The experiences of people who sell or exchange sex and their interaction with support services: lived experience engagement
This research informs our commitment to develop a model for Scotland which effectively tackles and challenges men’s demand for prostitution. It seeks to map service provision in Scotland, and gathers lived experience input on service experiences.
4 Lived Experience Findings: Accessing Services
The following section presents the findings from the lived experience engagement around accessing services.
4.1 Routes into Specialist Services
This section draws on survey data shared by people with lived experience both during the facilitated survey, and by interview participants, to explore the routes into specialist services, the methods of access used, and key challenges and barriers to access.
Participants who were engaged with a specialist service were asked how they first connected with this service. The responses are summarised in Figure 8.
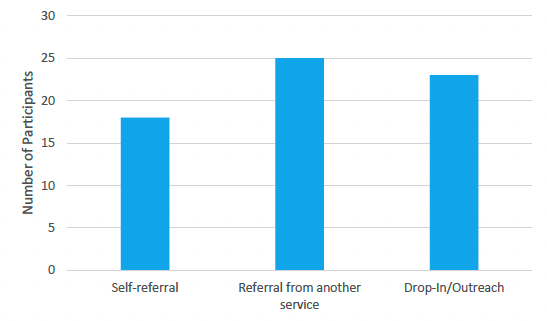
The data indicates that options for all three referral routes (self-referral, referral from another service and drop-in/outreach), are important to facilitate service access, as a number of participants had used each specified route into specialist services. Of the 66 participants who had accessed specialist services, the largest group reported that they had been referred to specialist services through mainstream services (n=25). This highlights the importance of clear referral pathways from mainstream services and ensuring that there is a strong knowledge of the available specialist service provision for people who sell or exchange sex within mainstream services. Reflecting the findings of the mapping survey, these results highlight the potential benefits of joined up or partnership working in connecting people with specialist support in this area. The benefits of improvements in onwards referrals are particularly striking when viewed alongside the previously presented data suggesting both that mainstream services are often unaware of the specialist services available in their area (see section 3.2.1) and also that people who sell or exchange sex are often reluctant to disclose their involvement to these services (see section 3.3.1). It is notable that despite these limitations this still represents the most common route in to specialist services amongst this sample. Improvements in knowledge of mainstream services and referral routes could be expected to result in easier access for many more people into specialist support.
Outreach or drop-in services were the second most common route-in to specialist services (n=23). Of those who chose to specify the type of outreach which had allowed them to engage with services, the majority had been approached whilst selling or exchanging sex on the street, or in saunas. One participant had been contacted proactively through her profile on the Adultwork website. These findings highlight the importance of proactive outreach as an element of service delivery.
Self-referral (n=18) was the route-in for the remaining participants who had engaged with specialist services. Of those who had self-referred, three participants noted that they had been referred into services with the support, or on the recommendation of a family member or friend. Participants were given the option to specify 'other' but no additional methods of referral were identified from the responses.
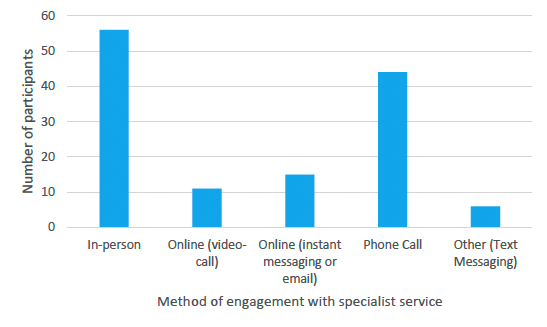
Participants who had engaged with specialist services were additionally asked to select all the relevant methods by which they engage with this support service, with the option of selecting as many as they used. The results are displayed in Figure 9. This information is particularly relevant in light of the Covid-19 pandemic and associated restrictions to give a sense of how specialist support is being delivered across Scotland. The most common methods were in-person (n=56) and phone call (n=44). Substantially fewer chose to engage online, with video calling being the least popular online option. Participants had the option of also selecting 'other' to specify another method of engagement. Of these, 2 participants flagged up in-person activities here and have been categorised under in-person, and 6 shared that they engaged using text messaging. Many participants engaged in a number of ways, for example in-person with appointment reminders by text message. These results indicate the benefit of providing a range of options for people to engage with specialist services, as all methods were used by a number of participants. Amongst this sample, face-to-face support remains an important element of support provision.
The adoption of technology such as video calling, was discussed further in relation to accessing both mainstream and specialist services, and the restrictions in place during the Covid-19 pandemic. The key themes are summarised here. For the majority of those who were already engaging with regular support, this was not interrupted by a move to remote engagement. Overall, participants spoke positively about their experiences with support during the pandemic, and the majority of this was attributed to the ways in which technology was utilised and embraced.
Participants said:
'We turned all my face-to-face sessions into video sessions and carried on. The pandemic really fed into my anxiety disorder and my worker helped me work through that and gain extra support and confidence' [FS7]
'I call or text my worker and she gets back to me quickly. My worker provided me with a phone, internet and laptop to engage with services during Covid' [FS40]
During the pandemic, the availability of remote options was essential for support to continue. For many participants, the increased use of technology was a positive, and they had continued to prefer remote method of engaging once restrictions lifted. For those relying on translation services, accessing support using the telephone was particularly convenient. One participant said:
'I can contact my caseworker by text or call and she will call me back very quickly with an interpreter' [FS37]
Some participants who had begun engaging with support during the pandemic, reported that they did not feel the need to engage in face-to-face support once it returned to being an option:
'I don't feel the need to do face to face. The trust is already there. In fact, it has [been] since the first time we spoke.' [FS5]
Reflecting this preference, a number of participants shared that for them, accessing services online or via the telephone provoked less anxiety. One participant spoke to the benefits they found in using an online app to access sexual health services:
'Just typing it out is probably easier as well than being on the phone sometimes. The first time you go, you're going to feel stressed and worried about, 'Oh, look at me. I'm here because I have this, this or this,' or you think you have this, this or this. A phone-call, as well, can be quite daunting. I feel like it's a bit less, not less personal, but I feel like you can take a step back and think. Obviously, if it's a conversation on the phone, you have to just say it, but you can think of what you're saying, what you're happy to say and then what you want from it. You rehearse it and everything.' [I3]
Whilst for the majority, accessing support via technology made a useful addition and improved accessibility, there were some noted barriers this presented. For participants who accessed services on an ad-hoc basis or relied on receiving their support through outreach or drop-in, the closure of in person services resulted in difficulties accessing any support. One participant shared:
'I had an awful time trying to get any support at all really because at the start literally everywhere was closed. it was quite a hard, difficult, dark time for me.' [FS23]
For others, the requirement to engage with technology, even when given this as an option, was a substantial barrier. Participants said:
'I'm no good online' [FS45]
'I struggled online due 2 my phone not being fully accessible' [FS43]
'Don't go online' [FS57]
For these participants, it is essential that services retain an element or in-person or phone support in order for them to be able to engage.
Many participants reported that they were provided with the hardware required to connect remotely with support, such as a mobile phone or tablet, which they would not otherwise have had access to. Whilst this is something that services were able to facilitate during the pandemic with people already engaged, a lack of access to technology would prohibit people from making an initial approach to the service this way. Additionally, a number of participants spoke to the fragility of this as a way of accessing support, noting that when they ran out of data, or if the technology broke or was lost, there was no way of them getting support or even making contact to request a replacement. The clear message was that face-to-face remains a crucial part of service delivery for many, and without this provision they simply cannot access support.
For others, although they were able to access remote support, their personal preference was for face-to-face contact. They said:
'it gets me out the house and sometimes I need pushed to do this.' [FS3]
'I felt that services only offered phone support, this really impacted on my mental health, which became frustrating and it was so easy just to hang up.' [FS21]
'I do better face-to-face… I think some people are loving it and it's been more accessible to them. But then, people like myself are getting fed up of all appointments and everything being online.' [I6]
A number of participants expressed concerns about privacy and being overheard whilst accessing support remotely. This was particularly important during periods of lockdown when finding a private space to make a telephone or video call was more difficult and remained so for those living in shared or hostel accommodation or with someone who monitored their communications. For some, the availability of instant messaging, email or an app may alleviate this concern, but it necessarily limits support to written communications and is reliant on strong levels of literacy and proficiency in the language of the app as well as ongoing access to appropriate technology. One participant said:
'In the Highlands, they're just a chat service from NHS Highland. You didn't even need to call. I could do it at home, with my parents there. I could just go on my phone and type it, instead of actually having to phone, that was actually really helpful, especially with lockdown and things. You just go on and then you put in your name and things, and then you just say what you're looking for. Then they'll talk to you. They'll ask you, if you have questions and then they'll send you information through that as well, links to stuff, to look at where you go or anything. They normally send you a little leaflet to look at. It's a lot easier than just on the phone. You can screenshot it as well, so you know exactly what it is that's been said.'[I3]
Whilst this participant had a positive experience in some services, participants said that the move to automated, or online systems resulted in a lack of flexibility. One participant who had engaged with sexual health testing online during the pandemic shared that this had involved filling in a form with tick-boxes, and no option to disclose her selling of sex and subsequently to request additional testing. She noted that when services had been face-to-face she was able to easily have this discussion with workers at the clinic she attended.
Taken together, the data shared around routes into and methods of accessing services, makes a strong case for the value of joined up and partnership working with clear referral routes into and out of specialist services. Additionally, the data highlights the importance of offering a range of technology options alongside in-person support for facilitating easy access.
The participants experiences strongly indicated the value of flexibility and a suite of access options to meet individual needs and preferences in order to best facilitate access to services.
4.2 Challenges and Barriers to Mainstream and Specialist service access
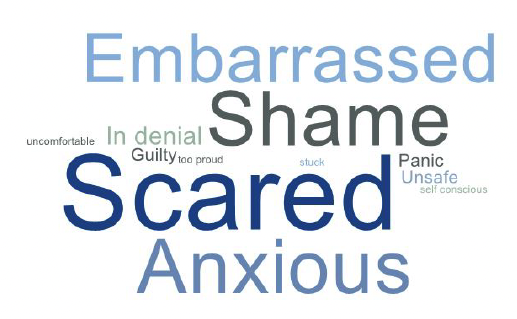
Technology and access routes are not the only factors impacting on the ability of individuals to access services. Participants were asked to share the reasons that they do not access some services, or the reasons they believe that others who sell or exchange sex do not access services. This information refers to both mainstream and specialist services, as the challenges and barriers frequently mirrored each other here. The graphic in Figure 10 displays the range of emotions participants reported prevented individuals from accessing services. Most common were fear, shame, anxiety and embarrassment.
The complete discussions around service access have been thematically analysed and are explored here. The core challenges that participants faced in accessing services were:
- Identifying a Service
- Practicalities
- Emotional barriers
- Social barriers
These themes are discussed in more detail in the following section. Also present in the data was a substantial number of barriers raised in relation to the role that addiction has in presenting challenges to accessing services. It is impossible to isolate the role that addiction plays from other related social, emotional and practical factors. As such, the impact of addiction has been considered within these sections, but it is important to note the prominence narratives around addiction had in the data and the role it plays for a large number of the participants in creating and exacerbating many of the challenges presented here around accessing services.
4.2.1 Identifying a service
One of the most prominent barriers to access participants raised was not knowing that services existed until they were referred to them or approached during proactive outreach. A number of participants felt it would have made a substantial difference to their life and experiences if they had known about the service they eventually engaged with earlier. The comments from these participants echo those shared by many others in both interviews and surveys:
'I wish I had known about them at the very start' [FS4]
'I wish I found this service years ago.' [FS5]
Additional participants reflected these sentiments in response to being asked what would have helped in the past, saying:
'knowing that I could have accessed support like [this service], that way much of the problems would never had happened.' [FS8]
'Knowing more about [service] earlier - I think more people would get support if they knew about it.' [FS29]
'Knowing about the service sooner' [FS26]
As well as the negative impact participants report this delayed engagement with support had on them, it is possible to infer from these experiences that there are likely to be people who would currently like support who do not know what services are available or how to access them. Participants were explicit in their belief that earlier access to support may have helped them avoid negative experiences related to selling or exchanging sex.
One participant who had self-referred into specialist services noted similar difficulties in locating information about support, even when actively seeking it. They said:
'[you] have to dig to find out about support on offer/where it is. So more information to let other people know about stuff.' [FS17]
Again, this participant expresses concern for other people who might be struggling to locate the support they would like or be unaware of their options. Another participant reflected her concerns about others not knowing services exist, saying:
'there's lots of girls who do this who don't want to or have nothing else to turn to. They need to know what is out there to help them and who they can talk to.' [FS32]
Other issues raised in identifying appropriate support services relate to being unaware that they were eligible for support from the services that they knew about. One participant noted the benefit in:
'Better advertising of the range of behaviours that could constitute the sale of sex. I was involved in sugar dating so when it all went wrong for me I did not really know that I would be entitled to any support or help' [FS7]
Another participant reflected this sharing that the broad range of experiences people have selling or exchanging sex left her unclear as to whether there was any support suitable for her. She recalled her experience approaching a service which did not offer the support she wanted around exiting, saying:
'I know you guys are fighting for the rights of people that are still in the industry but can somebody help me please to get out of this industry because I don't want to be there,' and they couldn't help me either. They told me, 'Nobody has those services to help you get out. The only services you'll come across are organisations saying they're supporting and helping women that have been trafficked and in the sex industry' [I2]
Through her recollection of this exchange, she highlights an awareness of a perceived hierarchy of need in relation to people who sell or exchange sex, with the responses to those who have been trafficked being much more supportive than those who have not. Through this, she recalls being left believing that there were no services that would support her, as she had begun selling sex through social and economic, rather than physical, force. The result is that she felt she did not fall within the eligible categories she has identified: those seeking support without wanting to stop selling sex and those that have been trafficked. Through both experiences, the participants highlight the benefits of services being clear in their service offer, including clear eligibility criteria and ensuring available services cover the range of experiences and support needs. Additionally, both experiences here point to the value of clear messaging and clear definitions for what constitutes the sale or exchange of sex and therefore who can access support around this.
The final challenge raised in relation to identifying an appropriate service was that participants felt there was no suitable service for them. The majority of participants had successfully engaged with support and did not hold this view, however, two participants expressed strongly that they knew what support was available, and that they were eligible but felt there was nothing that addressed their needs. One participant explains:
'coming out of the industry there's nothing there to help you really. Not really in the scale of what kind of help you want. There are no services that give you exactly what you need, there are a lot of services out there that are doing things like art projects and stuff like that but I don't think that's really helping people with the actual help that they need.' [I2]
For this participant, the support offered did not align with what she felt she needed. She spoke to her experience of services being lacking, and cohesive exiting support not being available. She went on to share her experience of feeling like she needed to exit alone and that she was not supported through this process. She shared:
'it's so hard to try and make sense of everything that has happened. There were no courses to help me make sense of it… There was nothing for me at all. I had to try and figure it out myself' [I2]
Her experiences call for a broad range of services, including post-exiting support.
4.2.2 Practicalities
For participants who successfully identified appropriate support, there were a number of practicalities that could prohibit them from accessing these services. For some, opening times were not able to accommodate their routine. They said:
'Opening hours, I would like the drop in to be open through the night' [FS11]
'My lifestyle then [stopped me accessing support] I slept all day and worked the streets at night' [FS13]
'I'm only usually out by night' [FS45]
Particularly common across all participants was experiencing difficulties with getting an appointment which was suitable for them. Participants shared:
'It is too hard to get an appointment, reception staff are rude and impatient' [FS35]
'Hard to get an appointment so just gave up.' [FS17]
For others a long wait time to be seen meant that they did not engage by the time the appointment came around, as either their circumstances had changed, or they had lost momentum in their attempts to access support. Participants affected by this said:
'I waited for 12 weeks to get appt' [FS29]
'the wait time meant no longer engaged.' [FS31]
One participant shared how her support experiences were impacted both by long waiting times and feeling the provision was not sufficient for her needs. She shared:
'I had to try and get put on waiting lists with counselling, I waited months to get counselling, just counselling on its own. I waited months to get doctors appointments for health stuff. I tried to go to [specialist service] to get help, I got 2 talking sessions with someone. That's not going to help me really.' [I2]
As well as issues around waiting times and ease of getting appointments, another practical barrier was the service not being in an easy to access location, for example on a bus route. Participants shared that they stopped going to services that were 'too hard to get to' [FS17] or difficult to travel to [FS46]. For another participant, it was not the physical location of the service, but the fact that it was co-located with other services that caused her issues with access. She said:
'The location - it is in the same building as addiction services which I have engaged with previously. This triggers me a bit now I'm in recovery.' [FS33]
For her, the location of the service in a place she had previously accessed during a challenging time represented a mental barrier to engagement.
Another practical barrier that participants raised was around services not being able to meet their individual access needs. For one participant, access was initially difficult due to her proficiency in the English language. She says:
'The first time I started it was difficult because my English was not very good. It is better now, easy enough as my English improved.' [FS40]
Although this did not result in the participant disengaging, all services need to be designed in order to accommodate people with translation or interpretation requirements. As well as this, in line with all support services, for some people there are likely to be physical barriers to access in buildings which, for example, are not wheelchair accessible. One participant shared how the service she accessed was able to provide her with childcare, and this represents an important additional consideration for people with caring responsibilities.
For a number of participants, the practical barriers they faced were in the set-up of the service itself. They felt that the conditions of service delivery meant that, were they to disclose their involvement in selling or exchanging sex and seek support around this, another service they were currently receiving would be withdrawn. One area where a number of participants raised this was in relation to housing. One participant explained:
'When you're staying in homeless hostels and stuff, these specific supported accommodations, if you have any sort of income, the rent you have to pay is extortionately high and nobody could afford it. And then, you'd be on the streets homeless, which nobody wanted to be. So, you can't talk to the support staff there or anyone.' [I6]
In this way, the income threshold for paying for supported accommodation was reported to prohibit participants from seeking support around selling or exchanging sex, as this would require them declaring an income. Similar experiences, or fears were reported in relation to having benefits withdrawn if their income from selling or exchanging sex became known. One participant shared:
'People who are on benefits because they're really poor, who are also [selling sex] because they're really poor can't disclose that they're [selling sex] and making money because they'll lose their benefits. Yeah but those people might still need help with benefit advice or money so they'll have to keep it absolutely zipped that they make any kind of money so they might be scared to go to services' [I5]
Another participant explained how she feels insecure on her benefits, and fears revealing about her involvement in selling sex. She says:
'every time with personal independent payment, they've cut me down in points. They're trying to get me off it, I'm sure. And it just doesn't feel safe. And I haven't told them about prostitution because I fear getting in trouble with the taxes. I haven't told the DWP. I haven't been able to. But maybe they should know and be able to recognise women who have been involved.' [I1]
Other participants also felt that the practicalities of service set-up prevented them from accessing the support they needed, but for them it was the combination of support they required that presented a challenge. Through this they highlighted a number of areas of siloed working, where access to one service may preclude them from accessing another. One participant spoke to the issues she faced in accessing mental health support when she was in addiction:
'if you're using drugs you will not get to see a counsellor. You will not get to see a psychologist, you will not get to see a psychiatrist.' [I4]
The same participant felt that there was not suitable support for her whilst she was pregnant to address the issues she felt she wanted to around both addictions and mental health:
'I got my daughter took off us because, and they don't touch you when you're pregnant, they'll not see you when you're pregnant and they'll not touch you three months after you're pregnant, and I just think that mental health is a big part of why people are taking drugs and that should be in every service. Regardless of if you're taking drugs or not at the time you're a human being, somebody's daughter, somebody's Mum and you need to be seen.' [I4]
For this participant she felt the lack of a service that could accommodate her multiple needs resulted in the trauma of having her child removed from her care after birth, which she believed may otherwise have been avoided. To further illustrate this, she shared that once she was no longer pregnant and able to access support, she regained care of her child. These siloed support services were raised as problematic by a number of participants and in some circumstances, they felt this may prevent them from accessing the services they needed. These findings are particularly important in relation to the finding that participants in this sample attended services to address an average of seven different support needs (see section 3.3). However, whilst for these participants the sharing of information without procedures to mitigate negative impacts represented barriers to accessing other services, for others, lack of information sharing between services meaning that the need to repeat their story became a barrier in itself. One participant explained:
'It's like you have to tell your story over and over again. So you're working with one service and then you're getting directed to another, and then sometimes information isn't getting passed on, you're having to go through everything again. And that's not down to, well, it is down to the services, it should be working alongside each other, you know. And that's a barrier because services will not work together.' [I4]
She described this repetition as a barrier, and it is likely that the experience of having to revisit difficult or traumatic experiences at each services provides a substantial barrier to some people who sell or exchange sex from engaging with the support they may want.
4.2.3 Emotional Barriers
Alongside practical considerations, emotional factors played a large role in participants ability to access services. The three most prominent subthemes around this were trust, fear of judgement and it being 'not the right time'.
4.2.3.1 Trust
Lack of trust was frequently raised as a barrier to engagement with support services. Trust was understood in different ways, but for some this manifested as not trusting the workers at the service enough to share their experiences with them. One participant said:
'It was difficult at first because of my trust issues but I soon realised my worker was there to help me.' [FS30]
In some cases, trust was reported to be particularly difficult to establish where the worker was male, due to difficult and traumatic experiences many female participants reported having had with men. One participant shares how the particular attributes of one male worker made it especially difficult for her to engage with the service, and eventually resulted in her stopping. She said:
'I didn't like having male staff either - they were ok but I wanted a woman worker but I was assigned a male case worker. I didn't really go too much and just stopped. I didn't want to have to say that the worker reminded me of an old customer and I knew the women all had full caseloads so didn't want to start off working with a man and then change when a woman became free.' [FS32]
For others, experiences with males who bought sex had resulted in a lack of trust for their whole profession. One participant who shared her experiences through fieldnotes shared how one man who bought sex from her was a nurse, and this has impacted on her relationship and perception of the medical profession. [I7] For her this presented a substantial barrier to engaging with any men within the medical profession.
As well as a lack of trust in workers as individuals, participants frequently reported concerns about where their information would be shared, and not trusting the service to keep their information confidential. One participant said:
'A lot of girls are afraid that services will tell each other if we are involved and that puts them off.' [FS32]
One participant shared her fear that any disclosure she made to any medical services, may be shared with mental health services, and used as a judgement on her mental wellbeing. She said:
'It's just one box they can tick that might lead to me like getting sectioned or something you know. I just don't trust them to have an unbiased approach to using that information.' [I5]
Particularly frequently mentioned were social services, and participants reported having substantial fears about information they shared about selling or exchanging sex being shared with them. Participants said:
'Don't like social work so any hint of that and I avoid [accessing services]. It's not worth it if it ends up disrupting your life. You're better off on your own.' [FS34]
'Scared of losing kids, scared of everything they do' [FS53]
Another common fear reported was not trusting that the service would not report them to the police for selling or exchanging sex, and that they would then face prosecution. In this way the criminalisation of the individual selling or exchanging sex can be seen to directly contribute to difficulties participants faced in accessing support. One participant said of this:
'The fear of being arrested, I knew that sexual health services have a certain level - because they're doctors - they have a certain level of privacy protection. They aren't allowed to share their information even if they wanted to and it could cost them their jobs if they do and it would be an enormous scandal so I felt safe talking to them and disclosing to them why I wanted the tests and why I was there more often than most people … but I would never tell any other services.' [I8]
Fear of arrest was reported to prevent people who sold or exchanged sex from seeking any support they may wish, but was also raised as a barrier to reporting any crimes against them. In this way, fear of arrest and lack of trust in the police preventing participants from accessing the justice and associated victim support they were entitled to. They said:
'I wouldn't have reported to the police, no… I wouldn't contact the police, I was too scared.' [I2]
'If I was raped by a client, it would be very tricky to go to the police because I wouldn't want to tell them I was [selling sex] ... so you can't give them all the information for your own safety. Like that's how it should be viewed not like you're breaking the law and bad things happen to you… it's an absolute mess.' [I5]
Another participant spoke to their experiences of someone buying sex from them when they were underage and then stealing the money back. They reported that their lack of trust in the police, and fear of arrest resulted in them not reporting the crime against them. They said:
'I think, knowing that if you go and report someone for that because it's a bad thing to do, then you're not going to get in trouble, but obviously, you have done something wrong, so finding that balance between it and things like that. If you do need to report someone for it, the police might have a bit of stigma about it as well. If you approach them about it, they could have the same issues.' [I3]
In this way there is a clear link between reported lack of trust in the police, and participants feeling unable to access the support and justice that they are entitled to as the victims of crime.
In addition to lack of trust and fearing negative consequences, a number of participants reported having had negative experiences in the past which they felt were directly caused by accessing services. This left them not wanting to access services again because they did not trust that the services would act in their best interests, and not worsen their situation. A number of these negative experiences related to support they were accessing around addiction. One participant shared:
'[what would have helped is] not being cut off my methadone, I had never been on the street before that, if they hadn't cut me off then I wouldn't have met punters who still try to contact me and would not have had to use other drugs to cope and maybe I would not have panic attacks, being cut off my methadone completely changed my life for the worse, they shouldn't be able to do that' [FS3]
Another sector that was attributed by a number of participants as contributing to an increase, rather than decrease in their support needs was housing. In particular, participants spoke to the negative impact that being in hostel accommodation had on them, or on people they knew. One participant shared:
'Stop putting us in hostels, there's too much drugs going on. I would rather live on the streets than go back to a hostel.' [FS19]
Additionally, two participants spoke to the environment of the hostel being a place that many people begin selling or exchanging sex in the first place. They said:
'I know a sixteen-year-old that is going along the road. Went into a hostel, never took drugs and now injecting heroin and prostitution. So it's just dived.' [I4]
'I've been through the homeless services a few times and my longest time spent homeless was about 2 and a half years and I met a lot of other women who got involved in [selling or exchanging sex], whilst homeless.' [I6]
These stories illustrate the fear that participants have, that engaging with certain support may result in a deterioration of their circumstances, particularly round addiction. These fears are a substantial barrier to them trusting the service enough to engage and attempt to receive support.
4.2.3.2 Fear of Judgement
Fear of judgement was a particularly prominent barrier participants faced to accessing services. Reflecting the findings on disclosure to mainstream services (see section 3.3.1) for many people it prevented them from talking to services about selling or exchanging sex, even when they were accessing these services for something else. In this way, fear of being judged acts as a barrier to accessing appropriate support, even once within mainstream services, and a barrier to initial engagement with specialist services. One participant shared experiences reflected by many others when she said:
'Most [people who sell sex] feel they are judged and have terrible shame about their past.' [FS5]
Another participant said:
'if I have heard from anyone else that they didn't get treated too well - then I don't want to go. I don't like to go to services anyhow but if I think they are going to be all snotty, then I won't go near them.' [FS32]
A number of participants shared that fear of judgement means they never talk about selling or exchanging sex with anyone, and that trying to do this in order to receive support is a substantial barrier. One participant whose experiences were recorded using fieldnotes explained how she felt about herself. She shared that she:
'Does not like to talk about selling sex as she 'feels dirty' she is constantly washing herself and showering but she can never feel clean. She knows someone who has scrubbed themselves with wire wool but she has never gone that far herself. She feels that all the blame and judgement is on her and people just see her as a 'dirty little prostitute'. [I7]
This high level of self-judgement prevented her from feeling able to talk about her experiences with services, as she fears they will judge her as harshly as she judges herself. Others reflect this feeling of the judgement and expectation of judgement coming from within themselves. One participant shared:
'In the past I would have been too embarrassed. I would have been in my own head feeling like an idiot.' [FS7]
As well as fear of being judged negatively, other participants reported that they fear being seen as a victim or pitied. One participant shared:
'some people don't want to be seen as a victim, I don't see myself that way, I used to but now I think I'm a survivor - a lot of sh*t things have happened but I'm still here. It can be hard to speak to anyone about it, you are scared that you won't be believed or you will be pitied. You don't want anyone looking down on you and sometimes when you speak about these things people just feel sorry for you.' [FS29]
Another participant whose experiences were recorded using fieldnotes also echoed these fears of not being believed. She shared that:
'she took Valium when she first sold sex so she did not remember what she was doing, when she came round she realised that the man she was with was taking photos and videos of her, and he mentioned sharing these with his friends. [I7].'
For her, her fragmented and partial memories meant that she felt she could not give a clear account of her experiences, and this made her fear that services would not believe her experiences. The idea of not being believed, having taken the risk to talk about her experiences and open herself up to potential trauma was too big a barrier and resulted in her not disclosing to services.
Whilst many participants felt they were judged based on their experiences of selling or exchanging sex, other participants related feeling that they were judged by services because of their use of substances. One participant shared her experiences:
'I have really bad anxiety so I don't like going to new places or without someone with me. I need to use (street) valium before I can even get out the door and some services look down on you or think you don't want support or think that I am too under the influence when I'm not and if I am it's because I need to be to come in the first place.' [FS28]
In this way, this participant felt that her reliance on services meant services doubted her motivation and did not offer her the support she needed.
As well as feeling that their presentation after using substances made services judge them, another participant shared that she felt that her reputation from actions in the past precluded her from accessing services currently. She said:
'I would like services to get to know me first, not to take on other people's opinions before working with me. Some services are not willing to work with me.' [FS1]
This participant's experience indicates that she felt that a reputation of being 'difficult' had meant that she is now unable to engage with services, even when she feels she has acted appropriately with them. For her, the judgement that many fear has been realised, and she expects this to happen each time she now attempts to access services.
4.2.3.3 'Not the right time'
Another prominent theme raised in relation to barriers to accessing services was that of it not being 'the right time'. One participant summarised the responses around this when she said:
'I think sometimes it just needs to be the right time, I don't know if it would have made any difference if [my worker] was there back then cos I don't think I would have listened [FS19]
Further participants shared their experiences of not being ready to accept help or admitting to themselves that they needed it. They said:
'they see it as a weakness, admitting you're struggling, but really it's not. It's a strength and I always make that clear to people. You asking for help is a strength so give yourself a bit of credit.' [I4]
'At that time I don't think I was ready and didn't think I needed it and could sort it all myself.' [FS28]
'before I was too proud to ask and say that I needed help and just couldn't accept it. I had too much pride and I thought I could do it myself but I was wrong. I needed the help, take the help!!' [FS23]
Another participant reflected this experience of not being ready to accept help, and not wanting to face the issues they wanted support with. She said:
'I'm good at locking things away but I'm at the point I'm ready to open that box and talk about everything inside my head and what's going on in it.' [FS23]
Some participants had experienced attempts to engage with support in the past, which had not been successful, prior to successfully engaging with their current service. They said of these:
'I have had other support in the past but I didn't really want to work with them or avoided it and got discharged because I was too anxious and just didn't take it seriously. At that time I don't think I was ready and didn't think I needed it and could sort it all myself.' [FS28]
'I met [worker] a few years ago at an event. I went up and spoke to her but I wasn't too nice!' [FS32]
Whilst these experiences do not directly suggest any particular change in provision, they do signal the importance of support being available long-term, so people are still eligible when they are ready to engage, and also ensuring that there are not substantial penalties where people disengage and support is still available if and when they return.
4.2.4 Social Barriers
As well as practical and emotional barriers to accessing services, a number of barriers were raised which related to participants' social world. A common challenge was encountering others who might be accessing services, or the fear that they might. For some, entering any crowded environment was difficult. One participant shared the negative impact that this had on her:
'when too many people go at the same time, I get anxiety going into a hall for something to eat and everyone looks at me' [FS23]
A number of other female participants particularly noted that for them the issue was going to services where there may be men, or groups of men around. One participant said:
'I wasn't too happy with lots of men around as I hadn't had too good experiences with men in my life from [when] I was young. There was always men hanging around the front of the building and I hated having to walk through them.' [FS32]
For these participants, a service being crowded, particularly with men was enough of a barrier to prevent them accessing the support they wanted from there. For others, the service was too often frequented by people they knew and did not wish to see, and the fear of encountering them prevented them from accessing the service themselves. They said:
'I don't like mixing with people especially people from my past who might use the service.' [FS11]
'Didn't want to engage or associate with others who were using the service.' [FS31]
Whilst many participants did not specify what it was about the people from their past that made them avoid the service, those who did most frequently cited the prevalence, and likely offer of drugs. One participant reflected this when she said:
'just looking at the building gives me panic attacks, there are always people there offering you drugs or know that you are vulnerable or skint so they prey on you.' [FS3]
For others, it is other people in their social world, not at the service itself who serve to prevent them from accessing support. One participant shared that the influence of her partner made her fear accessing support. She explained she did not go to services in the past:
'Because I was with my ex, too afraid of going somewhere to ask for help, just felt horrible' [FS55]
Asking directly about coercive others in participants lives was outwith the scope of this research, however a number of participants did volunteer that the physical, coercive and emotional abuse of another prevented them from accessing services they may otherwise have chosen to engage with. One participant, who did not want to be recorded, so had her contributions recorded though fieldnotes shared how:
'Her partner put her out to sell sex, and she was stripped naked and left out in the snow by someone in a car, she didn't know where he was taking her. Her partner blamed her for not running away, but she thought if she ran she would have frozen to death.' [I7]
Another participant, whose contribution was recorded through fieldnotes shared the impact that being stalked had on her. She shared about:
'cars following her for hours on end, people following her in the street, and how these circumstances combined to make it very difficult for her to escape or to be able to consider accessing services' [I9].
In circumstances such as those shared, when participants were subject to ongoing abuse and control, it is often not possible for them to access support and any attempt is likely to put them at substantial risk of harm. For participants who had been trafficked or forced by someone else into selling sex, the circumstance of the relationship with their exploiter are likely to limit their ability to access services. In these circumstances, accessing services before intervention is simply not an option.
Some participants reported that rather than the physical presence of others, it was the threat of others and living under constant fear that prevented them being able to access services. One participant explains:
'I feared for my life, I went to work and I didn't know who was going to walk through my door. I had all the gangsters who knew who I was and I didn't know who they were. Living with that amount of stress on a daily basis does do something to you, it changes you.'[I1]
For her the circumstances of existing under constant stress and pressure prevented her from attending appointments at specific times or being able to engage meaningfully with services that required her to leave her house and present at an office at a certain time and place. Another participant reflects this, as she explains how living in this survival mode left little capacity to proactively seek out and engage with support, even though she identified it as something she needed. She says:
'Your life is a bit hectic because you're constantly in fight or flight. You honestly are. You don't know who's walking to your door next anyway, first of all clients, you don't know who they're going to be coming to your door so you're always on guard thinking, 'What if they kill me?' Loads of people get killed in this industry and you know that but you take that risk because of the money, but you still know in the back of your mind all the time that if somebody walks through your door, they could potentially be the person that's going to murder you because you don't know these people. That's always in the back of your mind.' [I2]
In this way social barriers can have a substantial impact on an individual's ability to engage with services, whether this is through the people present in the building itself, or those exerting their influence over individuals who want to access services. It is important that services consider the impact of social barriers where access may be a challenge.
Contact
Email: anthony.nevin@scot.gov