Type 2 Diabetes Mellitus - quality prescribing strategy: improvement guide 2024 to 2027
This quality prescribing guide is intended to support clinicians across the multidisciplinary team and people with Type 2 Diabetes Mellitus (T2DM) in shared decision-making and the effective use of medicines, and offers practical advice and options for tailoring care to the needs and preferences of individuals.
11. How to improve outcomes in disadvantaged groups
The 2019 Scottish Health Survey highlights inequalities in the prevalence of doctor diagnosed diabetes in Scotland.[4]
- Men are more likely to be living with diabetes than women (7% versus 4%, respectively)
- Those living in areas of higher deprivation are disproportionately affected (10% in most deprived quintile verses 4% in least deprived quintile), see Figure 2 in section 1.
Socio-economic inequalities in prevalence have increased progressively since 2003. Compared to those living in areas of lower deprivation, people with diabetes living in areas of higher deprivation in Scotland were more likely to develop fatal or critical care unit-treated COVID-19.[63] In the UK, T2DM is approximately 3-5 times higher in ethnic minority groups.[64]
- It is estimated that by 80 years old, 40-50% of South Asian and African Caribbean men and women will have T2DM.[65]
- These groups are significantly more likely to be diagnosed before the age of 40.[66]
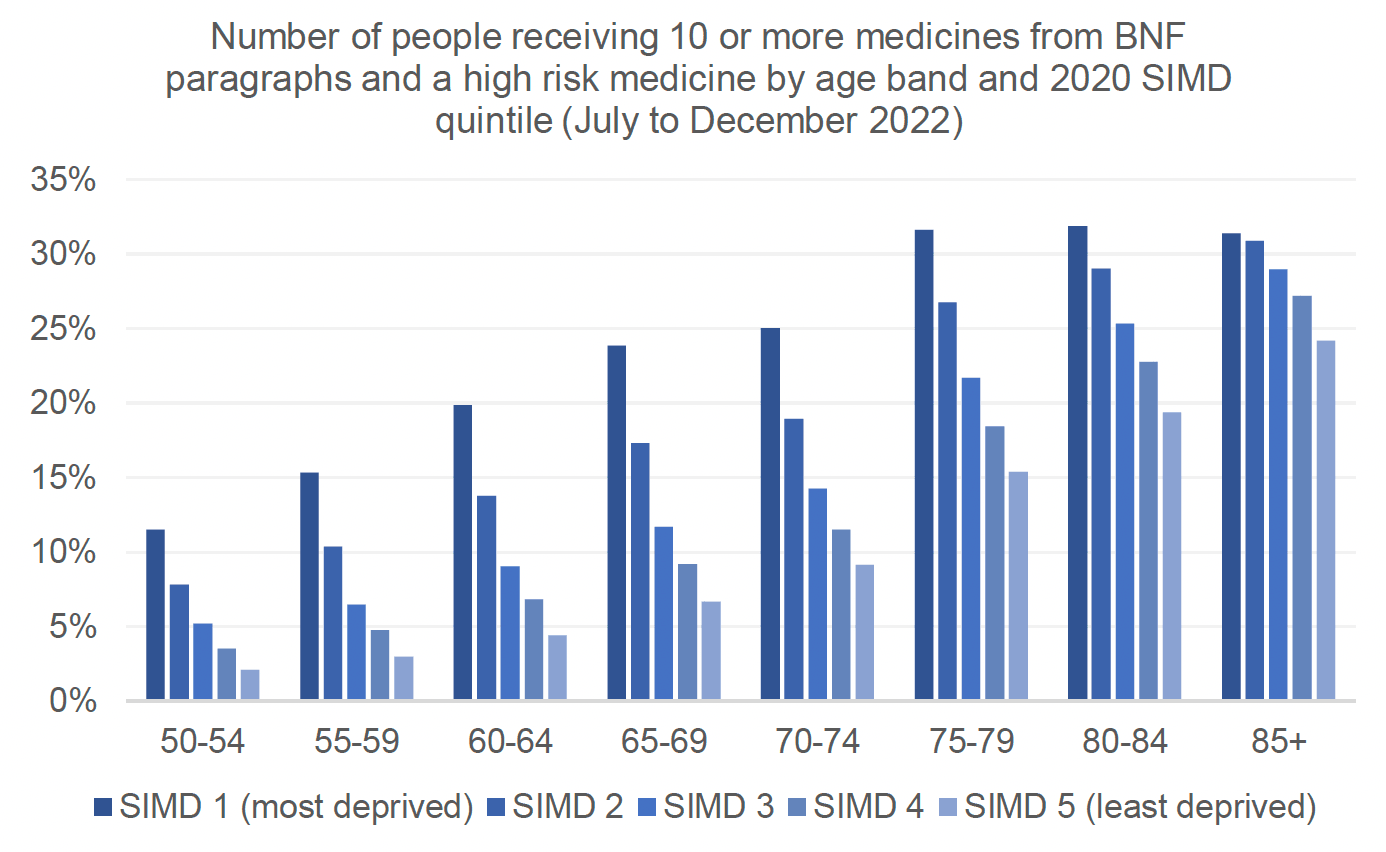
It is also important to note that people from deprived communities take more medicines than those from less deprived communities and therefore the medication treatment burden for these individuals is higher. Chart 8 shows comparison of medication burden across age groups, by level of deprivation.
Inequity in access to care and treatment
A number of cultural barriers have been identified that impact on minority ethnic groups accessing diabetes services, which will include regular review of prescribing and monitoring.[67] These include:
- strong adherence to cultural norms
- religious beliefs
- linguistic diversity/language barriers
- health literacy levels
- low accessibility of culturally appropriate service and
- ‘low concordance with western professional advice’[67]
Service design - improving equity of care and outcomes for disadvantaged groups
The design and delivery of T2DM services can advance equity and inclusion for those most disadvantaged. As reported in Diabetes: my information, my support, digital access may not be suitable for all.
“Variable access to the internet and weak telephone signal mean that I can have difficulty in getting online or using a video call. The question of alternatives to digital access have to be available for those in digital poverty.” (Person with lived experience, from Diabetes; my information, my support)[11]
The following table outlines approaches that can support improved care and outcomes for disadvantaged groups.
Table 9: Approaches to support improved care and outcomes for disadvantaged groupsApproach:
Human Rights Based Approach (HRBA)
Principle:
Adapted from Scottish Human Rights Commission
Aligns to the values of realistic medicine and person-centred care
Actions:
Service design targeted at the people who need it most, through
- Participation
- Accountability
- Non-discrimination
- Empowerment
- Legality
Approach:
Cultural competency
Principle:
Understanding the key issues relating to culture that influence the access to and experiences of care.
Actions:
Health workers should gain culturally competent knowledge of different cultures.
Information should be available in individuals’ first language to support their treatment
Discussion of medication taking during Ramadan.
Consider adaptations to ethnic foods to empower patients to adopt healthy lifestyles rather than to abandon familiar foods.
Approach:
Trauma-informed service design[68]
Principle:
Traumatic events are more frequently experienced by people in low socio-economic groups and from black and minority ethnic communities.
Actions:
Everyone in the Scottish workforce has a role to play in understanding and responding to people affected by trauma. Some will be specialists/enhanced workers, but all should be informed or skilled to respond to those affected by trauma.
Approach:
Co-designed services
Principle:
Co-designed services are more likely to be acceptable to both providers and end users, and therefore adopted and sustained.
Actions:
Ensuring underrepresented and disproportionately affected groups are part of this process and development.
Approach:
Digital inclusion
Principle:
In line with the Digital Health and Care Strategy[69]
Principle:
Availability of digital services, such as My Diabetes My Way will undoubtedly improve service access, engagement and self-management.
Actions:
Include individuals at the heart of digital transformation of services.
Ensure the infrastructure exists in Health Boards to digitize services.
Approach:
Others
Actions:
- Impact assessments
- Links to wider determinants of health
Contact
Email: EPandT@gov.scot