Gender identity healthcare: evaluation of the impact of Scottish Government funding
This report presents findings of an independent evaluation into the impact of Scottish Government funding, as allocated to NHS Health Boards, to implement local work to improve access to, and delivery of, gender identity services. The evaluation covers period between December 2022 and August 2024.
6. NHS Lothian - Adult Services
6.1 Overview of the clinic
The Lothian Gender Identity Clinic is based at the Chalmers Centre in Edinburgh, and is open to GP referrals from within the NHS Lothian, NHS Borders and NHS Fife areas. While primarily based at the Chalmers Centre (and situated under the umbrella of the Lothian Sexual and Reproductive Health Service), the GIC also has the potential to engage with patients across its catchment area through the sexual health service’s 10 local clinics spread throughout different GP services. The GIC publishes data relating to patient referrals on its website: this data shows that the number of new referrals received by the clinic increased from 167 in 2015-16 to 588 in 2023-24, while the average wait time from referral to first appointment increased from 256 days in 2016 to a peak of 1049 days in 2022, before declining to 852 days in 2023.[85]
Current staff mix
In 2018, according to the SPHN report, the GIC was staffed by one consultant psychiatrist, one specialist nurse practitioner with a background in mental health, and an administrator.[86] In recent years, however, the staff team has grown and evolved largely as a result of the additional SG funding - and now includes:
- Consultant Psychiatrist (0.70 WTE)
- Consultants in Community Sexual and Reproductive Health (0.40 WTE)
- Endocrinologist Consultant (0.25 WTE)
- Clinical Psychology Band 8B (0.80 WTE)
- SRH/ GP Specialist Speciality Doctor (0.60 WTE)
- Lead Research & Development / QI Consultant (0.20 WTE)
- Clinical Nurse Specialist - Gender Lead Band 7 (1.00 WTE)
- Mental Health Nurse Band 7 (1.00 WTE)
- Nursing Band 6 (2.40 WTE)
- Nursing: Clinical Support Worker Band 3 (1.40 WTE)
- Research and Development Band 7 (0.40 WTE) and Band 6 (0.40 WTE)
- Gender Admin Team Lead Band 4 (1.00 WTE)
- Administration secretary Band 3 (2.00 WTE)
- Project Manager Band 6 (0.40 WTE)
- Voice Specialist Band 7 (0.10 WTE) and Band 6 (0.60 WTE)
- Pharmacy Band 8A (0.20 WTE)
In total, therefore, the Lothian GIC Adult Service draws on the equivalent of 13.85 WTE staff, as of August 2024.[87] The GIC has sought in recent years to develop a multidisciplinary approach to providing care and support around gender identity, incorporating the expertise of a range of healthcare professions.
6.2 Scottish Government Funding Proposal
In its funding proposal to the Scottish Government, submitted in June 2022, Chalmers GIC set out a “comprehensively revised model of care to improve service resilience, succession planning and patient experience/ access using a multidisciplinary team approach to provide the right care by the right clinician at the right time.”[88] The total amount of funding applied for was £575,597 for 2022-23, with indicative costs for 2023-24 and 2024-25 calculated as £692,300 and £601,074 respectively. After submitting the proposal, the GIC was allocated £192,000 in December 2022 to support work in 2022-23; it received £732,000 to support work in 2023-24; and the amount allocated for the service in 2024-25 was £732,000. The total funding allocation for NHS Lothian for the three-year period of funding 2022-25 was thus £1,656,000.
At the core of its SG funding proposal was the development of an “authentic patient-centred multidisciplinary model of holistic care”, drawing on the principles of the Realistic Medicine model. The approach is intended to enable the provision of care to take place on a needs-led and patient-centred basis, based around each patient’s preferences and circumstances. In particular, this model involves triaging patients before their initial gender assessment, and allocating them for initial assessment with the practitioner who would best assess their needs depending on complexity, with a multidisciplinary shared decision-making approach maintained at each stage of the pathway. Other aims included the development of greater clinical and non-clinical human expertise and resources to deliver gender care to those who require it; improving capacity, access and waiting times for gender care and better supporting those on the waiting list; and improving communication, data reporting, waiting list management and patient contact as well as reducing patient complaints. More specifically, the proposal sets out an ambition of reducing waiting times to 18 weeks within three years of receipt of funding.
The proposed service base at the Chalmers Centre offers a hybrid model of face-to-face and virtual consultations based on patient preference, as well as potentially utilising the Centre’s network of 10 local clinics as the model develops. NHS Lothian proposed to utilise the vast majority of SG funding to recruit staff in order to develop the GIC’s multidisciplinary team, with a total of 8.9 WTE additional staff proposed for the GIC. Specific posts identified for recruitment in the proposal included a consultant gender specialist, a consultant endocrinologist, psychologist, pharmacist, mental health nurse, specialist doctor, nurses and research and development support.
NHS Lothian’s proposal also included plans to support improved access for patients to GP shared care, speech and language therapy, and wigs.
6.3 Mapping the System
A range of organisations are involved in the delivery of gender identity services in NHS Lothian beyond the GIC, including GP services, third sector organisations, and other healthcare providers and partners across Lothian.
Firstly, collaborative working with GPs is crucial to several aspects of service delivery, including initial referrals to the GIC, blood testing, and prescriptions. GIC staff have described their efforts to develop and maintain good working relationships with GPs as an important part of their plans to ensure the successful delivery of services, in particular the management of gender affirming hormone therapy. GIC staff have acknowledged the difficulties that sometimes emerge in working with GPs who do not feel that they have the capacity to take on additional work of this kind.
The GIC also refers patients to a range of other health services (when appropriate) in relation to the provision of specific aspects of gender identity healthcare, including facial hair removal, speech and language therapy, fertility services and mental health services. The GIC provides in-house sexual health screening and contraceptive advice. Also of relevance are various groups and initiatives established under the auspices of local Health and Social Care Partnerships across the GIC’s catchment areas - for example, a non-gendered Survive and Thrive group developed by East Lothian HSCP.
In addition, third sector groups play important roles in different aspects of services locally, in providing support to individuals on waiting lists, signposting to counselling and other social support services, and providing other forms of one-to-one and group support in relation to gender identity. The GIC works collaboratively with trans stakeholder groups and GIC staff described being interested in exploring new avenues for collaboration with third sector partners such as LGBT Health and Wellbeing, learning from the experiences of other services across the UK such as the care navigation support offered by Indigo Gender Service in Manchester.
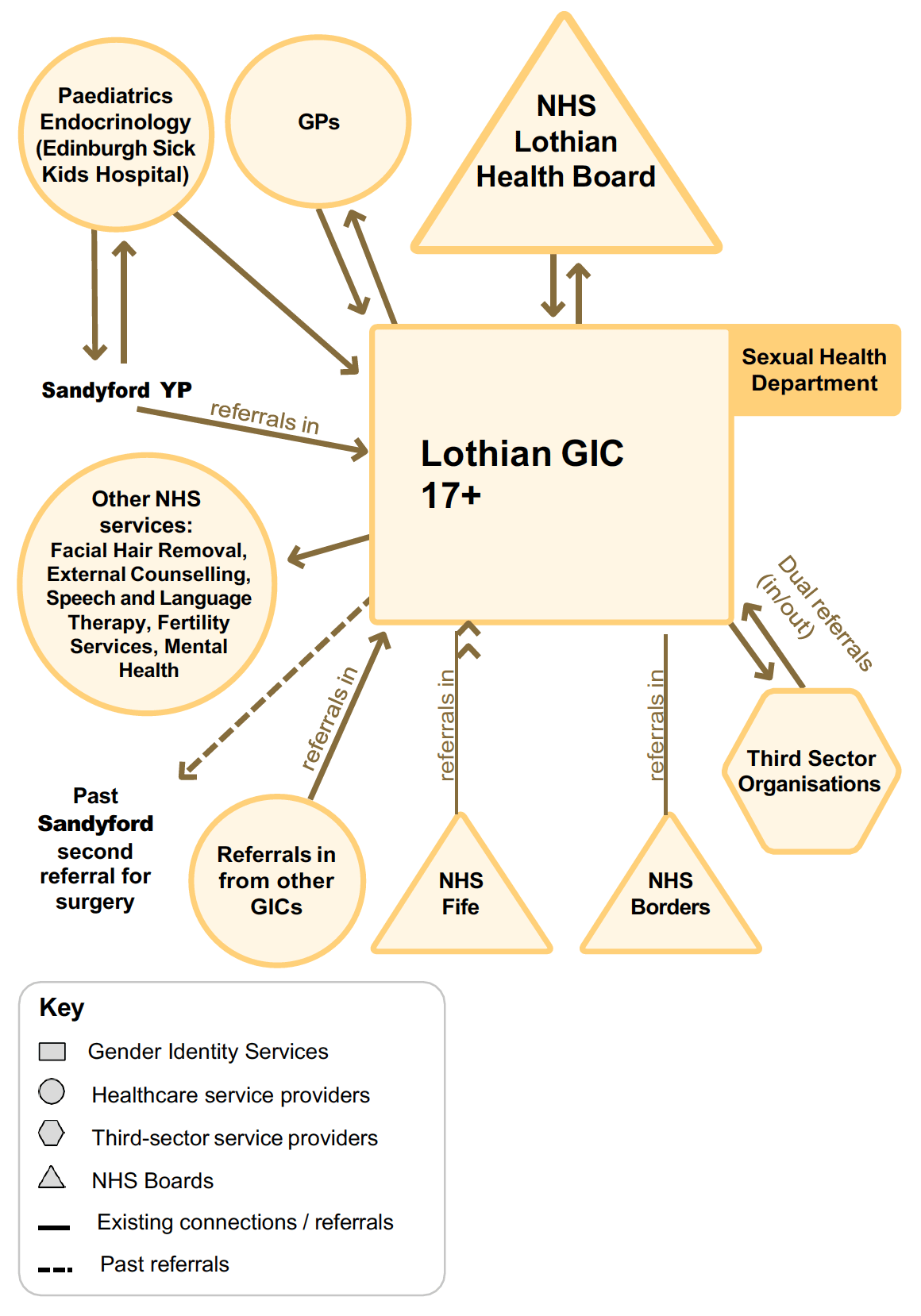
The Lothian (Chalmers) GIC system relationships map shows the linkages that the clinic has made with healthcare service providers and partners across Lothian. The clinic operates a multidisciplinary and needs-led approach to services for people aged 17+ seeking gender identity care (Chalmers is the only adult services GIC in Scotland that sees people from the age of 17). Most referrals of young people to Lothian GIC come directly from Sandyford, and a small number come to the Lothian GIC via Paediatric endocrinology. Endocrinology is an integral part of the GIC. Previously, Lothian GIC would request second opinions for surgery from Sandyford, but now these are done within the team. Once someone is assessed as being suitable for surgical intervention they are referred locally or nationally to GDNRSS depending on what surgery is required. Most staff are trained in sexual health and the GIC has recently started a sexual health clinic at LGBT Health and Wellbeing
The clinic has arrangements in place with other primary and secondary healthcare service providers in NHS Lothian, including facial hair removal services. It also has close links with third sector organisations, where there are dual referrals in and out of the clinic, for example around counselling and support for individuals on waiting lists. There are two other Health Boards referring in: NHS Fife and NHS Borders. The clinic is exploring specialist training and development for staff to strengthen their knowledge in gender dysphoria. For instance, three new GIC staff members are undertaking the Royal College of Physicians Professional Certificate in Core Capabilities in Clinical Practice for Adult Gender Identity Healthcare.
6.4 Services being delivered
Lothian GIC adopts a holistic and multidisciplinary approach to the delivery of services. Some key aspects of the services delivered through the GIC are summarised below.
Those referred to Lothian GIC by their GP first undergo an initial appointment of around 90 minutes at the clinic, which is usually conducted by a nurse, medical consultant or clinical psychologist, who has expertise in issues of particular relevance to the patient in question. Through this appointment, staff seek to identify the extent of the gender incongruence experienced by the patient, before working to put in place a treatment and care plan suited to the patient’s needs. This initial stage following referral also involves blood tests, risk assessments, further contact with GPs, and the identification of services relevant to the patient’s needs (for example, speech and language therapy, fertility preservation, and facial hair removal). The Lothian GIC follows the guidance in the Gender Identity Healthcare Protocol (which was updated and published in September 2024) throughout for assessment and care planning.
A significant amount of administrative work is required following initial appointment, including the composition of detailed letters to GPs, the recording of diagnoses, and the setting up of any necessary referrals; the clinic must also navigate different pathways and processes depending on the patient’s location (i.e. whether they are based in Lothian, Fife or the Borders). According to the Lothian Service Improvement Work document[89], the purpose of signing a shared care agreement with Lothian GPs would allow for GPs to monitor and adjust hormone levels based on blood test results which the GIC would interpret. The GIC also facilitates surgical referrals, which involves further assessments and a national waiting list. After an initial period of more intensive assessment and support, patients at the GIC may move to annual or biannual check-ups, involving the monitoring of areas such as blood pressure and liver function. Here, the Lothian GIC follows the NHS Scotland endocrine guidance and fertility preservation guidance.
The GIC also provides any wider additional support required by patients, particularly those (for example older individuals) who may lack language and knowledge about transgender and non-binary issues. The GIC seeks to offer social acceptance, support and relevant resources to these individuals in advance of the initiation of any medical treatments. Finally, patients are kept in the GIC’s records if they disengage or no longer need to access services for a period, so as to enable them to re-engage and seek any additional treatment or care from the GIC as their needs evolve throughout their lives.
6.5 Partnership working and cross-clinic links
Lothian GIC has good relationships with third sector organisations including LGBT Health and Wellbeing and LGBT Youth Scotland. Staff meet regularly with the third sector and have generally had good engagement. These links have evolved into Lothian GIC (along with Sandyford GIC) contributing to the funding of a post with LGBT Health and Wellbeing, as well as providing funding to LGBT Youth Scotland to provide sessional support to young people on the waiting list. GIC staff commented, however, that relationships with third sector organisations have been damaged by the NHS Lothian decision to pause surgical referrals and the lack of discussion or communication about this with patients and organisations Lothian GIC works with.[90]
There are, however, suggestions as to how relationships and practice can be improved. Staff highlighted examples of good practice in England, such as the third sector links that the Indigo clinic in Manchester has fostered, with third sector employees working with the GIC in the role of ‘navigators’: supporting people on the waiting list, signposting when necessary and generally offering peer support. There were discussions about how this system could be commissioned to support the work of the GICs in Scotland.
“I think there’s a number of potential things that could be developed [for those on waiting lists] and I think it's all got to be tested. I would suggest commissioning a third sector organisation to work with the GIC to try various different things and understand the impact of those various different things. And if you’re looking for what you can try and do, go talk to Indigo in Manchester who are doing exactly this with care navigators.”
Outside the third sector, there are monthly informal MDTs for gender clinicians in Scotland. These MDTs had been previously funded, however the network had to ‘stand down’ due to challenges recruiting a new clinical lead.
Additionally, Lothian GIC has engaged extensively with primary care, which has been positive. Staff highlighted that ‘sharing care and responsibilities’ with GPs would have a positive impact on the patients accessing the service. Indeed, the GIC recently finalised two shared care agreements (SCA) with local GPs in East, West and Mid Lothian and City of Edinburgh to support prescribing and blood screening. Under the SCAs, which began on 11 November 2024, “the GIC undertakes full assessment and treatment counselling/consent, and, where appropriate, will then ask GPs to prescribe endocrine treatment. The GIC will recall patients in line with the SCA protocol and undertake any tests or other monitoring required. The exception, agreed with the GP Sub-Committee, is bloods for those on testosterone injections, where these have to be taken immediately pre-dose. Those on hormonal treatment will also be offered a review at GIC: for suitable low risk patients, that may be through Patient Initiated Followup (PIFU). Chalmers GIC will then write to the GP to advise about ongoing prescribing.”[91] A representative from the NHS Lothian Medical Committee explained that the SCAs followed several years of discussions, which focused on “the evidence base [and] working out who does what, and what we could ask GPs to do i.e., the nuts and bolts of the SCA in terms of ‘tasks’ as well as responsibility.” The resulting SCAs were seen as a key development in gender identity care, and staff hoped that they could act as a blueprint for other Health Boards.
6.6 Training and Education
Training and education were highlighted by staff as an area that requires further development. Recruitment is a significant issue due to a lack of available practitioners and clinicians with the prerequisite skills in gender identity. If recruitment is successful, there is a significant roll-on effect on the clinic in terms of the time it takes existing staff to train new staff, who may lack pre-existing expertise around gender identity.
Internally, Lothian GIC has supported the work of NHS Education for Scotland (NES) to create a knowledge and skills framework. The GIC has also developed an in-house knowledge and skills framework for gender healthcare, with each staff member having a mentor and participating in individual and group supervision, reflective supervision and in-house training sessions.[92] Training for staff at Lothian GIC includes participation in MDT meetings, the shadowing of clinicians, observation of staff during clinics with feedback, the provision of books and reading materials for staff, and training and development days. There are two MDT meetings per week, and there is a focus on reflective practice. Two nursing staff have attended a nurse prescribers’ course and all of the nursing staff have had their membership of the British Association of Gender Identity Specialists (BAGIS) paid for, and have also been paid to attend BAGIS annual meetings. The skillset of some of their staff, including ‘a long-established GP trainer’, has helped to develop a training mindset within the clinic. As previously mentioned, three GIC staff members are undertaking the Royal College of Physicians Professional Certificate in Core Capabilities in Clinical Practice for Adult Gender Identity Healthcare. The more experienced members of the MDT are involved in their training and the consultant psychiatrist is their supervisor. All staff also have regular clinical supervision with a senior member of staff.
The general skill set required within GICs was also raised in interviews. One staff member highlighted the fact that gender identity healthcare is a ‘generalist specialism’; whilst specialist skills are indeed important, ‘you don’t necessarily want people with very specialised skills’. This may be a factor driving some of the differences between Lothian GIC and others. Lothian have built a varied MDT, drawing on specialist knowledge and skills whilst also building generalist skills within their team.
There was a sense, however, that while there have been steps to improve training and development, it does often take ‘a back seat’ in order to bring waiting lists down, although it is important to recognise that Lothian’s GIC waiting times are not the same as those of Sandyford. As one staff member highlighted, it is important to “have time to stop and learn” and to build training into their day-to-day work.
Once staff have been recruited, retention is a further challenge for not only Lothian GIC, but other GICs across Scotland as well. For Lothian specifically, challenges with retention were linked to additional pressures, such as those faced by practitioners who are required to build reflection into their professional registration. For those practitioners, reflection may feel less like a learning opportunity and more of a ‘tick box’ exercise, especially within the context of a busy GIC:
“I think to make sure that we can maintain the staff that we've got ... we’ve got to give them enjoyment, fulfilment in their work. It just enlivens us. The time to learn as well as work [...] Just to actually stop and think about what we've just done. And maybe ask a couple questions about that, and then maybe look it up and see, so that's why that blood level's like that, and so on. Instead, it's like ... OK, right, next patient. Even with reflection, I feel like there's always a demand within reflection. It's like this is your time for reflection, and now we need you to write that down.”
Staff discussed how to improve skills and knowledge through learning being less prescriptive and more organic. When considered alongside pressures associated with working in a GIC, staff felt learning should be encouraged when opportunities arise.
“Sometimes you just need time to do whatever it is that you find value in doing in that moment, and not have to provide something for it, because the thing that you're gaining is in your brain. And that's what makes you a good clinician is because you actually have the chance to develop your learning and your knowledge.”
Training and development, then, is a complex issue that all of the GICs face. Lothian specifically have focused on developing an MDT with ‘generalist speciality’ skills, whilst also recognising that there is a gap that Chalmers currently seems to be filling. Staff highlighted the requirement for training and development to become part of the day job, and to move from a ‘prescribed’ to a more organic system.
6.7 Impacts of the Funding on Service Delivery
Lothian GIC staff have observed a range of positive impacts experienced as a result of the additional SG funding, helping the GIC to better address key challenges and improve the overall quality and efficiency of service delivery. In response to a questionnaire carried out as part of this research, the GIC highlighted particular impacts as including increased overall capacity; a reduction in the waiting list; the ability to offer a hormone monitoring recall system; additional capacity to develop quality improvement projects and develop induction material for new staff; and the provision of training for GPs, psychiatrists and psychologists.
Perhaps most notably, the funding was seen as having directly contributed to the GIC’s recent success in reducing waiting times for patients, from around three years prior to the onset of the funding to around 15 months as of November 2024.[93] This was primarily because the funding enabled the recruitment of more staff and it facilitated the provision of additional sessional support for those on waiting lists, through contracts with the third sector.
The GIC’s use of the additional funding to recruit staff has contributed significantly to the expansion and enhancement of the GIC’s multidisciplinary team, including the recruitment of additional nursing, medical and psychology staff and the expansion of the GIC’s speech and language offering. This was felt to have helped make the MDT more dynamic and effective, increasing the comprehensiveness and richness of the care received by patients as well as improving the capacity of the team.
The funding was also highlighted as having contributed to several administrative and logistical improvements in the GIC. For example, the introduction of new clinical support worker posts has helped with the management of long-term hormone medication monitoring. This includes through the facilitation of blood tests and blood pressure checks, as well as ensuring that patients receive sufficient reminders and follow-ups for these and other checks. The clinical support workers were also seen as having helped with improved triaging and validation of the GIC waiting list, helping ensure that patients and staff are better informed and prepared in advance of appointments and improving ease of decision making.
Finally, staff emphasised that the funding has contributed to the maintenance of a positive “Chalmers culture” by enabling the recruitment of people that fit in well with this culture and with the existing staff team. Whilst not specifically related to the funding, one staff member highlighted that “it is not to do the funding, but there is, the stakeholder group is still active, and there is to be a funded PPV [patient and public voice] post to that group, which bluntly, has come about entirely because of the Scottish Government's lived experience coordinator and how well that works.”
Nonetheless, staff were also keen to emphasise some factors that facilitated the use of the SG improvement funding. In particular, the presence of an established business case (first produced in 2019, and updated in 2021-22) and service model well in advance of the onset of funding was seen as critical in enabling the GIC to take full advantage of the additional investment. Staff were appreciative of the service manager for Hospital & Hosted services and the Senior Management Team for Edinburgh Health and Social Care Partnership “taking a risk” and agreeing to fund the GIC expansion before receiving the SG improvement funding; this enabled the GIC to start recruiting and developing the service before other GICs. This also meant there was a clear plan for how any additional funding would be used, and a well-established multidisciplinary model in place to build upon. Staff also noted that the waiting lists experienced by the GIC prior to the onset of the funding - though having grown considerably over the preceding years - were not of the same scale as those of the Sandyford GIC. Had the GIC faced demand and a waiting list of this scale, while facing recruitment and retention challenges, it was felt by some members of staff that it would have been more difficult to maximise the impact of the additional funding even with a plan and model in place.
6.8 Impacts of Funding on Patient Outcomes
Waiting Lists and Patient Numbers
Official statistics in development reported by Public Health Scotland (PHS) found that, as of 31 March 2024, there were 931 people waiting for an initial outpatient consultation at NHS Lothian adult gender identity services. Of that number, 7 people had been waiting between 3-4 years, 8 had been waiting 4-5 years, and 16 people had been waiting more than 5 years.[94] The number of people waiting had increased by 14% between 30 June 2023 and 31 March 2024. During this period, NHS Lothian adult gender services had received 592 new referrals for outpatient appointments.
While not forming part of the official statistics in development, the Chalmers GIC confirmed that there were a total of 760 individuals on the waiting list for an initial assessment as of 12 August 2024. Waiting time as of August 2024 was approximately 584 days, amounting to a 43% decrease in waiting time for initial assessment since 2021.[95] In relation to patient numbers, numbers of GIC new referrals, initial appointments and follow-up appointments have all risen since the allocation of additional SG funding. As shown in Table 3, over these years numbers of initial appointments have grown closer to numbers of new referrals into the service, with the number of initial appointments exceeding new referrals in 2024-25 so far.
|
2021-22 |
2022-23 |
2023-2024 |
2024-2025 - Q1+Q2 |
|
|---|---|---|---|---|
|
New referrals |
306 |
531 |
588 |
268 |
|
Initial appointments |
67 |
269 |
512 |
348 |
|
Follow-up appointments |
1226 |
1770 |
2740 |
1760 |
Service User Impacts
In July-August 2024, a survey was sent to users of gender identity healthcare services across Scotland, to enquire about their experiences. It comprised a mix of open and closed questions. The survey received 74 responses. A total of 15 out of 74 respondents to the service user survey indicated that they were either currently accessing, on a waiting list to access, or had in the past accessed services at NHS Lothian (Chalmers) GIC. The majority of these respondents (12) were currently accessing services, while one respondent was on a waiting list and the remaining two had accessed the GIC’s services in the past but not currently. Table 4 below provides a summary of these respondents’ responses to the survey.
|
Current status |
No. |
% |
|---|---|---|
|
Currently accessing services |
12 |
80 |
|
On a waiting list |
1 |
7 |
|
Have accessed services in the past |
2 |
13 |
|
Total |
15 |
100 |
|
Has your overall experience with your GIC been a positive or a negative one? |
No. |
% |
|
Positive |
9 |
60 |
|
Negative |
3 |
20 |
|
Neither positive or negative |
3 |
20 |
|
Total |
15 |
100 |
|
Since the allocation of additional SG funding (from Dec 2022), have you noticed any changes in how gender identity services are delivered in your area? |
No. |
% |
|
Yes |
3 |
20 |
|
No |
10 |
67 |
|
Don’t know |
2 |
13 |
|
Total |
15 |
100 |
|
If you are being seen by a GIC, do you feel that you have a say over the gender identity care you are receiving? |
No. |
% |
|
Yes |
9 |
60 |
|
No |
3 |
20 |
|
Don’t know |
1 |
7 |
|
Would rather not say |
1 |
7 |
|
Not answered |
1 |
7 |
|
Total |
15 |
101[98] |
As can be seen in Table 4, most of the 15 survey respondents to the survey who were accessing Chalmers GIC described having had a positive overall experience. Most respondents (9 people) described positive experiences with the staff with whom they had interacted, describing them as being helpful, kind, supportive and considerate. Others welcomed being able to access different aspects of gender identity healthcare via the GIC, in some cases after long waiting times:
“The staff have been pleasant and practical about my situation. They have been responsive and considerate.”
“I chose positive because my overall experience has been that. Finally accessing care has been life saving for me.”
However, even where respondents felt their overall experience had been positive, frustrations were still expressed with aspects of the GIC’s services, most frequently in relation to waiting times. In the words of one respondent:
“Once I’ve gotten through the initial waiting list, the staff have been fantastic. However, waiting lists for all aspects of help are extremely long.”
Looking at respondents who have had either a negative overall experience (3 people) or who felt their experience was neither positive nor negative (3), some additional frustrations emerged, including difficulties communicating with the GIC and the length of time between appointments. One respondent described their experience as follows:
“The amount of time between appointments is insane (5+ months), they do not keep in contact with you and even when you are under their service you can barely keep in contact with them because they never respond to phone calls nor emails, people (including myself) are constantly falling off of their system including waiting lists, they occasionally impart false information or refuse certain treatments for shoddy reasons.”
Two-thirds of respondents (10 people), meanwhile, said that they had not noticed any difference in how gender identity services are delivered in their area since the onset of additional SG funding, with only a fifth of respondents (3 people) saying that they had noticed a difference. The main impact noticed amongst those who had noticed a difference was a reduction in waiting times, with one respondent feeling the funding had meant they were seen by the GIC sooner than they would otherwise have: “The estimated waiting time [...] significantly decreased, which I'm very happy about.”
Those who had not noticed a difference, on the other hand, observed that there continue to be long waiting lists and bottlenecks at different parts of the system: “I haven’t seen an improvement in waiting times but that could be due to the stage I’m at.”
More positively, most respondents (9 people) said they felt they had a say over the care they are receiving from the GIC, with a minority (3 people) saying they felt they did not have a say. Looking to the future, respondents expressed a range of thoughts with regards to how they would like to see gender identity healthcare delivered in their area, including a greater role for primary care providers (particularly GPs) in the delivery of gender identity healthcare, a move to an informed consent model of care, and better access (with shorter waiting times) to services such as wig provision. In a follow-up interview, one service user expressed their appreciation of staff at the GIC:
“It took maybe 18 months to two years to get the initial appointment at the gender clinic. It was the clinic in Edinburgh and it was one of the specialist nurses that I saw to begin with. That was really good. She was lovely, really helpful.”
For another service user, their experience of the initial appointment was equally as positive, however they also highlighted that:
“If anything…the appointment seemed a little bit too relaxed given that there's a waiting list out there. Well, I mean, it was good. It was what the appointment should be like. But I was just thinking, should I have this long when there's other people waiting?”
Another aspect that became clear during the interviews was the experience of service users regarding communications from the clinic. Whilst service users felt that during their face-to-face appointments, communication felt supportive, outside of the appointments communication became sparse. This was especially true for one service user who had highlighted that their surgery referral had been halted, and there had been no wider discussion or ‘clear timeline’ for the next steps in their care plan. A member of staff at the GIC explained that the decision to halt surgical referrals was not made by the GIC; and that the NHS Lothian Health Board had advised the GIC not to communicate the pause on surgical referrals to patients. They felt that this had a “negative impact on relationships between patients and the GIC staff.”
Respondents to a survey of third sector and non-NHS organisations carried out as part of this research pointed to several impacts on outcomes amongst GIC patients they felt had occurred as a result of the funding. As noted above, Chalmers GIC has been relatively successful (compared to others) in reducing waiting times for services since the onset of the funding, helping patients access and benefit from the GIC’s services in a more timely manner than previously. In addition, one respondent stated that the GIC was now easier to contact because of the additional administrative and reception staffing recruited with the funding, with positive consequences for patient wellbeing.
Respondents also welcomed the evolution in the skills mix of the GIC which has taken place as a result of the funding. One respondent stated that with the growth of the multidisciplinary team approach was felt to be depathologising and facilitated more person-centred care (based on their engagement with people accessing care). Respondents also highlighted that they felt the GIC had improved in terms of its engagement with third sector organisations as a result of the funding, creating more opportunities to explore ways in which the GIC and third sector organisations could work together to provide support to those accessing services.
One third sector survey respondent, for instance, cited Lothian GIC as an example of a GIC which has “managed to cut waiting lists considerably, which has been really positive.” The respondent felt this had been achieved by “changing the skill mix of staff at the clinics and using MDTs, which means they are impacted less by staffing shortages and able to recruit from a wider range of healthcare practitioners.” As a result, the respondent observed that “trans and non-binary people seem to be feeling positive about the direction of travel” at the GIC. This view was confirmed in interviews with third sector representatives, with one person saying that, “Lothian [GIC] are doing really well. They’ve definitely seen their waiting list decrease” while another interviewee felt that “there’s a bit of a buzz around Lothian, and some people [service users] seem to be feeling really positive about the direction that it’s moving in.”
6.9 Structural and systemic issues
As with the other cases, a number of structural and systemic issues emerged as having an impact on the GIC’s ability to deliver services as effectively as possible. These issues related to governance, increasing referral numbers and levels of need, deficiencies in long-term strategic planning, and staff retention and sustainability.
Firstly, it was highlighted that, while the National Gender Identity Clinical Network for Scotland (NGICNS) plays a welcome role in attempting to provide guidance and governance to GICs across Scotland, there remains a lack of a larger medical body that gender healthcare sits within. This in turn means that there are not always clear guidelines and standardised procedures for GIC staff to follow in the provision of different aspects of services. At the same time, GIC staff felt that there were robust and well-established mechanisms for clinical governance and a clinical governance group in place that meets regularly and has appropriate representation.
In addition, as seen before, the number of referrals to the GIC has increased rapidly in recent years, with anecdotal evidence suggesting that some patients are moving to the Lothian catchment area in order to access services quicker than they might in other parts of Scotland, further increasing the demand on the services provided by the GIC. The scale and complexity of this need, with some patients also requiring broader social support of the kind described earlier, means that managing and reducing the waiting list is likely to remain a formidable challenge for the GIC in the years to come.
A need for greater strategic planning also emerged as a key concern, particularly in relation to managing the long-term sustainability of the service in the midst of rising demand. Difficulties have been encountered in attempting to encourage strategic planning experts from elsewhere in the Health Board to take an interest in the future of the Lothian GIC, whereby strategic planning was viewed as vital to gender identity services, in understanding the nature of demand and how best to address it. Relatedly, while the Chalmers Centre itself was seen as a broadly good host for the GIC, it was felt that NHS Lothian more widely - as a large Health Board encompassing the second-largest residential population in Scotland - did not fully prioritise the service and lacked in some respects a sufficient understanding of the GIC’s needs.
Finally, the high demand for services was seen as placing a significant burden on clinicians in Lothian, who are required to manage complex roles often without spare time to reflect and focus on their own wellbeing. In this context, it was felt that maintaining and retaining staff was a key challenge to address for the GIC. Balancing the intensive workload and high demand for services with realistic expectations in terms of staff performance and wellbeing is likely to be critical to preventing burnout and therefore ensuring the long-term sustainability of the GIC in the years to come.
6.10 Conclusion
To help evaluate the effects of SG funding on services at Lothian GIC, we have developed a bespoke Theory of Change for NHS Lothian, shown below. This is based on the main ToC presented at the start of this report, and then tailored to NHS Lothian based on its aims for the SG improvement funding, the activities they have since undertaken, and the outcomes these changes are leading to.
Situation:
- Wider structural context (high demand for services, long wait lists, overstretched staff, lack of specialists)
- Consideration of local context (situated at Chalmers Centre in Edinburgh; catchment area of NHS Lothian, Borders and Fife)
- Fostering collaboration / relationships (links to third sector organisations, GP practice, other relevant healthcare providers / services)
Inputs:
- Total of £1.66m SG funding allocated to NHS Lothian over 2022-25 to improve access to, and delivery of, gender identity services
- Use of this funding by NHS Lothian to support activities, by:
- Hiring new staff, especially with expertise in gender medicine
- Increasing the hours of existing staff to see more patients/ build relationships
- Staff training / development
Activities:
- NHS Lothian implementing plans to improve services, in line with funding:
- Build capacity of front-line staff
- Map attendances
- Further develop pathways, including waiting list triage and GP communication
- Implement endocrine / GP shared care agreement
- Initiate training of new post holders
- Support and training strategy
Preconditions:
- Robust data & evidence
- Specialised training on gender identity for GIC staff and general training for mainstream NHS staff
- Safe and fulfilling workplaces
- Local, regional and national leadership
- Empowered and resourced staff, able to confidently make decisions
- Shared care GP agreements
Outcomes:
- Changes to meet the needs of patients (improved wait times, expansion of multi- disciplinary team, more support to those on waiting lists)
- Changes to understanding of systems (improved data collection and monitoring, increased provision of staff training and development)
- Changes to governance of systems (improved triaging and validation of waiting list, quality improvement)
Impacts:
- Realistic Medicine vision:
- Empowered patients, Personalised Care, Informed Decisions, Joined Up care
- GIC-specific:
- Accessible, inclusive services (including pre-service support), educated workforce, sustainable and well-funded services, good governance, strong networks, mainstreamed care, reduced inequalities
Overall, the data we have gathered suggests that NHS Lothian has been able to make progress with regards to waiting times and other aspects of service delivery as a result of having received SG funding. Crucially, the GIC has been able to expand and enhance its multidisciplinary team, thereby building the capacity of its front-line staff. This has enabled the GIC to further develop patient care pathways, map attendances and develop a patient-centred and needs-led model of gender identity healthcare drawing on the diverse range of skill sets present in the staff team. The GIC plays an important role in the wider gender identity healthcare landscape in Scotland, with staff in Lothian helping provide advice and training to staff in other GICs. The Lothian GIC has also developed close links to a variety of local partners involved in delivering different aspects of gender identity healthcare, including third sector organisations. Crucially, the GIC has developed strong relationships with local GP services, which has led to the creation of Shared Care Agreements. The presence of a well-established business plan and expanded service delivery model well in advance of the receipt of the SG funding was pivotal in facilitating the GIC’s achievements in these respects.
These activities are aligned with the goals set out in the NHS Lothian proposal for SG improvement funding, and the data suggest that the SG funding has had a positive impact on outcomes, including reducing waiting times and improving patient care. Respondents to the survey and interviewees who had engaged with the NHS Lothian GIC expressed their appreciation of efforts to reduce waiting times. Service users also described the staff working within the clinic positively, which highlights the importance of keeping staff morale high and creating the right team mix and the impact that this can have on patients' experience. Interviews with staff also suggest that the SG funding has had a positive impact on staff satisfaction owing to a strong and distinct ‘Chalmers culture’. Whilst some service users relayed in the survey and interviews that the GIC’s communications with patients could be further improved, the overall sense was that the GIC was providing a good experience of care for the patients they are supporting.
Nonetheless, as with Scotland’s other GICs, Lothian GIC also continues to be affected by a number of systemic and structural challenges. Staff interviewees identified some obstacles that have hindered their ability to make all of their intended improvements to services. Examples of these challenges included: the rising demand for gender identity services in Lothian; the risk of staff burnout; the need for greater strategic planning; and the lack of overarching guidance and governance at national-level in relation to aspects of gender identity healthcare. These issues may be addressed if leaders at the local (GIC), regional (Board) and national (SG/NHS Scotland) levels put in place a number of best practice learnings - which are elaborated in full towards the end of this report - around staff wellbeing support, continuous improvement ethos, strong communications with patients, sharing the responsibility across Health Boards, consistent structures and pathways, long-term core funding, clinical governance, and the strengthening of structures around national networks and policy learning. Addressing these issues may help to ensure the continued sustainability and effectiveness of Lothian GIC in providing gender identity services.