Type 2 Diabetes Mellitus - quality prescribing strategy: improvement guide 2024 to 2027
This quality prescribing guide is intended to support clinicians across the multidisciplinary team and people with Type 2 Diabetes Mellitus (T2DM) in shared decision-making and the effective use of medicines, and offers practical advice and options for tailoring care to the needs and preferences of individuals.
6. Why is it important to consider ASCVD, CKD and HF risk?
Comorbidities must be considered, especially atherosclerotic cardiovascular disease (ASCVD), heart failure (HF) and chronic kidney disease (CKD) which can increase mortality. Newer therapies have positive outcomes for people with diabetes and these comorbidities, thus reducing the long-term complications and associated personal and financial costs.
With the increasing evidence of positive long-term outcomes independent of glycaemic control from the newer agents, the expert working group considered the place of sodium-glucose co-transporter-2 inhibitor (SGLT-2i*) and glucagon-like peptide 1 receptor agonist (GLP-1RA) in therapy, recommending their use in NHS Scotland, considering:
- increasing evidence of positive long-term outcomes independent of glycaemic control
- incorporation of SGLT-2i and GLP-1RA into guidelines from the American Diabetes Association (ADA), the European Association for the Study of Diabetes (EASD)[3] and more recently NICE 28[2]
- duration of time since publication of SIGN 154,[1] and
- prescribing in frailty (section 9)
- licensed indication
People with T2DM with high risk of, or established atherosclerotic cardiovascular disease (ASCVD) and heart failure
Established atherosclerotic cardiovascular disease (ASCVD), heart failure (HF) or chronic kidney disease (CKD) are important indications for use of the newer therapies of SGLT-2i and GLP-1RA. There is good evidence from large randomised clinical trials that people with a history of ASCVD, CKD and/or HF benefit from glucose-lowering treatment with SGLT-2i* and GLP-1RA.[42],[3] A recent population-wide study showed that more than 70% of people with T2DM in Scotland currently on non-pharmacological/ lifestyle management, or metformin monotherapy, have ASCVD, CKD or HF[43] (see NTIs section 14). Trial evidence is readily available online and more continues to emerge.
See Figure 7 – Summary algorithm of prescribing choices in T2DM, based on ADA and EASD[3], and NICE[2] recommendations.
Cardiovascular disease and risk factors
Cardiovascular disease risk is an important factor to consider for those with T2DM. Treatment selection for hyperglycaemia should consider whether a person has:
- established ASCVD (ischaemic heart disease, stroke); or
- cardiovascular risk factors of:
- QRISK2 more than 10% in adults aged 40 and over (or other validated tool); or
- a clinically assessed elevated lifetime risk of cardiovascular disease (defined as the presence of one or more of the below cardiovascular risk factors in someone under 40).
- hypertension;
- dyslipidaemia;
- smoking;
- obesity; or
- family history (in a first-degree relative) of premature cardiovascular disease.[44]
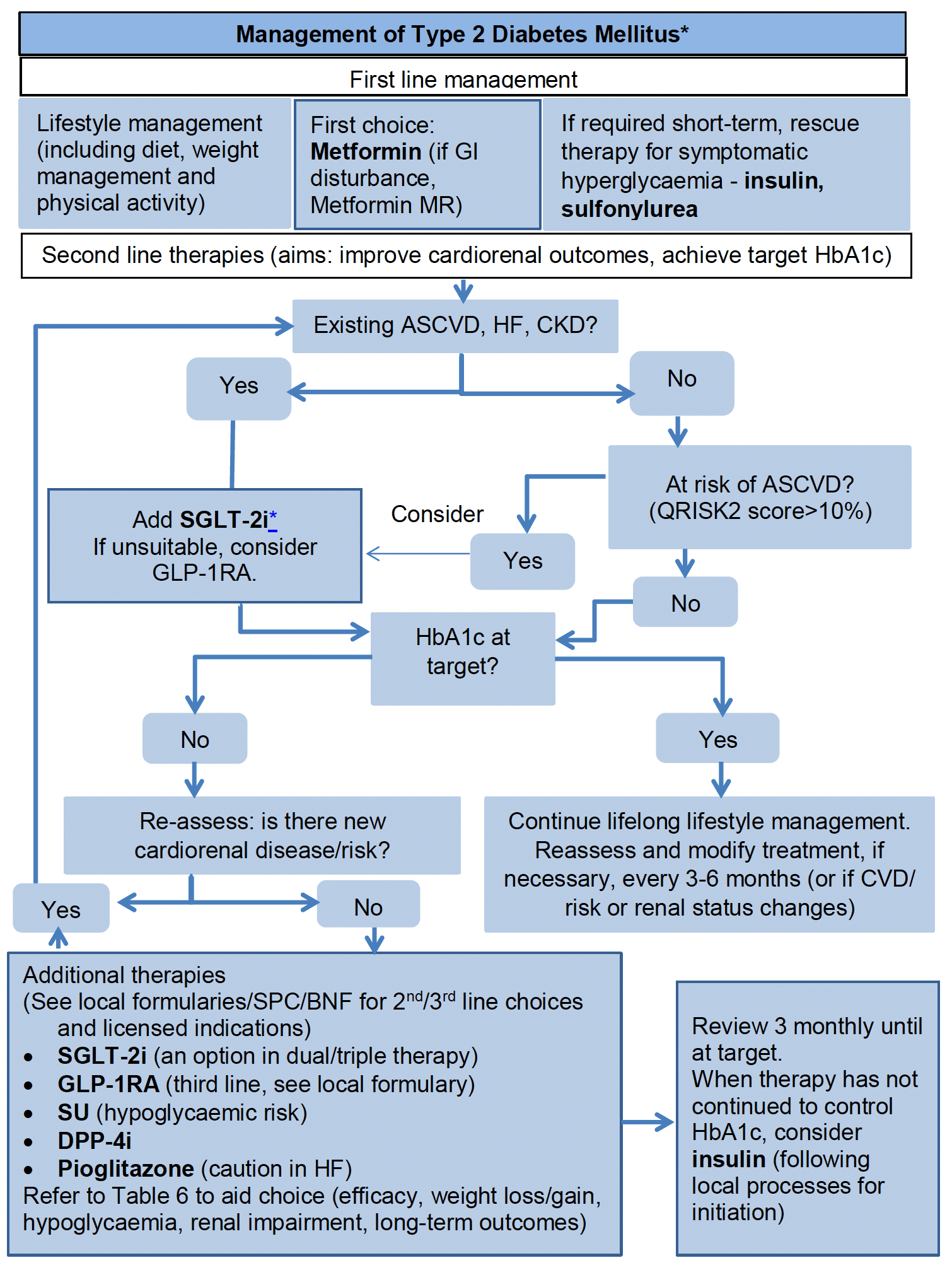
Graphic text below:
First line management:
- Lifestyle management (including diet, weight management and physical activity)
- First choice: Metformin (if GI disturbance, Metformin MR)
- If required short-term, rescue therapy for symptomatic hyperglycaemia - insulin, sulfonylurea
Second line therapies (aims: improve cardiorenal outcomes, achieve target HbA1c):
- Existing ASCVD, HF, CKD?
- Yes - Add SGLT-2i* If unsuitable, consider GLP-1RA [then skip to HbA1c at target question below]
- No - At risk of ASCVD? (QRISK2 score>10%)
- Yes – consider add SGLT-2i* If unsuitable, consider GLP-1RA
- No - HbA1c at target?
- Yes - Continue lifelong lifestyle management. Reassess and modify treatment, if necessary, every 3-6 months (or if CVD/ risk or renal status changes)
- No - Re-assess: is there new cardiorenal disease/risk?
- No - Additional therapies (See local formularies/SPC/BNF for 2nd/3rd line choices and licensed indications) SGLT-2i (an option in dual/triple therapy) GLP-1RA (third line, see local formulary) SU (hypoglycaemic risk) DPP-4i Pioglitazone (caution in HF) Refer to Table 6 to aid choice (efficacy, weight loss/gain, hypoglycaemia, renal impairment, long-term outcomes)
→ Review 3 monthly until at target.
When therapy has not continued to control HbA1c, consider insulin (following local processes for initiation)
- Yes – return to start of flow chart
Definitions:
ASCVD: MI, stroke, any revascularisation procedure, CVD (including transient ischaemic attack, unstable angina, coronary artery disease, amputation)
HF: chronic heart failure (excluding acute)
CKD: <60ml/min with ACR >30mg/mmol
*Based on NICE NG28, ADA/EASD and SIGN
Abbreviations:
SGLT-2i: sodium-glucose co-transporter-2 inhibitor
GLP-1RA: glucagon-like peptide 1 receptor agonist
DPP-4i: dipeptidyl peptidase-4 inhibitor
SU: sulfonylurea
Increased risk of eDKA with SGLT-2i
See MHRA Drug Safety Update April 2016 [47], March 2020 [48]
See section 6 *
Any modifiable risk factors for ASCVD (hypertension, hyperlipidaemia, smoking, obesity) should be addressed. For useful links to lifestyle information see List 1.
Prescribing choices
1. Metformin remains first line.
2. SGLT-2i should be prescribed for individuals with established ASCVD,[43] heart failure or chronic kidney disease. Individuals at high risk who have not yet developed these complications may also benefit.
3. A shared decision-making approach is recommended, considering:
- beneficial effects e.g. weight loss, extent of glucose-lowering efficacy
- adverse effects e.g. in relation to the degree of hyperglycaemia, or the risk of hypoglycaemia; DKA
- preferences e.g. route of administration, oral verses injectable, frequency of administration, daily or weekly
SGLT-2i contra-indications/cautions:
- people 75 years and older are at increased risk of volume depletion
- not recommended for initiation when eGFR is <15 ml/min/1.73m2
- have less glucose-lowering efficacy with eGFR <45 ml/min/1.73m2
- should be avoided in those with:
- factors predisposing to DKA/eDKA
- pancreatic insufficiency
- drug or alcohol misuse disorder
- a low/ultra-low carbohydrate or keto diet
- excessive alcohol consumption
- frequent bacterial urinary tract infections or genitourinary yeast infections
- low bone density or high risk for falls/fractures
- current foot ulceration.
- factors predisposing to DKA/eDKA
* Increased incidence of euglycaemic diabetic ketoacidosis
With increasing use of SGLT-2i, there has been an increased incidence of eDKA in addition to DKA. Therefore the MHRA[45] has issued the following advice:
- use SGLT-2i with caution in those with risk factors for DKA, (including a low beta cell reserve, conditions leading to restricted food intake or severe dehydration, sudden reduction in insulin, increased insulin requirements due to acute illness, surgery or alcohol misuse), and discuss these risk factors with individuals
- test for raised ketones in individuals with signs and symptoms of DKA, even if glucose levels are near-normal
- discontinue treatment if DKA is suspected or diagnosed
- do not restart treatment with any SGLT-2i in those who experienced DKA during use, unless another cause for DKA was identified and resolved
- during and after surgery or during acute serious illness:
- interrupt sodium-glucose co-transporter 2 (SGLT2) inhibitor treatment in patients who are hospitalised for major surgical procedures or acute serious medical illnesses
- monitor ketones during this period – measurement of blood ketone levels is preferred to urine
- restart treatment with the SGLT2 inhibitor once ketone values are normal and the patient’s condition has stabilised.
Furthermore emerging advice[46],[47] regarding the period of treatment interruption is:
- For three days prior to planned surgery (four days if prescribed ertugliflozin), (or immediately if unplanned surgery) and for a further three days after surgery
- During acute illness, e.g. diarrhoea, vomiting (see sick day guidance)
Individuals considering an SGLT-2i should be advised about the risks of eDKA associated with a low/ultra-low carbohydrate or keto diet.
See Case Study 3.
Due to the different licences for SGLT-2i* (and GLP-1RA), prescribers should familiarise themselves with the indications and contra-indications as well as interactions listed in the BNF and/or the Electronic Medicines Compendium before initiating therapies. Where there is no difference between drugs within a class, the most cost-effective drug should be chosen, and NHS boards should consider their formulary choices.
The recent NICE[2] guideline ‘Type 2 Diabetes in adults: management’ supports the introduction of SGLT-2i* as first-line therapy with metformin, if the individual has chronic heart failure or established atherosclerotic cardiovascular disease. These drugs should be started sequentially, with metformin first, then once tolerability is established, the SGLT-2i* can be started.
Cardiovascular disease and risk should be reviewed regularly and may require a change/addition to therapy. See Figure 7.
People with T2DM and chronic kidney disease (CKD)
T2DM is a risk factor for developing CKD and therefore monitoring for CKD should be part of the annual review. Frequency of monitoring is dependent on the classification and stage of CKD.
Classification of CKD[48] is based on a combination of glomerular filtration rate (GFR) and albumin to creatinine ratio (ACR). The risk of adverse outcomes increases as CKD category decreases (GFR) or as ACR increases. This happens independently but with greater risk if both are present (see Table 7).
Prescribing choices
Table 8 outlines prescribing choices for people with CKD.
| Treatment options | ACR category A1: normal to mildly increased (less than 3 mg/mmol) | ACR category A2: moderately increased (3 to 30 mg/mmol) | ACR category A3: severely increased (over 30 mg/mmol) |
|---|---|---|---|
| ACEI/ARB to highest tolerated dose | No | Yes | Yes |
| SGLT-2i (dependent on licence) in addition to ACEi/ARB | No | Consider | Offer |
Offer an ARB or an ACE inhibitor if ACR is 3mg/mmol or more (titrated to the highest licensed dose that the individual can tolerate). This is a lower ACR threshold than for those without diabetes.
If the ACR is between 3-30mg/mmol, consider offering an SGLT-2i* (dependent on licence) in addition to the highest tolerated dose of ACEi or ARB.
If the ACR is over 30mg/mmol, offer an SGLT-2i* (dependent on licence) in addition to the highest tolerated dose of ACEi or ARB.
N.B. Consider the appropriateness of therapy with other factors such as increasing frailty, due to risks of side-effects, e.g. hypotension and falls, against time to realise benefit of therapy.
See case study 4.
Other medication for the treatment of T2DM in CKD
Consider dose reduction in response to reducing renal function in:
- Metformin;
- SGLT-2i*;
- GLP-1RA;
- DPP-4i; and
- ACEi, ARBs, diuretics and NSAIDs.
Note that people treated with medication that can affect kidney function during acute dehydrating illness (with or without existing renal disease) should be issued with Medication sick day guidance to prevent acute kidney injury.
National Therapeutic Indicator
Individuals with T2DM and existing atherosclerotic cardiovascular disease (ASCVD) who may benefit from treatment with SGLT-2i and/ or GLP-1RA.
This indicator (see Chart 5) should have a high level of SGLT-2i and/or GLP-1RA prescribing, indicating good practice, with suitable patients receiving appropriate medication.
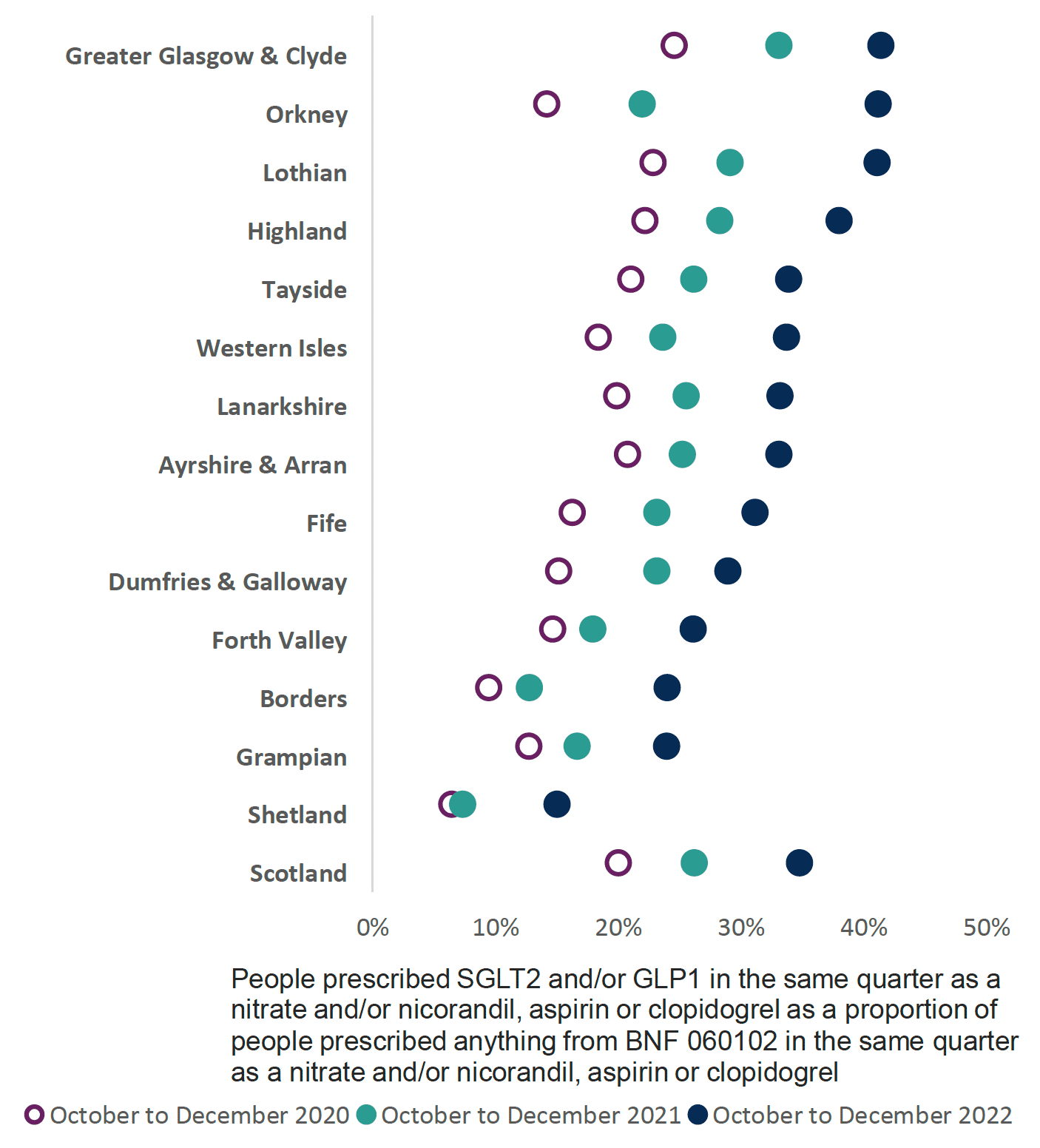
Chart 5 identifies individuals prescribed SGLT-2i and/or GLP-1RA in the same quarter as a nitrate and/or nicorandil, aspirin or clopidogrel as a proportion of people prescribed anything from BNF 060102 in the same quarter as a nitrate and/or nicorandil, aspirin or clopidogrel. This surrogate marker indicates there is a proportion of those with T2DM who may benefit from treatment with SGLT-2i or GLP-1RA, irrespective of glycaemic control.
Although the indicator is limited to ASCVD, there will be others with chronic heart failure (cHF) and CKD, who would similarly benefit.
The Scottish Therapeutics Utility (STU) tool available in all GP practices enables identification of those with T2DM and ASCVD, cHF and/or CKD (see section 12).
Due to the change in prescribing guidance, clinicians should identify individuals who would benefit from prescribing of SGLT-2i* or GLP-1RA. These include people:
- with T2DM and existing CVD and cHF;
- at high risk of CVD; and
- with T2DM and chronic kidney disease, based on eGFR and elevated ACR values.
These identified individuals should have all prescribed medicines reviewed to ensure their doses are appropriate for the degree of renal impairment.
People with T2DM with no ASCVD, HF, CKD
There will be individuals with T2DM, who are not at risk of or do not have ASCVD, cHF or CKD. For those individuals consider:
- whether weight loss or minimising risk of hypoglycaemia is a priority for the individual
- where weight loss or minimising weight gain is a priority, SGLT-2i* and GLP-1RA remain appropriate therapies in line with local guidance
- where minimising the risk of hypoglycaemia is a priority, GLP-1RA, SGLT-2i* and DPP-4i are suitable second line therapies
- DPP-4i and sulfonylureas are also acceptable second line therapies either used alone or in combination, considering the following:
- the degree of hyperglycaemia (sulfonylureas more efficacious in the short term)
- potential adverse effects (e.g. DPP-4i's are not associated with a risk of hypoglycaemia or weight gain)
- sulfonylureas may have particular benefit in steroid-induced diabetes and in individuals with normal or low BMI and T2DM (Type 1 diabetes must be excluded in such individuals)
Other agents (e.g. thiazolidinediones, acarbose) are now rarely used in treatment.
See case study 2.
Ongoing review for all with T2DM
At each review consider:
- lifestyle and diet advice (see List 1 for resources), reinforced with an assessment of the individual’s current risk factors.
- an assessment of cardiovascular and renal risk with:
- blood pressure
- lipids and
- smoking status
- glycaemic control
These should all be treated in line with respective treatment targets.
Review 3-6 months after initiating therapy or amending treatment. A significant proportion of individuals with T2DM continue to have sub-optimal diabetes and cardiovascular management. While ensuring timely review can be challenging, it is important to guard against clinical inertia and the long-term sequelae of suboptimal management (see Figure 7).
Contact
Email: EPandT@gov.scot