Type 2 Diabetes Mellitus - quality prescribing strategy: improvement guide 2024 to 2027
This quality prescribing guide is intended to support clinicians across the multidisciplinary team and people with Type 2 Diabetes Mellitus (T2DM) in shared decision-making and the effective use of medicines, and offers practical advice and options for tailoring care to the needs and preferences of individuals.
2. How can we reduce harm from polypharmacy?
By ensuring the right person receives the right treatment for their condition with the appropriate clinician, harm from polypharmacy can be reduced. This is achieved through regular medication review and shared decision-making, considering all medicines prescribed, including those bought by the person and any traditional and complementary therapies.
Appropriate polypharmac[8] is present, when:
a. all drugs are prescribed for the purpose of achieving specific therapeutic objectives that have been agreed with the individual;
b. therapeutic objectives are being achieved or there is a reasonable chance they will be achieved in the future;
c. medication therapy has been optimised to minimise the risk of adverse drug reactions (ADRs); and,
d. the individual is motivated and able to take all medicines as intended.
Inappropriate polypharmacy is present, when one or more drugs are prescribed that are not or no longer needed, either because:
a. there is no evidence-based indication, the indication has expired, or the dose is unnecessarily high;
b. one or more medicines fail to achieve the therapeutic objectives they are intended to achieve;
c. one, or the combination of several medicines drugs cause inacceptable adverse drug reactions (ADRs), or put the individual at an unacceptably high risk of such ADRs; or
d. the person is unable or not willing to take one or more medicines as intended.
Polypharmacy in diabetes
Polypharmacy is common for those living with T2DM. In addition to management of hyperglycaemia, there is often the prevalence of comorbidities including:
- atherosclerotic cardiovascular disease (ASCVD)
- chronic kidney disease (CKD)
- heart failure (HF)
- depression
National Therapeutic Indicator
Polypharmacy in diabetes: Number of people prescribed three or more categories of diabetes medication as a percentage of all people prescribed an anti-diabetic drug.
Chart 3 below shows the increasing trend of people being prescribed multiple medicines for diabetes. While this prescribing will very often be appropriate polypharmacy, the chart serves to demonstrate the quantity of medicines prescribed.
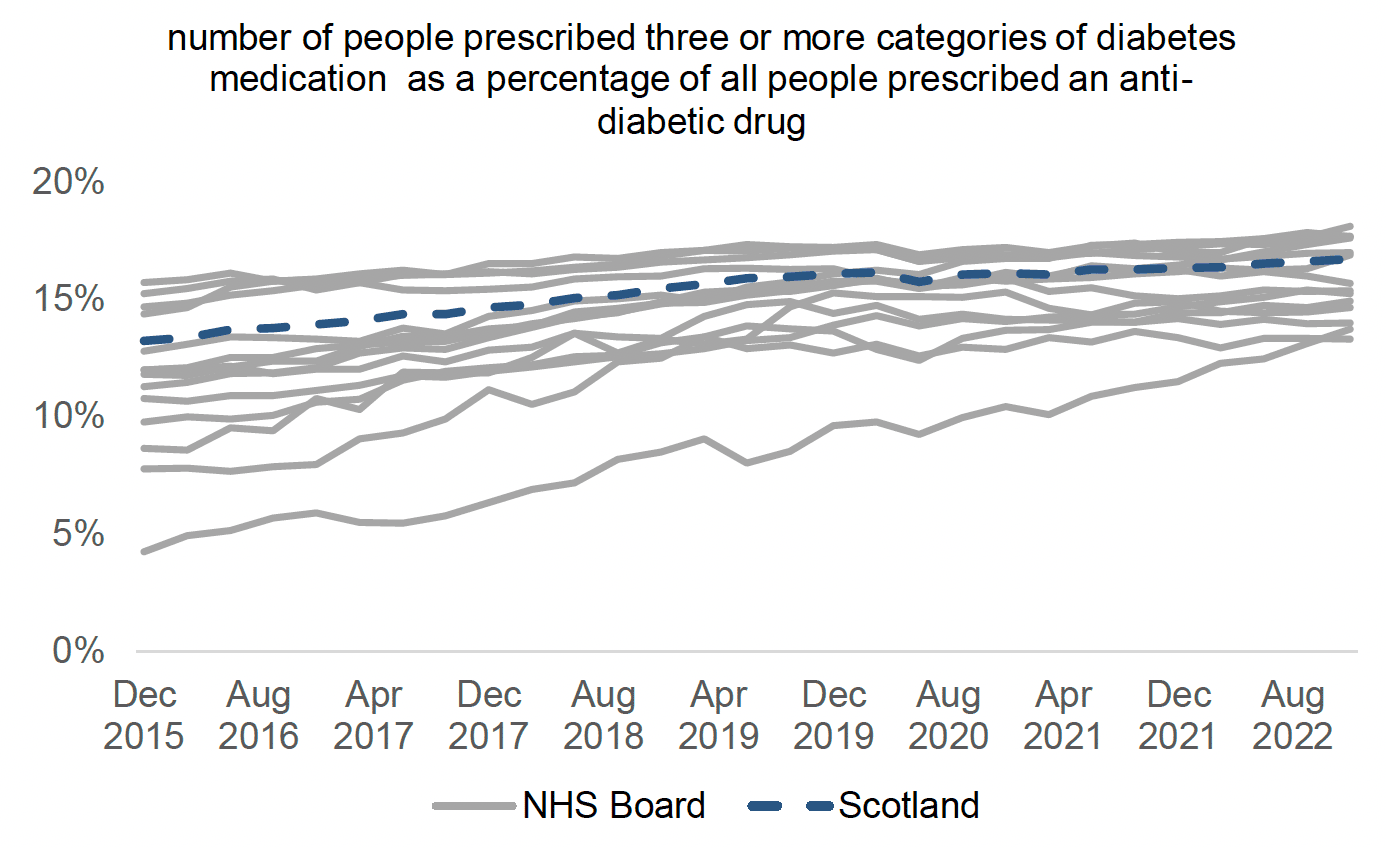
Variation between national Health Boards is reducing. Boards should consider their position in this data and the steps required to ensure that polypharmacy in diabetes is appropriate. More information and details are available in sections 12 and 14, and on the Public Health Scotland website.
A polypharmacy review (following the 7-Steps approach) should ensure optimal management of T2DM and other conditions. It should include addressing aggravating lifestyle factors and consideration of the most appropriate medication at the right dose, with regular review. The following 7-Steps are intended as a guide to structure the review process.
Step 1: Aim: What matters to the patient?
Step 2: Need: Identify essential drug therapy.
Step 3: Need: Does the patient take unnecessary drug therapy?
Step 4: Effectiveness: Are therapeutic objectives being achieved?
Step 5: Safety: Is the patient at risk of ADRs or suffers actual ADRs?
Step 6: Sustainability: Is therapy cost-effective and environmentally sustainable?
Step 7: Person-centred: Is the person willing and able to take therapy as intended?
The 7-Steps to appropriate polypharmacy demonstrate that the review process is not in fact a linear single event, but cyclical, requiring regular repeat and review (see Figure 2 below). The circle is centred on what matters to the individual, ensuring they are provided with the right information, tools and resources to make informed decisions about their medicines and treatment options. It should be used at both initiation and review of medicines.
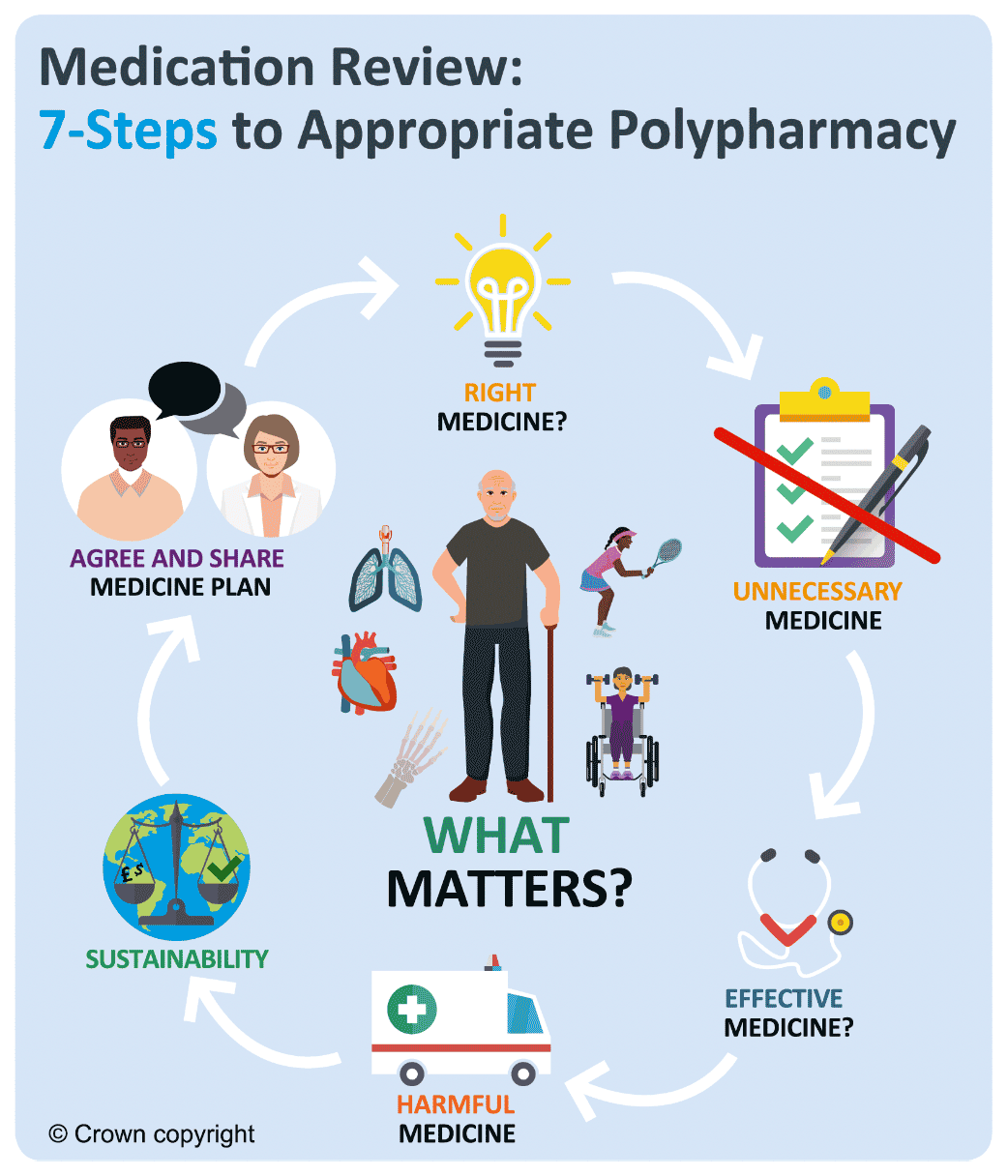
Graphic text below:
Medication Review: 7-Steps to Appropriate Polypharmacy
- What Matters?
- Right Medicine?
- Unnecessary Medcine
- Effective Medcine
- Harmful Medcine
- Substainability
- Agree and Share Medicine Plan
See Table 2 below for an overview of key considerations at each step for an individual with T2DM.
Table 2: 7-Steps medication review processStep 1.
Aims
What matters to the individual about their condition(s)?
Process:
Review diagnoses and consider:
- therapeutic objectives of drug therapy
- management of existing health problems
- prevention of future health issues, including lifestyle advice
Person specific issues to address:
- to prevent long-term diabetes complications
- is there co-existing cardiovascular or renal disease?
- maintain good mental health
Step 2.
Need
Identify essential drug therapy
Process:
Identify essential drugs (not to be stopped without specialist advice*)
- drugs that have essential replacement functions Drugs to prevent rapid symptomatic decline
* with advice from healthcare professional with specialist interest
Person specific issues to address:
- insulin
- sulfonylurea for immediate management of hyperosmolar symptoms
Step 3.
Does the individual take unnecessary drug therapy?
Process:
Identify and review the continued need for drugs
- what is medication for?
- with temporary indications
- with higher than usual maintenance doses
- with limited benefit/evidence for use
- with limited benefit in the person under review (see Drug efficacy & applicability (NNT) table)
Person specific issues to address:
- SU for immediate reduction of symptomatic hyperglycaemia
- SU for long term use; pioglitazone and gliptins less effective than other sub-classes
- co-prescribing of DPP-4i and GLP-1RA not appropriate, stop DPP-4i.
Step 4.
Effectiveness
Are therapeutic objectives being achieved?
Process:
Identify the need for adding/intensifying drug therapy to achieve therapeutic objectives
- to achieve symptom control
- to achieve biochemical/clinical targets
- to prevent disease progression/exacerbation
- is there a more appropriate medication to achieve goals?
Person specific issues to address:
- consider target dependent on other factors, e.g., frailty?
- SGLT-2i and GLP-1RA have positive ASCVD and CKD outcome data
- if co-existing ASCVD or CKD, SGLT-2i or GLP-1RA may be more appropriate than gliptin or pioglitazone.
Step 5.
Safety
Does the individual have or is at risk of ADR/ Side effects?
Does the person know what to do if they’re ill?
Process:
Identify individual safety risks by checking for
- appropriate individual targets
- drug-disease interactions
- drug-drug interactions (see ADR table)
- monitoring mechanisms for high-risk drugs
- risk of accidental overdosing
Identify adverse drug effects by checking for
- specific symptoms/laboratory markers
- cumulative adverse drug effects (see ADR table)
- drugs used to treat side effects caused by other drugs
Medication Sick Day guidance
Person specific issues to address:
- if frail, is HbA1c less than 48mmol/mol. Reduce therapy
- check renal function and dose adjust where necessary, e.g., metformin reduce dose if eGFR <45ml/min and stop if eGFR <30ml/min
- women of child-bearing age – metformin and insulin are suitable in pregnancy but others are not. Individuals should be made aware of this.
- temporarily stop SGLT-2i, metformin and SU during dehydration illness
Step 6.
Sustainability
Is drug therapy cost-effective and environmentally sustainable?
Process:
Identify unnecessarily costly drug therapy by
- considering more cost-effective alternatives, safety, convenience -
Consider the environmental impact of
- inhaler use
- single use plastics
- medicines waste
- water pollution
Person specific issues to address:
- metformin modified release less cost effective than standard release, but appropriate if previous gastrointestinal intolerance.
- if insulin therapy required, are reusable pens and cartridges suitable, rather than disposable pens?
Step 7.
Person-centredness
Is the person willing and able to take drug therapy as intended?
Process:
Does the person understand the outcomes of the review?
- Consider teach-back
Ensure drug therapy changes are tailored to individual’s preferences. Consider
- is the medication in a form they can take?
- is the dosing schedule convenient?
- what assistance is needed?
- are they able to take medicines as intended?
Agree and communicate plan
- discuss and agree with the individual/carer/welfare proxy therapeutic objectives and treatment priorities
- include lifestyle and holistic management goals
- inform relevant health and social care providers of changes in treatments across the transitions of care
Key concepts in this case
- …
- ...
See case studies for examples of applying the 7-Steps medication review process.
Environmental impact of polypharmacy and healthcare
The healthcare industry is increasingly asked to account for the negative environmental impact generated through providing medical care.
In Scotland, every ten days a 10-tonne truck of medicines waste (from community and hospital pharmacies) is transported for incineration. There are associated costs for incineration; travel costs and the environment impact (see Figure 3 below) and in addition, direct costs of unused medication.
There are many factors which contribute to medicines waste and a Department of Health and Social Care report in September 2021[13] showed that overprescribing is commonplace. Evidence is limited, but the review estimates that it is possible that at least 10% of the total number of prescription items in primary care need not have been issued.
This guidance supports reducing inappropriate prescribing through review of medication for those with long term health conditions. This includes promoting person-centred decision-making; providing guidance and support for clinicians and suggesting alternatives to medicines, where appropriate, such as physical, social activities and lifestyle change.

Graphic text below:
Medicine waste disposal in Scotland
- 365 tonnes of waste are incinerated every year
- this disposal alone costs £0.25 million a year
- with a CO2 equivelance of 28 car journeys around the world (700,000 miles)
The Royal Pharmaceutical Society policy, ‘Pharmacy’s role in climate action and sustainable healthcare’,[14] identifies medicines as contributing 25% of carbon emissions in the NHS.
This can be reduced by:
- improving prescribing and medicines use
- tackling medicines waste
- preventing ill health
- improving infrastructure and ways of working
With regular medication reviews to address inappropriate polypharmacy in T2DM (and other comorbidities), the environmental impact can be reduced. Small changes can have an impact, such as considering the use of re-useable insulin pens and cartridges rather than pre-filled pens, which can have a lower CO2 footprint as well as reducing plastic waste. The RCGP[15] has identified that prescribing accounts for over 60% of general practice’s carbon footprint.
The Sustainable Markets Initiative (SMI) established in 2020 identify seven levers to reduce carbon emissions in care pathways. Those that relate to diabetes include.[16]
1. Preventing disease onset – dietary and lifestyle management to prevent and manage T2DM
2. Diagnosing early – to treat earlier and prevent long-term complications
3. Optimising disease management – utilising newer therapies has positive long-term outcomes and reduces incidence of ASCVD, CKD and HF – see example below
4. Improving the efficiency of interventions – as above
5. Delivering care remotely or closer to home when appropriate – digital innovations
6. Using lower-emission treatments – re-usable insulin pens
It is estimated that an individual with T2DM and late-stage CKD, requiring dialysis several times per week, will have associated carbon emissions 70 times of someone managed with insulin, and 200 times those managed with oral hypoglycaemic therapies.
Of 100 individuals with pre-diabetes, 15% will develop cardiovascular or renal disease, accounting for 50% of the carbon emissions of this group.
Therefore prevention of and effective management of T2DM will have a positive environmental impact alongside potential reduction in healthcare utilisation.
Pharmaceuticals in wastewater
The Royal Pharmaceutical Society's Sustainability Policies also point to the occurrence of pharmaceuticals in the environment. Every oral dose of a medicine taken is either excreted unchanged or converted to a metabolite with 30-100% entering our wastewater system which cannot currently remove all traces. The occurrence of pharmaceuticals in the environment is of global concern, and there is already evidence that they can affect aquatic wildlife, increase microbial resistance and enter the human food chain.
Evidence has already identified metformin and sitagliptin in waterways across the world, and further studies are needed identify the wider environmental impact of other anti-diabetic medication. These two examples highlight the importance of preventing diabetes and that all prescribing and review of medication should consider environmental impact and sustainability.[17],[18],[19],[20]
Contact
Email: EPandT@gov.scot