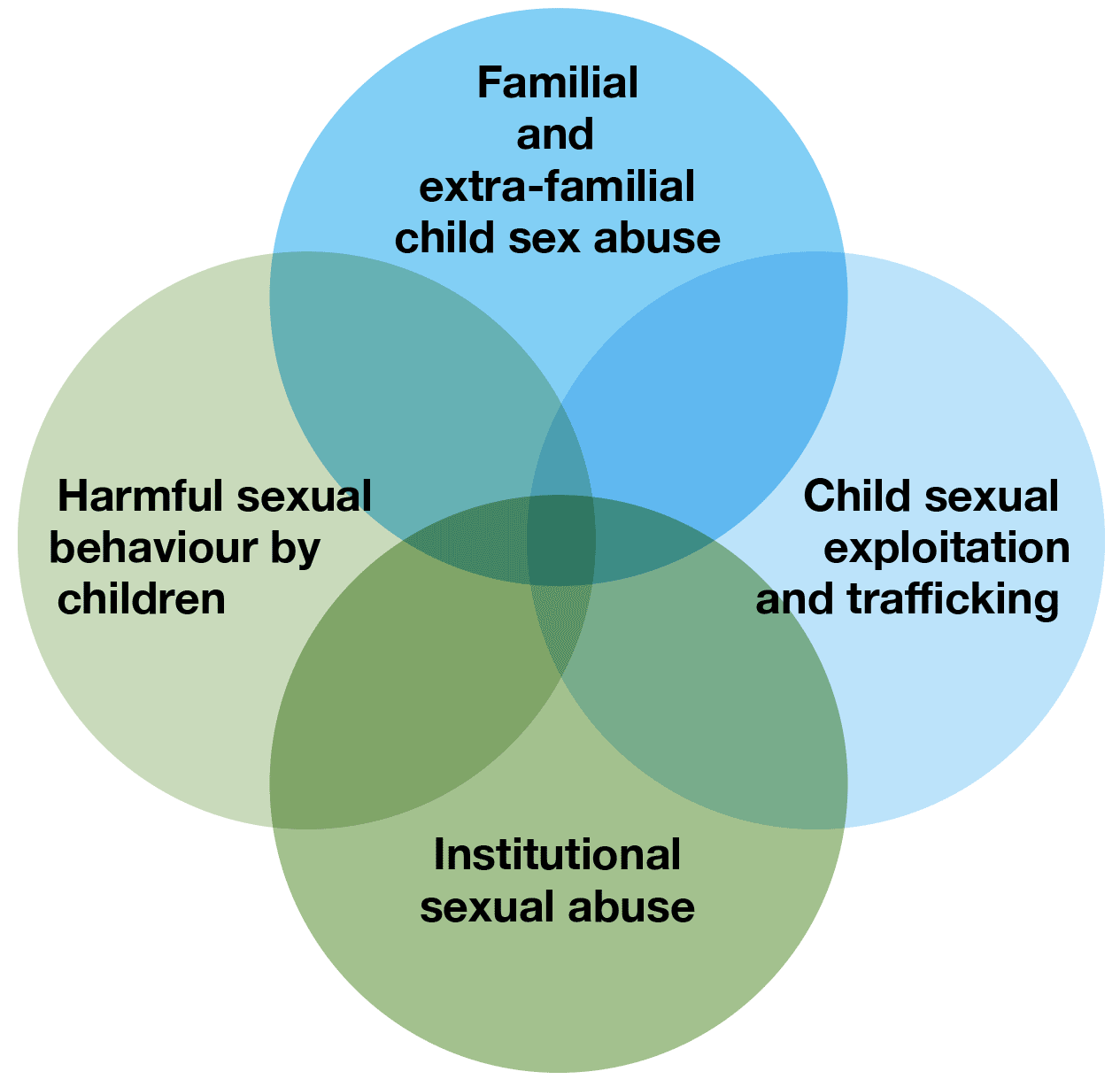
4.168 Overlapping categories of sexual abuse are represented in the diagram above. All require a child protection response. A child may experience multiple forms of maltreatment from different persons. Exposure to other forms of harm, such as domestic abuse or parental alcohol and drug use, may increase vulnerability to sexual abuse.
4.169 Children rarely come forward to disclose sexual abuse, especially when it occurs within the family network. Identification of sexually abused children by child protection systems in Scotland and the UK remains very low (NSPCC, 2021). This makes it critical that professionals and the public are aware of potential signs of child sexual abuse. This includes recognising indications of abusive relationships between an adult and a child, or between two children. Sexual abuse in the family may be perpetrated by a family member (including a member of the extended family) or by a person close to, or known to, the family, such as a neighbour, family friend, partner of a parent, or another trusted adult. Children under the age of 18 may also sexually abuse others within the family (as indicated below).
4.170 Abuse of power and trust, secrecy, trauma, a realistic or an imagined fear of the consequences, may all paralyse the ability of many victims to speak out, or cause subsequent retraction. Some children may be unable to seek help because of their age, understanding or disabilities. There may be under-reporting in some communities if dynamics such as obedience to paternal authority, shame and family honour act as isolating factors. It is common for survivors not to talk about the process of abuse until adulthood and when a child or adult feels able to speak, this is rarely a single event. For some, feelings of fear and shame are a permanent block to sharing, even if the abuse happened a long time ago.
4.171 The person that may first hear, realise or suspect that a child is being abused may be a non-abusing parent, sibling, friend, carer or keyworker. This could be at an unexpected moment, in a moment of high stress, or in a moment of sufficient safety. Third Sector organisations may be crucial intermediaries and sources of support. The response of those to whom a child signals alarm may determine what the child then shares. Sometimes children try to tell or signal their anxiety and this is not heard. Some 'telling' happens indirectly through presentation, and sometimes the telling happens gradually.
4.172 What a child needs when trying to share or signal an abusive experience for the first time is likely to depend on age, understanding and context. It may depend on whether the child is in a state of crisis or acute fear, or whether it has become possible at that moment because the intuitive or learned sense of safety with the other person provides enough containment to allow painful experience to be shared.
4.173 Most children need to know they have been heard and that how they feel has been recognised by someone who has remained quiet and calm and has not suggested details or judged actions. Sometimes this may include hearing confused feelings about the abuser. In most situations the child will need to know that the listener cares for them and will help to keep them safe, but cannot keep secrets that are harmful to the child (or to others), and will have to talk to someone else about how best to help. The person first hearing or recognising the abuse can help by keeping the door open for the child to talk further. The child may need support in getting through the rest of the day or night and then over time as feelings of fear and exposure can rise. They may need to feel they are not alone, that there are people who will listen and help, and that there are also people who do not need to know.
4.174 Indicators of abuse of a child may be physical, behavioural, social or psychosomatic. For example, they could include a combination of: concerning changes in behaviour at home or in school; avoidance of an adult; sexually inappropriate behaviour; health anxieties such as soreness in the genital and anal areas; sexually transmitted infections; pregnancy; and other indirect signals of anxiety. These may include feelings of isolation, stigma and difficulty in trusting others; sexualised behaviour, low self-esteem, withdrawal, aggression and disruptive behaviours; self-destructive behaviours and/or substance abuse. None of these examples are in themselves signs of sexual abuse. All necessitate professional curiosity about what lies behind these symptoms.
4.175 Contextual considerations. Practitioners involved in assessment, planning and intervention should consider the dimensions of risk and safety/protection 'online', in the family, and in the community. There may be a concentration of risk in specific locations.
4.176 Investigative components and processes when there is a concern about risk of significant harm are outlined in Part 3 of this Guidance. They should be co-ordinated and multi-disciplinary. When required, joint investigative interviewing will be carefully planned and trauma-informed. The national approach will be supported in forthcoming revised guidance. The Scottish Government's exploration of the child-centred Barnahus approach is also referenced in Part 3.
4.177 All practitioners should be trauma-aware. There must also be recognition that the process of sharing may not be a neat single event. Detail or experience may be released in fragments, at times, in a manner, and with persons determined by the child.
4.178 There is no single cause or explanation for the occurrence of child sexual abuse (CSA). The internet is a powerful vector for the development of the demand for sexual images of children and for sex with children. Perpetrators have often experienced traumatic maltreatment themselves as children. Some but not all are sexually fixated on children. Confused boundaries and parental use of alcohol or drugs can contribute to an environment in which multiple harms occur. Young children and children with disabilities may be particularly targeted by predators.
4.179 The impact of CSA is affected by the interaction of many factors including the age when it started, the nature and duration of the abuse and the relationship with the perpetrator. There are many mediating variables to do with non-abusive adults, the child and their wider environment. A distinctive interaction of risk and resilience factors plays out for each person in their world, over time. Effects often endure throughout adult life. They affect physical and mental health, family and intimate relationships, faith, education and work. Victims and survivors can also be more likely to experience sexual, physical or emotional abuse again (Fisher et al 2017). Those traumatised by CSA may be disproportionately represented in prison, homeless facilities and psychiatric care (Nelson 2017). However, appropriate support and therapy can promote recovery.
4.180 Supervision and training is essential for development and support for the skills and knowledge that open rather than close doors for children; and informs confident work with families. Practitioners need both critical consultation and support in emotional territory that may have disturbing resonance.
4.181 There have been fluctuations in reporting of sexual abuse in the UK. This may be linked to fluctuations in public awareness and attitude following high profile inquiries.
4.182 Prevention, interruption and deterrence of child sexual abuse requires strong collaborative intent within national policy, public and community education, parenting support, and evolving technological strategies. Children's Services Plans provide an opportunity to develop community or parent/child-focused prevention strategies to aid the identification or prevention of child sexual abuse in the family environment, as well as the recognition and interruption of wider exploitation. Child protection guidance is just a part of the foundation for protective action.
4.183 Resources supporting early recognition and prevention of child sexual abuse have been developed for individuals, families and practitioners by 'Stop It Now' (Scotland) at: https://www.stopitnow.org.uk/stop-it-now-scotland/resources/ and https://www.theupstreamproject.org.uk/identify. The Centre of Expertise on Child Sexual Abuse (Home - CSA Centre) provides access to research, practice knowledge and training to improve prevention and response. NSPCC offers resources and advice for those worried about child sexual abuse (Preventing Child Sexual Abuse & Keeping Children Safe | NSPCC, What Parents Need to Know About Sexual Grooming | NSPCC). The Scottish Government's Parent Club website offers tips and advice on parenting for families. The section on Child Sexual Abuse explores some of the myths around child sexual abuse and exploitation and how to spot the signs that something may not be right. It also looks at how to talk to your child about this issue, and how parents and carers can support their child if they have been a victim of sexual abuse or exploitation.
Sexual offences and signposts to legislation
It is illegal to:
- cause or incite a child to engage in sexual activity
- arrange or facilitate a child sex offence
- meet a child following sexual grooming
- have sexual communication with a child
- take, make or have indecent photographs of children
- sexually exploit a child (including paying for or arranging sexual services of a child)
Part 4 of the Sexual Offences (Scotland) Act 2009 lists offences criminalising sexual activity with a child under the age of 16 as categorised by the age of the victim.
Part 5 of that Act provides for offences concerning sexual abuse of trust. The Act provides that it shall be an offence for a person, over the age of 18, in a position of trust over a child or young person under the age of 18, or a person with a mental disorder, to intentionally engage in sexual activity with that child or person.
Child Abuse Images - The taking, distribution, publication and possession of indecent images of children under the age of 18 is prohibited by section 52 and section 52A of the Civic Government (Scotland) Act 1982.
The Abusive Behaviour and Sexual Harm (Scotland) Act 2016 (s2) makes it a criminal offence to disclose or threaten to disclose intimate sexual images. Sharing of intimate images (sometimes referred to as 'sexting'), is a term referring to the production and sharing of youth-produced intimate or sexual imagery by children who are under the age of 18. The imagery includes nude or nearly nude images and/or sexual acts; but does not include children sharing adult pornography or exchanging sexual texts which do not contain imagery. Neither does it include the sharing of sexual photos and videos of people under the age of 18 with or by adults, which would be a form of child sexual abuse and which must be referred to the police immediately by the designated child protection lead.
The Protection of Children and Prevention of Sexual Offences (Scotland) Act 2005 ('the 2005 Act') provides for an offence of 'grooming' which makes it an offence for a person to meet or travel to meet or to make arrangements for that purpose, in relation to children under the age of 16 for the purposes of committing a sexual offence following earlier communications (section 1), and for specific offences concerning the sexual exploitation of children under the age of 18 through prostitution (e.g. section 9) or the sale of sexually abusive imagery.
The 2005 Act also includes provisions for Risk of Sexual Harm Orders (RoSHOs) including interim orders, which are civil preventative orders aimed at protecting children from those who display inappropriate sexual behaviour towards them. To obtain a RoSHO, it is not necessary for the individual to have a conviction for a sexual (or any) offence. However, they must have done one or more of the following acts on at least two occasions:
- engaged in sexual activity involving a child or in the presence of a child
- caused or incited a child to watch a person engaging in sexual activity or to look at a moving or still image that is sexual
- given a child anything that relates to sexual activity or contains a reference to such activity
- communicated with a child when part of the communication is sexual
and as a result of those acts there is reasonable cause to believe a RoSHO is necessary.
The 2005 Act extends the use of Sexual Offences Prevention Orders (SOPOs) under the Sexual Offences Act 2003, so that they can be applied to those convicted of sex offences by the court when they are sentenced. Both SOPOs and RoSHOs place conditions (i.e. prohibitions and positive obligations) on those subject to the orders.
It is intended that RoSHO will be replaced in 2023 by Sexual Risk Orders (SROs) as provided for by sections 26 to 38 of the Abusive Behaviour and Sexual Harm (Scotland) Act 2016. The grounds and conditions on which the SROs can be made are wider than those for the previous order, so it could be used by the police to manage risk against adults as well as children. A court will be able to grant a new order if it is satisfied that it is necessary to protect a person from 'sexual harm'.
Accompanying Scottish guidance will be available on the application for, as well as the application of, SROs.
Also relevant
- Vulnerable Witnesses (Criminal Evidence) (Scotland) Act 2019
- Definitions and legal references in relation to CSE may be found in a practitioner briefing (Scottish Government 2016). https://www.gov.scot/publications/child-sexual-exploitation-definition-practitioner-briefing-paper/
A practice insight on this topic has been drafted to illustrate and explain key practice considerations, offer a resource, prompt reflection and signpost selected sources. It can be found in the Practice Insights supporting document alongside this Guidance.
Resources and References - Child sexual abuse
Child sexual exploitation
4.184 This section should be read in conjunction with sections on sexual abuse, under-age sexual activity and harmful sexual behaviour by children and young people.
4.185 Article 34 of the UNCRC requires public authorities to undertake to protect children from all forms of sexual exploitation and sexual abuse, in particular, by taking all appropriate national, bilateral and multilateral measures to prevent:
- the inducement or coercion of a child to engage in any unlawful sexual activity
- the exploitative use of children in prostitution or other unlawful sexual practices
- the exploitative use of children in pornographic performances and materials
4.186 Definition. Child sexual exploitation (CSE) is a form of child sexual abuse in which a person or persons of any age take advantage of a power imbalance to force or entice a child into engaging in sexual activity, in return for something received by the child and/or those perpetrating or facilitating the abuse. As with other forms of child sexual abuse, the presence of perceived consent does not excuse or mitigate the abusive nature of the act.
4.187 'Child' in this context means child or young person up to age 18. Boys as well as girls may be victims. Although CSE is not a specific criminal offence in itself, there is a range of criminal and civil options that can be used to disrupt and prosecute this form of abuse. See this link for a definition and practitioner briefing.
4.188 A child protection response is required, the manner of which will be determined following an inter-agency referral discussion. 'Disclosure' is not a prerequisite for a child protection investigation. CSE is under-recognised.
4.189 Exchange is the distinguishing factor in the various forms of CSE. The nature of the exchange may be material and emotional, including, food, accommodation, drugs, alcohol, cigarettes, gifts, affection, or a sense of belonging. In some situations the abuser or facilitator may also achieve financial gain or status. Alcohol or drugs may be given to the child. Exchange may take the form of compliance with sexual activity in order to avert a threat of harm to the child or to someone close to them. Children who have shared images of themselves may experience threats unless they comply with an abuser's demands. Perpetrators manipulate and apply coercive control.
4.190 In all forms of CSE there is an imbalance of power. This may relate to the abuser's age, gender, intellect, physical strength or other resources. Grooming may draw a child or children in to abusive processes or events. Grooming means targeting, befriending and establishing an emotional link with a child in order to manipulate, exploit, traffick or otherwise abuse them. Grooming can take place over a short or long period of time - from weeks to years. Violence and intimidation may form part of the coercion. Grooming can involve forming relationships with a child's family or friends and manipulating their trust or reliance in order to abuse a child.
4.191 A child may be drawn in to CSE in search of some form of affection, relationship or belonging. The child may or may not understand this as abuse. This does not equate to choice and consent, even for a 16- or 17-year-old who might legally consent to sex.
4.192 CSE may be associated with child criminal exploitation (CCE). CCE is not defined in law but is a term that has come to be associated with 'county lines'. County lines is a term used in the UK to describe gangs and organised criminal networks involved in exporting illegal drugs into one or more importing areas (within the UK), using dedicated mobile phone lines or other forms of 'deal line'. They are likely to exploit children and vulnerable adults to move and store the drugs and money, and they will often use coercion, intimidation, violence (including sexual violence) and weapons.
4.193 Child criminal exploitation occurs where an individual or group takes advantage of an imbalance of power to coerce, control, manipulate or deceive a child into any criminal activity, in exchange for something the victim needs or wants, for the financial or other advantage of the perpetrator or facilitator, or through violence or the threat of violence. The victim may have been criminally exploited, even if the activity appears consensual. Child criminal exploitation does not always involve physical contact - it can also occur through the use of technology. The criminal exploitation of children is not confined to county lines but can also include other forms of criminal activity such as theft, acquisitive crime, knife crimes and other forms of criminality. CCE requires a child protection response. Further information may be found in the section on CCE below.
4.194 CSE is often hidden. As with other forms of sexual abuse, the process of disclosure is rarely a discrete event, and patterns of disclosure and retraction are common. It may take many years, or may never happen. Fear, anticipation of stigma, reprisal, loss and shame that might follow disclosure intersect differently for each child. They are among the most common barriers to early recognition and help, alongside feelings of entrapment and helplessness. Shame and fear may be more pronounced within some cultural groups. Boys who have been abused often struggle to share their experience throughout life. Both containment and disclosure can be profoundly disturbing for the child and others closely affected. A trauma-informed approach to assessment and support is essential at all stages.
4.195 Sexual exploitation can occur through digital technology, in direct contact, or through a combination of both. Its occurrence often goes unrecognised and victims can feel isolated in plain sight. CSE of teenagers is more common than victimisation of young children.
4.196 CSE may be perpetrated by:
- family members, including being sold for sex
- older adults
- peer networks, within which abuse of power may occur
- gangs
- criminal networks
4.197 Digital technologies are often a vector for:
- grooming online for sexual abuse offline
- children viewing abusive images of children
- selling children online for abuse offline
- making abusive images of children
- sharing and viewing abusive images of children
- access to chat lines via the internet, social media, and online gaming platforms or mobile phones
- sharing of intimate images
(See further guidance in this section.)
4.198 It is the shared responsibility of professionals, parents and carers to support children's resilience, security and safe use of online technologies. Recommended links and resources may be found in the reference section.
Factors that may interact to create vulnerability
- abuse, neglect or an early adverse experience
- disrupted family life, including family breakdown and care experience
- domestic abuse
- bullying and peer pressure
- absence from education
- running from home or care
- experience of exclusion or isolation, especially in transitional phases
- drug and alcohol use
- poverty or homelessness
- poor health and low self-esteem
- learning disabilities and autism
- living with attitudes that normalise exploitation and violence in sexual relationships
- access to adult pornography and experience of attitudes that normalise sexual violence
- exploration of same-sex relationships and questioning of sexual orientation or gender identity can also result in children who identify as lesbian, gay, bisexual, transgender or intersex (LGBTI) being more vulnerable to CSE
Possible indicators of CSE
- going missing from home or school during the day, overnight or longer
- multiple callers/visitors including unknown adults/older young people
- entering/leaving vehicles driven by unknown adults
- evidence of/suspicion of physical or sexual assault
- disclosure of assault followed by withdrawal of an allegation
- unplanned pregnancy and/or sexually transmitted infections (STIs)
- peers involved in sexual exploitation
- drug/alcohol use
- isolation from peers/social networks
- exclusion or unexplained absences from school or college
- relationships with controlling adults
- unexplained money or 'gifts', including expensive clothing, new phones and other items
- frequenting areas known for adult prostitution
- children under 13 years asking for sexual health advice
- concerning use of mobile/internet/online devices (sending/receiving sexual images)
- multiple phones or SIMs, being protective of a phone, abnormally high volume of secretive calls, change in behaviour as a result of phone contacts
- depression, self-harm and suicidal thoughts
However, CSE can occur without obvious indicators, and careful assessment is needed to explore the meaning of the indicators above, which may be related to other issues.
4.199 Some CSE involves trafficking and criminal exploitation. This is when children are recruited, transported or exchanged in order to be exploited. Travel may include short distances (e.g. taxi rides) or medium distances (e.g. across a rural/island region or into an urban centre), as well as international travel. Assessments of possible CSE should consider if a child has been trafficked for the purposes of CSE. The immediate priority is to secure the safety and respond to the needs of the child. They should also be referred to the National Referral Mechanism (NRM) as explained below in the section on child trafficking. Not all trafficking involves CSE.
4.200 Some children and young people involved in CSE may be coerced into committing crimes by those who perpetrate CSE. This could include committing crime to escape abusers, or as a cry for help. Those who experience CSE may experience a punitive and criminalising response for engaging in antisocial behaviour, and may not be recognised as children who have been sexually exploited. It is essential that professionals engage with them, listen, and take time to understand the context of behaviour and choices with which the child has been faced. Victims of CSE require protection and support.
4.201 Children who run away find themselves making survival choices when they have nowhere to stay and feel alone. Abusers may befriend a child before or after they run, offer false sanctuary, or encourage the involvement of peers. Some children run to avoid abuse or out of fear of abusers, or of the consequences of being held to account for behaviours. A non-believing response from professionals or family increases risk of running. The National Missing Persons Framework for Scotland provides guidance for a multi-agency response when an individual goes missing, outlining roles and responsibilities, and including questions to use in risk assessment for concerns including sexual exploitation (Scottish Government, 2017).
4.202 Recruitment by children of other children for CSE does occur. The power and traumatic bond between abusers and victims can drive this process. Where a child is both a victim and has been involved in CSE of others, they require an approach to assessment and intervention that has a focus on their trauma and needs.
4.203 In some situations CSE has been continuing within communities, locations or institutions and authorities and the public have not suspected or responded to early signs of abuse.
4.204 The core components of the GIRFEC National Practice Model apply within an effective child protection response to suspected CSE. A Sexual Exploitation Risk Assessment Framework is being reviewed and revised (Barnardo's, Scotland 2020). Child Protection Committees must oversee relevant local inter-agency procedures and assessment frameworks.
4.205 The National Action Plan to prevent and Tackle Child Sexual Exploitation, published in 2016, set out the Scottish Government's plan to tackle the issue of child sexual exploitation. It focuses on prevention of abuse, prosecution, and supporting children and young people affected by child sexual exploitation. A Report on the Delivery of the Action Plan was published in 2020.
4.206 A practice insight on this topic has been drafted to illustrate and explain key practice considerations, offer a resource, prompt reflection and signpost selected sources. It can be found in the Practice Insights supporting document alongside this Guidance.
Resources and References - Child sexual exploitation
Indecent images and internet-enabled sexual offending by adults
4.207 Internet-enabled sexual offending includes possession, exchange and distribution of indecent images of and/or with children (IIOC); production of IIOC; sexual solicitation (online interaction with minors for sexual purposes); non-consensual sharing of sexual images; and conspiracy crimes such as working with others to distribute IIOC or to solicit children. All such behaviour causes significant harm to children. Investigation by Police Scotland will be necessary. An inter-agency referral discussion (IRD) will be necessary in relation to identified children who may be at risk of significant harm. Relevant legislation is signposted above in the section on child sexual abuse.
4.208 Most people who offend are male. Many are in relationships and have children. Motivations vary: some have a long-standing sexual interest in children, while some behaviours are exploratory or relate to the seeking out of extreme sexual material.
4.209 Beyond the direct and indirect abuse of children caused by the behaviour listed above, practitioners concerned with child protection will be concerned to know:
- is this person likely to commit a contact sexual offence with a child?
- has the person already committed contact sexual offences with a child?
4.210 The Risk Management Authority in Scotland's recent review of current evidence suggests that those convicted for viewing IIOC only are in general less likely to commit further sexual offences than other types of sexual offenders. When they do re-offend, it tends to be repeat viewing of IIOC. Increased risk of sexual offending is associated factors that include:
- previous sexual convictions
- other convictions
- problem alcohol or drug use
- domestic abuse
- other sexually inappropriate behaviour
- children being present when IIOC is viewed
4.211 Even when an individual is deemed 'low risk', this does not equate to no risk. For this reason, where the individual who has committed an offence has access to children, a holistic, in-depth assessment completed and reviewed by skilled and experienced practitioners should be the norm. Multi-agency assessment and close co-operation between child and family services and Criminal Justice Social Work and Sex Offender Policing Units is needed to evaluate the level of risk to children, and to recommend proportionate protective measures. This is a complex analysis. There may be no other police intelligence or indicators of significant harm. Dynamic variables include the degree of acceptance and attitude of the person who has committed the offence, along with acceptance of the potential risk by the non-abusing parent and immediate family, as well as the partner relationship, parenting styles, and the age, needs and circumstances of the children.
4.212 If risk is low, if the children feel safe to speak to key adults, and if comprehensive adult safeguards are in place, then it may not be necessary to compel the person to leave the family home while a full assessment is undertaken. In other circumstances there may be sufficient uncertainty about risk such as to require the taking of steps to ensure that the person does leave until a multi-agency assessment can review the options and form a Child Protection Plan. A written, shared family safety policy understood by all is needed to define arrangements for supervised contact, entry into children's rooms, sleep-overs, and any situations in which risk might be predicted.
4.213 Investigative processes can be experienced as devastating by the person who has committed the offence, their children and partner. Existing risks can be accentuated by stress. Shame, loss, fear, general anxiety and financial insecurity may be intensified by family, community and public reactions as well as by media coverage. Parents may not know what to say to their children. Children need extra support in these circumstances.
4.214 If accessed or required, the efficacy of treatment for those convicted for viewing of IIOC is not well researched. The person's engagement, understanding of their offending behaviour and evidence of change will be the subject of a post-programme report.
4.215 Children also access illegal and extreme material on the internet. For some, this behaviour can become compulsive and developmentally harmful. When such concerns arise, practitioners must explore the relevant history and context in order to identify any risks to the young person, as well as from them towards other children. Other guidance in this section covers harmful sexual behaviour by children and other forms of sexual abuse and exploitation.
Resources and References - Internet-enabled sexual offending
Children and young people who have displayed harmful sexual behaviour
4.216 This section may be read alongside the section below on serious harmful behaviour by children.
4.217 Harmful sexual behaviour (HSB) is defined as "sexual behaviour(s) expressed by children and young people under the age of 18 years that are developmentally inappropriate, may be harmful towards self or others and/or may be abusive towards another child or young person or adult" (Hackett, 2014).
4.218 Children's sexual behaviour may be described on a continuum ranging from normal to uncommon behaviours, including serious sexual violence.
| Normal |
Inappropriate |
Problematic |
Abusive |
Violent |
|---|---|---|---|---|
| Developmentally expected |
Single instances of inappropriate sexual behaviour |
Problematic and concerning behaviours |
Victimising intent or outcome |
Physically violent sexual abuse |
| Socially acceptable |
Socially acceptable behaviour within peer group |
Developmentally unusual and socially unexpected |
Includes misuse of power |
Highly intrusive |
| Consensual, mutual, reciprocal |
Context for behaviour may be inappropriate |
No overt elements of victimisation |
Coercion and force to ensure victim compliance |
Instrumental violence which is physiologically and/or sexually arousing to the perpetrator |
| Shared decision-making |
Generally consensual and reciprocal |
Consent issues may be unclear |
Intrusive |
Sadism |
| May lack reciprocity or equal power |
Informed consent lacking or not able to be freely given by victim |
|||
| May include levels of compulsivity |
May include elements of expressive violence |
From Hackett (2010) in: Report of Expert Group on Preventing Sexual Offending Involving Children and Young People (Scottish Government 2020, p30)
4.219 Practitioners' ability to determine if a child's sexual behaviour is harmful will be based on an understanding of what constitutes healthy sexual behaviour in childhood, as well as issues of informed consent, power imbalance and exploitation. Resources such as the Brook Traffic Light tool can be useful in recognition of potential child protection concerns about children's sexual behaviour.
4.220 Assessment of harmful behaviour is indicated if the behaviour meets any or all of the following criteria:
- it occurs at a frequency greater than would be developmentally expected
- it interferes with the child's development
- it occurs in a context of coercion, intimidation or force
- it is associated with emotional distress
- it occurs between children of divergent ages or abilities
- it repeatedly recurs in secrecy after intervention by caregivers (Chaffin et al., 2002)
4.221 Some children sexually abuse other children. This may include harmful sexual behaviour:
- between similar-age children in the context of intimate relationships
- in the context of gangs
- between children within the same family
- between older and younger children
- online and/or face-to-face
- including abuse that falls within the definition of child sexual exploitation
4.222 Children may be involved in sexual discussions or acts, whether directly or through the use of digital technology. This may include the sharing of images that are harmful to self and/or others, given their age or stage of development (Hollis et al., 2017).
4.223 Behaviours vary in nature, degree of force, motivation, context, level of intent, level of sexual arousal, and the age and gender of victims. Just as there is a continuum of behaviour, there needs to be a continuum of potential responses, ranging from broad educational input on consent and relationships, through to multi-agency public protection arrangements for serious sexual offences.
4.224 Those children who harm may have been harmed themselves. Many will have unmet emotional needs, use coercion and aggression as coping strategies, have poor emotional regulation, have experienced pre-adolescent sexualisation, and/or have unresolved trauma. Some may have developmental delay, intellectual impairment or be affected by autism.
4.225 Whether an immediate response to harmful sexual behaviour is required depends on interacting considerations relating to risk, age and context. In all actions and decisions the primary professional consideration must be to safeguard and promote the wellbeing of the children involved.
4.226 In all cases where a child or young person displays sexual behaviour that may cause significant harm, immediate consideration should be given as to whether action should be taken under child protection procedures, in order both to protect children harmed or at risk of harm by the behaviour and to address any child protection concerns that may at least in part explain why the child/young person has behaved in such a way.
4.227 A risk assessment should be carried out to determine whether the child or young person should remain within the family home and, if necessary, to inform the decision as to what might be an appropriate alternative placement. In the event that an alternative placement is needed, residential staff or foster carers need to be fully informed about the harmful or problematic sexual behaviour, and a risk management plan drawn up to support the placement. Teamwork between all involved is the key to safety.
4.228 Where concerns are below the threshold of significant harm towards or caused by a child, there may still be a need for co-ordinated assessment and support to address the needs underpinning troubled or troubling behaviour.
4.229 Sexual abuse between siblings, when they are children, may be the most common form of intra-familial child sexual abuse, although data on prevalence is scant. Professionals need to be precise about the language they use to label sexual behaviours of siblings which can include developmentally normal sexual interactions between young sibling children; problematic sexual behaviour between siblings which may be harmful to each child involved; and sibling sexual abuse which could include a range of persistent and exploitative behaviours which can be significantly harmful immediately and over the lifespan. Case records should include detailed descriptions of the behaviours in addition to the labels for the avoidance of any future doubt.
4.230 Some children abused by siblings think they will not be believed. Children who have sexually abused a sibling may often have experienced abuse and trauma themselves. Their needs as children must also be recognised and supported alongside the assessment of risk, safety plans and options for the management of sibling contact if siblings are separated. Family relationships and needs must be considered as a whole. The cultural context must be considered in the assessment and approach to support.
4.231 Every individual and every relationship in the family may be impacted. The recognition of sibling abuse usually creates a crisis for the family as a whole. Parents can feel torn between the need to support and protect each child. Their response is a key variable in assessment, interim safety planning and a co-ordinated inter-agency plans supporting recovery. Sensitive support is therefore necessary to help the family recognise where harm has occurred while also encouraging them to recognise that change and healthier relationships are possible. Sibling sexual abuse: A knowledge and practice overview (csacentre.org.uk).
Early and Effective Intervention (EEI) is not a 'disposal option' but rather a co-ordinated, planned support for children who come to the attention of the police for offending, concerning or harmful behaviour. Police Scotland 'risk and concern hubs' should identify when referral for an IRD under child protection processes or EEI may be appropriate. EEI should include the concerning and harmful behaviour of children aged under 12 years.
Referral to the Principal Reporter can be considered at any stage if there are reasons to believe a child may need compulsory measures. One of the potential grounds for a hearing is that the child's conduct has had, or is likely to have, a serious adverse effect on the health, safety or development of the child or another person (Children's Hearings (Scotland) Act 2011, section 67(2)(m)).
The Age of Criminal Responsibility (Scotland) Act 2019 was implemented in stages. It was commenced in full on 17 December 2021. The Act raised the age of criminal responsibility in respect of children under 12 years of age, but makes provision for their referral to a children's hearing on grounds other than having committed an offence. This could apply to children who are suspected of violent or dangerous behaviour which has caused or risks causing serious physical harm to another person or who, by behaving in a sexually violent or sexually coercive way, have caused or risked causing harm (whether physical or not) to another person. A flow chart depicts the relationship between provisions in the Act and Child Protection Processes.
Care and Risk Management (CARM) processes may be applied when a child (aged 12-17) has been involved in an incident of a serious nature (irrespective of the legal status of the incident) or where a pattern of significant escalation of lesser behaviours suggests that an incident of a serious nature may be imminent. The lynchpin of effective CARM processes is the inter-agency referral discussion that must occur when concerns of this nature arise. CARM Guidance (CYCJ 2021) can be accessed at: https://www.rma.scot/resource/standards-guidelines/.
4.232 When parents find that their child has acted in a way that has sexually harmed others, they may experience feelings of shock, denial, confusion, guilt, shame, anger, isolation and powerlessness. Feelings of hurt, love and anger can coincide with conflicted priorities, particularly when the victim of harm is a member of their own family. Parents have a critical role in promoting safety and helping their child move on from behaviour that may harm themselves or others. Parents often need sensitive support to help them understand what has occurred and how to work together.
4.233 Every child's plan should be holistic and tailored to need and context. Risk assessment and management measures and interventions are essential, but should be balanced with nurture and encouragement. Plans should build on those skills and relationships that promote resilience. The GIRFEC Wellbeing indicators apply. In addition, each child should receive individual attention within a systemic approach, so that they become more able to:
- understand their feelings and behaviour
- meet their own needs in a socially acceptable way
- develop skills in the context of home, school and community
- enjoy positive relationships at home, at school and in the community
- encourage and sustain longer-term change, anticipating stresses
Resources and References - Harmful sexual behaviour by children
Child protection in the digital environment/online safety
4.234 The internet, online services and associated technologies are an integral part of our everyday lives, and particularly so for our children and young people. These offer many opportunities that support learning, engagement with others and, crucially, helping children and young people to find the right support and help. We want all children and young people to be empowered and confident to access the digital world creatively and fearlessly. Article 17(e) of the UNCRC expects public authorities to develop appropriate guidelines to protect children from information and material injurious to his or her wellbeing. Protecting them from online harm is a challenge in a fast changing media environment. A sense of anonymity and disinhibition can escalate risks. Signposts to key legislation in relation to sexual offences are provided above in the section on child sexual abuse.
4.235 Definition. Online child abuse is any type of abuse that occurs in the digital environment and the internet, facilitated through technology and devices such as computers, tablets, mobile phones, gaming devices and other online-enabled devices.
4.236 If abusive content is recorded, uploaded or shared by others online, there is a risk of the on-going experience of abuse.
4.237 Online abuse can include online bullying; emotional abuse and blackmail; sharing of intimate images; grooming behaviour; coercion and preparatory behaviour for abuse including radicalisation; child sexual abuse and sexual exploitation as described above. Spyware which enables monitoring and tracking of activity on devices and offline locations may be used abusively. Perpetrators may be strangers, family members, friends or professionals.
4.238 Primary protection involves collaborative, preventative action. Listening to the views of children and young people is critical in ensuring that the on-going development of protective efforts are relevant and beneficial. Exposure to risk of online sexual harm is a common experience.
4.239 Prevalence. A Crime Audit published by Her Majesty's Inspectorate of Constabulary in Scotland (HMICS) in 2016 reported that 11.4% of recorded sexual incidents had a cyber-element to them, and a significant proportion of these involved children.
4.240 Education/Training. Children should access education that addresses online sexual harm before spending unsupervised time online. This should include information about why it occurs, the different forms it can take, how to identify it, its possible impacts, and what to do if it happens. Children need help to understand what constitutes harm within the context of peer relationships or existing online networks. The 'normality' of such occurrences can reduce awareness of the harm caused to individuals and the harm caused by creation of normative expectations, particularly sexual demands made in relation to girls.
4.241 Education around online sexual harm must be embedded in the school curriculum for children and young people. It is important that children and young people are supported in building their own resilience in the online world. Being online offers positive opportunities and avoidance-based messaging may be unhelpful. Schools are the most common source of learning about sexual harm, however family members, friends, peers and the media are also significant sources of learning. References for this section offer relevant resources and specific links.
4.242 Professionals involved in assessment and planning should develop a knowledge of online risks, the impact of technology on the lives of children and young people and the use of technology by parents and carers which may impact on children. This includes an awareness of the way technology, including spyware or equivalent, may be used abusively, to coerce and control. Professionals should consider the use technology from the child's perspective, with a view to working together on plans relevant to the situation.
4.243 Response. In relation to youth-produced sexual imagery, staff:
- must in any instance follow relevant agency protocol, listen to the child, and report to the designated child protection lead
- must not view, download or share such imagery, or ask a child to share or download it - this is illegal. It is relevant to take note of who the child says has sent the image, who has seen it, and the relevant host website if known, as this information could help in taking steps to remove it
- must, if the imagery has already been viewed, report this fact to the designated child protection lead
- must not delete the imagery or ask the child to delete it
- must not ask the child or children involved in the incident to disclose information regarding the imagery. This is the responsibility of the designated child protection lead
- must not share information about the incident to other members of staff, the child or children involved or their, or other, parents and/or carers
- must not say or do anything to blame or shame any child involved
- must explain to the child that the material must be reported, and reassure the child that they will receive support and help
4.244 Reporting to Police Scotland or to social work for consideration of an inter-agency referral discussion (IRD) will normally be the recommended response to ensure the concern is placed in context, and that next steps are proportionate, supportive, and if necessary, co-ordinated. An IRD will be completed to allow appropriate child protection measures and on-going risk assessments to be progressed through joint information gathering, information sharing and decision-making through the IRD.
4.245 Information and advice on complaints procedures and reporting routes to social media providers about inappropriate content can be accessed from Report Harmful Content.
Harmful online challenges and hoaxes
4.246 Harmful online challenges entice people to do dangerous activities. They are often deliberate lies designed to seem truthful, which mislead and upset people. In some cases, online challenges or hoaxes may appear interesting or exciting whilst still encouraging people to do something that is not safe or not real. Harmful online challenges and hoaxes are commonly distributed through social media and messaging apps, often inspiring or daring others - including children and young people, to participate or share.
4.247 When children and young people encounter these online challenges and hoaxes, they might be tempted to do or share things out of curiosity, or to impress their friends or to feel part of a community. This content can spread very quickly and reach large audiences, leading to a range of hype and panic and sometimes resulting in harm.
4.248 Professionals should be aware that it is not helpful to share targeted warnings that name and/or described the challenge, hoax or video in question; or which platform the content appears. Doing so may cause distress to both children and families and/or raise curiosity and drive children to the content that is of concern. Therefore, targeted warnings should not be issued to the general public.
4.249 Response. Parents, carers and professionals working with children should:
- have regular conversations about children's experiences online and how they can stay safer
- recognise that online peer pressure can be very overwhelming for children
- support children to think critically about whether the content they encounter online may hurt or harm them or someone else
- talk with children about strategies for saying no to things which may sound fun but they don't feel comfortable doing
4.250 When a professional becomes aware of such a challenge or hoax circulating amongst children and/or young people, they should:
- remind children they can talk to a trusted adult if they:
- see something online that they are unsure about, or makes them feel a bit uncomfortable
- see something online that may be appealing but which they suspect may not be true and may be harmful
- see something that frightens or worries them
- are approached by someone that makes them feel uncomfortable
- respond calmly when a child or young person tells them about something online that causes concern
- not blame a child that has taken part in a challenge/hoax but have an open and honest conversation about why they wanted to do it and give them support
4.251 Action required. Where a professional becomes aware of an online challenge or hoax circulating amongst children or young people, every effort must be made to ensure this has not resulted in an incident of actual harm to anyone. The police should be notified as soon as possible in any case. Where an online challenge or hoax has resulted in harm to a child or young person then this should be reported in line with child protection procedures.
Resources and References - digital environment/online safety
Under-age sexual activity
4.252 This section should be read in conjunction with adjacent sections on sexual abuse and harmful sexual behaviour by children and young people. A gender-based analysis informs national policy and guidance (Scottish Government 2017). The Scottish Government (2019) has published Key Messages for Young People on Healthy Relationships and Consent (Scottish Government 2019), a resource which includes advice for professionals working with children of secondary age, 12-17.
4.253 Protecting children means supporting them as they learn about healthy, respectful, consensual and safe relationships. Practitioners require local service protocols which are clear about the law. They must be provided with key messages in support of professional judgement about what is a proportionate and ethical response for each situation.
4.254 There are situations that do not require child protection processes, in which a young person may need immediate support in relation to their sexual risks, development and relationships. These may be addressed either on a single-agency or multi-agency basis, depending on needs and circumstances.
4.255 In cases where it is assessed that criminalising the behaviour is not in the best interest of any child involved, there should be a multi-agency decision taken as to how to best engage the offending child or children involved to ensure that they are supported in learning the concept of consent, why their behaviour was considered inappropriate and the potential future consequences of repeating this behaviour. Consideration should be given to the best method of engaging the child, including when, where, and by whom, taking into account their circumstances and those of their family. Consideration should also be given to the best way of involving parents or carers, and all engagement with the child/children and their family should happen in a trauma-informed way. Note that children under the age of criminal responsibility cannot be held criminally responsible for their actions; however the proposed supported learning described here is also relevant to children aged under 12 years.
4.256 Child protection concerns arise when the impact of under-age sexual activity could cause significant harm. A young child (under 13 years of age) cannot consent to any form of sexual activity (within Part 4 of the Sexual Offences (Scotland) Act 2009).
4.257 The 2009 Act maintains the age of consent at 16 whether a person is straight, lesbian, gay, bisexual and/or transgender. When there is reason to believe an offence against a child has been committed as defined in the 2009 Act, an IRD will be convened.
4.258 An IRD must also be convened with older children (over 13 years) who may have been pressured in to sexual activities involving force or exploitation, may have had indecent images taken, suggesting abuse or exploitation, or may otherwise be at risk of significant harm relating to sexual activity.
4.259 Section 37 of the Sexual Offences (Scotland) Act 2009 creates the offence of older children (aged between 13 and 16 years) engaging in sexual conduct with or towards one another. Assessing the risk of significant harm, deciding whether to hold an IRD and planning the next steps should include consideration of:
- any power imbalance between the persons involved
- the age, including any age difference, of the persons involved
- whether there was conduct involving overt aggression, manipulation, coercion or bribery
- any disinhibiting use of substances, under pressure or encouragement from a more dominant person or persons
- the child's use of substances contributing to risk of harm
- attempts to secure secrecy having been made by the dominant person, beyond what might be usual in a teenage relationship
- previous concerns recorded by police/health/social work
- persons involved denying, minimising or accepting concerns
- evidence of 'grooming'
4.260 Practitioners must be aware of the power and trust inherent in their own position and communication with each child. They must be aware of the influence of their own language, attitudes and boundaries
4.261 While consent to sexual activity under age 13 is not possible, support for children's learning should reinforce the message that 'consent' refers to a mutual process; that verbally obtained consent is necessary but not sufficient; and that it is always necessary to be sensitive to another person's feelings and fears, which may be communicated in an on-going process, not only in words but also in body language and non-verbal responses. Consent can be withdrawn at any time; that consent is required every time sexual activity takes place, even if a person has previously consented.
4.262 Power imbalances affect a child's understanding of consent and must form part of a practitioner's consideration when balancing issues of confidentiality, welfare and protection. A child's age, sexual identity, gender, disability, self-perception and ability to understand and exercise choice will all affect consent. Power imbalances can be created by fear, manipulation or threat. They can be created by differences in sexual knowledge, or by the dynamic when a child has been feeling excluded or unwanted. The social context and location of 'consent' may dismantle a child's ability to stand alone or stand aside and choose. Children may not understand that exploitative behaviour can constitute abuse.
4.263 If sexual activity is taking place/has taken place within a safe and mutually respectful relationship, then confidentiality should generally be maintained as there is a high threshold for when the duty of confidentiality should be outweighed. The facts and circumstances of each case must be carefully considered before deciding if the public interest favours the disclosure of confidential information.
4.264 If a young person is under sixteen and sexually active, professionals considering overriding the young person's confidentiality must first consider the circumstances of the specific case, consulting with child protection leads as appropriate. Whilst there is generally a high public interest in keeping sensitive information confidential, confidential information may lawfully be shared, for example, where there is an overriding interest which outweighs the duty of confidentiality. Decisions must be made in relation to this particular child, their needs in context, and the relevant legal basis. Overriding confidentiality must be justified and proportionate, taking into account the nature and probability of risk to the young person and/or others. The child's wishes and feelings must be heard and taken into account. The reasons for decisions made (for instance in relation to information sharing) must be recorded. Recognition should be given to the particular issues for LGBT young people. Schools should be alert to the fact that some young people may not have told everyone in their lives about their sexual orientation and/ or gender identity, and 'outing' them could cause needless distress. If a child protection or wellbeing concern is raised, schools should follow their existing policies.
4.265 Children may express and then retract concerns, depending on what pressures are facing them. Practitioners must seek to keep the door open so that the child knows where they might go to share anxieties or questions. Parental support will in most situations be a crucial part of the picture. When there are interacting concerns about how family circumstances impact on the child's safety in the wider world, practitioners will take this context into account in contributing to assessment and planning to support safety and wellbeing.
Resources and References - Under-age sexual activity
Pre-birth assessment and support
4.266 The Preamble to the UNCRC makes it clear all children need safeguarding and care, including appropriate legal protection, before as well as after birth; and Article 24(2)(d) requires public authorities to ensure appropriate pre-natal and post-natal health care for mothers in the context of access to health care services. In Scotland, all services providing for expectant mothers and babies must have protocols and supervisory structures in place to support equitable, proportionate, effective and timely action to keep mother and baby safe and well. A Pathway to Care for Vulnerable Families (0-3) (Scottish Government 2011) describes standard support expectations. The national approach to maternity and neonatal care is described in 'The best start: maternity and neonatal care plan executive summary' (Scottish Government, 2017). Maternity services for young parents | Turas | Learn (nhs.scot) is a resource informing support for young mothers and fathers.
4.267 All practitioners who work with expectant parents must be aware of parental behaviour and circumstances that could cause significant harm to an unborn baby. They must be aware of how to refer concerns about potential harm to statutory services; and confident about the lawful basis for information sharing. Child Protection Committees and Chief Officers will ensure frameworks for pre-birth assessment and support for children at risk are in place.
4.268 Health, police or social work will trigger an inter-agency referral discussion when there is reason to believe an unborn baby may be at risk of significant harm, as described in Part 3. The potential impact of an interaction of risk factors such as the removal of previous children; the impact of drug use; and/or the impact of domestic abuse and mental ill health upon mother and unborn baby should tip professional judgement towards the need for an IRD or parallel pre-birth processes.
4.269 Guidance on Part 12 of the Children and Young People (Scotland) Act 2014 highlights that pregnancy can be a turning point for parents involved in alcohol and drug use and criminal behaviour. Relevant services should be provided to pregnant women who the local authority considers are going to give birth to a child who will be at risk of becoming looked after (section 68(5) of the 2014 Act) and the father of the child ("or a qualifying person in relation to an eligible pregnant woman" under section 68(6) of the 2014 Act). The aim is to ensure that any decision-making is informed by assessment and support work begun as early as possible; and geared to the mother's and baby's specific needs, in the context of their family situation.
4.270 A pre-birth assessment can begin whenever pregnancy is confirmed, ordinarily at around 12 weeks gestation or at the point of initial scan. When there is a risk of significant harm, it should begin as soon as possible. This provides the unborn baby with the best possible opportunity to thrive and gives parents maximum opportunity to engage, achieve an understanding with key practitioners and family supports; and begin to work towards necessary changes.
4.271 Assessment should be multi-disciplinary, co-ordinated by a social worker as lead professional, consulting with key practitioners including GPs, midwives, family nurses, health visitors and relevant adult services. Professional judgement should be assisted by structured assessment tools. General principles in Part 3 of this Guidance apply.
4.272 The late allocation of the family to social work support can contribute to tensions in the working relationship, making a robust pre-birth assessment less possible. Continued uncertainty about the care plan will raise anxiety for expectant parents as the baby's arrival approaches.
4.273 Parents who are in their teens; care-experienced; who have had profoundly traumatic experiences; and parents with learning disabilities; are among those likely to need additional and sustained support, explanation and advocacy. Parents who have had no experience or understanding of child protection systems, may struggle to understand processes. Cultural and language differences often add to gaps in understanding. Some assessment tools may be helpful (for example, Best Beginnings: Parents with learning disabilities).
4.274 Part 3 describes Child Protection Planning Meetings, Core Groups and discharge planning meetings. Timescales for planning meetings are summarised in the appendices. Parents need time to read and understand or to get help in understanding reports before meetings.
4.275 Pre-birth involvement creates the opportunity for detailed care planning for the baby following the birth, supporting a smooth transition from maternity to Health Visiting/Family Nursing, whilst ensuring sufficient continuity of multi-agency support, especially in the first year. When an assessment concludes that a baby cannot be safely cared for with birth relatives, foster carers can be engaged early in the process. This means carers and parents can meet before the birth to plan the transition and to support development and sustaining of relationships essential for the baby as appropriate, as the plan evolves.
4.276 In some situations 'concurrent planning' is appropriate. This involves intensive but time-limited work with parent(s) towards the return of their child, within a timescale that is in the child's interests; while holding the possibility that the temporary placement might offer permanent care if a safe return to the care of parents cannot be achieved (CORAM 2013).
4.277 The revised Universal Health Visiting Pathway in Scotland: pre-birth to pre-school - gov.scot (www.gov.scot) has a strong focus on prevention and early intervention. It offers a consistent approach to the Heath Visitor role and services across Scotland. It presents a core home visiting programme as a minimum standard to be offered to all families with children 5 years of age and under and includes a pre-birth home contact at 32-34 weeks of pregnancy. Where a family are known to Health Visiting Services, the Health Visitor should be involved in any pre-birth assessment, pre/post-birth CPPMs and pre/post discharge planning meetings.
4.278 The Family Nurse Partnership (FNP) programme is an evidence-based change programme that is delivered in the parents' own homes and is offered to first time parents aged 19 years or under and eligible 20-24 year-olds in some areas, and their children. Family Nurses will visit regularly from the early stages of pregnancy and should be involved in any pre-birth assessment, pre/post-birth CPPMs and pre/post discharge planning meetings.
4.279 Permanent, loving, nurturing relationships are what matter most to children. The optimal route to permanence depends on the needs and circumstances of the child. Permanence might be achieved through:
- the child remaining within or returning to the family, (with or after support)
- by kinship carers obtaining a Section 11 Order via the courts; or
- by means of adoption orders being granted by the court in favour of an adoptive parent
4.280 The first stage of Scottish research on permanence planning (Biehal et al., 2019) underline that the pre-birth period is critical in terms of assessment and decision-making.
4.281 Two practice insights on this topic have been drafted to illustrate and explain key practice considerations, offer a resource, prompt reflection and signpost selected sources. They can be found in the Practice Insights supporting document alongside this Guidance.
Resources and References - Pre-birth assessment and support
Children who are looked after away from home
4.282 Article 9 of the UNCRC outlines general requirements for public authorities when children are lawfully separated from his or her parents in his/her best interests.
4.283 Child protection for children looked after away from home involves integration of some of the general features of good assessment and planning. It also involves clearly defined processes when child protection concerns, such as allegations against carers, arise in placement.
4.284 Child protection concerns relating to unaccompanied children should be addressed by the same inter-agency processes as for a UK national.
4.285 A looked after child may be placed with kinship carers, with foster carers, prospective adopters, a residential school setting, or in residential care in a children's house.
4.286 The best protection is preventative support. Thorough assessment of carers and of children's needs, alongside planning and support of placements, are key to ensuring that placements can meet children's needs for safety and nurture. Once in placement, trust and physical and emotional safety evolve through routine experiences of nurture, empathy, nourishment, sleep, daily achievement, understanding, play, choice and hope.
4.287 A key outcome of child protection and work with looked after children should be the development of a child's sense of stability and safety, achieved through the building of trusting and nurturing relationships with their adult care givers. This refers to exploring, promoting and sustaining relationships of enduring and protective significance. This includes relationships with brothers and sisters. "Where living with their family is not possible, children must stay with their brothers and sisters where safe to do so and belong to a loving home, staying there for as long as needed" (Independent Care Review, 2020).
4.288 When children are placed quickly, in response to a crisis, any initial discussion between those seeking and providing services must be thorough, to ensure the risks are recognised and can be sufficiently supported. This includes risk assessment about co-placement of children whose behaviour could pose risk to others.
4.289 Growth of relationship, trust and recovery is likely to depend on appreciation of the impact of trauma, neglect and disrupted attachment for each child. This requires attention to what each child is communicating, not only by what they say, but what they do and how they present.
4.290 Sustaining care. It is to be expected that looked after children who have had to leave the care of their parents will usually experience complex emotions and distressed, disrupting behaviours. Many will have experienced separation and loss in their early years, and will have been emotionally and physically neglected or abused. Layers of trauma are likely to result in deep-rooted fearfulness, anxiety, lack of trust and confusion. A constant need for reassurance and for soothing can occur when there is underlying confusion, fear and emotional distress. This can be bewildering and exhausting for carers.
4.291 Carers and their families need guidance and support to enable them to offer trauma-informed care, appropriate to the developmental needs and known life history of each child. The Independent Care Review has underlined the need for preventative support for kinship Carers, foster carers and adopters. ("Whatever the mode of arrangement, Scotland must ensure that children living in kinship care get the support they need to thrive." Independent Care Review, 2020).
4.292 When looked after children are moving between placements and between authorities, transitional arrangements must be negotiated and planned in order to avert what may otherwise emerge as child protection concerns. Sufficient transitional support when children move on from placements may likewise reduce crises that could be anticipated. The Independent Care Review has emphasised that, however urgent the situation, "� children and their carers must have access to information about their rights and entitlements at any point in their journey of care."
4.293 Safer caring. A co-produced family agreement, involving everyone living in the house, helps to ensure that each resident child and adult, and visitor, knows how to behave to keep everyone in the house feeling safe (including pets). This is advised for registered foster carers to ensure that everyone who lives in the household, and those who visit, know how family rules and boundaries work.
4.294 Disabled children who require extra time, skill and support, should only be placed with carers who have the time, skills and support to deliver safe care for each child placed.
4.295 The lead professional has a role in ensuring the integration of safety and child protection aspects within a holistic and co-ordinated child's assessment and plan. Any significant change in a child's behaviours and wellbeing must be recognised, and the underlying needs considered within a child's plan.
4.296 Allegations against registered carers. Children need to know who they can speak to when they have anxieties about where they are living or about behaviour of others outside the placement. Local authorities must ensure that protocols for inter-agency investigation of allegations of abuse against carers are in place. Allegations about kinship carers with whom a child is placed should be investigated in the same way as allegations about a child living with parents.
4.297 Lead professionals have a responsibility to clarify concerns raised around a looked after child in collaboration with local child protection services. They will also need to liaise with service managers for fostering or residential services as required.
4.298 The main consideration in responding to any concern must be the safety of the child. Every looked-after child voicing a concern must be listened to and taken seriously. Concerns must be rigorously investigated. Equally, a carer's perspective should be heard. They must be treated fairly and with respect. Carers should be given information about the concern at the earliest point compatible with a thorough investigation. Where the concern involves reports of abuse, there will be an inter-agency referral discussion. The carer will be subject to investigation on the basis of local inter-agency protocols. Allegations of abuse by carers must be dealt with by appropriately trained child protection practitioners and managers.
4.299 Responses to allegations should be proportionate to the nature of the concerns raised. Whatever the action to be taken, practitioners will need to discuss the needs of the child, the context of their care, key events in their lives at that time and any possible triggers for a concern being raised, either by the child or others. Fostering or residential service providers should be included in the discussion. All practitioners involved with protecting the child need to be fully informed about the role of carers, and the regulations that relate to their work. These meetings will facilitate the sharing and assessment of information, leading to a decision as to the next steps to be taken. If emergency action is required to protect the child, the consequences of all alternatives should be considered, despite the pressure to achieve an immediate reduction of risk. Options for the way forward for a looked after child are the same as for children in their own families.
4.300 When concerns about a looked after child are raised, it should be remembered that further disruption, such as a sudden move into a new care environment, will further compromise their recovery. The consequences of removing a child must be considered alongside their safety. Placement stability should be maintained when this is safely possible. Each child's experience, views and presentation will be a central consideration.
4.301 Parents of looked after children. Child protection practitioners must keep the child's needs and wellbeing central in listening to parental concerns. Development of respectful relationships between the birth family and carers is essential for the child's short and long-term wellbeing and identity.
4.302 Inequalities. Children in the most deprived 10% of small neighbourhoods in Scotland are nearly 20 times more likely to be 'looked after' in care, or on the child protection register, than children in the least deprived neighbourhoods (Bywaters et al 2017). This is relevant at child, family, community and strategic levels to an understanding of the intersection of risks that must be addressed in child care and protection.
Resources and References - Children looked after away from home
Reunification or 'return home'
4.303 Child protection and reunification planning are connected in principle and process. To prevent repeated and compounded harm, reunification for children who have experienced chronic abuse and neglect should be preceded by a comprehensive assessment of whether or not the child should return home. Increased support is required when considering reunification. Continued assessment and regular review is required.
Prompts below are recommended by Wilkins and Farmer (2015):
- view the plan from each child's perspective, gradually and, stage by stage. Consider the child's timescales and need for emotional security. Ensure the child has persons they can trust and with whom they can share how they are coping with changes. Begin to think about what would be needed for reunification from the beginning of the placement
- strength-based approaches (such as family group decision-making) may be helpful to enlist the co-operation and understanding of key family members, to build a package of supports, and to consider options and contingency plans
- a methodical and structured approach to assessment and reunification is recommended. This is crucial when there are long-term and interacting concerns, such as use of alcohol or drugs leading to chronic neglect
- previous failed reunification plans should be taken into account. Analysis of the child, family history and strengths and concerns within and beyond the family is needed. Professional judgement about the likelihood of reunification should integrate multi-agency perspectives and assessment of capacity to change, and supervisory review of evidence and analysis
- relationships that will have lasting value to the child should be supported. Assess and plan for provision of any additional support needs a child may have, for instance in relation to mental health. Give families a reasonable opportunity and level of support to make the changes while keeping child's safety and best interests central to decision-making
- seek to understand and adapt to cultural differences. Seek to work as a team with family, carers and key professionals in preparing for change and reunification, as appropriate. Ensure there is evidence of parental abilities to sustain change
- help children and parents to work with practitioners to agree goals and understand what is happening at each stage. Agree lines of communication. Agree how to keep progress under close review. Consider how required support can be sustained, stepped up and stepped down as needed. Ensure that following reunification, the child is seen and heard regularly, so that significant changes are noticed and can trigger a supportive response
Resources And References - Reunification or 'return home'
Preventing the repeated removal of children
4.304 "If children are removed from the care of their parents, Scotland must not abandon those families. Families must continue to be provided with therapeutic support, advocacy and engagement in line with principles of intensive family support" (Independent Care Review, 2020).
4.305 Young women who have been unable to safely parent one child are most at risk of repeating the process. For vulnerable women, the interval between a child being removed and subsequent pregnancies are frequently short. However, co-ordinated planning and support for parents who have a child removed often ceases after removal, unless another child is at risk in the home.
4.306 When parents have complex and challenging needs, support to break the cycle, take control of their lives and develop new skills is essential. Such work is likely to require a holistic approach, in which key workers show persistence, proactivity, understanding, flexibility and work in relationship. Prevention and protection are inseparable concerns in this challenging area of practice.
Resources and References - Preventing repeat removal
Children and young people who are missing
4.307 The Scottish Government National Missing Persons Framework for Scotland describes a missing person as anyone whose whereabouts are unknown and:
- where the circumstances are out of character
- the context suggests the person may be subject to crime
- the person is at risk of harm to themselves or another
4.308 The Framework defines the roles and responsibilities of key partners in relation to prevention, response, support and protection of children and other vulnerable persons whose whereabouts may be unknown and may be regarded as missing.
4.309 In a child protection context 'missing' may cover a wide range of circumstances including:
- children and their families with whom statutory services such as health, education or social work have lost contact, and either the family location is not known, or for whatever reasons there has been no response to attempts to see the child
- children who are not known by or have been hidden from universal services
- children under 16 who have gone 'missing' from home, or under 18 from care, those who have run away, or been abducted either within or across borders
- 'missing' may include those who have been forced to leave their home base, or whose whereabouts are unknown. This may be for a wide range of reasons including injury, abuse outside the home including sexual exploitation, escape from abuse, including honour-based abuse and forced marriage, experience of crime, mental health problems, emotional distress, a lack of understanding or confusion, a wish to be somewhere else doing something else, pressure from others within or beyond the home base, bullying, the need to see another person, or some other compelling reason
4.310 Acting on concerns. If practitioners are concerned that a child or young person is 'missing', they should make every effort to make contact, visit if appropriate, and see that the child is safe and well. Health services may have cause to become concerned when significant appointments are missed without explanation, or missed consistently. This should be followed up. A recording of 'did not attend' is not sufficient. If practitioners are concerned a child may be at risk of harm, police or social work services should be contacted. Consideration should be given to an IRD, if there appears to be risk of significant harm as described in Part 3.
4.311 Child protection concerns may relate to the risk of harm which may have caused a child to go 'missing', risk of harm while a child is missing, potential on-going risks when a child has returned or been returned, or any combination of these dimensions.
4.312 Multi-agency risk assessment and co-ordination is essential for locating the child, considering options, and support. This could extend in cases of immediate urgency, up to the issuing of a Child Rescue Alert, or media alerts through the police when there is a reasonable belief that a child is in imminent danger and there is sufficient information available to enable the public to assist the police in locating the child. If a person or agency suspects that a child has been taken by, or is under the influence of, a third party (which may include parental abduction or 'grooming'), the police must be notified immediately.
4.313 Children on the child protection register. Local protocols will ensure that when a child whose name is on the child protection register goes missing, the appropriate local authority manager (and person accountable for the child protection register if different) should be notified immediately. Co-ordinated efforts should be made to trace the child and assess the circumstances. A Review Child Protection Planning Meeting should be convened. Health and education services should be notified to ensure that the child will be identified if they present at another health or education setting.
4.314 Local Child and Adult Protection Committees should ensure that there are specific and appropriate arrangements in place through guidance, protocols or procedures, which are known and implemented by relevant services. These should include response to children in transitional phases in which they may be at risk of abuse while their whereabouts is unknown or they are missing, and adult services and legislation may also apply.
4.315 Non-attendance and missing during the day. Local authorities should have robust guidance on attendance policy. Included-Engaged-Involved: attendance management guidance (Scottish Government 2019) outlines action in relation to non-attendance at school and when parents / contacts cannot be reached. If a child or young person is absent from school, and the school has not been notified of this absence, then it should be assumed the child is either missing or absent without parental awareness. Efforts should be made to contact parents, and failing this, other emergency contacts. If the school has been unable to establish contact with the parents, action must be taken to satisfy the school and the education authority that the child or young person is safe and well. This information should be contained within the local authorities robust guidance on attendance policy. If the parent cannot be contacted to confirm the whereabouts of the child or young person, the record of absence should be passed to a member of staff with responsibility for attendance (most often a member of the school's senior manager or pastoral care within secondary or home-school link worker where available) to consider the information in the light of known attendance issues, support needs or current concerns about the child or young person. This member of staff will be responsible for determining what further action is required, taking into account the age of the pupil; the implications for additional support to resolve any difficulties; and, if necessary, contacting the school's child protection co-ordinator as it is essential that local child protection procedures are followed. In the case of looked after or vulnerable children, when the child or young person does not attend school this should always be followed up immediately. To enable swift action to be taken it is vitally important that the school has an up to date and accurate record of the key contact information for the parent and social worker where relevant. In the case of children or young people who are looked after at home, then the social worker should also be contacted.
4.316 Children missing from education include those of compulsory school age who are not on a school roll and are not being educated otherwise (at home, privately or subject to any alternative educational provision). It may also include those who have not attended school for a period of time. School staff should be aware of the role of the Children Missing from Education Co-ordinator and work in line with the Children Missing from Education Service Guidance (2022), which contains resources and Children Missing from Education contacts. The Children Missing from Education (Scotland) Service provides guidance and advice on good practice concerning cases of children missing from education, and checks the national Management Information System (SEEMiS) to see if the child has enrolled at another publicly funded school in Scotland. The CME Service facilitates agreements between local authorities, national agencies and partners in England, Wales, Northern Ireland and Ireland to allow exchanges of information, and will support local authorities in using these agreements.
4.317 Unknown to education and home educated. A child may be unknown to services as a result of their removal from their local school, or because they have never been enrolled within an education authority. Where this is the result of a decision being made to home educate this should not, in itself, be regarded as a child protection concern. For further information, see the Government Home Education Guidance. A consultation about this guidance ran until 31 August 2022. The Scottish Government is currently reviewing the responses received ahead of considering refreshed guidance. Where a child leaves an independent school and there is uncertainty over their onward education it is good practice for independent schools to inform the child's education local authority, so as to avoid any child being unaccounted for.
4.318 Children in care settings such as residential or foster care are often reported missing. There were 7,598 Missing Persons Investigations by Police Scotland in relation to looked after and accommodated children in 2017-18. The risk of harm for these children is often increased by their existing vulnerability, and referral to the police may be necessary. However, there may be circumstances in which there is considered to be no risk, or a tolerable level of risk, in relation to a young person; for example, when they fail to return from a known location, and there are no concerns about their wellbeing. To affirm general principles during the COVID-19 pandemic, Scottish Government, Police Scotland and Social Work Scotland issued a Joint statement: Children and young people who go missing from care - Social Work Scotland
4.319 Considering a person 'not at home' rather than missing should only be used where it has previously been agreed that it might be an appropriate response for this child in these circumstances. However, it is necessary to have clear and consistent local inter-agency protocol and definitions. The protocol should outline the approach to prevention planning and risk assessment, a process for return discussions, and follow-up intervention processes to deal with escalating concerns from repeat episodes. 'Prevention' includes consideration of the element of risk, and recommended responses within a child's assessment and plan.
4.320 Partnership agreements. The Pilot National Partnership Agreement for Looked After Children who go missing from Residential and Foster Care in Scotland (CELCIS 2018) indicated that local partnership agreements and regular liaison meetings between Police Scotland and relevant local authority staff can support consistent, safe and effective information sharing and response. The role of the Police Missing Persons Operational Co-ordinator is key within such partnerships.
4.321 Missing families. If health, police, education, local authority social work or the armed forces become concerned that a family has disappeared from a known location, when there are or have been concerns of significant harm for the children or an unborn child, then local multi-agency protocols should encompass:
- the responsibilities of child protection leads in health and education and of key officers, in the local authority, in relation to the tracing of 'missing' children whose names are on the child protection register
- immediate, reasonable and practical efforts that will be undertaken to locate the family
- notifications to social work or police, as appropriate, if health or education services first become aware of this concern
- processes for notification and review of notifications. This includes:
- the NHS Scotland Children Missing from Known Address Form. This documents preparatory work undertaken within the health board area to locate the family. It should be filed within the child's health record or in the mother's record in the case of an unborn baby. A copy of the Missing Family Alert should be sent to all relevant health areas/staff and the practitioner/caseload holder raising the concerns. A copy should be placed in the child/children's health records (or in the mother's record in the case of an unborn baby) and an entry made on the chronology record
- Child Missing from Education alert
- other health or education 'flagging' systems locally agreed to alert services when a child or family re-appears
- process and timescales for co-ordinated review of notifications if a family is not found including inter-agency decision-making on further actions that can be taken
- process for notifications when a family is located (which may include protocol for recording) and follow-up with family concerned as appropriate
4.322 Each agency needs to develop its own policies and protocols to manage risk and track missing children. Local areas should consider a strategic multi-agency collaborative framework, including relevant Third Sector agencies and independent schools, to support individual agency procedures for responding to and tracking missing children.
4.323 Stranger abduction. A child may fail to return because they have been the victim of a crime. Police Scotland will give consideration to the relevance of section 171 of the Children's Hearings (Scotland) Act 2011 (offences related to children absconding from places where they are being kept by virtue of orders by a children's hearing or court or by virtue of a warrant) when there is evidence that a person has assisted them to abscond, concealed them, or prevented them returning. Previous guidance in this section on child sexual exploitation, trafficking, female genital mutilation and forced marriage may be relevant, alongside Part 2b on assessment and contextual safeguarding.
4.324 Missing across borders. When there are concerns about a child who may be at risk of significant harm moving back to their country of origin or elsewhere abroad, it may be necessary to liaise with overseas social work services to ensure that the child has returned, and that their safety is being assessed locally. The relevant embassy or consulate may be able to provide contacts for appropriate authorities. International conventions provide a framework to assist professionals seeking to collaborate with their counterparts in other countries. Local Authorities should use the 1996 Hague Convention on Jurisdiction, Applicable Law, Recognition, Enforcement and Co-operation in Respect of Parental Responsibility and Measures for the Protection of Children for international child protection cases, including those involving EU countries. Local authorities should already use the 1996 Hague Convention for non-EU child protection cases with those countries who have signed up to the Convention. Under the Convention, contracting states can ask each other for information or other types of help when a child's welfare or protection is at issue. The different types of requests include, for example:
- asking for another state's help in tracing a child
- asking for a report on a child habitually resident in another contracting state
- asking another state to take measures to protect a child's welfare
- seeking the agreement of another state for a child to be placed there in foster or residential care
- asking for the transfer of jurisdiction for a child from his/her home state, enabling an authority to make decisions about a child's welfare if it feels it is best placed to do so
4.325 The Convention was implemented by the Parental Responsibility and Measures for the Protection of Children (International Obligations) (Scotland) Regulations 2010 (SSI 2010/213, as amended) and these place duties on local authorities to respond in a timely way to certain types of request. A list of the countries that have implemented the Convention can be found on the Hague Conference for Private International Law website. In this list only those States which have 'entered into force' (EIF) are operating the Convention. Agencies that can offer practical advice, direct services and support on handling cross-border cases include Children and Families Across Borders (CFAB), which has a national advice line on inter-country casework (funded by the Department for Education and Africans Unite Against Child Abuse (AFRUCA).
4.326 Abduction in the context of domestic abuse. In situations where abducting mothers have been fleeing domestic abuse, they may be involved in return proceedings under the 1980 Hague Abduction Convention on the Civil Aspects of Child Abduction. General considerations in this guidance to those facing domestic abuse apply. Mothers are likely to require legal advice and support to ensure that there are protective measures in place for the child's safety and best interests within return arrangements.
4.327 Children and young adults. Part 1 of this Guidance outlines the potential overlap between child protection and the protective duties under the Adult Support and Protection (Scotland) Act 2007 (2021), the Adults with Incapacity (Scotland) Act 2000 and the Mental Health (Care and Treatment) (Scotland) Act 2003.
Resources and References - Children missing
Protecting unaccompanied asylum-seeking and trafficked children
4.328 Article 22 of the UNCRC sets out general requirements on public authorities to take appropriate measures to ensure that a child who is seeking refugee status or who is considered a refugee in accordance with applicable international or domestic law and procedures, whether unaccompanied or accompanied by their parents or any other person, receives appropriate protection and humanitarian assistance.
4.329 An unaccompanied asylum-seeking child (sometimes referred to as a child seeking international protection) is defined in UK immigration rules by the Home Office as a person under 18 years of age when the claim is submitted; applying for asylum in their own right; separated from both parents; and is not being cared for by an adult who in law or by custom has responsibility to do so.
4.330 Unaccompanied asylum-seeking children are the responsibility of the local authority in which they are found and require to be accommodated and supported under section 25 of the Children (Scotland) Act 1995. They are entitled, as any other child, to the full range of supports that can be made available to children under this and associated legislation and provisions. They should be allocated a social worker. They should be supported in accessing the full range of health care and education opportunities available to UK born children. Children who are outside their country of origin and separated from their parents, or legal or customary care giver, are the responsibility of the local authorities, who will assess their needs and offer support.
4.331 Children, variously categorised for reasons beyond their control, are children first, requiring care and protection from abuse and neglect. Whatever the immigration and asylum status of a child, immediate and continuing safety is the priority. As noted above, the UNCRC (Article 22) defines the right of any child seeking refugee status to receive appropriate protection and humanitarian assistance. The status of a child may change (e.g. from 'unaccompanied' to 'accompanied') without necessarily reducing risks.
4.332 Determination of immigration and asylum status is a reserved matter for the UK Government. However, child protection and care in Scotland is the responsibility of statutory services in Scotland. It is not appropriate for social workers to advise on immigration matters. Only those with the relevant qualification can advise if working in organisations regulated by OISC (Office of the Immigration Services Commissioner).
4.333 Refugee status: Decision-making on asylum is reserved to the Home Office. Social workers are not responsible for determining whether a child (in terms of the Refugee Convention 1951 Article 1A) "� has a well-founded fear of being persecuted for reasons of race, religion, nationality, membership of a particular social group or political opinion, is outside the country of his nationality, and is unable or, owing to such fear, is unwilling to avail himself of the protection of that country". Under current UK law, a person accepted as meeting the definition above will be granted Refugee Status and will receive Leave to Remain in the UK for a period of 5 years, after which they can apply for Indefinite Leave to Remain.
Principles essential to protecting unaccompanied children:
- unaccompanied children experience a confusing interaction of systems and rules. Article 3 of UNCRC sets out that: "In all actions concerning children, whether undertaken by public or private social welfare institutions, courts of law, administrative authorities or legislative bodies, the best interests of the child shall be a primary consideration." Necessary actions in relation to protection and care must relate to a child's wellbeing (Article 3.2). This should include consideration of the needs and views of the child. The 'best interests' principle is reflected in section 55 of the Borders, Citizenship and Immigration Act 2009, which places duties on the Secretary of State for the Home Department to ensure that immigration, asylum, nationality and customs functions are discharged having regard to the need to safeguard and promote the welfare of children in the UK (and this is as further reinforced in Home Office statutory guidance to section 55). In Scotland, section 17 of the Children (Scotland) Act 1995 places duties on local authorities in relation to looked after children, including those placed because they have arrived unaccompanied
- the European Convention on Human Rights (ECHR) potentially applies. It was incorporated into UK law by the Human Rights Act 1998 and is also reflected in the Scotland Act 1998. Relevant rights protected under the ECHR include: the right to life (Article 2); rights to respect for private, home and family life (Article 8); physical integrity and safety; freedom from torture, inhuman and degrading treatment (Article 3); protection from trafficking, slavery and forced labour (Article 4). It also includes rights to work, education and freedom of expression (Article 10), and the right not to be discriminated against (Article 14)
- further guidance on children's asylum claims (Home Office 2019) may be found at: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/ attachment_data/file/825735/children_s-asylum-claims-v3.0ext.pdf
4.334 Routes of Arrival. The most common routes of arrival of unaccompanied asylum-seeking children include:
- 'spontaneous' arrivals in local authorities, transport hubs or ports of entry
- transfers through the National Transfer Scheme (NTS), which is provided for through section 69 of the Immigration Act 2016, and allows for the legal transfer of unaccompanied asylum-seeking children from one local authority to another local authority in the UK, on a voluntary basis
- resettlement through the Vulnerable Children's Resettlement Scheme (VCRS) which will shortly be replaced by a new global settlement programme
- family re-unification with eligible sponsors through the existing Immigration Rules which is set out in the guidance an Overview of family reunion options in the Immigration Rules (Home Office, 2020)
4.335 Age assessment. The Human Trafficking and Exploitation (Scotland) Act 2015, section 12, makes provision for a presumption of age in relation to suspected child victims of human trafficking to be given the benefit of the doubt in circumstances of assessing age. If there is uncertainty about a suspected victim's age and reasonable grounds to believe they may be a child (under 18 years of age), a relevant authority such as a health board or a local authority should in exercising various statutory functions assume that the victim is a child (under 18 years of age) for the purpose of providing immediate support and services to the child until their age is formally established.
4.336 In cases where a young person is not necessarily thought to be a victim of trafficking, young people are increasingly being given the benefit of the doubt for the purposes of support during the age assessment process. Whilst this has not been explicitly legislated for, this position is supported by case law as set out in Age Assessment Practice Guidance for Scotland (www.gov.scot).
4.337 Communication and interpreting. Practitioners must be aware of and plan for additional communication support and interpreting needs when disability and/or language difference is a barrier to understanding.
4.338 Protective response is personal. Children in these categories often feel alone and afraid. They need calmness, they need to be listened to and heard. They need acknowledgement, acceptance, respect, honesty, sensitivity and care. First impressions of kindness or coldness have an impact. If a practitioner is accessible, responsive and reliable, this will promote trust and recovery. If the child absconds they need to know they can return.
4.339 Past trauma, persistent feelings of threat and anxiety about asylum decisions (when relevant) significantly impact on children's mental health. Re-telling stories several times (and not just for asylum purposes) is a common source of anxiety for young people. Alongside having a safe space to remember, they may also need encouragement and enough space to forget and form new routines and relationships, and to reconnect or maintain contact with families if safe to do so. For those who have travelled across borders, the strangeness, separations, language differences and confusing systems all combine to add to experiences which can be frightening, unsettling and re-traumatising.
Resources and References - Unaccompanied asylum-seeking and trafficked children
Child trafficking and child criminal exploitation
4.340 Article 35 of the UNCRC requires public authorities to take all appropriate measures to prevent the abduction of, the sale of or traffick in children for any purpose or in any form; and Article 36 requires public authorities to protect the child against all other forms of exploitation prejudicial to any aspects of the child's welfare.
4.341 Definition. The legal definition of the offence of human trafficking in Scotland is set out in the Human Trafficking and Exploitation (Scotland) Act 2015 ('the 2015 Act'). A person commits an offence of human trafficking if a 'relevant action' is taken with a view to another person being exploited (section 1). The offence of human trafficking is aggravated by being committed against a child (as defined in the 2015 Act as a person under the age of 18 years old) (section 6).
4.342 Relevant action. Section 1(2) of the 2015 Act defines 'relevant action' as any of the following: recruiting another person; transporting or transferring another person; harbouring or receiving another person; exchanging or transferring control over another person; or arranging or facilitating any of those actions. It is irrelevant whether the person consents to any part of the action. Travel between two places is not a requirement for an offence of human trafficking to have taken place.
4.343 Exploitation. The 2015 Act (section 3) describes what constitutes exploitation for the purposes of the offence of human trafficking. The following are examples of exploitation:
- prostitution and sexual exploitation
- criminal exploitation
- slavery, servitude and forced or compulsory labour
- securing services and benefits
- financial exploitation/benefit fraud
- removal of organs
- debt bondage
- begging
4.344 Child trafficking and exploitation is abuse, and an immediate child protection response is required, and an inter-agency referral discussion (IRD) must be undertaken when there is reason to believe a child may have been trafficked or exploited.
4.345 Awareness and recognition. A child may not realise, divulge or agree that they have been trafficked or exploited. The child may be:
- at risk of being moved, especially when inquiries begin
- threatened with personal or family harm if they speak out
- unaware that they are a victim of trafficking
4.346 Trafficking occurs both within Scotland and between Scotland and other countries. UK children can be the victims of trafficking. It is estimated that around 40% of unaccompanied children have experienced trafficking and exploitation. Current figures for the National Referral Mechanism (which is a UK-wide process for identifying and referring potential victims of trafficking and ensuring they receive the appropriate support) for England and Wales indicate that the highest number of referrals are for UK children who have been internally trafficked. The number of referrals from Scotland for UK children is lower but is growing.
4.347 Incidence. Trafficking is a largely hidden crime. It can be difficult to identify victims. Statistics are uncertain and incomplete. The numbers of children referred to the NRM across the UK has risen annually since 2009, and in 2016-20 the number of children referred has increased significantly, partly due to referrals of UK national children in relation to child sexual exploitation and child criminal exploitation (CCE). In Scotland, between 2012-20 the majority of children known to have been trafficked have been from South East Asia (particularly Vietnam), East Asia, Africa and Eastern Europe. Across the UK as a whole, UK nationals accounted for the largest number of children known to have been trafficked in 2020.
Child criminal exploitation (CCE)
4.348 CCE is a cause of significant harm and should trigger child protection processes and consideration of relevant preventative action. CCE is not defined in law but practitioners should be alert to the possibility that some children who are victims of trafficking may be exploited by gangs and organised criminal networks. CCE can be associated with 'county lines', which refers to criminal exploitation by gangs which export illegal drugs into one or more areas (within the UK). Gangs may use dedicated mobile phone lines or other form of 'deal line'. Such gangs are known to exploit children and vulnerable adults to move (and store) drugs and money and often use coercion, intimidation, violence (including sexual violence) and weapons. However CCE can also occur in the absence of these features.
4.349 Practitioner Guidance on Criminal Exploitation (2023) has been published to support a shared understanding of criminal exploitation of children and adults, and to help assist with early identification of those at risk. The guidance has been developed by a subgroup of the Serious Organised Crime Taskforce; however, it equally applies to child criminal exploitation which is not linked to serious organised crime.
4.350 Child criminal exploitation takes a variety of different forms and affects both male and female children. It can include children being forced to work in cannabis factories, being coerced into moving drugs or money across the country, forced to shoplift or pickpocket, or forced to threaten other young people. Any child being forced or coerced to commit crime must be seen as a victim of exploitation.
4.351 Child criminal exploitation is often unrecognised and this can mean children are more likely to be prosecuted for offending behaviour, rather than being recognised as victims of exploitation. Children may fear arrest and prosecution. They may be drawn in to CCE through other children.
4.352 It is critical for professionals to be aware of indicators of trafficking and exploitation, and to take appropriate safeguarding and procedural steps. A prosecution against someone who has committed a criminal act as a result of being trafficked or exploited would in some circumstances be contrary to obligations imposed by national law. Section 8 of the Human Trafficking and Exploitation (Scotland) Act 2015 requires the Lord Advocate to publish instructions about the prosecution of persons who are, or appear to be, victims of an offence of human trafficking. The Lord Advocate's instructions for Prosecutors when considering Prosecution of Victims of Human Trafficking and Exploitation provide that there is "a strong presumption against prosecution" of a child victim of human trafficking or exploitation who has committed an offence in the course of, or as a consequence of, being the victim of human trafficking or exploitation. Too often children are criminalised rather than seen as victims of criminal exploitation and given the appropriate child protection response.
4.353 Being aware of the indicators and risks that may suggest children and young people are being exploited and abused in such a manner is the initial step that professionals need to take. Then, considering how this is being facilitated, by whom, and for what purpose, may evidence there is child criminal exploitation occurring, which should inform the agencies involved and the approach to be taken to protect and intervene.
4.354 Contextual safeguarding needs to be considered in managing the risks posed to and from the child and other children who may be involved. A traditional focus on child and family and which does not consider the relevance of wider relationships and the location of harm, may not suffice in managing presenting behaviours or reducing contextual risks.
4.355 'Cuckooing'. Practitioners should also be alert to reports which may indicate someone's home has been taken over by intimidation or other means for the purpose of criminal activities. Signs of 'cuckooing' might include reports of:
- bags of clothing or bedding around the address
- increased visitors throughout the day or night
- increased vehicles outside the address, including taxis, new vehicles and hire cars
- increased anti-social behaviour in the area
- disengagement with support services
- drug paraphernalia around the address, and the smell of drugs such as cannabis
- barricades within and around the address, including weapons
Initial assessment and response to trafficking and exploitation
4.356 An assessment should always be comprehensive and follow GIRFEC principles. There are no risk-assessment tools that can predict the risk of trafficking or definitively identify those who have been trafficked. However, an indicator matrix has been developed to assist the recognition of such abuse both within the UK and across borders. The indicators complement and do not replace child protection procedures. Indicators in use across the UK reflect those applied in international texts and trafficking practice handbooks (IOM 2009; UNODC 2018 and Operational Indicators of trafficking in human beings, 2009) and in identification of child sexual exploitation (Hynes 2015).
4.357 If an agency or practitioner has concerns that a child may have been trafficked they should consult the indicator matrix and should always:
- contact social work or Police Scotland but not contact carers initially or seek their consent
- follow inter-agency child protection procedures
- an inter-agency referral discussion must follow
4.358 National Referral Mechanism (NRM). The UK has a responsibility to identify and record cases of child trafficking under the Council of Europe Convention on Action Against Trafficking in Human Beings. The NRM was set up by the Home Office to help victims of trafficking receive support, and to gather intelligence to help interrupt trafficking. Any child suspected of being a victim of trafficking should be referred to the NRM. In Scotland referral to the NRM should follow on from an IRD and Child Protection processes. Only designated 'first responders' can make a referral into the NRM For children, local authorities and police (in addition to the Home Office) are the first responders. Referral to the NRM is made online (National Referral Mechanism Toolkit for First Responders in Scotland).
Guardianship Scotland
4.359 Guardianship Scotland is a statutory service that provides a Guardian to unaccompanied asylum-seeking and trafficked children and young people in Scotland. The Guardians provide assistance and support in navigating the complex welfare, care, immigration, asylum and trafficking systems, often in a foreign language. The Guardian can advocate for children in engaging with the various authorities, and can speak on the child's behalf to avoid the need for them to re-live their experiences through constant re-telling of their story to different authorities. International research has shown that unaccompanied and trafficked children benefit enormously from guardianship arrangements.
4.360 Guardianship Scotland replaced a previous voluntary service called Scottish Guardianship Service on 1 April 2023. Local authorities are required through section 11 of the Human Trafficking and Exploitation (Scotland) Act 2015 (legislation.gov.uk) to refer eligible young people to Guardianship Scotland as soon as reasonably practicable. Guidance on how Guardianship Scotland operates is due to be published in Summer 2023.
Effective response to child trafficking and exploitation depends on a child protection response
4.361 Protocols, developed though Child Protection Committees, should emphasise the following matters:
- central and immediate focus on the child's safety, health and wellbeing
- practitioner awareness of indicators of potential abuse across agencies
- provision of a guardian for eligible children
- inter-agency systems that support identification and recording
- sufficient awareness of legal framework within core agencies
- prompt inter-agency referral discussion and response
- referral to the NRM following Scottish Child Protection processes (including IRD)
- consideration of the use of interpreters
- consideration of support needs of children who may be traumatised
- prevention and disruption of trafficking
- rigorous prosecution of offenders
- provision of assistance and support for victims
- protecting victims' rights in criminal proceedings
4.362 The Human Trafficking and Exploitation (Scotland) Act 2015 (Part 4) makes provision for Trafficking and Exploitation Prevention Orders (TEPOs), and Trafficking and Exploitation Risk Orders (TEROs). TEPOs can impose prohibitions or requirements on those who have committed a trafficking or exploitation offence, or who may commit such an offence, as well as those who in certain circumstances were acquitted of such an offence or who were found to be unfit for trial. TEROs may be imposed in respect of adults where there is a risk that the adult may commit a relevant trafficking or exploitation offence. TEPOs and TEROS could impose prohibitions or in relation to Scotland or elsewhere and could include other prohibitions e.g. on foreign travel.
Resources and References - Trafficking and CCE
Protection in transitional phases
4.363 Meaning. A significant trauma, loss or change in a child's care, core relationships and services may have a ripple effect, not only for the child, but also for those to whom they feel closest. This interaction informs effective assessment and planning of support during phases in which there may be heightened risks, as well as opportunities for growth.
4.364 Examples of transitional risks and opportunities:
- children who have been impacted by abuse or neglect, who are now moving onto adult life and services
- children who are impacted by parental health problems, or by drug and alcohol problems, and are now moving onto adult life and services
- disabled children and young people with complex needs who are moving onto adult life and services. They and their families often experience a sequence of service changes and loss of known professional supports within an age band during which their fundamental health and wellbeing needs may change little
- children moving between care placements or moving on from family-based, residential or secure care arrangements. Some of the most emotionally isolated and risky transitional phases may occur several years after the movement between or out of these settings
- parents who have lost a child involuntarily through statutory processes. There may be phases of heightened risk and opportunity to engage following such removal. Disengagement by and from services may increase the risk of repeat removal(s)
- children in transitional phases who are isolated, separated by the imprisonment of or otherwise removed from those to whom they feel closest, and whose help they need
- children in transitional phases within families who find services inaccessible or incomprehensible
4.365 Anticipation and prevention. In and of themselves, such phases do not trigger 'child protection' or 'adult protection' processes. There may be trigger points or critical moments when a child is excluded, isolated, hurt or afraid, when proactive support can make a long-term difference. Early collaborative planning and sufficient co-ordination and continuity of support are key to effective support through predictable transitions. This Guidance advocates an approach that is rights-based, has a focus on relationships, and seeks to build on resilience. Some areas have developed Young Person Support and Protection Protocols which raise awareness and signpost appropriate processes for children and young adults across a range of concerns, when there is a pattern of escalating concerns.
4.366 Signposts in this Guidance. The legal interface between child and adult protection processes are outlined in Part 1 of this Guidance, under the definitions of 'child' and 'principles in child protection'. In Part 2 the interface between child and adult protection is considered in relation to roles and responsibilities. The components of assessment and planning in Part 2B invite consideration of transitional needs. In relation to specific areas of risk, practitioners should apply evaluated and locally approved frameworks in the use of which they are trained and supervised.
Resources and References - Transitional phases
Bullying
4.367 The paragraphs below should be read alongside sections of overlapping relevance in this part of the Guidance, including child protection in the digital environment, hate crime, and seriously harmful behaviours and harmful sexual behaviours by children.
4.368 Meaning. In Scotland there is no single legal definition of 'bullying'. 'Respect for All: National approach to anti-bullying' provides the framework for anti-bullying work in Scotland and defines bullying as "both behaviour and impact: the impact is on a person's capacity to feel in control of themselves. Bullying takes place in the context of relationships; it is behaviour that can make people feel hurt, threatened, frightened and left out. This behaviour happens face-to-face and online." (Respect for All, 2017). Although the actual behaviour may not be repeated, the threat may be sustained over time, typically by actions, looks, messages, confrontations, physical interventions or the fear of these.
4.369 Bullying can occur between children and young people, and between adults and children. Online bullying should not be treated differently from face-to-face bullying. Bullying behaviour may be motivated by prejudice due to perceived or actual differences. This may lead to racism, sexism, homophobia, biphobia or transphobia, or prejudice and discrimination towards disability or faith (see section on hate crime).
4.370 Online bullying (sometimes called 'cyber-bullying') is technology-assisted. It can involve the circulation or sharing of rumours, messages, gaming and images. Bullying can cause significant and sustained harm and requires agency policies and protocols that are holistic, preventative, proactive and supportive. Bullying of any kind must be addressed quickly whenever it arises.
4.371 'Peer-on-peer abuse' may be used to refer to any form of physical, sexual, emotional and financial abuse, and coercive control, exercised between children and within children's relationships (both intimate and non-intimate). The term 'peer-on-peer' can obscure significant age and power differences.
Protective and preventative responses
4.372 An anti-bullying policy is a clear commitment to develop a respectful, equitable and inclusive culture and ethos within an organisation or establishment. Anti-bullying policies should be developed in partnership with children and young people, parents and carers, and staff, including volunteers.
4.373 The Recording and monitoring of bullying incidents in schools: supplementary guidance was published to support schools and local authorities. All schools are expected to be recording and monitoring bullying incidents using the new uniform approach that was introduced in schools in 2019.
4.374 Support should seek to prevent the 'criminalising' of children and young people wherever possible. However, adults and children and young people can seek appropriate advice from Police Scotland if they feel a crime may have taken place.
4.375 Consideration should be given to the context in which bullying has occurred. References to contextual safeguarding in Part 2B and below may be of relevance. There is a range of relationship-based approaches that can improve relationships and behaviour, promote equality and challenge inequality, and develop emotional wellbeing to help prevent and address bullying which includes restorative approaches, solution-oriented approaches, nurturing approaches, mentoring and peer support.
4.376 Education and social work services will consider triggering an IRD when there is a risk of significant harm to a child from bullying or peer-on-peer abuse. Referral to the Reporter will be considered when there is an apparent need for compulsory measures. When a crime is reported, the police will investigate, respond and consider the need for an inter-agency referral discussion under child protection procedures as defined in Part 3.
Resources and References - Bullying
Hate crime
4.377 The paragraphs below should be read alongside sections in this Part of the Guidance concerning child protection in the digital environment, bullying and harmful behaviours by children.
4.378 Definition. Hate crime is the term used to describe behaviour which is both criminal and rooted in prejudice. Hate crime can be verbal or physical and can be online or face-to-face. It has hugely damaging effects on the victims, their families and communities. Current hate crime legislation in Scotland allows any existing offence to be aggravated by prejudice in respect of one or more of the protected characteristics of race, religion, disability, sexual orientation and transgender identity. Prejudice or hostility also lies at the heart of some other offences which are recognised as hate crimes. These include racially aggravated harassment and stirring up of racial hatred. Once commenced, the Hate Crime and Public Order (Scotland) Act 2021 (passed by Parliament in March 2021) will consolidate, modernise and extend hate crime legislation in Scotland. It will add age as an additional characteristic and create new offences relating to stirring up hatred in relation to all characteristics protected under the Act.
4.379 Impact. The effects of hate crime can be emotional or physical and may impact on children's sense of security, identity and emotional wellbeing. Children who are victims of hate crime may experience high levels of anxiety, difficulty sleeping and potentially, suicidal feelings.
4.380 Prevention. Prejudice is learned from a young age. Therefore, children who have caused harm may not understand the consequences of their behaviour or the harm caused. There are many initiatives within Scottish schools to address prejudice-based bullying and hate crime (EHRC, 2017). It is likely to be an important facet of preventative, educational and rehabilitative action that offenders are given an opportunity to understand what a hate crime is and the impact that it has on individuals, families and communities.
4.381 Response. Support should seek to prevent the criminalising of children and young people wherever possible, unless in the public interest. However, adults, children and young people can seek appropriate advice from Police Scotland if they feel a crime may have taken place. Age of Criminal Responsibility (ACRA) legislation can be utilised by Police Scotland if appropriate.
4.382 Anyone who has experienced or witnessed a hate crime should be encouraged to report it directly to the police, a trusted adult or by using a third-party reporting centre. Third-party reporting allows victims and witnesses to report an incident without contacting the police directly. There are third-party reporting centres across Scotland, ranging from housing associations to victim support offices and voluntary groups, where specially trained staff provide support and assistance in submitting a report to the police. Find your nearest Third Party Reporting Centre. Police response will include the consideration of the need for an inter-agency referral discussion, taking in to account the impact, circumstances and protective and support needs of those involved.
4.383 Hate crime is often not reported to the police. Tackling under-reporting of hate crime and initiatives to deter people from committing hate crime remain key priorities for the Scottish Government, Police Scotland and COPFS.
Resources and References - Hate crime
Serious harmful behaviour shown by children above and below the age of criminal responsibility
4.384 Serious harmful behaviour in this context means behaving in a violent or dangerous way which causes or risks causing serious physical harm to another person, or sexually violent or sexually coercive behaviour, which has caused or risks causing harm (whether physical or not) to another person. (Please refer to section 15 above for further information about response to sexually harmful behaviour by children.) The revised Framework for Risk Assessment Management and Evaluation (FRAME) for children aged 12-17 (CYCJ 2021) details 'risk of serious harm' and standards of practice for this age group. Consideration must be given not only to the to the impact of threat and physical or psychological trauma caused; but also to the level of intent, use of force or coercion, and potential as well as actual harm.
4.385 Children that behave in this way may themselves have been abused or neglected. Whether or not they have been maltreated, they are likely to have additional needs relating to their behaviour or the impact of their behaviour. While the police and statutory services will take action to protect the safety of those involved in the situation and attend to the needs of victims, all investigative and planning activity triggered by a child's harmful behaviour must have regard for the child's wellbeing as a primary consideration.
4.386 As a result of the Age of Criminal Responsibility (Scotland) Act 2019, which fully commenced on 17 December 2021, a child under the age of 12 years is no longer able to commit and offence in Scotland. In practice this will mean that, whilst Police Scotland still have a duty to investigate and record any crime, a child under the age of 12 cannot be held criminally responsible for their actions. Operational Guidance has been published, and Ministerial Guidance was published in 2021 on Places of Safety and Investigative Interviews. The age of criminal responsibility is currently being reviewed to see what needs to be in place if the age is raised.
4.387 The 2019 Act provides police powers for immediate and planned investigation of seriously harmful behaviour. The 2019 Act also includes provision (section 28) for police response to a situation in which a child is behaving in a way that is causing or risks causing immediate significant harm to another person, by removing a child to a place of safety, types of which are defined by the 2019 Act (section 28(5)); and a list of which must be maintained in consultation with police and social work. A child can only be taken to a police station for these purposes if a police inspector (or above) considers that it is not reasonably practicable to keep the child in another type of place of safety. In each situation the most appropriate arrangements will be made in co-ordination with the local authority. Statutory Guidance on the use of a Place of Safety was published in 2021.
4.388 General principles underpinning all investigative and planning processes are summarised in Part 3 of this Guidance. If child protection concerns arise in relation to the child who has behaved harmfully to others then standard components of IRD processes apply. IRD components specific to the requirements of the 2019 Act will be set out in guidance being developed in relation to that Act. The immediacy of risk of harm to the child or children involved will determine the steps and prioritisation of steps taken.
4.389 If a formal investigative interview is required under chapter 3 of the terms of Part 4 of the 2019 Act, a legally qualified and approved Child Interview Rights Practitioner must be involved, for the purposes of protecting the rights of the child. A code of practice guidance has been developed that sets out the national standards of practice that apply to all Child Interview Rights Practitioners.
4.390 Discovering what happened in harmful circumstances is dependent upon trauma-informed, child-centred processes. This includes communication and co-ordination with those who care about and have responsibilities towards the child and other children closely affected.
4.391 The Principal Reporter can no longer refer a child to a children's hearing on offence grounds, where the offence took place when the child was under 12 years of age. As explained above, a child under the age of 12 years will no longer be able to commit an offence in Scotland. However, the Principal Reporter can refer a child to a children's hearing on non-offence grounds that may include reference to any serious harmful behaviour by the child.
4.392 If it appears that behaviours observed or reported fall short of risking or causing 'serious harm', the local processes for proportionate, co-ordinated 'Early and Effective Intervention' will apply within the Whole Systems Approach adopted in most areas. GIRFEC and Early and Effective Intervention aim to prevent children entering into formal systems if compulsory measures are not needed.
4.393 The Framework for Risk Assessment Management and Evaluation (FRAME) with children aged 12-17 sets out standards for children involved with offending behaviour as distinct from adults who offend. Effective practice requires joined-up planning at operational, tactical and strategic levels between criminal justice, adult protection, child protection and childcare services.
4.394 If it appears that a young person 12-17 is responsible for seriously harmful acts, local Care and Risk Management (CARM) processes apply. For details on the CARM process, see section 2 in the FRAME guidance. Although children of this age may be charged with an offence, the investigative and planning principles that are summarised in Part 3 of this Guidance apply.
4.395 Alleged offences of a serious nature involving children aged 12 or over can be referred to the Procurator Fiscal. Children aged 12 or over can be prosecuted; however, the offences must fall within the category of offences outlined within the Lord Advocates Guidelines to the Chief Constable on the Reporting of Offences to the Procurator Fiscal of Offences Alleged to Have Been Committed by Children.
Category 1: offences which require by law to be prosecuted on indictment or which are so serious as normally to give rise to solemn proceedings on the instructions of the Lord Advocate in the public interest.
Category 2: offences alleged to have been committed by children aged 15 years or over which in the event of conviction oblige or permit a court to order disqualification from driving.
Category 3: offences alleged to have been committed by people who are aged 16 or 17, and who are classified as children by section 199 of the Children's Hearings (Scotland) Act 2011.
4.396 Children aged 12 or over who are referred to the Procurator Fiscal are also referred to the Children's Reporter, and the Procurator Fiscal makes a decision whether the child can be dealt with in the children's hearing system or whether the case will be dealt with by the Procurator Fiscal after discussing the child with the Children's Reporter.
4.397 Children aged 16 or 17 who are subject to Compulsory Supervision Orders through the children's hearings system can continue to be managed in this system or can be prosecuted. This decision is made by the Procurator Fiscal following discussion with the Children's Reporter. Where criminal proceedings are initiated, the court can, upon conviction, choose to remit the child back to the children's hearings system for disposal under section 49 of the Criminal Procedure (Scotland) Act 1995.
4.398 Where a child aged 12 or over is referred to a children's hearing on the ground that they have committed an offence, in any resulting proof proceedings in the Sheriff Court the standard of proof is the same as the test that applies in criminal proceedings: beyond reasonable doubt.
4.399 The Scottish Government has consulted (2020) on raising the age at which a young person can be referred to a children's hearing from 16 to 18.
4.400 The Principal Reporter will consider other factors as well as the sufficiency of evidence relating to the grounds when deciding whether to call a hearing. The child's development, parenting and family and environmental factors are taken into account alongside the history of co-operation with any previous intervention; the impact of any previous intervention; the current motivation to change; and the willingness to co-operate with any intervention. Where a child is not referred to a children's hearing, the Principal Reporter may refer the child back to the local authority for them to work with the child on a voluntary basis, or may take no further action. A fundamental principle of the children's hearings system is that the hearing will consider the individual circumstances of each child, and should not make orders in respect of the child, such as Compulsory Supervision Orders, unless to do so is better for the child.
4.401 Article 40 of the UNCRC relates to the rights of children who have behaved unlawfully. In general terms public authorities are expected to provide a range of disposals such as supervision orders, care, counselling, education, training and support, to ensure that each child is dealt with in a manner appropriate to his/her wellbeing and proportionate both to his/her circumstances and relevant behaviour (see in particular Article 40(4)).
Resources and References - Serious harmful behaviour by children
Vulnerability to being drawn into terrorism
4.402 The Counter Terrorism and Security Act 2015 (section 26) places a duty on specified authorities in Scotland such as local authorities to have due regard to the need to prevent people from being drawn into terrorism. It also places an obligation on local authorities to ensure that a panel of persons is in place for its area to assess the extent to which identified individuals are vulnerable to being drawn into terrorism and, where appropriate, arrange for support to be provided. Revised HM Government Guidance (2021) is available for Scotland (Prevent Multi-Agency Panel Duty Guidance: Protecting people vulnerable to being drawn into terrorism (publishing.service.gov.uk). When assessing referrals to such panels, local authorities and their partners should consider how best to align such assessments with child protection legislation and guidance.
Resources and References - Vulnerability to being drawn into terrorism
Complex investigations
4.403 'Complex investigations' refers to a multi-agency response when there is reasonable concern about abuse involving one or more abusers and a number of related or non-related abused children or young people. The abusers concerned may be acting in an organised way to abuse children. Some such individuals and networks act in isolation. Others may use an institutional framework or position of authority to groom and abuse children. Guidance may be found above in the section concerning the response to child trafficking.
4.404 The nature of 'complexity' may be affected by environment in which abuse occurs. This may be an institution, establishment, club, group, internet-based, or a combination of scenes or locations.
4.405 Additional complexity may also relate to the length of time between the abuse and the report, or due to the extended period of time over which abuse may have occurred.
4.406 'Institutional abuse' is a term which may be used to encompass abuse in an institutional setting which may include non-accidental injury, sexual abuse, neglect in delivery of care and supervision, emotional abuse, or a combination of these.
4.407 'Ritual abuse' refers to the use of strategies, beliefs and ideologies that legitimise sexual and other forms of exploitation to both victims and perpetrators of organised abuse. Ritual abuse is sometimes associated with other organised abuse, including child sexual exploitation. Some victims may have experienced neglect and abuse both at home, and organised abuse in other settings. Vulnerability in one context can contribute to victimisation in another.
4.408 Child abuse linked to beliefs in witchcraft, spirit possession and other forms of the supernatural can lead to children being scapegoated and abused physically, sexually and emotionally. Fear of the supernatural is also known to be used to make children comply with being trafficked for domestic slavery or sexual exploitation. Such abuse is not confined to one faith, nationality or ethnic community. The number of known cases suggests that only a small minority of people who believe in witchcraft or spirit possession go on to abuse children. Abuse may happen at home or in another setting.
4.409 Survivors of organised and ritual abuse may only be able to report their experience many years later, with awareness often arising through 'flashback' memories. Survivor recovery may be further complicated if there has been involvement of family members, they have been made to recruit other victims, engage in abusive behaviour of others, or engage in the use and production of pornography. The imposition of beliefs and ideologies justifying the behaviour or the abusers may complicate investigation, support and recovery of those survivors who have been made to feel both shame and complicity.
4.410 Considerations in planning interviews. Where a child has been involved in pornography and filmed or become accustomed to their image being manipulated, recording of interviews may be particularly alarming. Local inter-agency child protection procedures should include contingency plans to deal with such cases.
4.411 Scope. Complex investigations may extend beyond the boundaries of individual services. The extent of concerns about abuse may not at first be apparent. When the factors above emerge, detailed planning is advised at strategic as well as at operational level. The purpose of such planning is to ensure a consistency of approach and clear areas of accountability, to scope investigations and the potential for these to grow, and to give initial consideration to options available. Standard IRD processes as described in Part 3 of this Guidance should underpin such planning.
4.412 A strategic management group will normally: establish the terms of reference of the investigation; provide strategic leadership for the investigation; agree the staffing of the investigation; agree such protocols as may be necessary.
4.413 Police and social work services should agree arrangements for convening planning meetings, setting up systems for sharing and updating information about the investigations progress, and co-ordinating support. All relevant agencies and services should be involved in these discussions.
4.414 Chief Officers should be alerted in such circumstances, including where the concerns involve a child or children outside the area. Senior managers from social work services and the police should ensure that arrangements for the investigation of linked cases are in place, so that children and adults are adequately protected.
4.415 When cases involve several children and adults in different households, it will be in the interests of the criminal investigation to prevent suspects from communicating with each other and destroying evidence. This will require careful co-ordination of investigations, interviews, and other assessments.
4.416 If a number of families, parents and carers are involved, the local authority should make clear arrangements to keep them informed of events and plans. Parents/carers are usually entitled to the fullest possible information. If it is unclear how many families are involved, decisions regarding information-sharing will be particularly complex. Agencies may need to restrict information provided to families and the public to avoid prejudicing criminal enquiries. This should be considered in the planning process. Parental involvement may need to be limited in order to safeguard the child. The reasons for this must be recorded.
4.417 Early involvement of the Procurator Fiscal and the Principal Reporter will be necessary. Police and social work services should agree a media and public communication strategy.
4.418 Specialist skills. The investigation of complex child abuse requires an investigating team with appropriate expertise. A teamwork approach is essential. It may be necessary to involve agencies which are trusted by the child or other witnesses. Specialist advice and support may be required from agencies with particular knowledge of the issues.
4.419 Systemic issues. Where there is evidence of institutional abuse, operational and strategic analysis should consider not only the responsibility of individuals, but also the contribution of culture, belief and systems within those institutions, organisations or communities which carried out the abuse. Common features include the isolation of victims and the privacy which may provide individuals with opportunity for the exploitation of power.
4.420 Partnership across areas. In anticipation of strategic and operational partnership that may be required from time to time, lead agencies should consider establishing links with neighbouring authorities and agencies to ensure access to necessary resources - including skilled staff and specific facilities such as interview suites - when dealing with complex multiple or organised abuse cases. Inter-agency procedures should reflect local arrangements to provide support, de-briefing or counselling for practitioners as necessary. For further information on supporting child witnesses, see the section on criminal prosecutions.
Resources and References - Complex investigations
Female genital mutilation
4.421 Article 24.(3) of the UNCRC requires public authorities to take all effective and appropriate measures with a view to abolishing traditional practices prejudicial to the health of children.
4.422 Female genital mutilation (FGM) is child abuse. This traditional practice is an extreme form of gender-based abuse, causing significant and lifelong physical and emotional harm. Cultural considerations and sensitivities should not override the need of professionals to take action to protect a child at risk.
4.423 Definition. The legal definition of FGM is to excise, infibulate or otherwise mutilate the whole, or any part, of the labia majora, labia minora, prepuce of the clitoris, clitoris or vagina (section 1 of the Prohibition of Female Genital Mutilation (Scotland) Act 2005). The World Health Organization defines four types of FGM. However, it should be noted that the term FGM is often not recognised by FGM-practising communities, and practitioners should use terms such as cutting or female circumcision instead.
4.424 Occurrence. FGM may be a risk from infancy through to adulthood, as the practice can take place in infancy, childhood and also before marriage. Disabled children may also be subjected to the practice. A girl or woman might be subjected to FGM more than once throughout her life. A girl or woman may be taken out of the country by her family in order for the procedure to be carried out.
4.425 Criminal offence. FGM has been illegal in Scotland since 1985. The Prohibition of Female Genital Mutilation (Scotland) Act 2005 made it a criminal offence to have FGM carried out either in Scotland or outside the United Kingdom. The Act also increased the maximum sentence on conviction on indictment from 5 to 14 years imprisonment (section 5 of the 2005 Act). The UK Parliament's Serious Crime Act 2015 (section 70) extends the reach of extra-territorial offences in that Act to habitual (as well as permanent) UK residents. The Female Genital Mutilation (Protection and Guidance) (Scotland) Act 2020 makes provision for FGM Protection orders and for Statutory Guidance on FGM. These provisions will strengthen the existing legislative framework for the protection of women and girls from FGM.
4.426 Psychological impact. FGM can be imposed by families that are in other ways protective. By contrast it may be associated with other forms of gender-based violence and so called 'honour-based' abuse, which can include child and forced marriage. Sometimes FGM can be linked to trafficking. Children affected by FGM experience lifelong psychological trauma.
4.427 Physical impact. FGM procedures cause severe pain, emotional and physical shock. Complications can cause death. Effects can include haemorrhage, wound infections, urinary retention, injury to adjacent tissues, fracture or dislocation as a result of restraint, and damage to other organs. Long-term health consequences include: chronic vaginal and pelvic infections; difficulties during menstruation; difficulties in passing urine and chronic urine infections; renal impairment and possible renal failure; damage to reproductive system (including infertility); infibulation cysts; neuromas; keloid scar formation; complications in pregnancy; delay in the second stage of child birth; maternal or foetal death; and increased risk of sexually transmitted infections. Surgical interventions during pregnancy and childbirth may be required.
4.428 Emotional impact. Immediate and long-term emotional impact is further complicated because the decision is usually made by those who are respected, loved and trusted. Adult survivors who experienced FGM as children have reported losing trust in those who forced them to undergo the procedure. Others experience family conflict and/or separation, especially in families when parental attitudes are divided. Women may experience recurrent sexual, psychological and physiological problems. FGM may also cause severe post-traumatic stress and can be associated with subsequent drug and alcohol problems, although this is less likely in cultures where drug and alcohol use is considered 'shameful'.
4.429 Awareness and response. FGM or the risk of FGM may first come to the attention of education or health professionals. A child can be considered at risk if they come from an FGM-practising community or if a close female relative is a survivor of FGM regardless of whether the community of origin traditionally practises FGM. A strong indicator could be the planning of an extended family holiday.
4.430 Every situation should be considered individually, rather than making automatic assumptions about levels of risk within specific communities.
4.431 Other child protection concerns may or may not co-exist. It is relevant to know if the family is from a community in which FGM is practised; if the girl's mother has experienced FGM; if the girl has a female sibling/cousin who has experienced FGM; and if it is known that the family is as yet not well integrated. Practitioners should be aware that attitudes within the same family may vary. Some women who have experienced FGM are opposed to their daughters undergoing it. Experience of coercive control and the size of the family/extended family/wider community may limit the protective capacity of some parents. Consideration should be given to how to give mothers safe and private space in which to talk. As with other forms of child protection work, there should be efforts to engage and seek a shared understanding in partnership with parents/carers, unless there are safety considerations. Survivors of FGM should be given the opportunity to speak with female practitioners.
4.432 Co-ordinated response: When it is believed that FGM has been carried out upon a child or when there is cause to believe it may occur, this should trigger an IRD, as outlined in Part 3. Schools may be in a good position to pick up on signs of a girl being at risk. A strategy discussion may be advised in order to consider the whole situation and tailor the engagement, investigation and support process likely to be in the child's best interests. The plan should take into account that other female siblings or close relatives may also be at risk.
4.433 Practice considerations: A multi-agency approach is required. National multi-agency guidance (Scottish Government, 2017, revision due 2023) provides indicators of good practice. Wherever possible, female practitioners are recommended for planned assessment. Practitioners will be sensitive to the time and privacy needed by those expressing concerns. Clear and simple language should be used. Those involved also need a clear understanding of the role of practitioners. Some children will not understand what has happened or what may happen. Care should be exercised in the use of interpreters and lay advisors from the same local community as the victim. (The Scottish Translation, Interpretation and Communication Forum Good Practice Guidelines, 2004).
4.434 Strengthening the law: As part of the National Action Plan to Prevent and Eradicate FGM (Scottish Government (2016), the Female Genital Mutilation (Protection and Guidance) (Scotland) Act 2020 was recently enacted. In reviewing local guidance, agencies will need to take into account the new Act's requirements. These include FGM Protection Orders and Statutory Guidance.
Resources and References - Female Genital Mutilation
Honour-based abuse and forced marriage
4.435 Article 24(3) of the UNCRC requires public authorities to take all effective and appropriate measures with a view to abolishing traditional practices prejudicial to the health of children.
4.436 A forced marriage is a marriage conducted without the full and free consent of both parties, and where duress is a factor. Duress can include physical, psychological, financial, sexual and emotional abuse. A forced marriage is different from an 'arranged marriage'. An arranged marriage is one in which the families of both spouses are primarily responsible for choosing a marriage partner for their child or relative, but the final decision as to whether or not to accept the arrangement lies with the potential spouses: both spouses give their full and free consent. The tradition of arranged marriage has operated successfully within many communities for generations.
4.437 Forced marriage is both a child protection and adult protection matter. Child protection processes will be considered up to the age of 18. Forced marriage may be a risk alongside other forms of so called 'honour-based' abuse (HBA).
4.438 HBA includes practices used to control behaviour within families, communities, or other social groups, to protect perceived cultural and religious beliefs and/or 'honour'. Such abuse can occur, for example, when perpetrators perceive that a relative has shamed or may potentially shame the family and/or community by breaking their honour code. This abuse can take many forms, including threatening behaviour, emotional blackmail, assault, rape, abduction, forced marriage, confinement and 'honour killing'.
4.439 Perceived transgressions which may trigger HBA include: supposedly 'inappropriate' makeup or dress; having a boyfriend/girlfriend; forming a relationship with someone of a different faith; showing same-sex attraction or having a same-sex relationship; kissing or intimacy in a public place; pregnancy outside marriage; and rejecting or seeking to escape from a forced/arranged marriage. Particularly for women, seeking a divorce (regardless of the reasons behind this) is extremely stigmatised and can lead to ostracism and honour abuse.
4.440 Children at risk. Those who might identify as LGBT and disabled children may be at increased risk of forced marriage. For LGBT people this is seen as a way of ensuring that their LGBT identity is not made public. Forced marriages are also seen as a way of ensuring that someone who needs care has a spouse who can provide this care. Furthermore, immigration can be an aggravating factor towards forced marriage: by arranging a marriage of a UK citizen with someone from overseas, the overseas spouse is guaranteed an easier entry into the UK. An estimated 80% of forced marriage victims are girls and women. HBA support work is mainly conducted by women's organisations. However, boys, especially those who might identify as gay, bi-sexual or transgender are also affected by forced marriage, domestic abuse, coercive control and other forms of HBA. Practitioners should be aware that forced marriage is not restricted to any particular ethnic or religious community.
4.441 Legal framework. Forced marriage legislation should be used in conjunction with child and adult protection legislation. In Scotland, a couple cannot be legally married unless both parties are at least 16 on the day of the wedding, and are capable of understanding the nature of a marriage ceremony and of consenting to the marriage. Parental consent is not required. The Forced Marriage etc. (Protection and Jurisdiction) (Scotland) Act 2011 introduced civil remedies for those at risk of forced marriage, and those who have already been forced into marriage. It introduced a civil Forced Marriage Protection Order (FMPO), which can be used to protect those at risk; it is a criminal offence to breach a FMPO. To extend protection for those at risk, section 122 of the Anti-Social Behaviour, Crime and Policing Act 2014 makes forced marriage an offence in Scotland.
4.442 The consequences of forced marriage can be devastating for the whole family, but especially to the young people affected. They may become estranged from their families and wider communities, lose out on educational opportunities, or become victims of domestic abuse. Rates of suicide and self-harm within forced marriages are high.
4.443 Potential indicators of honour-based abuse and forced marriages include:
- concerns voiced by child or person in child's network about going overseas 'to visit relatives' or attend a wedding
- concerns expressed about a dowry being collected (usually jewellery, clothing, other material possessions)
- a girl undergoing or at risk of undergoing FGM as part of her 'preparation' for the marriage
4.444 Education concerns:
- absence, or persistent absence, from education
- request for extended leave of absence and failure to return from visits of country of origin
- decline in behaviour, engagement, performance or punctuality
- being withdrawn from school by those with parental responsibility
- being prevented from attending extra-curricular activities
- being prevented from going onto further/higher education
- sudden changes in appearance or behaviour (especially young girls changing their dress code dramatically to adopt culturally/religiously appropriate clothing)
4.445 Health concerns:
- self-harm
- attempted suicide
- depression
- eating disorders
- accompanied to doctors or clinics and prevented from speaking to health practitioners in confidence
- experience of female genital mutilation (FGM)
4.446 Police concerns:
- reports of domestic abuse, harassment or breaches of the peace at the family home
- threats to kill and attempts to kill or harm the potential victim or another family member (emotional blackmail)
- truancy or persistent absence from school
4.447 Approach. Direct engagement with the family is not advised, as it may aggravate and expedite the risk of a child being taken abroad for a marriage. It is always advisable to contact a specialist organisation or community advisor for support.
4.448 Practitioners involved in this work should have sufficient training and supervision to support application of the required knowledge and skills. Scottish Government national guidance is under revision (due 2023).
Resources and References - Honour-based abuse and forced marriage
Fabricated or induced illness
4.449 Definition. Fabricated or induced illness refers to a process in which a parent or caregiver induces illness or a sick role in a child by exaggeration, deliberate non-treatment, fabrication or falsification of signs of illness. The process can include maladministration of medication or other substances causing symptoms of illness, and interference with equipment, observation charts or other documents relevant to the child's health. The caregiver may or may not genuinely believe the child to be ill.
4.450 Impact on the child can include actual physical harm, potential trauma, anxiety and confusion during multiple and sometimes invasive treatments and investigations, as well as social and emotional impairment of a child's development, identity and relationships.
4.451 Occurrence. Proven incidence is rare. It is more frequent in young children. A common feature is that the caregiver reports symptoms or signs, and health assessments cannot account for these signs. It can be a feature that symptoms are not seen by anyone other than the caregiver, that new symptoms are reported by the caregiver when one form of concern is resolved, or that multiple medical opinions are sought inappropriately.
4.452 Response. Where concerns do exist about the fabrication or induction of illness in a child, practitioners must work together in co-ordination, considering all the available evidence, in order to reach an understanding of the most probable reasons for the child's signs and symptoms of illnesses. Careful medical evaluation is always required to consider a range of possible diagnoses, including the possibility that some older children may present with fabricated symptoms, again requiring careful assessment, understanding and supportive response in relation to whatever the causes may be.
4.453 An inter-agency referral discussion will be necessary when risk of significant harm from abuse or neglect is identified as described in Part 3 of this Guidance. An IRD should be held in order to consider timing and responsibilities when co-ordinated investigation, planning and action are required, step by step, to ensure the child's physical and emotional safety and support. A chronology will be an essential feature within such a multi-agency assessment.
4.454 All agencies and practitioners should be aware of the potential indicators of illness being fabricated or induced in a child, and be alert to the risk of harm that individual abusers, or potential abusers, may pose to children in whom illness is being fabricated or induced. Practitioners must work together to form a multi-agency assessment and plan. Work should be in collaboration with parents/caregivers unless to do so would place the child at increased risk of harm. In any criminal or civil proceedings, practitioners must be prepared to give evidence as required.
4.455 Note : the Royal College of Paediatrics and Child Health (RCPCH) and the British Association of Social Workers (BASW) have both published resources to support practitioners in relation to fabricated and induced illness:
- Perplexing Presentations (PP)/Fabricated or Induced Illness (FII) in Children Guidance (RCPCH, 2021)
- Fabricated and Induced Illness Practice Guide (BASW, 2022)
4.456 RCPCH and BASW are working together with a view to developing multi-disciplinary guidance. The implications for multi-agency child protection in Scotland are under review. This subsection will then be revised as necessary.
Resources and References - Fabricated and induced illness
Death of a child
Sudden unexpected death in infants and children
4.457 For a very small number of children, their death may not be as a result of natural causes. In cases of sudden death the circumstances and cause of death must be explored sensitively and to the highest standards. Every parent has a right to understand fully the circumstances which led to the sudden unexpected death of their child.
Definitions:
4.458 An unexpected death of a child is defined as the death of an infant or child (under 18 years old):
- which was not anticipated as a significant possibility, for example due to an already diagnosed illness or health condition, 24 hours before the death; or
- where there was an unexpected collapse or incident leading to or precipitating the events which lead to the death
4.459 Sudden unexplained death in childhood (SUDC) is the death of a child which remains unexplained after a thorough investigation.
4.460 Sudden unexpected death in infancy (SUDI) is deemed to have occurred when there is no known pre-existing condition which would make the death predictable. If death of an infant is directly attributed to abuse or neglect, this would not be classed as a SUDI.
4.461 All infant deaths which happen suddenly, and for which there is no apparent reason, are unexpected. From the outset, all such cases are unknown or unascertained. The police have a leading role in the investigation of sudden and unexpected infant and child deaths. When the death of a child or infant is reported to the police, a Child Death Senior Investigating Officer (Child Death SIO) will always be appointed to oversee the investigation, whether or not there are any obvious suspicious circumstances. Since the cause of death is not at first known, a death certificate cannot be issued.
4.462 All sudden and unexplained child deaths must be reported to the Crown Office and Procurator Fiscal Service (COPFS). Police Scotland is responsible for investigating and reporting the circumstances of the child's death to COPFS. The police may also be tasked by COPFS to undertake investigations into the death of a child which has been reported by health professionals. Investigations, which include toxicology from post-mortem examination, may take several months. If, at any stage during a child death investigation, abuse or neglect is or suspected to be a significant or contributory factor in the death, then the police investigation will be tailored accordingly.
4.463 A collaborative and co-ordinated inter-agency approach is necessary in situations of a sudden or unexplained death of a child or infant. Alongside the child death investigation exists a responsibility for ensuring the safety and wellbeing of any other children or infants in the household or yet to be born that may be affected (Article 6 UNCRC). When there are surviving siblings, an inter-agency referral discussion will be considered in all cases and is the recommended mechanism to ensure early, multi-agency and co-ordinated decision making. This will enable appropriate single-agency or multi-agency support, assistance and intervention for families where this is required or provide assurance that no further action is necessary.
4.464 A Child Death SIO may consider engaging officers for specialist tasks, such as: interviewing child witnesses; obtaining relevant and necessary background information from police, local authority, health, parent/carers and anyone else who may have relevant information. In cases where the child or infant and their family were either not resident in or had recently moved to the area where the death occurred, the Child Death SIO will ensure that information is sought from local policing divisions/police forces and local authorities in any area where the child or infant is known to have previously resided.
4.465 In all situations a range of professionals are involved when a SUDI occurs. Not all professions will be involved in every SUDI. The interacting roles of professionals are outlined within Healthcare Improvement Scotland's Toolkit (https://www.sudiscotland.org.uk/professional- guidance/). In all situations, the sensitivity, skill and co-ordination of an inter-agency approach will significantly influence family experience within effective investigations. Investigations may form a helpful step within support for bereaved parents and relatives of the child or infant.
4.466 Once the Procurator Fiscal is satisfied that there is no criminality involved, permission is given for a SUDI review to take place. This is organised by health boards and will involve relevant inter-agency professionals and the family. The purpose of this review is to discuss all aspects of the death, including possible causes or contributing factors to see what lessons can be learned and to plan support for the family, particularly in identifying support needs for any future pregnancies.
Paediatric End of Life Care Network (PELiCaN)
4.467 The Paediatric End of Life Care Network was established in April 2019 with the aim of supporting delivery and improving access to high quality, patient and family centred, end of life care for children and young people; regardless of age, ethnicity or geographical location. The PELiCan Network mission is to ensure that any baby, child or young person who dies in Scotland has access to 'gold standard' end of life care from the point it is acknowledged that they are entering the end of life stage of their diagnosis. https://www.pelican.scot.nhs.uk/about-us
4.468 In relation to Police Scotland investigations of child death, Police Scotland has worked in partnership with PELiCaN to develop a sensitive approach when responding to an expected death in the community of a child or young person (hereon referred to as a child and defined as "a person under 18 years of age") with a life limiting condition. The approach ensures attending officers and the appointed Child Death Senior Investigating Officer (SIO) are fully aware of the unique circumstances, so that a proportionate and sensitive approach to the investigation is provided. When a child with a life limiting condition chooses to die at home (or at least out with a hospital or hospice) then an End of Life Care Plan is created by the child along with their doctor and family. This plan is officially known as 'Children and Young People Acute Deterioration Management' (CYPADM).
4.469 Once in place, PELiCaN notify Police Scotland and a marker is placed on the relevant address, highlighting there is a child residing at the address who is receiving end of life care. The notification sent by PELiCaN will also provide the following details:
- the nature of the life limiting condition
- if a Do Not Resuscitate (DNR) or Do Not Attempt CPR (DNACPR) order is in place
- the name of a medical professional who can provide further information and who will grant a death certificate (if no further Police investigation is required) It should be noted that a DNR/DNACPR notification is one which has been agreed with the parents and in some cases the child themselves. It instructs health care providers not to provide lifesaving treatment like CPR if a child's breathing or heart stops. The family will have a copy of the CYPADM. The presence of a PELiCaN marker on the relevant address does not negate Police attendance when receiving the report of the death of the child. It simply means that the child's death was anticipated or expected. The requirement for Police to establish the circumstances of the death and rule out criminality remains, however, the presence of the marker allows a proportionate and sensitive response to the family. The Scottish Ambulance Service is also notified of the End of Life Care Plan for the child by PELiCaN
National Child Death Review Process
4.470 A National Hub for Reviewing and Learning from the Deaths of Children and Young People has been set up by Scottish Government. It is hosted by Healthcare Improvement Scotland and the Care Inspectorate. Reviews will be conducted on the deaths of all live-born children up to the date of their 18th birthday, or 26th birthday for care leavers who are in receipt of aftercare or continuing care at the time of their death. The aim is to ensure that the death of every child in Scotland is subject to a quality review and that there is a consistent approach and coordinated process to learning from all local review activity. Data generated will inform national policy, education and learning and contribute to the prevention of child deaths in the future.
4.471 When a Health Board or local authority is notified about the death of a child or young person there should be clear governance arrangements and processes in place to determine the appropriate review mechanism. Engagement must take place early in the process with any other organisations involved in the child or young person's care to reach a decision about the most suitable review process. All organisations and agencies involved should work together to undertake one single review wherever this is possible and appropriate. The rationale for deciding which review process should be carried out should be clear, take into consideration any statutory, legal, or national requirements, and be reached in a timely manner.
4.472 The National Hub Guidance sets out the implementation processes for health boards and local authority areas when responding to, and reviewing, the death of a child or young person. Whilst organisations can establish their own structure and process for reviewing the deaths of children and young people, they should ensure the local processes align to this.
4.473 As with all inter-agency assessment and action, a sensitive, collaborative, respectful approach is essential at every stage, with sharp attention to the necessary sharing of information and preservation of evidence. All inter-agency professionals should ensure that the family involved in the process are treated sensitively. Scottish Government have provided funding to develop National Bereavement Care Pathways (NBCP) for five types of baby loss including the sudden unexpected death of an infant. Chief Officers will ensure that staff have access to appropriate support during any investigations, particularly if the circumstances of the case lead to a Learning Review.
Resources and References - death of a child
Community
4.474 Article 2 of the UNCRC requires that each child's rights are protected without discrimination of any kind, irrespective of the child's or his or her parent's or legal guardian's race, colour, sex, language, religion, political or other opinion, national, ethnic or social origin, property, disability, birth or other status. While child protection must be non-discriminatory it should also be sensitive to the significance of context, culture and community in each situation.
4.475 The sections that follow indicate considerations in relation to 'community'. The term community is used in a broad sense to encompass not only relationships that are connected to place, but also those that arise out of shared beliefs and values or common goals. Although this Guidance promotes consistent components of good practice across Scotland, effective child protection will require respect for distinctive elements of communities that influence not only the ecology of the child's world, but also, potentially, the ecology of professional judgement - for example in a small rural community in which personal and professional boundaries may intersect more frequently.
Cultural and faith communities
4.476 All faith organisations and cultural communities in Scotland share a commitment to the safety and protection of children.
4.477 Increasing diversity. Scotland's population of 5,438,100 (2018) is increasingly diverse in culture, faith and language. After English, Polish, Urdu, Scots, Punjabi and Arabic are most frequently spoken. In 2017, 158 languages were spoken as the main home language by pupils in publicly funded schools. The 2011 census asked those living in Scotland to state their religious affiliations. 32% said Church of Scotland; 37% said no religion; 16% said Roman Catholic; 1.4% said Islam; and around 0.1% said each of Buddhism, Sikhism, Judaism, and Hinduism.
4.478 Cultural sensitivity and competence. Cultural respect must be a consistent thread through child care and protection. Competence in an unfamiliar cultural context may entail consultation about specific culture and/or faith by which the child and family live their daily life. It will involve development awareness of services that provide advocacy, advice and support attuned to culture and faith.
4.479 Children's safety first. Working across differences in culture and faith can influence professional response in child protection processes. For example, fear of being thought racist and unsympathetic can lead to professional inaction (Lord Laming, 2003; Victoria Climbie Inquiry; para 16.7).
4.480 The best protection is prevention. For faith communities and organisations, clear, written and well-shared child protection and vulnerable adult policies and procedures are a first step to creating awareness and safety within the organisation/community. Volunteers, employees and those in positions of authority and pastoral responsibility need support in how they can recognise abuse; how they should respond to allegations or concerns about abuse; how they should record concerns and make appropriate referrals; and what behaviour towards children is acceptable and unacceptable within their role.
4.481 Fundamental preventative steps for faith organisations include: safe recruitment practices; safe practice in pastoral support with children and young people; online safety advice for appropriate use of digital and social media; child protection training for staff and volunteers; awareness raising within the faith community, for instance in relation to grooming processes; and the name and contact details for someone to speak to about any concerns.
4.482 Faith organisations should have designated child protection leads who have a role in passing on concerns about children to police or social work, and in developing and maintaining organisational policies and procedures. These individuals should undertake regular training and be aware of the local Child Protection Committee and procedures. Faith organisations have a role in promoting awareness of information, resources and helplines in relation to child protection and, for example, forced marriage and honour-based abuse.
4.483 Resilience. Faith and spirituality can be a powerful resilience factor when children and families benefit from associated community, guidance, hope and meaning, particularly in the context of feelings of isolation and insecurity. Faith and faith organisations can be a source of resilience and hope, particularly when communities face threat, loss and disaster.
4.484 Abuse of trust. Positions of power, trust and authority can provide opportunities to abuse. Gender-based oppression, coercion and control or family honour may be a feature in dynamics that keep abuse secret.
4.485 Families facing exceptional stress. Practitioners will be aware that, even when supported by faith and community, many migrating families and their children face exceptional stress, due to immigration status, poverty and accommodation concerns. They may experience feelings of isolation, separation, alienation, anxiety, disappointment, frustration and confusion.
4.486 Disabled children may be more vulnerable to victimisation and scapegoating in some cultural settings. They are likely to be less able to resist or share their experience. There is a collective responsibility to be alert, to challenge inappropriate behaviour, avoid collusion and report apparently harmful behaviour to statutory services. Response must be carefully planned, with victims' experience and safety a central consideration.
4.487 Experience of statutory services. Statutory services will seek to ensure children's hearings and child protection processes respond equally well in all areas and communities. Recent research highlights challenges for ethnic minority families in contact with the children's hearings (Henderson et al 2017). These challenges include: isolation; language difference; poor translation; concerns about confidentiality; family reluctance to raise concerns and accept support; lack of awareness of services and how the law operates in Scotland; and fear of service intervention.
4.488 Interpreting. When interpreting services are required, planning of investigative processes will take extra time and care. The Scottish Refugee Council, in partnership with five local authorities, has developed guidance which includes use of interpreters (2019). Practical headlines may be summarised:
- develop interpreting and translation policy and procedures
- train practitioners in work with interpreters
- never use friends/family members as interpreters in a formal context
- never place responsibility for interpreting for parents upon children
- offer people the option to request an interpreter of the same (or a different) gender for their appointments
- brief and de-brief interpreters on expectations, procedures and remit
- recognise that service providers have a duty of care to all parties
- note that interpreters may need support after distressing interpreting sessions
4.489 Child abuse linked to faith and belief. There may be tensions between a parent's beliefs and Scottish laws, for instance, in relation to physical chastisement. Where specific practices linked to tradition, faith or belief are harmful or used to justify behaviour that is abusive, then services must not hesitate to engage in order to understand and prevent further harm. Female genital mutilation is an example of a traditional practice which is a criminal offence in Scotland and will be treated as child abuse.
4.490 Practitioners may need additional training in order to work with child abuse linked to faith or belief. It can be advantageous when statutory and faith-based communities engage in dialogue in order to build trust, co-produce policy and share good practice.
Resources and References - Cultural and faith communities
Children and families in the defence community
4.491 There are nearly 10,500 men and women in the Regular Armed Forces and 4,000 Ministry of Defence (MOD) civilians from across the UK and beyond working in Scotland. This does not include reservists - a significant and connected network of personnel and families with feet in both civilian and service life. They and their families make a vital contribution to national and international security, and they are a vital social force within the Scottish economy and local communities.
4.492 There are communities that exist 'within' communities. For example, services, bases, units and regiments have networks and identities of their own. While service families may experience the full range of risks and concerns apparent in the civilian population, the resilience of and pressures upon service children and families can have a distinctive dynamic. Children may have experienced many changes of school.
4.493 Practitioners should seek to understand how this cultural context plays a part in the experience of each child and their family if a child protection concern arises. Parental or sibling deployment (and return home) can have an impact on children's mental health. British service personnel and veterans' health can be affected by pre-deployment stress, post-traumatic stress and re-integration stress following deployment or transition from service.
4.494 Increased parental stress is a natural feature for the parent who remains at home. Many service parents are very young when faced with these pressures and can feel isolated, despite a supportive service structure and community. As in some other community and institutional settings, it is possible for problems to remain hidden until a point of crisis.
4.495 When a child protection concern arises, generic processes apply as outlined in Part 3. However, there is an additional need to ensure the interfaces between the Ministry of Defence (MOD) and local authorities work effectively.
4.496 The Armed Forces Families & Safeguarding (AFFS) is responsible for providing the professional leadership and direction across the MOD for the development and implementation of safeguarding policy and practice. The Safeguarding Policy Team (SPT) as part of AFFS consists of experienced safeguarding professionals who provide subject matter expertise and guidance across the MOD and to safeguarding partners.
4.497 The SPT can act as a conduit between the MOD and the local authority for sharing information. If a local authority requires input from the MOD in relation to a child protection concern or have been informed of an allegation against a serving person of a safeguarding nature they are encouraged to notify the SPT at People-AFFS-Safeguarding-Mailbox@mod.gov.uk to promote timely information sharing.
4.498 The MOD have published a Joint Service Publications Directive and Guidance on Safeguarding. It is intended as a comprehensive framework for the safeguarding of all People in Defence: JSP_834_Part_1_V5.2_Nov_2021.pdf (publishing.service.gov.uk); JSP_834_Part_2_V5.2_Nov_2021.pdf (publishing.service.gov.uk)
Resources and References - Defence Community
Child protection in the context of disasters and public emergencies
4.499 Meaning. 'Child protection in disasters and emergencies' encompasses the prevention of and responses to abuse, neglect, exploitation, and violence against children in times of emergency, whether caused by natural or man-made disasters, conflicts, or other exceptional crises that threaten to overwhelm essential structures. The COVID-19 pandemic was a public emergency. Child protection in this and similar contexts must address all forms of physical and psychological abuse, sexual and gender-based violence, armed conflict, and deprivation of basic needs.
4.500 Relevance. Child protection following disasters is a matter of ethical and practical relevance in prevention, preparation, emergency responses and provision of subsequent assessments, planning, and diverse forms of support for children. For example:
- disasters in various forms have occurred in recent memory in Scotland due to terrorism (Lockerbie and Glasgow airport), mass shooting of children (Dunblane), and industrial disasters (Piper Alpha)
- we have children reaching the UK or seeking to do so, who have become more vulnerable when they and their families have had to leave their homes to seek sanctuary overseas due to disasters. Children and their families experience unanticipated loss and separation, trauma, exhaustion and confusion. They face multi-dimensional risks and insecurities during these transitions, but also have skills and strengths that those intervening should extend and support (The section above on unaccompanied and trafficked children may be relevant in this context , as will the People arriving from Ukraine - risk and need: public protection guidance.)
- a minority of those providing aid and others targeting 'lone' children in disaster contexts may behave abusively
- beyond immediate impact, the process of adjustment to disasters may be an invisible, long-term and cyclical process for children, families, practitioners and volunteers, becoming an ingredient in other crises and vulnerabilities
- strengthening children's (families', kin's and communities') capacities to cope with future disasters is a critical preventative function for protecting children
4.501 Legal basis for response to national disasters. Emergency legislation may be necessary in response to public emergencies, as has been the case during the COVID-19 pandemic. In relation to events of national impact in Scotland, the Civil Contingencies Act 2004 and the Civil Contingencies Act 2004 (Contingency Planning) (Scotland) Regulations 2005 (as amended) outline the immediate responsibilities of key organisations and their duty to prepare for civil emergencies within Scotland. The balance of activity and interaction between Scottish Ministers and the UK Government will depend on the nature of the incident.
4.502 Organisational response. The scale and nature of the emergency will determine the scope of organisational response. The COVID-19 pandemic required national and international response. In Scotland, central and local adaptations have had to be rapid, comprehensive and consistent in order to control infection, sustain essential services and protect those most vulnerable. Supplementary guidance on child protection was published by Scottish Government alongside other essential guidance. When emergencies are of a more local nature, Scottish Government have set out principles of emergency response in Scotland in Preparing Scotland: Scottish Guidance on Resilience. Responder organisations must come together through Regional Resilience Partnerships (North of Scotland, East of Scotland and West of Scotland) and will provide such strategic support for multi-agency planning as may be necessary.
4.503 Protective practice with children and families. A child safeguarding lens is necessary in prevention, preparedness, immediate relief, recovery and reconstruction. The COVID-19 pandemic heightened some risks in relation to coercive control, domestic and online abuse and as a result of suspension or reduction in direct contact with services. Conversely, support, relationship and essential decision-making have been sustained through a creative blend of technology assisted communication and essential direct contact within public health protection guidelines.
4.504 Gender, age, ethnicity, disability, sexual orientation, culture including language, religion, and economic status are all factors that should be considered in relation to risk and recovery. Assessment and development of plans to protect and support children, families and communities should (as with all areas of practice within this Guidance), be co-ordinated as necessary and formed together with those involved, including children, their families, communities and local child protection agencies.
Resources and References - Disasters and public emergencies
Historical (non-recent) reports of abuse
4.505 Definition. The term 'historical abuse', often referred to as non-recent abuse, refers to reports of neglect, emotional, physical and sexual abuse which took place before the victim was 16 (or 18, in particular circumstances) and which have been made after a significant time lapse. The complainant may be an adult, but could be a young person making reports of abuse in earlier childhood. The reports may relate to a person's experience in the family home, community or while they were a looked after and accommodated child in a residential, kinship or foster care setting.
4.506 Coming forward. A person may share an account of historical abuse in the context of a therapeutic or counselling setting, within the statutory or Third Sector. Others may report historical abuse directly to the police, social work services, health or education. It is possible that the person reporting historical abuse may not be a direct service user but a parent/carer, partner or other family member of a person accessing these services. People reporting historical abuse may state that the perpetrator is deceased, suggesting that there are no current child protection concerns. However, they may still want to be advised that they can share information with Police Scotland to make a report to allow them to consider information further (Adult Survivors of Child Abuse, Police Scotland).
4.507 Professional response. Any reasonable professional concern that a child may be at significant risk of harm will always override a professional or agency requirement to keep information confidential. All service providers have a responsibility to act to make sure that a child whose safety or welfare may be at risk is protected from harm. Service users should always be made aware of the circumstances when confidentiality needs to be breached, preferably during the initial stages of contact with a service.
4.508 When a report of historical child abuse is received by any agency, consideration needs to be given to the investigation of any current child protection concerns. This should include determining whether there are any children potentially still at risk from the suspected perpetrator(s). This may be in a professional capacity such as in a residential or foster care setting, within a personal family setting in the wider community, within other institutional settings, or a combination.
4.509 A person sharing their experience of abuse may be unable or unwilling to go to the police. Consideration should be given as to whether the person requires support and protection as an adult at risk of harm. Their needs must be balanced against the need to protect any child/children who might currently be exposed to risk from the suspected perpetrator(s). Where possible, there should be an agreement between agencies to allow individual support plans to be put in place.
4.510 Services supporting or taking part in investigations relating to persons reporting historical abuse should be mindful of potential barriers to making a report. As with other disclosures of abuse these may include a fear of not being believed, and uncertainty about how investigations will proceed. Feelings of distrust or suspicion may also arise, particularly if the abuse has happened within a care setting.
4.511 Referral of concerns about historical abuse to Police Scotland or social work will lead to consideration of an IRD in accord with Part 3 of this Guidance. A planned and co-ordinated approach should balance current child protection risks with support for the person. A trauma-informed approach is necessary in the planning and investigation of abusive experiences. Where investigations into reports of historical abuse suggest that the reported abuse was part of a wider organised network or involved multiple abusers, agencies should follow this guidance. For further information, see the section on complex child abuse investigations above.
4.512 Access to records. Investigation of reports of historical abuse will entail accessing relevant records. For example it may become necessary to access information from local authorities and relevant agencies in relation to former staff and carers. Local guidelines should include clear protocols on record-keeping and record management, including record retrieval, which could be for the purpose of assisting complex investigations.
4.513 Redress. Scottish Government has progressed a package of reparations for survivors of abuse in care in the context of the Action Plan on Justice for Victims of Historic Child Abuse (2014) and the SHRC Human Rights Framework for Justice and Remedies for Historic Child Abuse (2010). This includes a statutory financial redress scheme under the Redress for Survivors (Historical Child Abuse in Care) (Scotland) Act 2021, which provides an alternative to court action for those abused in care to receive acknowledgment, redress payment, and apology. Scotland's Redress Scheme became operational in December 2021. The scheme will remain open for whichever is the longer of five years from opening, or two years following the publication of the Scottish Child Abuse Inquiry's final report. For further information and guidance on eligibility and how to apply to Scotland's Redress Scheme, see https://www.gov.scot/collections/financial-redress-for-survivors-of-child-abuse-in-care/
Further support and information
People reporting historical abuse should be offered on-going emotional support. Local guidelines should set out referral routes to local services that specialise in childhood abuse and trauma and may be able to offer immediate helpline support, including:
National support initiatives
- Future Pathways Scotland's In care survivor support fund - Future Pathways is the Scottish Government-funded national support service for adult survivors of childhood abuse whilst in care
- The Survivors of Childhood Abuse Support Fund (2020-2024) is a new fund which will commence in April 2024 which is aimed at Third Sector and community-based organisations who support adult survivors of childhood abuse
Further information
- The Scottish Child Abuse Inquiry in to the abuse of children in care (up to age 18) is on-going, with investigations in to allegations of historical abuse of children in care, including children in foster care and residential schools. The Inquiry will report to Ministers upon recommended changes in policy, law and practice
- Social Work Scotland co-ordinate a national Historical Abuse Practice Network for staff involved in improving practice in relation to historical abuse
Child protection themes
The themes that have been recurrent in this Guidance may be summarised as follows:
1. Attention to the child's needs, rights, voice and experience is fundamental. This requires recognition of risk of harm to a child; risk of harm to others from a child; and recognition of the context in which such risks occur.
2. Recognition and engagement with family entails attention to the needs, strengths, perspective and experience of those family members who are key to the child's safety and wellbeing.
3. Information sharing that is protective must be relevant, proportionate, accurate, timely, necessary, and lawful.
4. Multi-disciplinary assessment of risk and strength should be structured and formed in collaboration between professionals, child and family. It should include analysis of what needs to change to prevent harm to the child, through the consideration of the interaction of factors that may help or hinder change.
5. Co-ordinated and collaborative planning requires agreed steps, expectations, responsibilities, outcomes, supports and timescales. Strength-based approaches may assist in bringing professionals and family together in shared objectives.
6. Practical help that is responsive to need also involves qualities in professional relationship, including reliability, honesty, respect, care, accessibility and encouragement.
7. Workforce: effective child protection depends on sufficient training in core knowledge, skills and values applicable to role, the supervision, support and leadership that sustains ethical practice, and a learning culture that integrates learning from mistakes.
Contact
Email: child_protection@gov.scot