Gender identity healthcare: evaluation of the impact of Scottish Government funding
This report presents findings of an independent evaluation into the impact of Scottish Government funding, as allocated to NHS Health Boards, to implement local work to improve access to, and delivery of, gender identity services. The evaluation covers period between December 2022 and August 2024.
4a. NHS Greater Glasgow and Clyde - Adult Services
4a.1 Overview of the clinic
The Sandyford Gender Identity Clinic (GIC) is based in Sexual Health Services in NHS Greater Glasgow and Clyde (NHSGGC). It is the only GIC in Scotland to operate both an Adult Service and a Young People’s (YP) Service. In this chapter we will discuss the Adult Service, while providing broader information about the Sandyford GIC in NHSGGC; while in the following chapter we will focus on the YP service.
Sandyford’s Adult Gender Service is open to GP referrals from seven NHS Health Boards: NHSGGC, NHS Dumfries & Galloway, NHS Lanarkshire, NHS Forth Valley, NHS Tayside, NHS Western Isles and NHS Ayrshire & Arran. Sandyford also accepts patients from the Argyll and Bute Health and Social Care Partnership (HSCP) area.[36] Sandyford previously accepted self-referrals into both the Adult and YP services (the only GIC to do so). From 13 August 2024, Sandyford only accepts referrals from a clinician (either a GP or Mental Health services) to both the Adult and Young People’s services. Those who self-referred previously have not been affected by this change.
Current staff mix
As of August 2024, there are 13.6 WTE (whole time equivalent) staff employed across the Adult Service and Young People’s Service at Sandyford GIC. This is delivered by 20 staff members, ranging from one member of staff who provides a single clinical session (4 hours per week) to full time members of staff (37 hours per week). Staff comprise a mixture of permanent, Sandyford-funded posts and temporary fixed-term posts, funded using the SG-allocated monies. The GIC has reported experiencing significant vacancies and difficulties hiring new staff, which is explored further below.
The Adult Service is currently staffed by the following permanent post-holders (which, put together, total the whole time equivalent of 3.9 staff[37]):
- Psychiatry: 0.4 WTE (two post holders)
- Psychology: 1.6 WTE (three post holders)
- Counselling: 0.5 WTE (one post holder)
- Occupational Therapy: 0.4 WTE (one post holder)
- Medical Secretary: 1 WTE (one post holder)
In addition, both the adult and YP services have been supplemented by temporary post-holders, which have been created with SG funding (totalling 5.5 WTE):
- Medicine: 0.5 WTE (one post holder working primarily in Adult Service)
- Pharmacy: 1 WTE (one post holder working primarily in Adult Service)
- Psychology Assistant: 2 WTE (two post holders)
- Operational Manager: 1 WTE (1 post holder working across both services)
- Waiting List Coordinator: 1 WTE (1 post holder working across both services)
Service history
The NHSGGC Gender Service has been “in existence for approximately 30 years.”[38] The service initially formed part of the Family Planning Service and had “approximately 10 adult patients who attended the service for support and advice with issues around Gender Dysphoria.” Demand grew slowly over time to around 30 patients. In 2000, the Sandyford Initiative opened and began to expand as more patients became aware of it, and by 2012, the service grew again to include a small number of young patients.[39]
Sandyford GIC sees patients who have been referred by GPs or Mental Health services, and until 13 August 2024 also accepted self-referrals. The adult service also offers “further assessment for complex presentations” and historically offered second opinions “for surgery for patients who are seen at gender services in NHS Grampian, NHS Highland and NHS Lothian.” The funding for this was “via an agreed financial framework that covers clinical and administration time.”[40] As of August 2024, the number of people on the waitlist for the young people’s gender service stood at 945, with 3637 people on the waitlist for the adult service.[41] The GIC provides an information-rich website[42] that is accessible to service users, with details on the services provided by the clinic and follow-on resources for patients.
4a.2 Scottish Government Funding Proposal
The total amount of funding applied for by NHSGGC from the SG in 2022-23 (for the final four remaining months of the year) was £712,484. In the proposal the expectation of indicative spend beyond 2022-23 and in total for the three-year period was £1,424,969 for both the adult and young person’s services. After submitting the proposal, NHSGGC was allocated £496,500 in December 2022 to support gender identity services improvement work for both the young person’s service and adult service in 2022-23; it received £400,000 to support work in 2023-24; and the amount allocated for the service in 2024-25 was £400,000. The total funding allocation for NHSGGC for the three-year period of funding 2022-25 was therefore £1,296,500.[43]
The NHSGGC proposal for SG funding was developed on the understanding that it would take several years to establish improved service capability and capacity both within NHSGGC and other Boards.[44] NHSGGC acknowledged the pressing need to build capacity in order to triage, diagnose, and enable appropriate treatment plans for patients, given the extensive wait times the GIC faced (for both adult and YP services). The main aims of the NHSGGC’s funding bid were to: develop an understanding of patient need for young people and adult services; build a demand profile to inform service-planning dialogue with referring boards; ensure that all patients receive an initial clinical triage call; support patients through complementary support purchased from third sector partners; and build capacity in the short term to enable assessments to be delivered, and where appropriate, treatment pathways to commence.
The proposal was for the service to build upon the preexisting multidisciplinary team (MDT), consisting of clinical psychology, consultant psychiatry, sexual health doctors, speciality doctors, occupational therapy and administrative support. It would adopt a virtual/telephone consultation approach where appropriate. It also aimed to introduce a new model of telephone/virtual triage and expand resources to work with the third sector. On the latter, the proposal outlined plans to strengthen relations with third sector organisations to provide early intervention support, and to undertake proactive communication with service users, as well as help advocate on the behalf of patients.
4a.3 Mapping the System
The system relationships map for NHSGGC (Sandyford) GIC in Figure 1 shows the size and complexity of relationships across the system. The Sandyford Clinic is the largest in Scotland, and it hosts two services: the Adult Service, and the Young People’s Service. All young people’s (YP) referrals across Scotland are made into Sandyford. Meanwhile, as described in section 4a.1, six Health Boards outwith NHSGGC make referrals into Sandyford’s Adult Services. In addition, the NHSGGC Sandyford GIC accepts patients from the Argyll and Bute HSCP area. In the past, Sandyford was the only clinic offering second opinions (on psychological assessments and surgery referrals) for adult services to all other GICs in Scotland. Until August 2024, Sandyford was the only GIC taking self-referrals, for both adult and YP services.
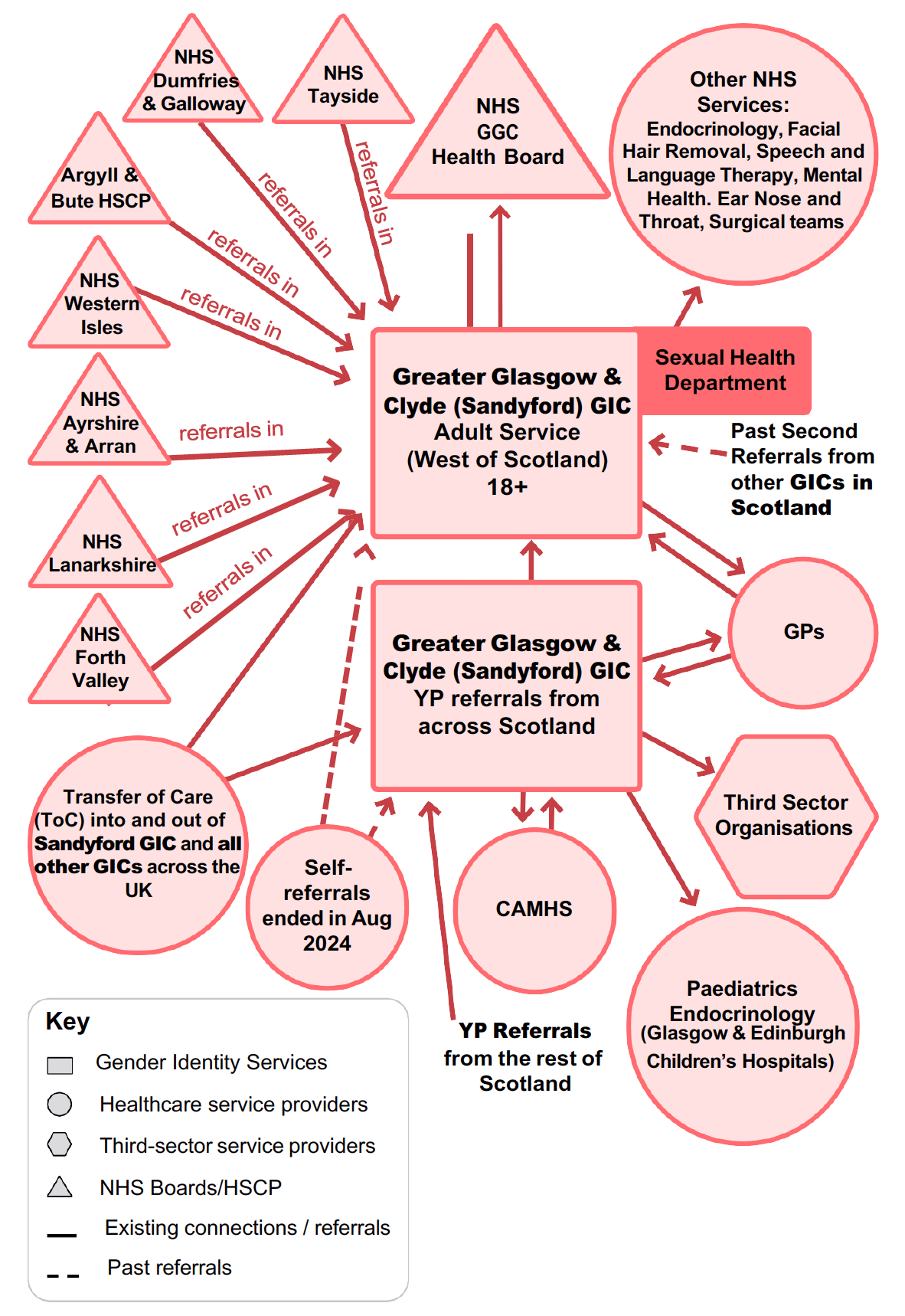
Sandyford GIC, like those in Lothian and Highlands, is based within Sexual Health Services at NHSGGC. Both the adult and young person’s services at Sandyford GIC are managed as part of the Integrated Sexual Health Service “and are well connected through Glasgow City HSCP and NHSGGC Board structures.” The Sandyford GIC itself has an established governance framework and the service is also well connected to other primary and secondary healthcare service providers in the Health Board, including endocrinology, facial hair removal services, speech and language therapy, mental health, ear nose and throat (ENT) and surgical teams, to whom it makes referrals. The GIC refers to and takes referrals from GPs, with staff reporting differing levels of support from GPs, and it also has links with third sector organisations.
4a.4 Services being delivered
In its written evidence to the Scottish Parliament’s Equalities, Human Rights and Civil Justice Committee on the Gender Recognition Reform (Scotland) Bill, the Sandyford Clinic outlined their service for trans people, and detailed how the team currently provides “[b]alanced clinical judgments and decisions'' which are taken through “multidisciplinary team discussions involving psychology, psychiatry, sexual health doctors, occupational therapy and endocrinology as appropriate. There is also regular patient specific communication with general practice.”[45]
While the GIC itself does not offer any support to individuals on the waiting list due to a lack of resources, it has recently invested in third sector support to which patients on the waiting list can be referred should they need support. The YP service has benefited from both an admin validation exercise which ensures that waiting lists are accurate and up-to-date (completed) and also a clinical validation exercise (partially completed). Once fully completed, this process will in turn be applied and performed in the Adult Service. The GIC uses the NHSGGC Access Policy for waiting list validation. Data for the service is held in the electronic patient record system NaSH (used by sexual health clinics in Scotland) and waiting times for a first appointment are reported to PHS.[46]
When assessing the services being delivered by the GIC (for both adult and young people), staff members found there to be a lack of strategy and governance for gender healthcare, creating a barrier for effective and efficient service delivery. This was partly due to recruitment issues. The service existed without a clinical lead for much of 2024, despite advertising the role several times. From October 2024, the service has had a 0.5 WTE Clinical Lead in place, provided by two post holders. Beyond immediate recruitment issues, of not having a clinical lead for a period of time, one interviewee also felt that the absence of a “Faculty of Medicine that oversees gender care” for Scotland was a barrier to creating good governance.
As staff recorded in interviews, service delivery at the Sandyford GIC currently faces a number of challenges. Waitlist lengths - which stood at 3637 people waiting for adult services as of August 2024 - are felt to be overwhelming and unsustainable. This is a challenge further compounded by staffing issues caused by a lack of clinicians, and problems filling current vacancies. In an interview in April 2024, one staff member said that “due to resource pressures, we’ve got significant vacancies,” while another interviewee expressed frustration that “we have advertising for permanent staff as well as temporary staff and we cannot recruit to it.” Anecdotally, one staff member revealed that, “I was probably spending like 4 to 6 hours additionally, at my kitchen table at night … it was just utterly unmanageable.” Another staff member shared, “there’s not enough medics in the adult service … What is the point in taking people off the waiting list and doing their assessment if we’ve not then got the capacity and the medical team to actually see them to get them started on their hormone treatment?”
Exacerbating problems further, staff suggested, was the national shortage of psychologists. “This is not unique to gender services”, one interviewee said, but it was felt that the Sandyford GIC was not people’s first choice of where to work, due to the politicisation of gender identity services and the media focus on the clinic. Staff also highlighted the lack of sufficient resources to meet the steadily rising demand for the service, and ways they’ve attempted to remedy it. One interviewee underscored how “[t]he medical staffing complement is not enough to meet the demand.” When the GIC hired a specialist clinical pharmacist with the SG funding, this not only enhanced the staff/skill mix of the MDT team and enabled service users to access gender affirming hormones, but a collateral benefit was to free up “some of the medical capacity in terms of reviews,” which enabled other staff to “see more new patients.”
Another issue brought to the fore during interviews was the prevalence of ‘diagnostic overshadowing.’ This is where gender incongruence is given primacy when patients present to GPs or mental health services with any mental health related issue, but are instead referred on to GICs, with medical professionals perceiving gender incongruence as the prime determinant for any mental health issue experienced by trans and non-binary patients. “Diagnostic overshadowing…can feel like you mention gender incongruence, and it’s a knock back,” one staff member relayed, “regardless of … what very good argument you’ve put to them for why their service is the better one to be supporting their mental health difficulty.” This issue echoes the pathologisation problems faced by trans patients with mental health concerns highlighted in the 2016 report from the National Institute of Economic and Social Research. [47]
Staff also raised issues around the overlooking of non-binary patients seeking access to GICs. One staff member said, “some patients who are non-binary - they’re not showing any signs of a particular gender - would not, by the norm, be put forward for any treatment. It would be exceptional circumstances for that, and that would be because of perceived distress.” This speaks to data collected in a research survey by Scottish Trans in 2016, which found that only 25% of non-binary research participants had ‘always’ felt comfortable sharing their non-binary identity when using gender identity services.[48] Additionally, a 2018 report by SPHN found that non-binary individuals reported “more negative experiences with clinicians,” whereby 24% of non-binary people surveyed disagreed or strongly disagreed that they felt listened to during appointments, compared with 11% of those identifying as a binary gender. [49]
One of the biggest issues facing, not just Sandyford, but all GICs in Scotland, is the problem of data management. NHSGGC acknowledged in evidence submitted to the Scottish Parliament Equalities, Human Rights and Civil Justice Committee “that there is an issue with lack of information about individuals on the waiting list and more resources are required to interrogate this and appropriately triage.”[50] In attempts to remedy this issue, the clinic has begun to upgrade the young people’s and adult services’ electronic record system (NaSH). It now includes “a gender identity summary which enables recording of age of onset of gender incongruence and whether before or after puberty, direction of transition, key conditions e.g. ASD, outcome of assessment, psychological, medical, non-surgical and surgical treatments, and de-transition.”[51]
4a.5 Partnership working and cross-clinic links
GIC staff interviewees felt that service capacity has been affected by the lack of shared care between the GIC and GPs. In situations where a GP is unwilling to participate in shared care, one interviewee said that “a service user who may otherwise be appropriate for discharge from the service will be retained for the purposes of prescription maintenance and blood monitoring,”[52] thereby adding to the GIC’s high workload. Another interviewee felt that the lack of shared care created challenges in maintaining effective relationships with GPs. They reflected that, “a big part of the clinical lead’s job is constantly trying to manage that tension with primary care and keep them on side, and that's why there's so much admin.” Offering further context, the staff member felt that GPs are under significant pressure and “like everyone else, they're not doing the things they don't have to do unless they have to do it…[but] I would say the majority of them go out their way.”
An interviewee from General Practice explained that the majority of GPs in Scotland, without expertise in gender identity healthcare, are unable to provide comprehensive gender care. “I think there is, amongst the transgender community, a lack of understanding of what specialist work is and why GPs cannot just prescribe anything and everything … I've had one person say GPs prescribing for transgender women is no different from GPs prescribing a [contraceptive] pill. It’s actually hugely different. It’s different doses, and by definition, the contraceptive pill is used in younger women … but there’s a small group of older [trans] people now, but they’re all going to get older and the risks go up with age. We don’t actually know what the long term risks are. So that’s the biggest reason why this should be specialist work.”
GIC staff interviewees shared their desire to develop a Shared Care Agreement (SCA) with GPs, to improve care for patients and support relationships with GPs. A SCA is a collaborative agreement between a GIC and GP(s) to provide joint care for patients and may involve GPs prescribing hormones or bridging prescriptions, and GPs and GICs working together to monitor and follow-up on gender reassignment treatment.[53] A representative from a GP organisation also highlighted the benefits of shared care, and the clarity it provides to both GPs and GICs as to their roles. However, it was felt that, while GICs had received funding to improve access to, and delivery of gender identity care, General Practice had not been compensated for its time in providing such care to patients or to support the development of SCAs, and had not received SG improvement funding. “Some shared care agreements and some new ones involve new work … and that's generally not resourced … General Practice is the only part of the NHS where productivity has gone up and our funding has gone down.”
With regard to other partnerships, the Sandyford GIC is hosted within the Glasgow HSCP (Health and Social Care Partnership), which manages a range of local health and social care services. The HSCP purchases complementary services from third sector organisations to support LGBTQ+ individuals and their families. This is supplemented with enhanced funding to provide specific support to people who are on the waiting list for, or in active care with, gender identity services.[54]
Interviewees also highlighted the cross-clinic link between Sandyford and the Highland GIC. The Highland GIC has seen an increase in clinical psychologists because of SG funding, and as a result, patients previously referred to Sandyford from NHS Highland have been handed back over. “The Highland service didn’t have psychology within their service [so] what would happen is they would see the medical doctor, who would [say] it looks like you're meeting criteria for gender incongruence, we need to send you to Sandyford for your clinical psychologist.” This in turn meant “a chunk of the waiting list for adults [at Sandyford] was actually Highland patients.” SG funding has allowed the NHS Highland service to employ more staff (see the chapter on NHS Highland), and Sandyford have been able to “pass all those people that [have been] waiting to see for their psychologist assessment back to Highland.”
4a.6 Training and Education
One of the biggest concerns to emerge from interviews was the issue of training and education. There was a strong feeling of ineffectual training on gender healthcare, and as a consequence, staff feeling under-confident when delivering services. When asked in a project questionnaire sent to the clinic: “What training do staff receive to provide care to service users?”, the response from one staff member was, “None. Other than induction there is no formal training for this service.” [55] Similar sentiments were echoed in staff interviews where they stated that “in terms [of] individuals in the service being ... skilled up or [receiving] formal training, there just isn’t any,” which has led to members of staff feeling out of their depth. “We don't have the knowledge and skills and really it should be a specialist service doing that,” another staff member added, “and if you want us to do this medicine, you need to pay us, you need to train us.”
Further issues arise when looking at where this training could come from, given that there is no umbrella organisation or professional body focusing on upskilling staff on gender healthcare. In the absence of an overarching Faculty of Medicine for gender healthcare and without a professional body establishing clear standards for what constitutes good trans healthcare, staff are currently relying on internal resources - turning to their colleagues and other services within their teams - to train each other. “The only expertise we have is within the service within Scotland…so when someone comes to the service, they have to be trained internally from an already very small staffing cohort.” Sometimes this takes the form of shadowing other clinicians and learning “from other people’s experiences” on the job, and for a lot of staff training also comes from “doing your own reading…reading the current policies, the current documents, understanding the political context.”
4a.7 Impacts of the Funding on Service Delivery
A key goal of this report is to better understand the impacts of SG funding on GICs in Scotland. Through interviews with staff at Sandyford, it appears there have been both positive outcomes, coupled with some issues when accessing funding. The clinic received £896,000 over two years, 2022-23 and 2023-24. When they received the first round of funding in December 2022, the clinic was unable to spend it before March 2023. A large portion of this money however was “ring fenced…for staffing,” and for a while, the clinic hired agency staff to help reduce waiting times.
As one staff member stated, “If you look at the data that we're publishing, it looks like waiting times have increased.” However, as they further explained, “more people are being added to the list at a rate faster than we can see them ... but we have more staff and we have been able to pick up new people off the waiting list. Genuinely without that money, without these secondments in place, [this] wouldn't have happened.”
Overall, there was a mix of views about the impact of the SG funding on staff satisfaction. Some interviewees felt that the boost to service capacity, and hiring of new staff, had a positive impact on staff wellbeing, with the team feeling more ‘supportive’ of each other. As one staff member said, “I think the money that's brought new staff members in has probably helped [staff satisfaction] … I’m reflecting back now when I started, even the admin workers were saying, ‘gosh, it feels that we've got a team again.” However, other staff felt morale was slightly lower. One staff member suggested that the structural challenges with recruitment, which could not be easily addressed with funding alone, had impacted the cohesiveness of the team.
Furthermore, one member of staff felt that the SG funding was unable to have a significant positive impact without also considering broader service redesign, including the need to address difficulties of recruiting new staff to this clinical area. They suggested that the SG has been “naive” in their thinking about how to improve NHS gender services, and that money alone “was not going to help.” The SG’s 2022-23 funding allocation letter to NHSGGC included a request that they “obtain external advice on how to make best use of what are limited resources available to them”. The SG also offered NHSGGC access to an external expert with experience of service redesign, with funding to be provided by SG.[56] However, Sandyford GIC considered the external expert to have insufficient expertise in young people’s gender care.[57]
4a.8 Impacts of Funding on Patient Outcomes
Waiting Lists and Patient Numbers
Official statistics in development reported by Public Health Scotland (PHS) found that, as of 31 March 2024, there were 3,283 people waiting for an initial outpatient consultation at NHSGGC adult gender services. Of that number, 510 people (16%) had been waiting between 3-4 years, 601 people (18%) had been waiting 4-5 years, and 167 people (5%) had been waiting more than 5 years.[58] The number of people waiting had increased by 12% (340 people) between 30 June 2023 (2,943 people) and 31 March 2024 (3,283 people). During this period, NHSGGC adult gender services had received 547 new referrals for outpatient appointments. While not forming part of the official statistics in development, the Sandyford GIC confirmed that there were a total of 3,637 individuals on the waiting list for the Adult Service as of 27 August 2024.[59]
Service User Impacts
In July-August 2024, a survey was sent out to users of gender identity healthcare services across Scotland, to enquire about their experiences. It comprised a mix of open and closed questions. The survey received 74 responses. A total of 48 out of 74 respondents to the service user survey indicated that they were either currently accessing, or on a waiting list to access, or had in the past accessed services at the Sandyford GIC. Over two-thirds of respondents (33) were currently on a waiting list to access services, while just under a fifth (9) were currently accessing services and 4 respondents had accessed the GIC’s services in the past but not currently. Table 1 provides a summary of the survey responses for these respondents.
| Current status | No. | % |
|---|---|---|
| Currently accessing services | 9 | 19 |
| On a waiting list | 33 | 69 |
| Have accessed services in the past | 4 | 8 |
| Not answered | 2 | 4 |
| Total | 48 | 100 |
| Has your overall experience with your GIC been a positive or a negative one? | No. | % |
| Positive | 7 | 15 |
| Negative | 25 | 52 |
| Neither positive or negative | 16 | 33 |
| Total | 48 | 100 |
| Since the allocation of additional SG funding (from Dec 2022), have you noticed any changes in how gender identity services are delivered in your area? | No. | % |
| Yes | 6 | 12 |
| No | 30 | 63 |
| Don’t know | 12 | 25 |
| Total | 48 | 100 |
| If you are being seen by a GIC, do you feel that you have a say over the gender identity care you are receiving? | No. | % |
| Yes | 9 | 19 |
| No | 11 | 23 |
| Don’t know | 20 | 42 |
| Would rather not say | 3 | 6 |
| Not answered | 5 | 10 |
| Total | 48 | 100 |
As can be seen in Table 1, just over half of respondents (25) described their overall experience with Sandyford GIC as being negative. Of these respondents, 18 were individuals currently on a waiting list. Many of these respondents described having waited multiple years on the list with little or no contact from the GIC, and with similarly little clarity as to when they may eventually be invited to attend an initial appointment or be able to access any kind of treatment. While some individuals on the waiting list described having accessed private healthcare as an alternative during this time, for others this option was not felt to be financially viable, and several described having experienced feelings of isolation, frustration, anger and resignation as a result of the length of time they had spent on the waiting list. In the words of one survey respondent:
“I have been on the waiting list for 99 weeks and 2 days, with absolutely no communication or support. I feel completely alone, like I can't live my life while I wait for seemingly forever, and I can't help but think the system is stacked against me.”
Even amongst the minority of individuals who described having had a positive experience overall, some described frustrations with aspects of their experiences such as waiting times for second opinions and a lack of correspondence from the GIC. Otherwise, respondents described positive experiences of treatment once they were able to access it, and members of staff being kind and understanding in relation to the difficulties caused by the length of the waiting list. One survey respondent summarised the positive and negative aspects of their experience as follows:
“They have been kind and the staff understand it is difficult to wait so long for so little back. The waitlist for a second opinion has been a nightmare. 3 years to find out if they are going to add you to another waitlist which is already years long is terrible.”
Most respondents (30) said that they had not noticed any changes in how gender identity services had been delivered in their area since the onset of additional SG funding, while a minority (6) said they had noticed a difference. Amongst those who said they had not noticed a difference, some respondents said that this was because they were still on the waiting list with little indication as to when their wait may end, and so any possible improvements in the service had not been noticed by them; while others described having similarly infrequent appointments and slow treatment after the onset of funding as they had experienced before: “I’m still waiting with no contact. I have no idea where I am in the waiting list or what’s happening, just stuck in limbo.”
Amongst the six respondents who had noticed a change since the onset of SG funding, three clarified that they felt the service had changed for the worse, with perceptions of lengthier waiting times and reduced communication. As one interviewee said, “I have seen a decrease in communication to none and a complete reduction in transparency via the website.” Another respondent felt that the waiting list moves somewhat more quickly now than in the past. Finally, just under a fifth of respondents (9) reported feeling that they have a say over the gender identity care they are receiving, while just under a quarter (11) said they did not feel this way. Looking to the future, key themes amongst respondents’ answers when asked how they would like to see services delivered in their area included: increased and more consistent staffing at GICs, greater transparency and communication around waiting lists, more ongoing mental health support (and information on how to access this), and increased training of GPs with a view to them taking on a greater role in the delivery of gender identity healthcare.
In addition to collecting data on patient outcomes through a survey with service users, a small number (3) of follow-up interviews were conducted with patients. A parent of a service user was also interviewed, who described the challenges of accessing the young person’s service. During interviews with service users, there was a recurring theme that those who had received treatment before the COVID-19 pandemic were ‘lucky’ as they had been able to access treatment in a relatively short time frame. One interviewee said, “I got referred to Sandyford about February 2016 and was seen in September 2016 and started hormone blockers in January of 2017. So I was quite lucky with that one.” For other service users, the delays experienced whilst waiting for their first appointment led to them seeking treatment privately or from abroad.
“That [NHS] treatment… you can't get it. [Private] gender healthcare has been life saving for me … I wouldn't have survived three years without doing this privately. I appreciate how lucky I am to be able to afford to do that, but it's been over £100,000 that it's cost me to do these things. But do you know, it's money well spent.”
Service users also highlighted difficulties in waiting for their first appointment, about both the lack of communication and the fear of losing their appointment:
“The initial letter says something along the lines of, when your name comes up, we'll send you an appointment and you have to confirm within two weeks or it'll get cancelled. Which is quite scary because if you missed that, if you were on holiday or something, you would just be off the list and you'd have to start again.”
Whilst the experiences of accessing services may have been negative, service users were keen to highlight that this was not attributable to the staff working in clinics:
“I don't necessarily have any feelings against the staff at Sandyford … I think they're probably doing the best they can, but I think they are overwhelmed and … part of the problem I think is there isn't a pathway for medical students and junior doctors to become gender medicine doctors. And I don't think there's a pathway for nurses to go into gender medicine and become nurse specialists either.”
Whilst some service users have had challenges accessing services at the clinic, others had positive experiences with individual staff, which they shared in interviews. For instance, one interviewee shared that the psychologist undertaking their assessment
“was really thorough and I really valued the fact that she wanted to work out how much of my body issues were to do with hate in my body and feeling a lot of shame around trauma, and how much of it was to do about my gender. She really was just incredible.”
4a.9 Structural and systemic issues
Gender identity healthcare in Scotland is facing embedded structural and systemic issues that filter down and impact the functions of GICs across the country. “There’s no standard of care across the country,” a staff member pointed out during an interview. Consequently, this not only places a large burden upon individual clinics to build their services from the ground up, dependent on the staff specialisms available to them, but it also complicates the cohesiveness of gender identity services in Scotland.
The World Health Organization’s reclassification of gender incongruence away from mental health (for medical reasons) has untethered gender identity healthcare from a defined home, leaving staff attempting to find another place to house it. However, given the lack of an overarching medical body, this leads to broader questions around where to place gender health services. As one staff member reported, “If they are placed in sexual health services … you’d go, wait a minute. What has this got to do with sexual health? It has got nothing to do with sexual health other than the fact that we are LGBT friendly.” The lack of professional medical guidance has led to uncertainty for staff, who have expressed concern around how to implement new standards. “HIS have come out with [draft] standards of care recently and they’re great … a really good kind of idea of what a gender service would look like. [But] it’s really difficult to read that at the moment and just think … who’s going to do that?”
Many staff also felt that the politicised nature of gender healthcare acts as a deterrent for staff coming to work at clinics. A member of staff outlined, “it stops people wanting to work in gender services because it's... such a hotly debated topic.” Even though “we're providing a really high level of care and we're getting good feedback from the people we are reaching out to and working with”, people “have such opposing views about gender identity, gender incongruence” that it stops “good clinicians being able to do their job or be involved in the research and it’s just so needed.” Indeed, Sandyford GIC is supporting longitudinal research by NHS England/National Institute for Health and Care Research into outcomes for young transgender people.
Staff cited concerns around funding, advocating for a permanent funding model for GICs. Temporary funding was seen to lead to job insecurity for staff filling fixed-term positions. As one staff member said, “people can't afford to take one year and two-year contracts. It has to be properly funded…we're not going to be able to make long-term change without that permanent funding and without people being able to come into a service and say, “yep, I'm here for the long haul, let's make a real difference.”
Another structural issue highlighted by staff is the complicated pathways of care. These “pathways need [to be] much more clearly delineated…they're not really written down,” one member of staff suggested in an interview, before outlining the following:
“[T]he type of patients that present to the service have changed a lot over the last decade…Ten years ago people would come to us and be questioning their gender and wanting to know what their options were. Over the last ten years, there’s been a big increase in the number of gender non-conforming identities…But also because of the increase in waiting lists … by the time they see us, [they] have pretty much socially transitioned, but now quite commonly have [also] had treatment in the private sector, so they may have started hormones [and had] surgery … Previously we dealt with everybody the same no matter if they'd had private treatment … But the population has completely changed and we're not really sure how to deal with that in a fair way.”
4a.10 Conclusion
To help evaluate the effects of SG funding on services at Sandyford GIC, we have developed a bespoke Theory of Change (ToC) for NHSGGC, shown below. This is based on the main ToC presented at the start of this report, and then tailored to NHSGGC based on its aims for the SG improvement funding, the activities they have since undertaken, and the outcomes these changes are leading to.
Situation:
- Wider structural context (high demand for services, long wait lists, overstretched staff, lack of specialists, high media attention)
- Consideration of local context (Adult Service: referrals from seven Health Boards; Young People’s Service: referrals from across Scotland)
- Fostering collaboration / relationships (arrangements with primary care, links with other GICs, links to third sector)
Inputs:
- Total of £1.3m SG funding allocated to NHSGGC over 2022-25 to improve gender services
- Use of this funding by NHSGGC to support several activities:
- Increasing capacity to see patients, deliver assessments and develop care pathways
- Developing understanding of patient need
- Building a demand profile to inform service planning
Activities:
- NHSGGC implementing plans to improve services, in line with funding:
- Improve triage and signposting of adult patients
- Carry out recruitment to GIC team
- Build partnerships with third sector to support patients
- Put in place agreed care plans reflecting patient needs
- Coordinate care with referring Boards
Preconditions:
- Robust data & evidence
- Specialised training on gender identity for GIC staff and general training for mainstream NHS staff, to enable joined-up care
- Safe and fulfilling workplaces
- National, local and regional leadership
- Empowered and resourced staff, able to confidently make decisions
- Shared care GP agreements
Outcomes:
- Changes to meet the needs of patients (improved wait times, support for those on waiting list, increased understanding of patient need)
- Changes to understanding of systems (validation of waiting lists, better recording of data)
- Changes to governance of systems (clearer referral criteria, revised pathways and processes, stronger links to other GICs)
Impacts:
- Realistic Medicine vision:
- Empowered patients, Personalised Care, Informed Decisions, Joined Up care
- GIC-specific:
- Accessible, inclusive services (including pre-service support), educated workforce, sustainable and well-funded services, good governance, strong networks, mainstreamed care, reduced inequalities
Data collected for this case study suggest that the SG funding has helped Sandyford GIC implement positive and necessary changes to help improve their services, in line with the Theory of Change set out at the beginning of this report. The funding has enabled the GIC to hire additional staff members and agency staff to help tackle waiting lists, and without such funding, staff believe this would not have been possible. The funding has allowed staff members to undertake administrative and strategic tasks, such as streamlining the internal process for patients and building up a comprehensive picture of patients waiting to be seen, to develop a better understanding of the demand profile. SG funding also provided for more time and space for staff to strengthen third sector links. These activities are aligned with the goals set out in the NHSGGC funding proposal, and have met with some positive outcomes.
However, many of the service improvements made by Sandyford GIC have not trickled down to adult service users, resulting in some of the outcomes and impacts set out in the ToC not yet being achieved. This is partly due to increasing demand and lengthening waiting lists, combined with the challenges the GIC has experienced in seeking to recruit staff to key posts. Respondents to the survey and interviews for this project highlighted their frustration with the long waits, with little to no communication or support from the GIC during the period that they were waiting. This has led to a feeling of isolation and uncertainty for people on waiting lists, who described a sense of being ‘stuck in limbo’. Service users who were able to access services described a more positive experience, especially in accessing Psychology services, and there was a sense of understanding that the staff were trying to do their best with little resources. When asked about the impact of SG funding, the majority of service user participants did not see any difference in services at Sandyford GIC. Many service users also described feeling ‘lucky’ to be able to access services after long waits, rather than viewing this as a basic right to healthcare. Notably, some patients on long waiting lists were able to purchase private gender identity healthcare, while others were unable to do so, suggesting that there may be growing inequalities in accessing care.
Another potential explanation for why some of the outcomes and impacts have not yet been achieved at Sandyford GIC may be due to the absence of key preconditions, which are necessary for activities to lead to outcomes. Notably, staff have expressed frustration around the lack of comprehensive training for GIC staff, as well as the dearth of education available to the general NHS workforce on gender identity healthcare. Staff have also drawn attention to problems around data collection and sharing in NHS data systems. The Sandyford GIC does not have shared care in place with GPs in NHSGGC; moreover, it is the responsibility of the other six other Health Boards and the Argyll and Bute Health and Social Care Partnership that are referring into Sandyford to facilitate shared care agreements via their Local Medical Committees. Finally, staff have shared their concerns around safety and wellbeing at work, especially due to the politicised nature of debates and media focus on the clinic.
Therefore, while the SG funding has begun to improve conditions for the clinic, Sandyford still faces overarching changes in delivering services in line with the Realistic Medicine vision and the impacts set out in the ToC. The absence of key preconditions at the local and national levels, combined with challenges in staff retention and vacancies and the politicised nature of the debate around services, has hindered the GIC’s ability to achieve all of the outcomes set out in its proposal. This may be remedied in future by leaders at the local (GIC) and regional (Board) levels putting in place a number of best practice learnings - which are elaborated in full towards the end of this report - around the development of a strong, cohesive team culture, a focus on staff wellbeing, strong communication with patients, clear and consistent pathways, and proportionate workloads across Health Boards. Furthermore, the GIC may benefit from the implementation of best practice at the national level, including long-term funding, standardised models of care, and comprehensive training to ensure Sandyford GIC is able to fully support patients and staff.