Scottish Breast Screening Programme: major review
Major review of the Scottish Breast Screening Programme.
Technology & Equipment
Breast Screening Digital Strategy
The Review Group discussed and supported the approach outlined in Scotland's Digital Strategy for Screening (see Appendix 9). The digital strategy is focused on the Scottish Screening Committee's strategic objectives set out in the 2018 screening review[19]. These are:
- Person centred approach with an increased level of service delivered consistently, putting people at the heart of decision making.
- To make screening more accessible, giving people the capabilities to enable them to have a greater role in managing their own health.
- To break down barriers to participation in the screening programmes and to address inequalities in the service.
- Making better use of data as an evidence base to improve planning as well as operational performance.
- Improve the performance of the screening programmes: better quality assurance; reduced clinical risk, and reduction in process time from screening to treatment.
- Improve outcomes through improved governance, accountability and better coordination of delivery of care.
The digital strategy and roadmap are driven by screening service needs and are designed to support and enable change. A number of key initiatives are being taken forward to support modernisation and development of the breast screening service. These include: cross-health board breast image reading/reporting; a Breast Screening PACS upgrade; current work to ensure breast screening mobile units are 4G/5G connected to allow online working; the development of a text appointments reminder system; the development of a Screening Intelligence Platform to improve data linkage, visualisation and reporting (further details in section 11 of this report); supporting the development of AI in breast screening mammography; and the Proof of Concept development of a Digital channel (screening App) to support screening interactions – potentially from online booking of appointments, reminders, communication, to health promotion messages.
The Strategic Case for Artificial Intelligence in Breast Screening Mammography
In Scotland, AI in Mammography is currently being tested by the Industrial Centre for Artificial Intelligence Research in Digital Diagnostics (iCAIRD) collaborative project. The mammography AI project within iCAIRD is the primary exemplar project for iCAIRD in Grampian. The project assesses the generalisability, performance, and usability of the Mia algorithm which is the AI software developed by Kheiron Medical Technologies, a collaborative partner within iCAIRD. In screening, the ambition is to utilise AI as an independent image reader, replacement one human reader in our current double-read system.
The outline strategic case for AI in breast screening mammography has been developed by the review team with the support of colleagues from across the service and from within iCAIRD. As part of this, a workshop session was held with the Review Group focussed on building the vision for Artificial Intelligence in screening mammography in NHS Scotland.
The strategic case outlines the development of AI in this field, the evidence and the evaluation work underway in Scotland; outlines the related workforce risk in Scotland; illustrates the potential benefits and the main areas of risk that will be monitored; indicates initial work on the views of women attending screening; describes the Scottish Breast Screening Programme's readiness to potentially adopt AI in screening mammography (subject to UK NSC policy decision); and describes the governance and development route forward and anticipated process to support further business case development. See Appendix 10 - The Strategic Case for Artificial Intelligence in Breast Screening Mammography.
As well as the process and pathway benefits outlined in the case, an estimate of the potential level of human resource (reader time sessions) saved annually is outlined at £527k, associated with the AI replacing one human reader. Within the current image reading resource there is a considerable reliance on a small number of individual readers who each read and report on a disproportionately high number of results. A significant proportion of radiology and advance practitioner staff, including these 'super readers' in the Scottish Breast Screening service, are now near to or at their retirement age, leaving the service vulnerable. The review conducted a survey of image reading undertaken in 2018/19 and 2019/20, showing that a significant proportion of the reader workload was covered either by staff who have now retired from the service, locum staff, or staff who have returned from retirement. This, alongside imaging workforce shortages, suggests an increasingly unsustainable future and reliance on locum cover, with the need to invest in more training for advanced radiographers. If AI is integrated into the reading process as an independent reader this will cover half of the screening image reading burden of approximately 1.72 million images read each year (4 images per woman screened giving circa 862k images annually in Scotland, each double-read).
Efficiency savings need to be offset against the costs of adopting and integrating AI into the screening pathway, which (given the current development status of research into practice) require to be estimated through the development of a full business case. Not all savings will be immediately cash releasing.
A development route forward has been designed, building on the work completed to date in the iCAIRD partnership, to conduct a POC (Proof of Concept) and real world service evaluation of Mia as an independent reader in the Breast Screening Service. This project will be taken forward by the Breast Screening Programme Board and led by Digital and Security in partnership with the iCAIRD collaborative and other partners.
Strategic recommendation: AI in breast screening mammography
The Review Group recommends that the Scottish Breast Screening Programme should progress to prospective evaluation and proof of concept for Artificial Intelligence in breast screening mammography, with a view to future adoption in the service subject to positive evaluation and formal UK NSC approval that AI can be used in the screening programme.
The Review Group approved the outline strategic case for Artificial Intelligence in breast screening mammography, and supported the further business case development process, to be led by DaS, with advice and support from the Breast Screening Programme Board.
Digital Breast Tomosynthesis (DBT)
Introduction and Background
Digital Breast Tomosynthesis (DBT) is an advanced form of breast imaging, which provides three-dimensional information of the breast (3D mammography). The SBSP currently uses conventional mammograms, in which two X-ray images are taken of the breast (top-to-bottom, and angled side-to-side) while the breast is compressed between a clear plastic paddle and an imaging detector. In DBT, the X-ray tube moves in an arc over the compressed breast, capturing multiple images, which can be synthesised into a set of 3D images by a computer.
DBT has been authorised for use within the English breast screening programme since 2016[20]. At that time, the NHS Cancer Screening Programmes announced that there was sufficient evidence to justify the use of the Hologic Dimensions DBT system in assessment in the NHS BSP. In Scotland, while two centres were involved in tomosynthesis trials, there has been no formal agreement to use DBT within the Scottish Breast Screening Programme. Currently there is very limited, inequitable access to tomosynthesis in the screening assessment service in Scotland, via units that were either research funded or symptomatic service funded. Four units across Glasgow and Tayside are tomosynthesis enabled, and in Grampian access is made to a tomosynthesis enabled unit located in the symptomatic service.
Health technology appraisal
The Scottish Health Technology Group (SHTG) has previously reviewed the use of DBT, at the request of Breast Screening Clinical Directors in Scotland. SHTG was asked to assess the clinical and cost effectiveness of digital breast tomosynthesis (DBT) compared with coned views for women who have been recalled from breast screening. SHTG found that DBT can be used to aid diagnosis for women who have been recalled from initial breast screening for further assessment. Most studies reviewed reported that diagnostic accuracy was comparable or superior to supplementary mammographic views (SMVs) which is the current standard of care. SHTG reported that it was not possible to comment on the cost effectiveness of DBT compared to SMV because no economic studies were identified. SHTG concluded that based on evidence that has been included in their rapid review, guidance from Public Health England has listed DBT as an option in women who have been recalled for assessment[21].
SHTG was also asked to assess the clinical and cost effectiveness of digital breast tomosynthesis (DBT) in addition to full-field digital mammography or synthetic 2D (FFDM or S2D) images, compared to FFDM alone for asymptomatic women attending for breast screening. SHTG concluded that while the evidence of diagnostic accuracy suggests that the addition of DBT to FFDM results in improved cancer detection, further information is required before the use of DBT can be justified in the screening population[22].
DBT is already available but disabled on most of the mammography machines in screening centres within NHS Scotland (as outlined in the mammography equipment replacement section of this report, below). The Scottish Breast Screening Programme (SBSP) should consider enabling DBT capability on a machine in each of the six breast screening centres in NHS Scotland, for use in women who have been recalled from breast screening for further assessment.
Review of the use of DBT in NHS Grampian
The Review Team asked the North East of Scotland Breast Screening Centre to retrospectively review utilisation of DBT in Grampian during 2018 and 2019 in breast screening patients. The team reviewed use of the Hologic DBT system they have access to, which is located in the breast symptomatic clinic. This is utilised for both symptomatic patients, and for additional assessment review of breast screening patients. Appendix 11 outlines the review findings. Patient outcomes were evaluated and actions proposed for future practice:
Due to limitations of distance to the symptomatic department, only a small proportion of screening assessment patients were referred for DBT (38 referred in 2018, 30 in 2019).
- The results show that there is a significant reduction in the necessity for further invasive tests and/ or MRI imaging.
- Fewer unnecessary tests has positive implications for the patient and is more cost effective for the breast screening centre.
- This review supports the use of DBT in women who have been recalled from breast screening for further assessment.
- We propose, in-line with Scottish Health Technology Group recommendations, that the Scottish Breast Screening Programme (SBSP) should consider enabling DBT use in the assessment setting in screening centres across NHS Scotland.
Benefits and Efficiencies
A number of benefits/efficiencies could be gained if DBT was introduced; these include:
- Reduction in the number of biopsies performed:
- Reduction in biopsy consumable costs (currently each mammotome stereotactic probe costs £200).
- Improved workflow in radiology and capacity creation in assessment clinics: Over time, all women attending for assessment may receive DBT as standard, thereby, minimising pre-assessment and identification of supplementary mammographic views to perform. This can take up to 1.5 hours per clinic by a Radiologist and would increase capacity for radiologists to read images and perform other duties.
- Improved workflow in radiography: with fewer additional views being required using DBT in both dense and non-dense breasts, workflow for radiographers could also be improved with less alteration of equipment to perform supplementary mammographic views. There is also potential for further role extension for Assistant Practitioners.
- Reduction in Radiation Dose: with reduction of supplementary mammographic views and less repeated images, it is anticipated there would be a reduction in radiation dose for participants.
It seems evident with the implementation of DBT that the assessment workflow would be improved and simplified, with the quality of service to women attending assessment clinics increased through reduced radiation and reduction of time in clinic. The potential cost efficiencies would also have a positive impact on radiologist time, creating radiology capacity to offset workforce risks described earlier in this report. The review attempted to ascertain the total demand for DBT in breast screening, however extrapolation from current use in Grampian would be unreliable given the limitations described in their review. The extent to which efficiency savings described above can support the implementation of DBT would require further analysis and forecasting, and would require to be provided within any agreed business case.
Procurement Considerations
Additional software and biopsy equipment would be required to support DBT implementation in screening centres within NHS Scotland.
The current framework costs are £50,000 per X-ray unit to enable DBT, therefore for an enabled unit in each centre this would give a total of £300K. The service costs for each unit enabled may also increase by approximately £4.5k p.a. A previous estimate considered the need for 5 DBT biopsy devices, currently at circa £20,000 per device.
It would be expected that a significant discount from the above indicative costs for licensing and ongoing maintenance would be achieved should a procurement for all centres together be taken forward. Discussion within the review has also considered the potential to link the enabling of DBT with x-ray unit replacement as part of a managed equipment replacement programme, as this is more cost effective. This should be further considered particularly for replacement of units now over 8 years old, and the larger group of units currently 6 – 8 years old.
The additional Picture Archiving and Communication Systems (PACs) image storage requirements associated with DBT will be minimal.
An initial period of training will be required for staff, albeit in some centres limited use is already made of DBT and therefore knowledge and application protocols on the pathway are already in practice. Additional Medical Physics resource has previously been estimated at 12 hours/week in the first year of implementation, reducing to 9 hours/week from year 2.
Strategic Recommendation
The Scottish Breast Screening Programme (SBSP) should consider enabling DBT for use in the assessment setting in screening centres across NHS Scotland. A business case should be developed by NSD, in collaboration with host NHS Boards, to realise the benefits and efficiencies identified. Consideration should be given to linking the enabling of DBT with x-ray unit replacement as part of a national managed equipment replacement programme, should this be agreed, and the route is more cost effective.
Mammography equipment replacement programme
Overview of the current inventory
In total there are 43 X-ray sets in use in the SBSP, including those co-located in joint screening / symptomatic departments. This total is inclusive of the 21x-ray units in the mobile fleet (and inclusive of the unit that covers servicing).
Since re-start of the programme in August 2020 following the Covid-19 related pause, 2 of the mobile units that were scheduled for replacement have remained in service to assist with capacity for recovery. This brings the current operational total to 23 (again, inclusive of the unit that covers servicing).
100% of X-ray sets are digital, providing Full Field Digital Mammography (FFDM).
Almost all units are from the same manufacturer, and most are the same model.
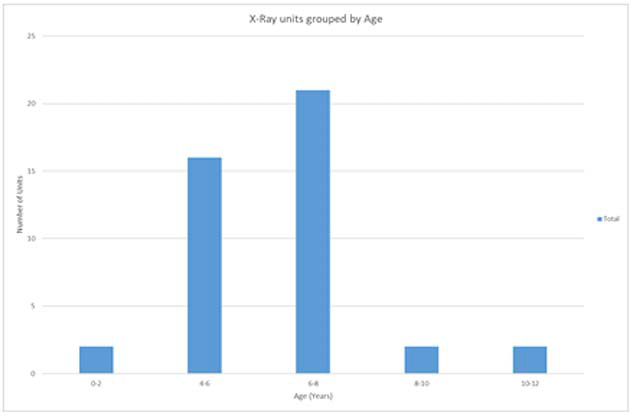
Almost half of the x-ray units are 6 – 8 years old, with 9% over 8 years old (Figure 1)[23].
Commonly accepted life for a diagnostic x-ray machine is ten years. Due to age, obsolescence and more intensive use, the service life of a mammographic x-ray machine used in the breast screening programme may be less than ten years[24].
Forty-two units are tomosynthesis ready but the functionality is not currently enabled, and therefore the machines are not used for tomosynthesis exposures. Four units in Glasgow and Tayside are tomosynthesis enabled, and in Aberdeen limited access is made to a tomosynthesis enabled unit located in the symptomatic service. Whilst this allows very limited, inequitable access to tomosynthesis in the screening service, tomosynthesis capability on these units is either research funded or symptomatic service funded.
Planning ahead
Currently the capital replacement of all mammographic x-ray units located in the static screening centres is the responsibility of the NHS Boards which host the screening centre. The capital replacement responsibility for mammographic x-ray units located on the screening mobile vans is the responsibility of National Services Scotland. Medical Physics support is provided from National Services Scotland for all mammographic x-ray units in breast screening.
Within NHS Boards that host breast screening centres, there is variation in where the service sits within lines of operational management. Three centres are managed as part of diagnostic imaging services, two are managed in breast surgical services, and one is managed in Oncology. Discussion within the review has suggested that greater strategic linkage into national imaging strategy, including equipment replacement planning, may be beneficial. Currently, for those centres managed within diagnostic imaging and therefore imaging networks, inclusion in wider diagnostic imaging strategy may be more straightforward, however all centres need to be aware of, and included in, strategic planning and developments.
National formula capital allocation is granted to individual NHS Boards. A mechanism to support Boards in planning collectively for the replacement of screening mammography x-ray units would be helpful to ensure that there is a national overview and readiness to respond to the availability of capital. A single, co-ordinated capital replacement programme for the Scottish Breast Screening Service could also incorporate NSS plans for units on the mobile fleet. Co-ordination of a national replacement programme could potentially form part of the working of the National Infrastructure Board.
Wider technical benefits, such as advising on the clinical and technical requirement for developments (such as digital breast tomosynthesis, or other screening imaging developments) may also be gained. This would support the ability of the Breast Screening Programme as a whole to move forward as one with technological advancements and new ways of working.
Strategic Recommendation
The review group recommends that a single, co-ordinated capital replacement programme for mammographic x-ray units in the Scottish Breast Screening Service should be developed, to support the prioritisation of capital with host NHS Boards and inform National Infrastructure planning.
Contact
Email: screening@gov.scot