Type 2 Diabetes Mellitus - quality prescribing strategy: improvement guide 2024 to 2027
This quality prescribing guide is intended to support clinicians across the multidisciplinary team and people with Type 2 Diabetes Mellitus (T2DM) in shared decision-making and the effective use of medicines, and offers practical advice and options for tailoring care to the needs and preferences of individuals.
5. Is Metformin always the first line prescribed therapy?
Metformin as a first line oral treatment option[1]
Metformin is the first line option unless there are contra-indications (see BNF).
The aim of treatment is to reduce HbA1c to an agreed target level in order to reduce long term complications from T2DM (refer to Table 3 for benefits of long-term HbA1c reduction).
Benefits:
- Metformin is effective, safe, inexpensive and may reduce risk of cardiovascular events and death.[36]
- Compared with sulfonylureas, metformin as first-line therapy has beneficial effects on HbA1c, weight and cardiovascular mortality and has reduced risk of hypoglycaemia.[37]
Many of the recent cardiovascular outcome trials compared new therapies added to metformin and not as first line options.
Side effects include:
- Gastrointestinal symptoms such as diarrhoea. This can be minimised by gradual increase of the dose when titrating to the dose required. A trial of metformin modified-release preparations could be considered according to local formulary guidance.
- Association with vitamin B12 deficiency. This suggests that periodic testing of vitamin B12 levels should be considered in metformin-treated patients, especially in those with anaemia or peripheral neuropathy.[38]
Prescribing notes:
- Metformin may be safely used in people with estimated glomerular filtration rate (eGFR) greater than 30 ml/min/1.73m2 (dose adjustments required if eGFR less than 45ml/min).
- Individuals should be advised to withhold metformin in cases of nausea, vomiting or dehydration (using Medication Sick Day guidance).
- If metformin has been withheld due to acute kidney injury/ inter-current illness, it can safely be restarted if the renal impairment has resolved.
National Therapeutic Indicator
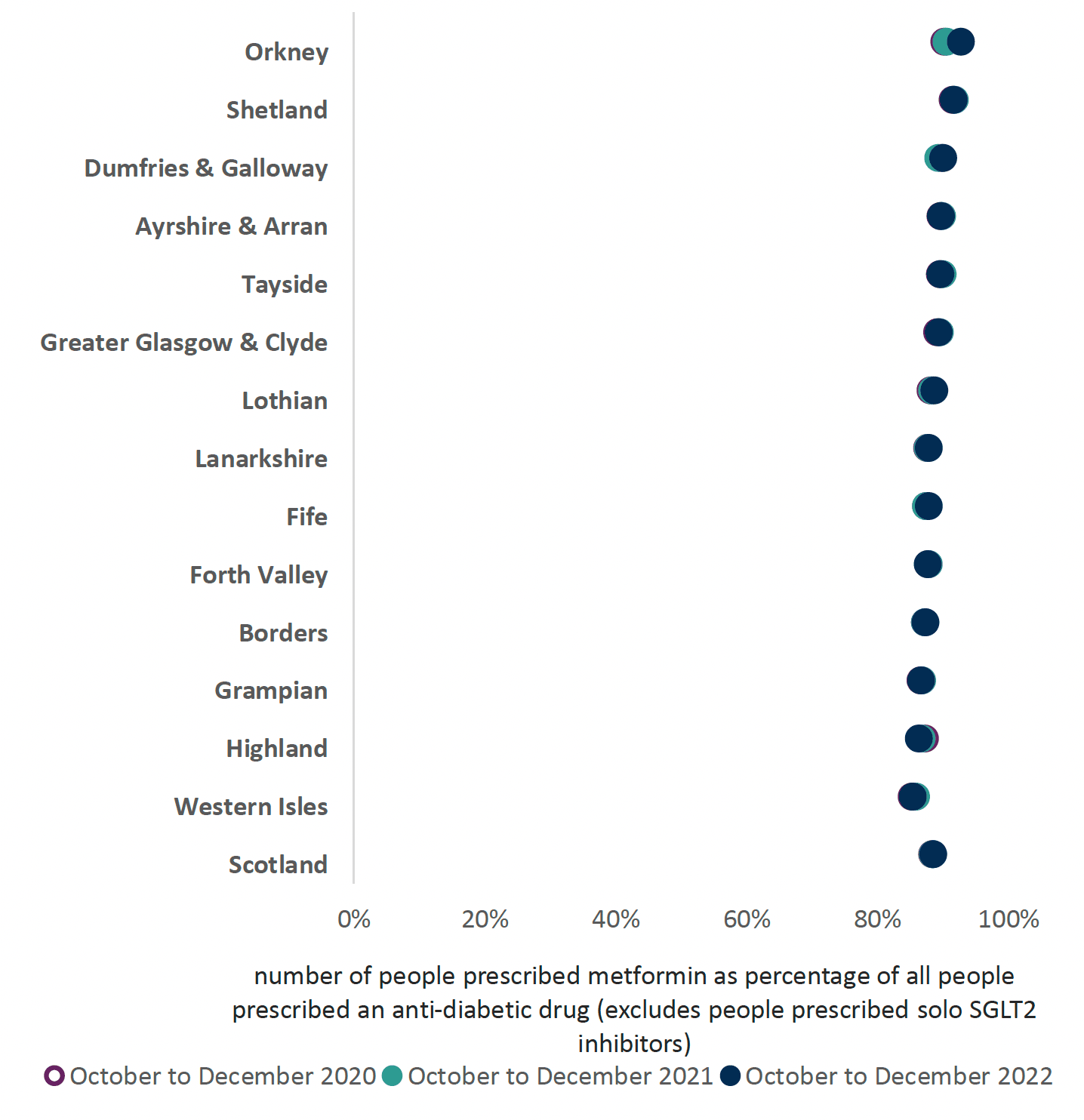
Metformin: number of people prescribed metformin as a percentage of all people prescribed an anti-diabetic medication.
This indicator (see Chart 4) should have a high percentage, as there are limited contra-indications for its use, and clinicians, GP clusters and boards should consider how their levels can be increased to ensure individuals are receiving evidence-based therapies.
When metformin is contra-indicated or not tolerated, the following factors should be considered, similar to those for second choices (see section 6 for more information).
When assessing an individual, it is good practice to establish whether the individual:
- has any existing atherosclerotic cardiovascular disease (ASCVD)
- has a very high risk of developing ASCVD (left ventricular hypertrophy (LVH) or aged >55 years and has carotid, coronary or peripheral artery stenosis >50%)
- has symptomatic heart failure
- needs to avoid or minimise the risk of hypoglycaemia (e.g. occupation, driving)
- needs to minimise weight gain
If HbA1c remains above the agreed treatment target for the individual, the following should be considered:
- optimising the dose of the current medication
- adding a drug of a different class
- stopping drugs that were ineffective and did not lead to a measurable improvement in HbA1c; and
- considering drug-specific and individual factors when selecting which anti-hyperglycaemic treatments to use
- reviewing and adjusting every three to six months in discussion with the person living with T2DM
See Table 6 for a summary of the benefits and cautions for anti-diabetic therapies, based on ADA[40] and ABCD.[41]
Prescribers should familiarise themselves with the prescribing indications and contra-indications of individual agents, as these may vary within drug classes as well as interactions listed in the BNF and/or the Electronic Medicines Compendium, before initiating therapies in line with local formularies.
| Drug/therapeutic class | Efficacy | Risk of hypo-glycaemia | Weight Change | CV Effects | Renal Effects | ||
|---|---|---|---|---|---|---|---|
| ASCVD | HF | Progression of DKD | Dosing/Use in CKD | ||||
| Metformin | High (11 mmol/mol) | No | Neutral/ modest loss | Potential benefit | Neutral | Neutral | Reduce/stop |
| SGLT-2i | High (9-11 mmol/mol) | No | Loss | Benefit | Benefit | Benefit | Adjust dose. Less glucose-lowering efficacy if eGFR <45 ml/min/1.73m[2] |
| GLP-1RA | High (9-11 mmol/mol) | No | Loss | Benefit/neutral | Neutral | Benefit | Adjust dose for some |
| DPP-4i/ Gliptins | Moderate (6-9 mmol/mol) | No | Neutral | Neutral | Neutral Caution^ | Neutral | Adjust dose for some |
| Pioglitazone | High (11 mmol/mol) | No | Gain | Potential benefit | Increased risk | Neutral | No adjustment |
| Sulfonyl-ureas | High (11 mmol/mol) | Yes | Gain | Neutral | Neutral | Neutral | Adjust dose for some |
^ see individual SPC for variation within class
| Additional information | Use in frailty | |
|---|---|---|
| Metformin |
|
Use with caution if previous episode of acute kidney injury |
| SGLT-2i |
|
Increased risk for volume depletion |
| GLP-1RA |
|
Once weekly injectable formulations available |
| DPP-4i/ Gliptins |
|
Caution in congestive heart failure NYHA class III and IV |
| Pioglitazone |
|
|
| Sulfonylureas | Avoid if inconsistent eating patterns |
Contact
Email: EPandT@gov.scot