Type 2 Diabetes Mellitus - quality prescribing strategy: improvement guide 2024 to 2027
This quality prescribing guide is intended to support clinicians across the multidisciplinary team and people with Type 2 Diabetes Mellitus (T2DM) in shared decision-making and the effective use of medicines, and offers practical advice and options for tailoring care to the needs and preferences of individuals.
1. Why is this quality prescribing guidance needed?
The purpose of this guide is to promote high quality prescribing in T2DM focusing on safe, person-centred care with shared decision-making throughout the process. A target HbA1c should be discussed with the person and individualised to them, taking account of lifestyle, frailty, comorbidities and medication side effects. This is especially important as decreasing elevated HbA1c levels reduces the risk of long-term complications.
In addition, this guide will raise awareness of the non-pharmaceutical management options for T2DM, provide information to monitor and review the multiple agents used to treat T2DM, and explore variation across Scotland. The scope includes adults with T2DM only.
This document does not replace current clinical guidance and should be read alongside SIGN 116 and 154.[1] The expert working group considered the increasing evidence for newer therapies, sodium-glucose co-transporter-2 inhibitor (SGLT-2i*) and glucagon-like peptide 1 receptor agonist (GLP-1RA), since publication of the SIGN guidance and the inclusion of these therapies in other national guidelines (such as NICE[2] and ADA[3]). The expert working group considered the place of these therapies in NHS Scotland, recommending their use (section 6).
This guidance provides additional information, such as prescribing safety and effectiveness indicators and guidance regarding the place of newer therapies in treatment, taking a person-centred approach, through the various stages of the disease process.

Diabetes in Scotland
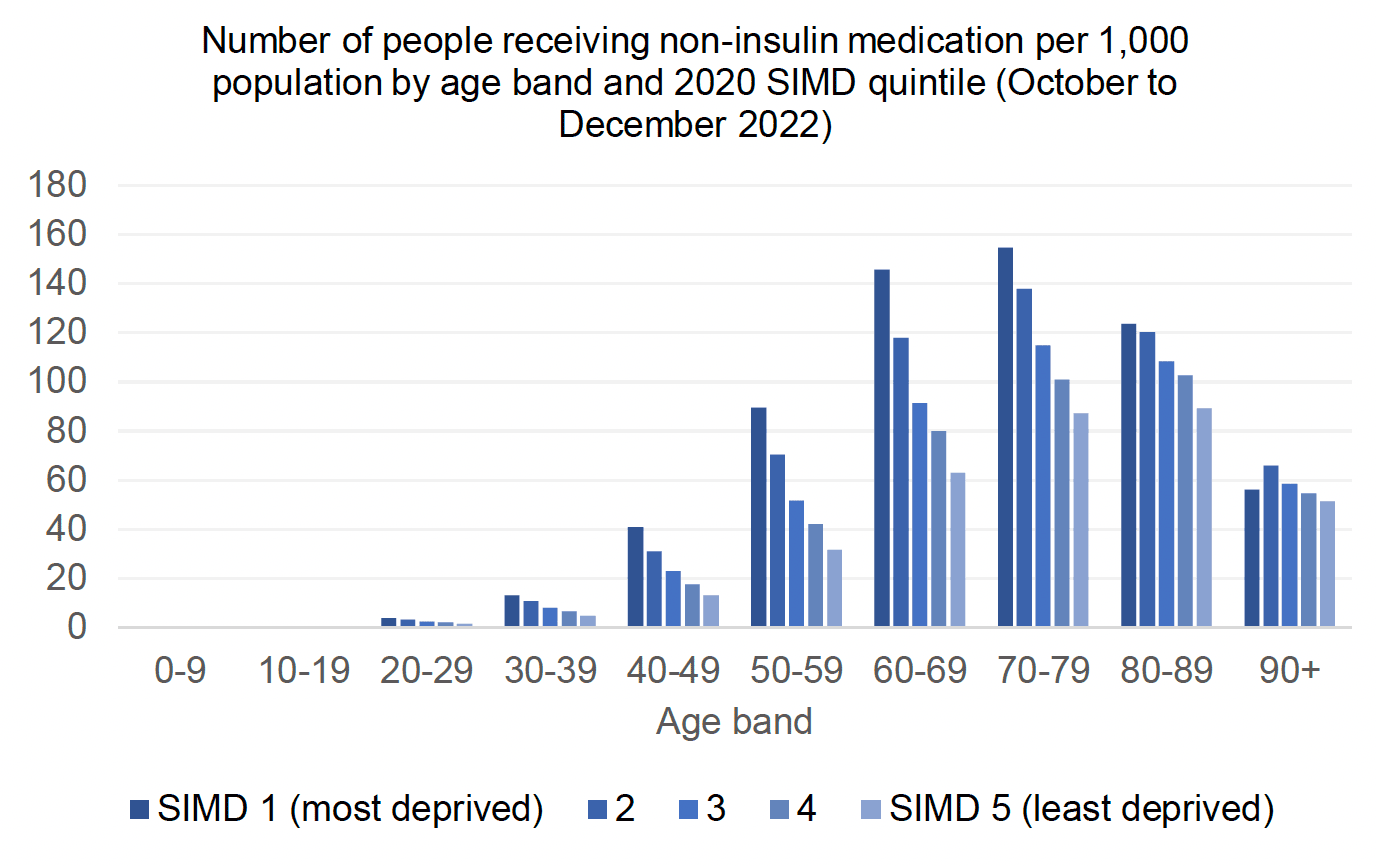
The prevalence of age-standardised diabetes in 2020 was higher among those living in the most deprived quintile (10%) compared with those living in the least deprived quintile (4%). This pattern was evident for both women and men and has been consistent across previous Scottish Health Survey years[4] (see Chart 1).
National policies and guidance
The Diabetes Improvement Plan (2021-2026)[5] reflects the importance of reducing health inequalities as priority four – Equity of Access. It aims to reduce the impact of deprivation and ethnicity on diabetes care and outcomes. It is recognised that there is a complex relationship between mental health problems, diabetes, raised BMI and those vulnerable to health inequalities. Therefore, these factors should be considered when planning the delivery of services.
In 2018, the Scottish Government published two key documents to help address the impact of T2DM on the health of the nation; The Scottish Government’s Diet and Healthy Weight Delivery Plan,[6] and The Scottish Government T2DM prevention, early detection and early intervention framework.[7] The overall aim is to reduce people’s risk of developing T2DM and, for those diagnosed, support remission where possible and the avoidance of diabetes-related complications.
The Effective Prescribing and Therapeutics Division’s Polypharmacy Guide and Realistic Medicine promote best practice and effective use of medicines to address an individual's needs. This maximises the therapeutic effectiveness of treatment and minimises the risk of medication associated harm, using the most cost-effective and sustainable options. Placing the person or carer at the centre of the journey promotes shared decision-making and individualised care.
Incidence and prevalence
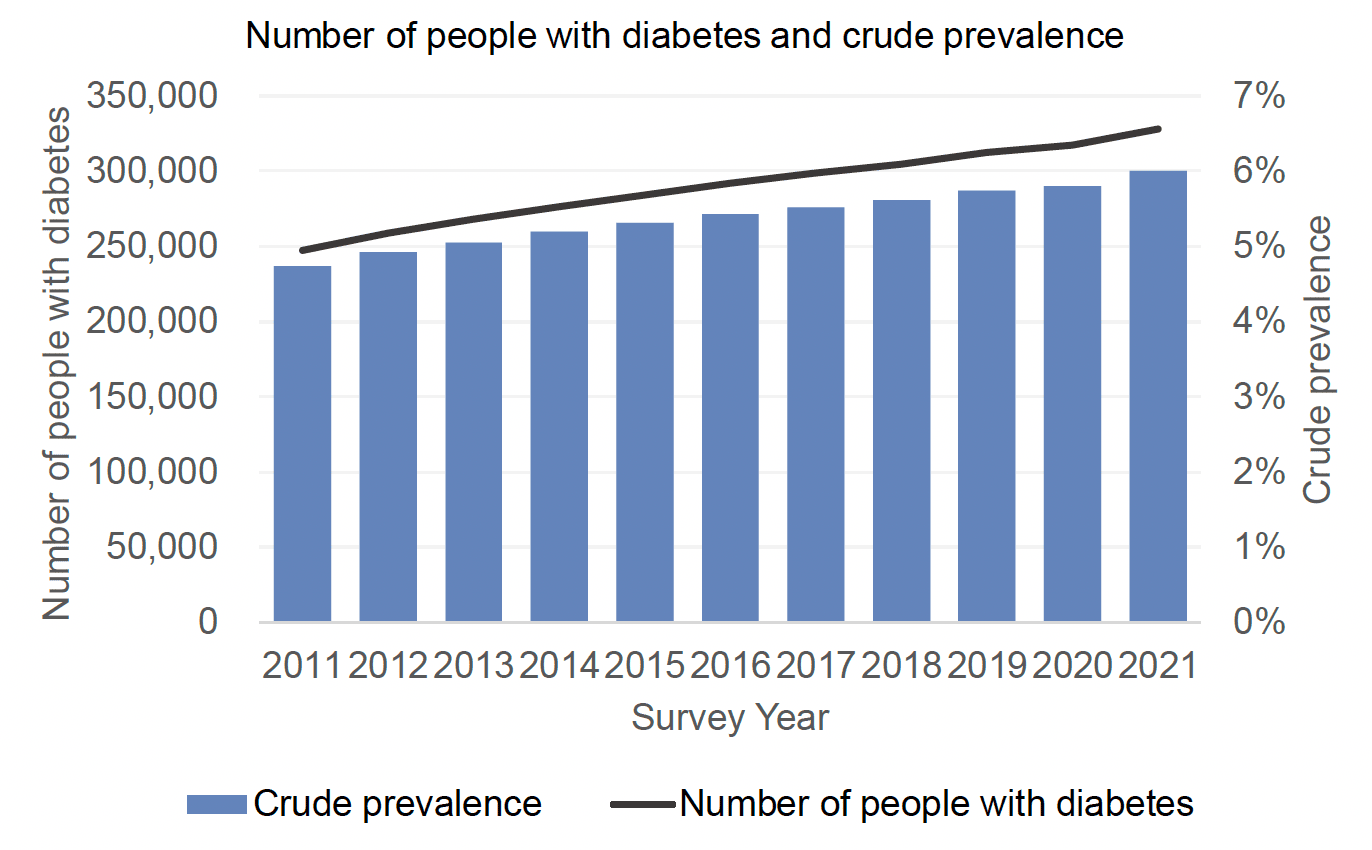
At the end of 2020 there were 327,927 people with known diabetes in Scotland recorded on Scottish Care Information-Diabetes (SCI-Diabetes), which represents a crude prevalence of 6.0% of the population of all ages (5,463,300). The full report is available on Diabetes in Scotland’s website.[10]
The increase in reported prevalence is influenced by numerous factors, including:
- demographic change - diabetes is more prevalent in older age groups, so increasing numbers of older people will increase the prevalence of diabetes
- improved survival – related to improvements in treatment and care of all medical conditions
- earlier diagnosis, including those in younger age groups
- rising obesity levels - having a body mass index (BMI) in the overweight or obese range (BMI >25 and >30 respectively) is the most significant modifiable risk factor for developing T2DM
Prescribing for people with T2DM
For people with T2DM evidence indicates that as well as addressing glycaemic control, there should be a focus on preventing cardiovascular and renal disease. Therefore, there is an expected increase in use of medicines with cardiovascular and renal benefits, with a reduction in use of drugs without evidence of benefit beyond glycaemic control.
High quality prescribing involves:
- shared decision-making to identify the appropriate therapies for the individual which includes risks and benefits
- review of dosage and side effects
- consideration of when a treatment is no longer effective and should be stopped
Clinicians can assess the impact of therapeutic interventions through monitoring glycaemic control or recorded weight, using the SCI-diabetes prescribing timeline tool. A trial of stopping a medicine, with careful monitoring, should be considered when there are doubts regarding the continued benefit to the person. It is also recognised that there will be individuals who require different treatments to those outlined in the guide.
There is a wide variation in glycaemic control in Scotland (information available from SCI DC). While there are times that some individuals will require an individualised target higher than the recommended value e.g. frailty, there may be a large number of people that would benefit from a medication and lifestyle review to optimise outcomes.
Benefits of the guide to individuals with T2DM
This guidance promotes a focus on diabetes prescribing with:
- structured person-centred review of the appropriateness, efficacy, and tolerability of treatment, utilising the 7-Steps approach to medication reviews; and
- consideration and support for non-pharmaceutical management to reduce medication burden.
The positive impact felt by people from their diabetes medicines is acknowledged, although meaningful patient orientated outcome data is not readily available at this stage. Individuals with T2DM also benefit from peer support, available from a variety of groups.
“I was very isolated because I had taken early retirement. I blamed myself for my diabetes and felt ashamed about it. During the pandemic, I had to shield and had little social contact. However, after contacting the Diabetes Scotland Volunteer Support Coordinator, I joined a weekly peer support Zoom call. The group was welcoming and provided a “lifeline” for me, helping me to understand diabetes better and accept my condition. The peer support has brought me company and laughter and I feel part of a community and less lonely.” (Janice, diagnosed with T2DM nine years ago (and living with other conditions)).
In line with international evidence, there is a general shift away from a single disease approach to person-centred care in the context of multimorbidity. It is therefore important to consider this document in the broader context of polypharmacy guidance and a holistic approach to care.
It must be accepted that guidelines are written to provide general advice and therefore a person-centred approach to review will allow for the complexities of multimorbidity.
The benefits of guidance to clinicians
This guidance provides a practical toolkit and examples of high-quality approaches to prescribing in T2DM. It includes case studies (section 13), process for review (section 2) and links to additional resources to identify those requiring review of therapy (sections 12 and 14). The guidance will be incorporated into the Polypharmacy: Managing Medicines app to allow easy access for clinicians to the guidance, alongside resources and shared decision-making tools for use in daily practice.
People with diabetes report a range of experiences at diagnosis, highlighting the need for person-centred care and a holistic approach to management. The following quotes are from people with lived experience of T2DM in Diabetes: my information, my support,[11] produced by The Health and Social Care Alliance Scotland.
“The GP was very thorough. I got much help and guidance from the Practice Nurse. I get regular checks and discussions and am invited to raise questions at any time. I use ‘My Diabetes My Way’ to check on results and to check progress… I feel that I am well supported – given the current pressures on the Health Service.”
“I was told, ‘you have diabetes, and it is all because of what you put in your mouth’… I left his surgery in tears and was comforted by the reception staff who were very kind… This was an awful way to be told you have any illness.”
The benefits to organisations / Health Boards
Included in the guide is a suite of data indicators that can help focus resources on areas that will benefit from review (see sections 12 and 14). Case studies provide examples of how to implement quality improvements prescribing in diabetes, using a person-centred approach (section 13).
Previous guidance considered variation between boards with regards to prevalence, cost and improvements in HbA1c. However newer agents can affect longer term outcomes, independent of HbA1c values, and therefore comparisons using the previous parameters are inadequate to show the whole system effect.
Diabetes prescribing accounts for 11.8% of the total medicines spend in primary care in Scotland (for the year to end March 2022). Table 1 below shows the relative spend on diabetes medicines and classes. Boards should reflect on the relative split of this spend, considering therapies which have less evidence and/or effectiveness.
Additionally due to the complications of T2DM and comorbidities, prescribing costs are attributable to management of hypertension, dyslipidaemia, diabetic neuropathy and others. People with diabetes have a significant impact on hospital resources (accounting for a greater proportion of beds) with more frequent emergency admissions and longer stays.[12] Additionally individuals with T2DM, accounting for age, require twice as much support as those without T2DM.
Therefore, the reduction in whole system costs of managing secondary comorbidities and complications will outweigh any short-term increase in medicines costs.
| Medication and Devices used in Diabetes Total Spend | Section | Section Spend | Class of Diabetes Medication and Devices | Spend |
|---|---|---|---|---|
| £142,322,223 | Insulins | £34,109,276 | Short-acting insulins | £13,875,219 |
| Intermediate and long-acting insulins | £20,234,057 | |||
| Antidiabetic drugs | £70,157,783 | Sulfonylureas | £1,970,483 | |
| Metformin | £6,953,361 | |||
| DPP-4 inhibitors | £11,222,683 | |||
| Pioglitazones | £260,691 | |||
| GLP1 analogues | £21,115,564 | |||
| SGLT2 inhibitors | £28,607,278 | |||
| Other | £27,723 | |||
| Treatment of hypoglycaemia | £569,314 | Glucose | £355,791 | |
| Glucagon | £213,523 | |||
| Diagnostic and testing | £37,485,849 | Blood glucose testing strips | £10,470,113 | |
| Interstitial fluid sensors | £25,573,648 | |||
| Other | £1,442,088 |
Total GP Practice prescribing costs for 2022/23 were £1,179,885,584, diabetes reimbursement costs made up 12.1% of this.
Contact
Email: EPandT@gov.scot