Scottish Breast Screening Programme: major review
Major review of the Scottish Breast Screening Programme.
Access
Improving access to breast screening is particularly challenging for the programme, with screening delivered on a locality basis across Scotland (to minimise travel and distance for all as potential barriers to attendance), and with the need to continually focus on improving participation by women in our most deprived communities (with uptake being approximately 20% lower in our most deprived communities compared to the least deprived). National screening policy, IT systems, local service configuration, and breast service clinical pathways all effect and seek to support access to breast screening. Access was a key workstream within the review, and this section outlines consideration of: call and recall for breast screening; aspects of the use of current capacity; self-referral; inviting women for screening who are on breast cancer treatment or follow-up pathways; and the link with breast cancer Family History services.
Breast Screening Call/Recall - options & suggested future model
Reviewing call and recall processes
In the Scottish Breast Screening Programme women are currently invited for screening based on the GP practice with which they are registered. Women are attached to one of the six Breast Screening Centres based on their current GP Practice registration, or, for non-registered women, based on their Area of Residence. GP Practices are 'opened for calling' by Breast Screening Centres and women who are eligible to be called from the practice are allocated an appointment for screening. Allocation to appointments from the block set aside for the Practice has historically been a randomised process, and is not based on previous invitation or attendance dates.
Breast Screening is therefore unlike some other screening programmes where the offer is based on the participants' age or a specific recall date. Practice based calling was introduced at the outset of the breast screening programme to support screening delivery on a locality basis, whereby women are invited to a screening location close to their home or GP practice. It was adopted to minimise travel for women, as distance from a screening delivery location is understood to be a barrier to attending for screening.
Women can telephone to change their appointment time, and all women within a geographical area can choose to attend the local Breast Screening Centre or an alternative mobile location if they are unable to attend an appointment while the mobile screening unit is within their locality.
Adverse events
There have been two major adverse events in the Scottish Breast Screening Programme in recent years, both involving a failure to invite women who were eligible for screening. The causes of these incidents related to the limitations of the former breast screening IT system to track women who moved between GP practices (and subsequently were not issued with an invitation to screening as a result), and slippage in the screening programme schedule which meant that women who were eligible in the screening round, but had matured to over the agreed screening age (70 yrs. and 364 days) by the time their Practice was called for screening, were not invited. Safeguard reports have subsequently been developed and implemented in the Scottish Breast Screening System to avoid these events from reoccurring.
Previous discussion with the Scottish Screening Committee, associated with responding to adverse events and the performance of the Scottish Breast Screening Programme, have given rise to consideration of whether options to change the way in which women are invited to breast screening should be explored as a longer term strategy. Subsequently, call/recall processes for breast screening were placed in the scope of this review.
Breast Screening Call/Recall options workshop
In order to explore potential methods for call/recall that may improve the Scottish Breast Screening Programme a workshop was held with participation from members of the review group, breast screening services in Scotland, and NHS Board screening co-ordinators.
Potential methods examined included the following criteria:
- Practice based calling (the current method)
- Age
- Postcode
- Date of Last Screen/Next Test Due Date
Practice based calling
The consensus from the workshop was that practice based calling is not currently working effectively, and is not future proof. Increasing incidence of GP practice mergers (often with little advanced notice) and changes, the continual need for safeguarding reports to help track women moving between GP practices, the large geographical area covered by many practices, and the move away from GP screening-list validation were key issues. It was however acknowledged that practice based calling was well established and understood, with the breast screening IT system in place to support this method. Participants also flagged the potential to refine the existing system of practice based cohort management to improve screening clinic scheduling and the allocation of appointments.
Age
Calling for breast screening based on age alone was considered an unsuitable method. This method would involve calling from all geographical areas of the screening centre catchment simultaneously, and would require all locations to be visited in every year of a screening round which would be inefficient and unfeasible. It was acknowledged however that age based calling would be an easier process for women to understand.
Postcode
Calling for screening based on postcode would deliver what was deemed to be an essential focus on the geographical location for screening delivery. Postcode based calling was seen as potentially suitable for both urban and rural areas, would remove the current problematic issues associated with GP practice based calling, would offer the potential to link to locality and community groups to support health promotion and tackling inequalities, and would allow whole geographical areas to be called together. Relatively minor changes would be required to be made to the Scottish Breast Screening System to base calling cohorts on postcode clusters rather than GP practices. The benefit of calling on postcode alone was questioned however, and it was acknowledged that geographical planning support from the Scottish Breast Screening System would be required. Safeguard reports would still be required to pick up participants moving between different geographical areas.
Date of Last Screen/Next Test Due Date
Date of Last Screen/Next Test Due Date was regarded as an important criterion; however, it was considered that this would be better utilised in combination with another of the criteria for calling. Next Test Due Date was regarded as more personalised to individual women, and potentially a more efficient method of calling. Concerns around access and the potential negative effect on uptake were raised however if Next Test Due Date was used alone for calling, given there would be no geographical criteria.
Preferred option
Following consideration of the options identified the preferred way forward was to use a combination of the criteria (rather than any single-criteria based method), focusing heavily on geographical location. A method based on a combination of Postcode and Date of Last Screen/Next Test Due Date was initially preferred and prioritised for further development. It was felt that this model would retain the benefits of the current practice-based calling model, but would avoid issues associated with reliance on GP list data, and introduce flexibility which would lead to improvements. This method was seen as suitable for both urban and rural locations, would be feasible to develop in the Scottish Breast Screening IT System, and would retain a 3-year programme based on location. A mechanism to capture women who move in/out of geographical areas, and for inviting women becoming eligible for screening was noted as necessary.
Developing call-recall functionality in the Scottish Breast Screening System
The review team requested an examination of how the Scottish Breast Screening IT System (SBSS) may be developed and used to implement potential alternative methods for calling women to the Breast Screening service in Scotland.
The external supplier of SBSS was asked to outline possible alternative methods focusing on:
a) Shifting the focus for when a woman is selected for calling and when and how she is called to a screening appointment. Moving away from a call date associated with a GP practice to a call date (due date) associated with the woman herself.
b) Managing the youngest cohort (50-53yrs age group) to ensure that they are called in a timely manner based on their age and not based on which GP Practice they are attached to.
c) Moving to a selection and allocation model that uses the data within the Scottish Breast Screening System to assist the system users to determine where and when it is appropriate to relocate the mobile screening units, to screen the eligible population routinely and efficiently.
Whilst at the same time keeping the principles of calling the majority of women as close to their place of residence as possible.
Moving the call date from the practice onto the individual woman, and considering clustering the eligible women due for calling in a manner that allows women to be called as close possible to their place of residence, was identified as a potentially feasible option that could be used as alternative to practice-based screening, subject to further specification.
Developing this option would potentially change how the 'callable cohort' in SBSS was managed, away from a fairly static cohort list generated at the point of opening a practice, to a more dynamic cohort list based around, for example, women due to be called in the next 6 months. This potentially would allow SBSS to better manage current anomalies caused by:
1. Women moving practices: as women would now keep their own call date, and would become eligible based on their last screened date not on their old or new practice scheduled date
2. Practice merges: These no longer have any effect on the woman's call date
3. Newly eligible women at 50 years of age: would be brought into the system and allocated a recall date based on their DOB
4. Movements into Scotland: these women would be allocated a recall date based on the day they entered SBSS, or based on previous screening history from other parts of UK.
In the current calling model, SBSS uses GP Practice to group women in the eligible cohort for screening. An alternative grouping based on the recall date assigned to the woman, and her Area of Residence would be required, to enable calling clients by due date and screening location. Postcode areas may assist in a possible geographical grouping mechanism, however a more permanent solution to mapping to geographical area would be essential to allow the SBSS system to map a person to their nearest screening site. With incorporation of the new CHI, SBSS functionality should improve in this regard, potentially better facilitating mappings between screening sites and client locations.
In this method, although the focus will shift from calling the Practice to calling to person, the use of GP Practice to assist in appointment allocation and ensuring that women are screened at a local location may also be retained in some form within the SBSS allocation process.
Taking forward work on further specification
It is recommended that further specification and development work be taken forward to develop this strategic option, and also to explore the further potential for more automated and advanced planning for screening schedules.
Breast Screening Centres and system users should be central to the design of further specification for system development, particularly around incorporating operational business processes for appointment allocation and mobile screening clinic scheduling.
As a shorter-term development to assist improvement to current call-recall processes, use of new functionality recently developed in SBSS should be explored and used. This recent functionality allows Breast Screening Centres to prioritise individuals on Practice lists based on their date of last screen (historically a random process). SBSS now also orders women into first time screening invites; previous attenders; and previous non-attenders.
Strategic Recommendation
The Review Group recommends that a new approach to breast screening call-recall be taken forward which is more person-centred and is based on calling individual woman (rather than the GP Practice they belong to) based on their Next Test Due Date. Development of the Scottish Breast Screening System algorithm should also incorporate age, Area of Residence, and screening location to enable identification of women becoming newly eligible for breast screening, and local geographical cohorting of invites.
NSD and DaS should take forward the further specification work necessary to support development of the Scottish Breast Screening System. The Breast Screening Programme Board should advise and support this development, recognising that a person centred focus; incorporation of the new CHI functionality; and the potential to further automate planning, forecasting and allocation are key drivers for change and development.
Capacity utilisation, and the potential to improve access and patient experience
Location of services – long term service integration
There remains a consensus view across the Scottish Breast Screening Programme that in the longer-term screening centres and symptomatic breast services should be co-located. This is in line with the agreed recommendations of the 2012 review of breast screening in Scotland. Two centres currently operate this model (North of Scotland and East of Scotland). In the four areas where breast screening is currently not co-located NHS Board systems are either actively progressing co-location plans as part of wider acute hospital capital plans (NHS Grampian and NHS Lothian), or at screening service level would support working towards colocation (South West, and West of Scotland BSC). Co-location is broadly supported for reasons of potential service efficiency, improved communications and pathway management, as well as the advantages of single premises and facilities. In many areas Clinical Directors already have clinical management responsibility across symptomatic and screening services, and some screening service managers already work across screening and symptomatic.
Location of services – design and delivery
Feedback received from women who don't routinely attend for breast screening included feedback on a number of 'environmental factors' relating to the design and delivery of the breast screening service and how these may impact uptake. These included both the location of screening delivery, and the practical and psychological barriers to attendance.
Feedback on the user-friendliness of screening venues focussed on the mobile units. Women flagged the potential to locate screening clinics in health centres or community hospital facilities for example as a way of providing improved, more discreet, user-friendly and accessible environments than mobile provision. This was balanced with feedback on travel time and distance, particularly in rural and semi-urban areas, where it was thought that too great a distance presented a barrier to participation. This highlights the need to both improve mobile screening provision where geography and population size require a mobile programme, and to take the opportunity of improving the screening venue in urban and semi-urban areas which have the population base to sustain more static screening provision.
Satellite screening centres
Discussion with Breast Screening Centre teams around service delivery (location of current services and key operational issues, capital / premises strategy, the degree of integration with symptomatic services etc.) led to interest in exploring the concept of 'satellite screening centres' as a means to improve service delivery. Such units, as satellites from the main static screening centre base, would allow for more fixed, permanent access points for screening and a reduced reliance on the mobile fleet.
Geographical maps of inequalities in uptake in breast screening (referenced earlier in this report) were developed and used to support this discussion, noting that the central belt of Scotland has by far the greatest concentration of areas of lower levels of uptake and, given the population density, the largest proportion of invites for breast screening. Centres in the central belt of Scotland indicated that satellite screening facilities would potentially be beneficial. The three centres outside of the central belt did not feel that more static provision would assist delivery. Work to explore the concept further was taken forward with the central belt screening centres.
Current capacity utilisation
To help consider current capacity utilisation, screening clinic appointment data was reviewed over a two-year period (18/19 – 19/20) using data drawn from the Scottish Breast Screening System (SBSS). Appendix 4 shows a summary of utilisation data across the SBSP, and for each breast screening centre.
A summary of the picture for the whole Scottish Breast Screening Programme is noted in the table below. Overall this shows slightly better utilisation in static centres than mobile provision. Data shown in appendix 4 for the central belt centres shows a better utilisation / lower DNA rate in static provision. Data for the North centres and South West shows the opposite, a relatively better utilisation / lower DNA rate in mobile screening rather than static.
| Static and mobile | Mobile | Static | ||
|---|---|---|---|---|
| All SBSP | Total appointments available over the 2 yrs (total capacity) | 638,743.00 | 467,308.00 | 171,377.00 |
| Total Num. of appointments remaining filled on the day | 576,212.00 | 424,287.00 | 151,899.00 | |
| Total Num. attended appointment over the 2 yr period | 429,093.00 | 312,421.00 | 116,652.00 | |
| Number DNA'd over the 2 yrs | 140,751.00 | 105,652.00 | ||
| % Appointments remaining filled on the day | 90.2 | 90.8 | 88.6 | |
| % DNA from appointments remaining filled on the day | 24.4 | 24.9 | 23.1 | |
| % Ultilisation (proportion attending appointments remaining filled on the day) | 74.5 | 73.6 | 76.8 | |
Appointments data reviewed included the over-booking of clinics (therefore the utilisation statistics in the table above are accurate after programmed over-booking has been taken into account). Overall a significant number of appointments are lost to late cancellation and then, further to this, a high proportion of staffed capacity is lost to DNA's (24% DNA overall).
The case for more static satellite provision in the central belt
Each of the three central belt Breast Screening Centres indicated support for a hybrid model with more static centres to replace some of the mobile fleet.
The primary drivers for this change are:
- - the potential to develop a more client focussed service based on feedback (see benefits below).
- - the increasing difficulty of finding suitable community sites for the mobile fleet.
It has become increasingly problematic over recent screening cycles to identify suitable mobile location sites. The service has no funding to pay for sites and has previously relied on local community/commercial sites being offered free of charge. Some of the issues have been highlighted as a result of the pandemic, namely closed carparks, closed public buildings, closed community properties and lack of toilet facilities for staff and also clients. It is worth noting that there are no toilet facilities on the current mobile fleet.
Both the West of Scotland and the South East Scotland services wish to explore the possible use of static centres for central belt locations, where the population numbers would allow continuous screening at the location over the whole 3-year cycle.
Two potential location models have been suggested, both of which would capitalise on public transport links and car-parking availability, and both would therefore optimise patient access and consequently attendance.
- Use of NHS, Community, or Local Authority facilities
- Use of retail facilities and centres.
High level modelling by Breast Screening Centres has indicated that up to 70% of the eligible population for the central belt (and up to 95% for the South East) could be encompassed by this change if fully implemented for all suitable geographical areas.
Benefits anticipated include:
- Familiarity of location for clients and staff alike
- Potential for better uptake in deprived areas by reducing the barriers to attendance for these communities
- Allow service to reconfigure to book strictly by age or by post-code
- Allow clients to self-book at any time within 2 months in advance of due date
- Allow clients to choose location closer to home or closer to work / leisure
- Avoidance of the 3-yearly negotiation and uncertainty about the location of sites
- Allow clients to rebook to catch up following a cancellation or non-attendance, with no cut-off date as the facilities are always present
- Simplification of communication, relevant signage/paperwork/advance publicity
- Better link with community at location
- Cost savings (savings on mobile unit replacement, transport, supplies)
- Service resilience and efficiency will improve
- Potential for extended day working, not currently realistic on mobile units due to staff safety and travel consideration
- Provide static facility for each sub-region of catchment areas
- Image transfer by fixed broadband connection rather than less robust 4G or manual delivery would give more resilience
- Greater use of skill-mix, associate staff on-site supported remotely by senior radiographers
- Reduced carbon footprint
The potential for rationalisation of screening centre boundaries, and the potential to share screening facilities, is also noted.
Appendix 5 details submissions developed for the review from the West of Scotland and the South East of Scotland Breast Screening Centres. The South East service also highlighted four hospital or Community Treatment Centre facilities in areas with low uptake levels and high deprivation which, if NHS facilities were preferred, would be of initial interest.
Reducing barriers to attendance and increasing convenience
Section 5 of this report outlined key barriers to participation and attendance of screening appointments. Satellite Screening Units, situated in populous areas with the greatest potential to target improved uptake in surrounding communities, offer the potential to better respond to many of these. Greater appointment flexibility could be provided (including the availability of appointments, supporting choice of convenient attendance, potential for evening and weekend provision etc.); a more accessible physical environment; and more discreet and user-friendly facilities.
Strategic recommendation – central belt screening satellites
The Review Group recommends that further work is progressed by NSD, supported by the Breast Screening Programme Board, to develop a Scottish Breast Screening Service strategy for central belt satellite static screening centre provision, including their locations. This should develop an agreed approach, common planning assumptions for the SBSP, service configurations, and further scope and identify potential central belt satellite facilities in liaison with NHS Boards.
During the period of the review, COVID lockdown measures have meant that neither service leadership teams nor the review team have been able to visit potential satellite sites and develop discussion with site management regarding feasibility, scope, and potential. The review team has progressed some initial geographical mapping work (assessing travel times, distance, demand base) however as insufficient engagement has been undertaken with potential sites this has not been used to inform strategy, and instead has been limited to illustrative work only and to help develop the necessary dataset with Public Health Scotland. Potential exists to build on this with the Public Health Scotland Geospatial service.
Self-Referrals in over 70's
Background
Breast Screening programmes in all four UK nations routinely invite participants aged 50 to 70 years old for triennial screening. Although participants aged 71 and over do not receive screening invitations, they can self-refer for screening every three years. Self-referrals were paused in Scotland when screening restarted following the Covid-19 pause and currently remains so to allow limited screening capacity to be used for the age 50 to 70-year-old population. Self-referrals were also paused temporarily in the other UK nations but have now recommenced in England and Northern Ireland
Evidence
There is a lack of randomised-controlled evidence around the risks versus benefits of screening participants aged over 70 years. The evidence that does exist is mixed and there is no clear consensus of opinion. Although the risk of breast cancer increases with age, cancers affecting participants in this age-group are more likely to be slower growing[3]. The survival benefits associated with screening may be reduced by co-morbidities affecting life-expectancy and also a higher risk of complications/side-effects of treatment[4]. The risk of harm from over-diagnosis and subsequent over-treatment also increases[5]. A review paper concluded that individualised decisions about continued screening participation should be made after consideration of estimated life expectancy[6].
Cost-effectiveness modelling of screening participants older than 70 estimated that screening would lead to over-diagnosis in 6.2% of screen-detected women at the age of 72 years, increasing up to 37.9% at the age of 90 years. Under commonly quoted willingness-to-pay thresholds in the United Kingdom, the study suggested that an extension to screening up to the age of 78 years represents a cost-effective strategy[7].
In 2018, the Welsh Breast Screening Programme (Breast Test Wales) conducted an evaluation of screening participants aged over 70[8]. They found a deprivation gradient, with participants in the most deprived quintile accounting for significantly less of the screen appointments, compared with the least deprived. The Cancer detection rate was 1.6% of and was significantly associated with a past history of breast cancer.
Of the 2,543 patients aged over 70 with breast cancer recorded on national data systems, 14% had been referred from the screening programme. The screening-referred participants were significantly younger, likely to reside in less deprived areas, had more non-invasive tumours and were more likely to undergo conservation treatment compared to the non-screening diagnosed group.
The median survival was longer for the screening-diagnosed participants. Survival was poorer for those residing in the two most deprived quintiles and decreased with age with a marked decrease occurring between the age of 80 and 90 years. The factors significantly and independently associated with poorer durations of survival were non-screening referral and increasing age.
The consensus view of the participant focus groups was in favour of screening over 70 years. However, there was recognition that this may cause alarm to elderly participants. The participants would prefer to see the programme extended with routine invitations and two specific suggestions were made: the option to opt-out following invitation; a staggered (by increasing age group) roll-out.
Citizens Juries were conducted in Australia[9] amongst participants aged 70–74 regarding the acceptability of ceasing to invite that age-group for government-funded mammography screening. Participants were of diverse sociocultural backgrounds/levels of educational attainment. Both juries concluded by majority verdict that the screening programme should continue to send invitations and promote screening to the 70-74-year age group. Reasons given for the majority position included: (1) sending the invitations shows that society still cares about older participants, empowers them to access preventive health services and recognises increasing and varied life expectancy; (2) screening provides participants with information that enables choice and (3) if experts cannot agree, the conservative approach is to maintain the status quo until the evidence is clear. Reasons for the minority position were the potential for harms through over-diagnosis and misallocation of scarce health resources.
To gain a conclusive answer around the effectiveness of screening participants aged over 70 a cluster-randomised trial (AgeX)[10] is under way in England. The trial began in 2009 and has randomised more than 4 million participants to receive, or not receive, one additional breast screening invitation. Screening records of trial participants are linked electronically with routinely collected government records to help assess the short-term and long-term effects of the additional screening.
Following the suspension of routine breast screening throughout the UK in March 2020 due to COVID, and the subsequent pressure on breast screening capacity, the AgeX investigators decided in May 2020 that further randomisation into the trial should cease permanently. The trial itself will continue as follow-up by electronic linkage to routine government records continues throughout the 2020s and beyond. For breast cancer mortality the first report is scheduled to be on the follow-up to 2026, after which there will be subsequent reports on longer follow-up.
Self-Referral Activity in Scotland
Data from SBSS for the period 2016/17 to 2018/19 were extracted and participants who were screened at the age of 71 years or over were identified. Those who had received a screening invitation and were being screened at age 71 due to slippage were excluded so that only true self-referrals to screening were considered.
Over the three-year period, a total of 32,492 participants self-referred into the Scottish Breast Screening Programme. The proportion of total screening activity comprising self-referrals was 5.7% overall but this varied considerably by Screening Centre (see Table 1). Rates were lowest in the West of Scotland (3.9%) and highest in the North East and South West (both 7.2%).
| Breast Screening Centre | Number of Self-Referrals | % Self-referrals (of total screening activity) |
|---|---|---|
| East | 3442 | 6.0 |
| North East | 4868 | 7.2 |
| North | 2463 | 6.9 |
| South East | 9249 | 6.5 |
| South West | 4338 | 7.2 |
| West | 8132 | 3.9 |
| Scotland | 32,492 | 5.7 |
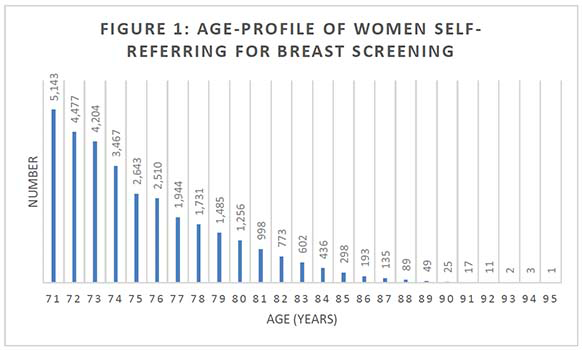
Figure 1 shows the age profile of participants self-referring for breast screening. The majority (65%) were aged 75 years and under. 85% were aged under 80 years.
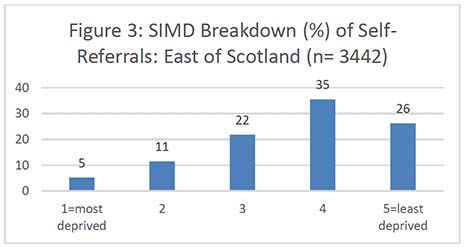
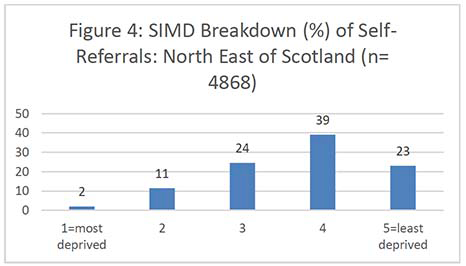
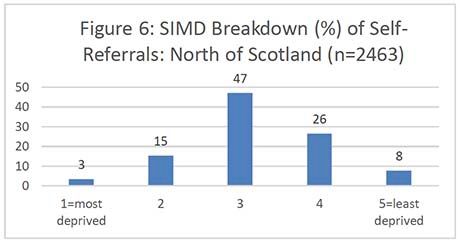
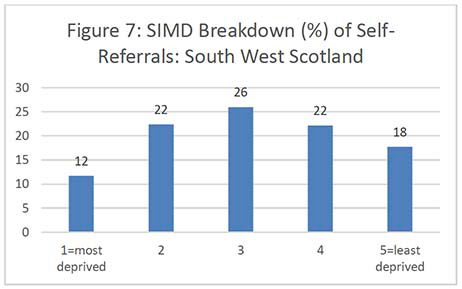
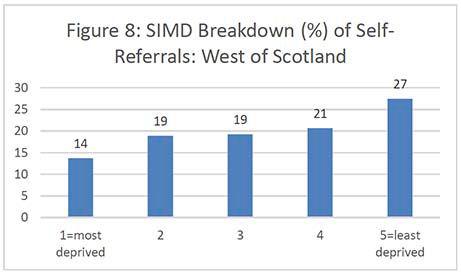
Figures 2-7 show the SIMD breakdown of self-referrals in each of the six screening centres. At a Scotland-wide level and in most screening centres, a gradient exists between the least and most deprived participants, with 53% of self-referrals coming from SIMD 4 and 5 (least deprived quintiles) compared to 26% from SIMD 1 and 2 (most deprived quintiles). The gradient is less marked in the North of Scotland but this may be because data zones in rural areas tend to cover a large land area and reflect a more mixed picture of people experiencing different levels of deprivation. The gradient in the South West (which also covers a significant rural area) is also less marked than across the rest of the country.
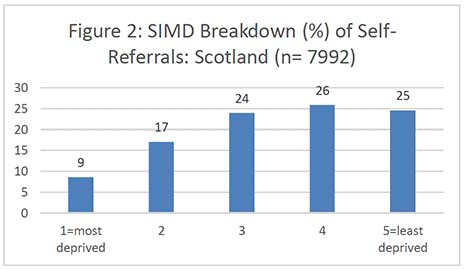
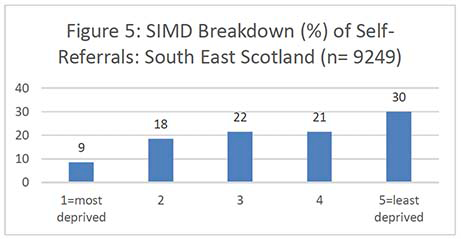
It's important to note that the number of women aged 71 years and over in each national SIMD quintile also varies significantly by Board, i.e. some Boards have only a very small number of women in the most deprived quintile which affects the self-referral SIMD gradient. Unfortunately, it was not possible to obtain a SIMD breakdown for the exact populations served by each screening centre as some health boards are screened by more than one centre. Appendix 6 contains the SIMD profiles of the over-70 female population in each health board.
Screening Outcomes
The mean cancer detection rate amongst self-referring participants was 1.4% which is higher than the overall cancer detection rate in the 50 to 70-year-old screening cohort (0.9%). This is because breast cancer incidence increases with age. In addition, service feedback indicates that many of these women have previously been screened, and may include worried women with breast symptoms, some of which have been reported to their GP. These factors, as well as age, may influence the higher cancer detection rate in this group. When analysed by deprivation, the cancer detection rate was relatively stable within each quintile.
| SIMD 2020 Scotland level | Self-Referral Screens | % SIMD | Number of Cancer Cases Detected | % Cancer Detection |
|---|---|---|---|---|
| 1=most deprived | 2777 | 9 | 42 | 1.5 |
| 2 | 5538 | 17 | 83 | 1.5 |
| 3 | 7779 | 24 | 103 | 1.3 |
| 4 | 8406 | 26 | 128 | 1.5 |
| 5=least deprived | 7992 | 25 | 108 | 1.4 |
| Total | 32492 | 100 | 464 | 1.4 |
Conclusions
Between 2016/17 and 2018/19 32,492 participants self-referred for breast cancer screening in Scotland which was 5.7% of total breast screening activity. Self-referral rates vary from 3.9% in the West of Scotland to 7.2% in the North East and South West. This is a significant amount of additional workload, especially for the smaller centres. Participants from the most deprived quintiles are under-represented amongst self-referrals which has the potential to widen further inequalities in screening and cancer outcomes that already exist within the core screening age-range.
As expected, the cancer detection rate is higher in this group than in the 50 to 70 age-group. Without data linkage to national cancer datasets and a longer period of follow-up it is not known whether continued screening after age 70 brings mortality benefits. This question will only be answered when the AgeX trial reports in 2026. In addition, cancer detection rates are significantly higher in self-referring participants who have a past history of breast cancer.
Evidence from Wales and Australia shows that participants aged over 70 support the policy of continued screening, despite the potential risk of over-diagnosis/over-treatment and increased risk of treatment side-effects.
Population projections from Scotland suggest that if current self-referral patterns continue, numbers will increase year on year due to the ageing population (see Table 3).
| Baseline 2016/17 - 2018/19 Self-Referrals (Scotland) | 5 Year Projection | 10 Year Projection | 20 Year Projection |
|---|---|---|---|
| 32,492 | 35,839 | 37,626 | 45,716 |
Going forward, potential options for the Scottish Breast Screening Programme include:
1. Status quo until AgeX trial reports in 2026 (including decision to restart self-referrals once Covid pressures have lessened).
2. Suspension of over-age referrals until AgeX trial reports in 2026.
3. Consider further restriction/targeting of self-referrals, e.g. previous history of breast cancer.
The options were discussed with the Review Group and Option 1 was the preferred approach as the group accepted that it would be challenging to deviate from the position in the other UK nations in the absence of robust evidence on the issue. The group also agreed that it would not be appropriate to make a recommendation to cease or restrict self-referral without further public engagement and consultation. It was also acknowledged however that the Breast Screening Programme is under significant pressure following the Covid pause and capacity has still not returned to 100% due to social distancing requirements that prevent over-booking of clinics. It was agreed that whilst significant Covid pressures continued, the available screening capacity should be used for the core 50-70 years' age group rather than for a group in whom there is currently no conclusive evidence of mortality benefits.
Further discussion took place around the possibility of future research activity to target the self-referral opportunity on a sub-set of over 71's who might most benefit. This would be considered targeted screening though and is currently outwith the remit of the screening programme.
Inviting women on the breast cancer follow-up pathway
A number of women are being invited by the Scottish Breast Screening Programme to attend for breast screening while they are receiving treatment for breast cancer, or when they are in mammographic follow-up following a diagnosis of breast cancer.
Inviting women who are currently on a treatment or follow-up pathway causes both confusion and unnecessary distress to them. As such these invitations may be deemed inappropriate; however current national UK breast screening guidance requires these invites to be issued as a failsafe measure. Current policy and guidance states that everyone except those women who have had a bilateral mastectomy, or who have previously signed a disclaimer letter to remove themselves from the breast screening invitation process, should be invited[11].
Previous procedures in place to identify women who would benefit from suspension from screening, or removal
Historically, General Practitioners were asked to check screening lists for accuracy and to identify women for permanent or temporary removal from screening. Breast screening 'Prior Notification Lists (PNLs)', produced from the Community Health Index (CHI), with details of each woman registered with a given practice were used to support this process. GPs were asked to permanently remove women who were known to have had bilateral mastectomy, or who were terminally ill, or temporarily remove women identified with recent breast cancer, mammogram, or were otherwise not well enough to attend. This process was stopped in light of inaccuracies in practice returns, resulting in some women not being invited for screening when they should have been. For this reason, and after a review of the resource involved, breast screening programme policy changed to cease list validation by GPs.
Suboptimal patient experience, and a lack of co-ordinated care
As well as complaints and correspondence from women seeking to improve the process, Breast Screening Centres frequently deal with distressed women contacting the centre to query their invitation for screening. For women who have been diagnosed as an interval cancer this is particularly distressing and confusing.
Where women who are on follow-up do attend their screening appointment for mammography, this may consequently disrupt their acute hospital-led mammographic follow-up schedule (via which, annual mammography will already have been arranged), causing wasted appointments in the acute sector and additional difficulties for the clinicians rearranging follow-up schedules.
With separate, unlinked, breast screening and symptomatic breast service / acute imaging IT systems, and no reliable system in place currently to allow breast screening to routinely identify women in breast cancer follow-up, there is a risk that women may also receive unnecessary radiation (attending for screening within a 6-month period of having attended a hospital follow-up appointment for mammography). Acute hospital PACS systems (where the follow-up mammographic image is stored) are separate to the breast screening PACS system, making cross-checking and confirmation more challenging for the service.
The size of the problem, and impact on capacity
Cancer registry data was matched onto the breast screening review data extract (covering 2016-2019) to determine the number of individual woman invited to screening who already had a breast cancer diagnosis before her first offered screening appointment. There were 9,003 women in total aged between 50-70, and who were not a self-referral to screening, that had a cancer up to 5 years prior to their first offered screening appointment[12]. This equates to approximately 3000 women per year. Removing these women from uptake calculations shows an estimated 0.7% improvement in adjusted uptake for the Breast Screening Programme overall (range of 0.6% to 0.8% improvement in uptake at breast screening centre level). Developing IT systems capability to account for and adjust the uptake calculation in this way routinely would be beneficial and show a truer picture of programme uptake.
During the period of this review, following the restart of breast screening services (after a pause in screening activity due to COVID-19) the West of Scotland Breast Screening Centre carried out a snapshot audit of contact from women on the follow-up pathway. In August 2020 the centre was contacted by 99 women from 20 GP practices who cancelled their appointment and advised that they were on a breast cancer follow-up pathway, a further 110 women contacted the centre in September 2020.
Whilst many women do contact the Breast Screening Centre to cancel their appointment there is no routine exclusion code applied to the record and therefore cancellation negatively affects the level of recorded uptake, and overall programme performance. If cancellations are late notified to the centre the ability to reuse the appointment slot may be lost, which reduces capacity.
Proposed improvements:
- Short term: Use of exclusion codes in SBSS
The Scottish Breast Screening Programme National Users Group (NUG) has proposed the scoping and development of a change to the national breast screening IT system, SBSS, to facilitate exclusion periods for women on follow up surveillance programmes. The ability to add in start and end dates for exclusion could be developed. A system report could be run which shows all women excluded from screening due to follow up. The day after the exclusion period ends, the patient would automatically return to routine recall status. A proposed method of identifying women would be via local clinicians in the short term and potentially the Scottish Cancer Registry and Intelligence Service (SCRIS) and could be applied following agreement form a senior member of screening admin staff. The exclusion code should be applied for 5 years and automatically removed. There would be the ability to switch back to routine recall manually or extend the follow up period if the patient developed another cancer.
This change is now proposed for inclusion on the development matrix for SBSS changes, to be prioritised within the technical development programme.
For women identified as having received a recent mammogram, SBSS already has functionality to record a reason of "cancelled recent mammogram". This should be systematically applied to the record of those who contact centres to advise of recent mammograms. Although this cancels the current screening offer, again it is reliant the woman making contact with the breast screening centre.
The measures above will assist in codification and quantifying the issue. Both recording of data, and integrated IT System functionality need to be significantly improved before policy could be changed and women temporarily removed from calling to the breast screening programme. In the absence of reliable systems, there is a considerable risk that if the wrong period of time is used for temporary removal, a woman may not start to be called again at the correct time. Failing to commence screening invitation at the appropriate time may introduce a risk of potential legal action should a further cancer occur.
- Short term: Improve the text of the screening invitation letter
The current invitation letter used across the Scottish Breast Screening Service already asks women invited to contact the Breast Screening Centre if any of the following are relevant:
- have had breast X-rays within the last six months.
- are currently being treated for breast cancer or having follow-up tests.
- have had both breasts removed.
- have a disability/special requirements or are a wheelchair user.
- have breast implants.
The letter also refers to the potential that the invitation may have been received inappropriately, and again asks women to contact the centre in such instances so that records can be amended.
The wording of the current breast screening invitation letter should be improved to better explain why the Breast Screening Programme continues to invite women who may have had recent mammograms, are in treatment or follow-up for breast cancer, or have previously had both breasts removed.
- Longer term: Scoping the potential for IT linkage to support cross referencing of databases
There are currently no links between the Scottish Breast Screening System and any hospital IT system. Hospital systems do not have any automatic means of identifying follow-up protocols. Data from the Scottish Cancer Registry could potentially provide information on women diagnosed, however any potential transfer of information to SBSS would require to be followed-up manually by looking at correspondence. Accepting that there would be a responsibility at breast screening centre level for gaining accurate and up to date information, the scope to improve IT linkages should be further explored.
- Longer term: Integrated national PACS solution
With the PACS reprovisioning for breast screening due in 2023, it is planned to combine the six currently separate breast screening PACS archives together with the National Global PACS archive. This could potentially serve as a national database for imaging, offering the potential of coding follow-up mammograms so that they could be identified. The data quality would need to be robust for call/recall, however this would potentially provide a single source of truth for demographics nationally and would minimise risks of loss to recall or follow up if the patient moves within Scotland, or develops a metachronous cancer during the follow-up period which may reset the timing of follow up. This solution has been proposed to the NSS PACS Reprovisioning team from Breast Screening and has been added to the "must have" requirements for the output based specifications to be presented to vendors later this year.
- Longer term: Follow-up standardisation
A survey of regional cancer networks undertaken to enquire about breast follow-up arrangements in local NHS Boards revealed that follow-up protocols for breast patients vary considerably throughout the country. This variation in practice further challenges the ability of the breast screening programme to safely introduce temporary exclusion arrangements for screening. Moving to standardised national follow-up guidance across Scotland would minimise risk.
A number of Health Boards are considering moving to Patient Led Follow Up (PLFU). Traditionally patients have been seen in a clinic every year by a nurse, clinician or surgeon in addition to having annual mammograms. Under the PLFU process, women attend for annual mammograms, and are only recalled to clinic for further assessment if there are any concerning changes. Women can also self-refer with a new symptom at any time. This process has been established in the South West of Scotland centre for 5 years where there is a robust database of all patients on PLFU. If a standardised minimum dataset for follow-up patients was agreed nationally, this could possibly serve as a cross reference for exclusion.
Strategic Recommendation
Inviting women who are currently on a treatment or follow-up pathway causes both confusion and unnecessary distress to them. However, it does ensure that no women are inappropriately excluded from the programme. Recent issues in another screening programme have highlighted the risk that this poses. The Review Group recommends that NSD, PHS, and DaS supported by the SBSS National Users Group:
- − Develop the use of exclusion codes in SBSS to facilitate the temporary removal from calling to breast screening for women on follow up surveillance programmes
- − Improve the text of the screening invitation letter to better explain why the Breast Screening Programme continues to invite women who may have had recent mammograms, are in treatment or follow-up for breast cancer, or have previously had both breasts removed.
- − Scope the potential for IT linkage to support cross-referencing of databases
- − Use the Breast Screening PACS reprovisioning as an opportunity to provide a mechanism for coding follow-up mammograms so that they can be identified
- − Scope the potential to move to more standardised national follow-up guidance across Scotland
Family History Screening
Background
The Review Group asked the review team to reflect on the potential impact of genomics on breast screening. In doing so, the Review Group recognised that genetics was a topic placed out of scope for the review, however the group wished to gain a better understanding of the genetics landscape, direction of travel, and any key issues that may influence the current review. Following review, the group recognised that genomics for breast screening is still in development and establishing the evidence base, however noted the increasing focus on risk-based approaches to screening delivery. Subsequent discussion around risk management, and the acknowledged high level of demand in breast symptomatic services, led to the group questioning whether family history activity would be better provided via breast screening services.
Review of Family History Screening
The review considered:
- Previous review work undertaken to examine what the impact would be on the Scottish Breast Screening Programme (SBSP) if the six breast screening centres across NHS Scotland were to take responsibility for the ongoing management of women with a family history of breast cancer. This work had been undertaken in the context of the release of CEL 6 (2009) 'Cancer Genetics Services in Scotland – Management of Women with a Family History of Breast Cancer'. We noted that the previous review concluded that it did not believe there is any merit in moving the management of women with a family history to the breast screening service. The previous review did however recognise the potential for closer working through greater service integration / co-location of screening and symptomatic services - potentially more closely aligning family history and screening service provision over time.
- Work undertaken in 2013/14 via a short life working group to address the applicability of the recommendations from NICE guideline 164 for the Scottish population. NICE guideline [CG164] covers familial breast cancer: classification, care and managing breast cancer and related risks in people with a family history of breast cancer. This was published in June 2013, and updated in November 2019.
- The current Family History patient pathway in Scotland including primary care services, genetics services, and breast symptomatic services
The review noted that there is currently no accurate overview of the number of patients, or the number in each risk category, in the family history services across Scotland. There remains no standardised IT system and a reliance on paper based or local IT systems.
It was also noted that currently, scheduling for breast family history surveillance is undertaken locally in each breast symptomatic unit, commonly using virtual clinics to book and manage the scheduling of women. There would therefore be potential advantage in centralising family history surveillance calling via the Scottish Breast Screening IT system (SBSS), thereby providing a standardised system and improving safety. This would only be an option if services were to be integrated, and a business case for development would be required as the SBSS system is based on a 3-year call/recall protocol and would require further system development to accommodate more frequent recall patterns for family history women.
Additionally, whilst clinical guidelines (NICE guideline 164) are in place and adapted for the Scottish population, other elements of the family history service pathway could potentially be improved by integration with screening services. Quality assurance and reader standards could be developed for the service, and (with a single, standardised IT system) a better overview of annual activity nationally could potentially be gained, which would also support greater insight into cancer detection in this group etc.
Review recommendation
Overall, the review group noted that there were more potential opportunities present now within breast screening than at the time of reporting the previous review of Family History (2009) – in particular a single, standardised IT system (SBSS), and some initial evidence from experience that clinical examination may be removed from the family history pathway acceptably. The review group acknowledged that a larger piece of work would be needed to fully assess the potential advantages, feasibility, benefit, and costs of integrating with screening, or whether key improvements could be made in the family history pathway independently. The group recommended that any further work should be referred for national cancer policy consideration, potentially in the context of supporting greater service integration and co-location.
The review group noted the following key issues, which may inform any further consideration:
- Clinical guidelines and associated clinical management and referral support is already in place and the NICE guidelines (which cover complex assessment and clinical management issues) have been adapted for use in Scotland. The Primary Care and Genetics service elements of the pathway are well established. The strengths associated with current clinical guidelines, GP, Genetics service, and surveillance clinic provision should be retained and developed.
- There is a need to assess the level of benefit that may be gained from improving image quality, reader standards, and quality assurance if integration with screening is further considered.
- There is a need to assess the benefit, feasibility, and cost of incorporating patient calling to various surveillance protocols into the SBSS, to potentially provide a single national and standardised system.
- Access to, and arrangements for MRI capacity and reporting via the breast screening service would need to be considered for high-risk women on the family history pathway.
- There is a need to assess the evidence for clinical examination as part of the current pathway for women in high-risk categories, and the desirability and options for change.
- The capacity available in the Scottish Breast Screening Service including additional clinic/ additional staff capacity requirements would need to be fully assessed – given that all / most of the activity from the current surveillance clinics delivered by NHS Boards in each region would need to be transferred.
- Learning from the pathway arrangements, standards, and assurance systems in place to support family history screening in Breast Screening services in England and Wales.
Contact
Email: screening@gov.scot