Gender identity healthcare: evaluation of the impact of Scottish Government funding
This report presents findings of an independent evaluation into the impact of Scottish Government funding, as allocated to NHS Health Boards, to implement local work to improve access to, and delivery of, gender identity services. The evaluation covers period between December 2022 and August 2024.
5. NHS Highland - Adult Services
5.1 Overview of the clinic
The NHS Highland Gender Identity Clinic (GIC) is based in the Highland Sexual Health Service at Royal Northern Infirmary Community Hospital in Inverness.[73] The GIC provides adult gender identity services to patients living in the NHS Highland Board area[74], with no other Boards referring in.
Current staff mix
The core staff of the NHS Highland clinic currently comprises:
- 1 speciality doctor working within the service on 0.4 WTE (2 days pw)
- a gender identity nurse practitioner who works 3 days a week (on a 0.6 WTE contract, of which 0.2 WTE is SG non-recurring funding)
- an endocrinologist consultant support working on a 0.05 WTE contract (which is Scottish Government non-recurring funding)
- a Gender Identity Psychology Service comprised of a Lead Psychologist, and 2 bank psychologists (totalling 0.4 WTE, from non-recurring SG funding)
- Gender administration support on 0.6 WTE (of which 0.2 WTE is SG funding)
- a gender identity clinical lead has just been recruited to the service (0.1 WTE)[75]
In total, therefore, the Highland GIC Adult Service draws on the equivalent of 2.15 WTE staff, as of May 2024.[76] In addition to core staff, the GIC receives support from other NHS Highland teams: Speech and Language Therapy and Psychosexual Therapy (within the wider Sexual Health service). Psychiatry/Psychology do not provide support to the GIC, but GIC patients may be referred to Mental Health for comorbid mental health problems. The current staff have built up considerable experience in delivering gender identity healthcare services and offer training to other organisations.
Service History
The GIC has always been based within Sexual Health Services at NHS Highland. According to one staff member, the clinic was established by a consultant in the genito-urinary field in sexual health, who was inspired to create a gender identity service for patients with gender dysphoria in the Highland area after working at a similar clinic in New Zealand. Together with a consultant psychiatrist and psychologist, he was able to provide a skeleton service, including psychological assessments sought externally from the Sandyford Clinic and hormone prescriptions provided internally. In 2016-17, a new clinical lead was hired, with a background in general practice who was based in Sexual Health. They began working one day a week “to take on the cohort of patients and any new ones” and to build structures around the clinic. A nurse was also hired, with a mental health background, who worked two days a week at the clinic, alongside continued external assessments from Sandyford GIC.
At the time, patient numbers were relatively low, and, as stated by one staff member, patients were “coming in for prescriptions or for injections. GPs weren’t particularly involved.” In 2017, the GIC was managing 85 patients, and the following year, it received NHS Highland funding to hire a Speciality Doctor who was employed on a 0.2 WTE contract at the GIC; a Psychosexual Therapist who provided 0.2 WTE psychosexual counselling support to individuals across the whole sexual health service, a gender identity nurse on a 0.4 contract, and admin support on a 0.2 contract.[77] When funding was allocated in 2017-18, there was no direct access to Endocrinology services for patients, and limited access to clinical psychology services. At that point, the Highland GIC was referring patients to Endocrinology at Grampian, with whom they had a close relationship, and psychological assessments were sent to the Sandyford clinic. The GIC was also relatively fragile due to its small staff team. For instance, according to one interviewee, in 2021 the GIC was unable to take on any new patients “following the sudden resignation of the GI nurse,” despite demand for services growing.
In June 2022, NHS Highland submitted a funding proposal to the SG to expand the GIC team and its services to patients, to bring endocrinology and psychology services in-house, and to put the GIC on a more sustainable footing.
5.2 Scottish Government Funding Proposal
The total amount of funding applied for by NHS Highland was £60,133 for 2022-23, which was anticipated to be a recurring annual cost for the years 2023-24 and 2024-25. After submitting the proposal, NHS Highland received £20,000 in December 2022 to support work (over 4 months remaining of the year) in 2022-23; it received £70,500 to support work in 2023-24; and £70,500 to support work in 2024-25. The total funding allocation for NHS Highland for the three-year period of funding 2022-25 was £161,000.
The NHS Highland funding proposal sought to create a multidisciplinary team (MDT) within the service because, as they suggest, “[m]ultidisciplinary collaboration helps to ensure equity of access and clinical effectiveness for all patients accessing gender reassignment.”[78] In securing SG funding, the aims of the Highland GIC were to:
- engage more with endocrinologists which, up until recently, was supplemented on an ad hoc basis by endocrinologists in NHS Grampian
- strengthen internal psychological support and “provide those accessing the service with access to clinical psychology referral”
- provide additional nursing time to engage with those currently waiting to be seen, and to engage further with third sector organisations to help facilitate support networks locally
- increase administrative support to assist with “management of the increased referrals and to engage with individuals who are waiting to be managed by the service” while also providing online and physical resources[79]
The proposal for SG funding provided a list of new staff members it wished to hire, including a consultant endocrinologist, a specialist nurse, a clinical psychologist and admin support. With this additional support, NHS Highland sought to:
- improve access to services, e.g. provide a dedicated ‘Live Chat’ with a nurse who is available on a regular basis to deliver evidence-based advice and signpost to appropriate resources
- improve access to clinical psychology locally, e.g. adopt a more person-centred, multidisciplinary approach to care
- provide locally supported endocrinology services
- increase administrative support which will ensure “the workload generated by the reduction in waiting times is managed in a timely manner, reducing the need for duplication of work and streamlining patient processes”
When describing how the funding proposal links to wider Health Board activities to reduce waiting times, improve data collection and support those impacted by long waiting times, NHS Highland detailed their Together we care strategy (a set of objectives to be completed over the next five years). These objectives include delivering the best possible health and care outcomes for the population, reducing barriers to access, and improving experience and outcomes through co-production. The proposal also outlined how the service was expected to run with additional staff, including endocrinology (4 clinical sessions per month), clinical psychology (1 session per week), speciality doctor (1 session per week), nurse (3 sessions per week) and administrative support (3 days per week).
In an interview with GIC staff, following the allocation of SG funding, current priorities within the NHS Highland service were highlighted: “[t]he priorities now are probably a bit different than they would have been even a year ago, because the wait time for the first psychological assessments are down so significantly now. So now I think it's more about efficiency within the system.” According to the staff member, efficiency in this context meant a greater coordination of services within gender identity healthcare, e.g. getting initial psychological assessment and then being prescribed hormones quickly, without a significant waiting period, with the same degree of speed being applied to prescriptions, speech and language, and hair removal.
5.3 Mapping the System
When asked in a project questionnaire about current service models and the main partners (both within and out of the NHS) supporting patients throughout the process, NHS Highland reported how they had links with speech therapy, gynaecology, sexual health, endocrinology and administrative staff within the NHS. And for those outside the NHS, the clinic has links with GPs who refer into the service; the University of Highlands and Islands; clinical health psychology; psychosexual psychology and counselling (that the GIC can refer to); and third sector organisations such as Trans Scotland and LGBT Health and Wellbeing. During staff interviews, a member of the team referred to the layout of the service as a “weather hub…[with] these little spokes coming off”, with the team comprising, at full capacity: one speciality doctor, a clinical lead, a nurse, administrative staff, and the aforementioned spokes as a team of clinical psychologists, endocrinologists, speech and language therapists, people doing hair removal, and those who specialise in fertility preservation.
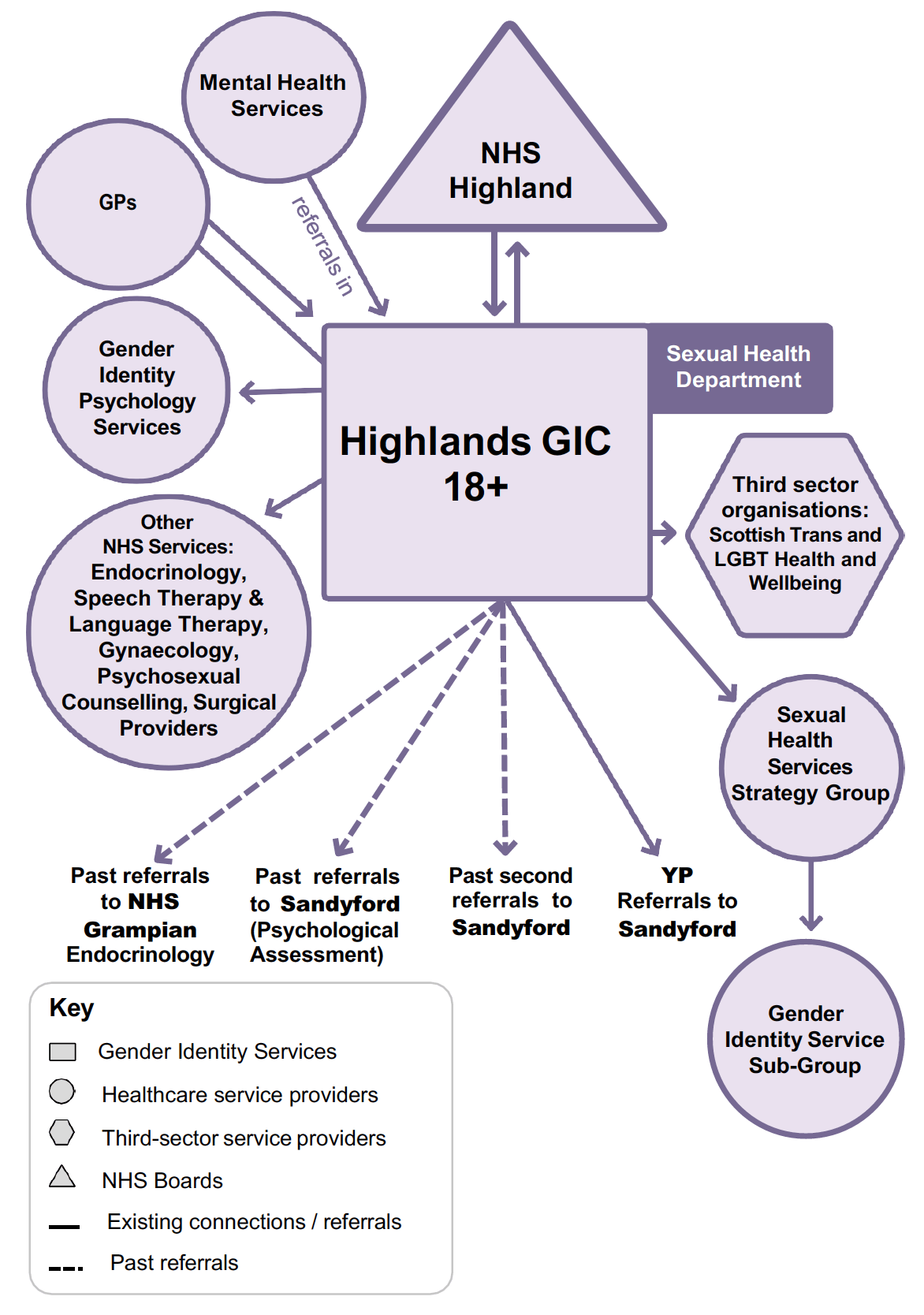
The system relationships map for the Highlands GIC demonstrates how this system has become a mature, well-resourced and joined-up system. As mentioned, the clinic is based in Sexual Health in NHS Highland, where it receives additional support from sexual health staff, and has created a Gender Identity Service Sub-group. It has also developed links with NHS Highland Psychology, where it has been able to develop a Gender Identity Psychology Service. Finally, the clinic has arrangements in place with other secondary healthcare service providers, such as endocrinology and speech and language therapy services. GPs make referrals into the GIC, and it refers out. The clinic also has growing links with third sector organisations, although it has been noted that there is limited local third sector provision specifically for trans and non-binary identifying individuals in NHS Highland (whereby local services are more under the wider LGBTQ+ umbrella). Staff within the GIC have been engaged in outreach activities, including informal training of staff in mainstream services and public education. Staff have good levels of training and the GIC is seeking to hire more staff. In the past, the GIC made referrals for psychological assessments to Sandyford, and referrals for endocrinology services to Grampian, but both services are now housed within NHS Highland. Patients under the age of 18 seeking gender identity healthcare are referred to the Sandyford Young People’s Service in NHSGGC.
5.4 Services being delivered
Based on responses to an evaluation project questionnaire, the NHS Highland GIC confirmed that its current gender identity service works in the following way. When patients reach the top of the waiting list, they are invited to attend an initial clinical assessment (or ‘triage’ appointment) to gather essential clinical information and provide a point of access for wider sexual health where indicated. From there, the patient will be referred for psychological assessment. Following the psychological assessment, the patient will then have any recommendations actioned, which may include fertility preservation, hormone therapy, speech and language therapy, hair removal, or surgical referrals, all of which are managed within the main GIC.[80]
A gender specialist reviews referrals to then be added to the waiting list. If patients have been on the waitlist for another NHS GIC, Highland honours their original referral date. Patients are always seen according to their referral date; there is no fast-track or priority list. For those waiting for their initial clinic appointment (before the psychological assessment), the clinic currently has a resource pack to share with patients to provide support, advice, and networking. Clinical advice is also provided to GPs should they contact the clinic. In response to a questionnaire question asking if the SG funding had made a difference to the way NHS Highland was able to deliver services and improve patient outcomes, the reply from the GIC was: “Yes, MDT formed, governance strengthened, local services for local people, investment in Endo and psychology locally, pathways need streamlining, waiting times will drop significantly over time.”[81]
When thinking about service delivery, the Highland GIC service operates through a referrals process, which primarily comes from GPs, although occasionally referrals come from sexual health services when the individual does not wish for their GP to know. Face to face clinics are managed by the medical team at the service, and are carried out in person with the option of selecting ‘Near Me’ (video appointments) for those who prefer it. This choice is opted for more regularly in remote and rural areas. In the service currently, there are around 2 days per week of clinical psychology time.
The GIC faces some challenges however, due to the small size of the team. The lack of administrative staff had previously hindered the GIC’s ability to forge stronger links with third sector organisations. This is one of the GIC’s aims for the SG improvement funding, and the increase in the gender identity nurse practitioner’s hours has since enabled them to focus on strengthening ties with the third sector. The lack of ample administrative support has also meant that nurses and medical staff are often undertaking administrative tasks, such as managing onward referrals for patients, which has led to issues of overwork to meet the workforce gap.
Staff also cited issues raised to them by service users. Some service users complained that they did not feel comfortable in the GIC waiting room in the previous location (Raigmore Hospital), and other individuals expressed their frustration over having to travel long distances to access services because there are currently no local provisions in place (that is, they cannot be seen at their GP practice). In an attempt to rectify some of these issues the GIC has introduced telephone consultations and has reinstated a live chat functionality which was inaugurated during the pandemic. Staff stated in interviews that this is an online service “and it means that young people can access a nurse specialist Monday to Friday online through our website and chat online with them.” Staff have additionally tried hosting ‘live chats’ around gender, but these were not well attended events. To better understand what sort of support patients on waitlists wanted from the clinic, staff sent around a survey but only received three responses.
Staff have run into further problems when trying to work with GPs. As described by one interviewee, some GPs are “ridiculously good in administering injections, prescribing, monitoring, and arranging blood tests [while] others will say, it’s nothing to do with us, we’re not allowed to do that”. One interviewee cited the example of a patient who is on three weekly injections and has to get two buses from over an hour away because their GP will not administer the injections. This in itself, staff felt, places patients in a vulnerable and potentially dangerous situation, “especially when they’re early on in their transition and people don’t accept them – it can be dangerous to go out on two buses into town.” A staff member of an organisation representing General Practice expressed similar concerns about patients needing to travel long distances for prescriptions: “if you're in Highlands and Islands, it’s not feasible for somebody in a remote island to go all the way to Inverness for a blood test, for instance. So I think there you would need to have a Shared Care Agreement that was local, but with specialist oversight, which can be distant.” They felt that a Shared Care Agreement, with clarity around roles and which was resourced for GPs engaging in new work, would help improve patient care.
5.5 Partnership working and cross-clinic links
When thinking about cross-clinic links that Highland has with the three other GICs in Scotland, there are “meetings that take place nationally…with clinical staff within the gender service,” one Highland staff member suggested in interview, “and some of that is kind of peer support as well as learning from each other.” They continued:
“I think the meetings that we're having as a result of the funding has increased and improved communication and I now know who the people are who work in the different clinics, which I would never have had any idea of previously and it would have been a struggle to try and find out who you need to speak to for any given thing.”
“[W]e've got at least a few links in each gender clinic, especially with Lothian,” one staff member explained. Interviewees reflected that Highland had a solidified relationship with the Lothian GIC, with one member of the team recently visiting the Chalmers clinic for a day to observe the day-to-day process of their clinic. Additionally, Lothian are “in the process of publishing shared care guidelines and which…we would hope that that is something that we would emulate in Highland.” In addition, historically, NHS Highland would refer patients to Sandyford GIC for psychological assessments, where patients would be added to a waiting list, and work closely with them. However, that service has been in-housed within NHS Highland as a result of the SG funding. Finally, in the past, endocrinologists in Grampian GIC provided a lot of (unpaid) support to Highland GIC Speciality Doctors which helped establish the clinic. Therefore, there appears to be good cross-clinic working between NHS Highland and all three other GICs in Scotland.
5.6 Training and Education
One of the main systemic issues facing GICs in Scotland today is access to training and education on gender healthcare, and as a result, NHS Highland has found it “a challenge” to train current and new staff. This lack of training also has a knock-on effect on the hiring process. As one interviewee stated, “people are not attracted to come into gender as a clinical area because they’re fearful…because of the political climate, never mind the fact that there’s not a clear training and supervision pathway.”
Much like the Sandyford clinic, staff at the Highlands are turning inwards to provide their own training and knowledge sharing. One staff member said, “I knew what I was talking about in terms of psychological assessment … [w]hy would I not use that information to disseminate to others? It just seems like common sense.” During interviews, staff suggested the need for a new knowledge, skills and training framework that “needs to be very clear.” Staff felt that it should not only encompass the full remit of gender healthcare, such as psychological assessments, hormone prescribing etc, but also training on “trans awareness in a very broad manner.” This awareness-raising was considered to be important in the face of “skewed and fear mongering” media representations of trans and non-binary identities.
Not only do these gaps in training and education exist in GICs, staff suggested, but they also exist in GP clinics. “A lot of [GPs] don't feel comfortable and…it’s a lack of education,” one staff member reported. “We find that, you know, if somebody went to dermatology, somebody went to see ear, nose and throat, and then they had a treatment recommendation sent to the GP, the GP would quite happily prescribe it on recommendation of a specialist. But as soon as it comes to gender, they go. Whoa, no.” A staff member representing General Practice explained that hormone prescriptions for trans and non-binary patients required specialist oversight, especially regarding long-term impacts and possible interactions with other medications, and that a Shared Care Agreement could provide clarity for GPs around gender identity prescribing.
5.7 Impacts of the Funding on Service Delivery
Prior to receiving the SG improvement funding, NHS Highland was running a fragile skeleton service with one specialty doctor, a nurse working two days a week, and patients referred to Sandyford GIC for psychological assessments. The service was “almost [a] one man band and…it was a very, very small service with one clinician who worked one day a week and one nurse,” one staff member commented.
Staff felt that the SG funding “provided an opportunity for NHS Highland to change the way they manage patients in [the] Highlands,” and now the clinic operates an MDT service (recruiting psychology and endocrinology staff) which is safer and more secure, from a governance perspective, according to staff in interviews. This new model of care, while taking time to implement, and negatively increasing workloads currently, will eventually result in a more streamlined system of work, staff felt. New admin staff has also provided capacity for nurses to build stronger connections with the third sector. Finally, in addition to the Gender Identity Service Group Meeting which looks at strategic improvements in the delivery of care, NHS Highland also has a well-attended functioning Clinical MDT that takes place monthly. The GIC is also starting to produce a number of Standard Operating Procedures which clarify processes for access and referrals in line with the relevant updated national documents, e.g. the new protocol.
One of the biggest changes seen at NHS Highland is around psychological assessments, which are now also conducted within the Board. “We have invested in psychology services,” one member of staff commented when discussing the use of the SG funding, “we have a number of hours going to the psychology service per week,” they continued, before highlighting the impact of the funding on psychology services:
“It allows us to be flexible with the psychology funding and what we did last year [we] will likely do again this year if we have sufficient funding…if it looks like we're spending less in other aspects, then we will plough that into psychology because it's those assessments that patients are really waiting for as the first step of their journey.”
The in-housing of psychology at Highland GIC has enabled the clinic to conduct psychology assessments (often online), rather than referring patients to Sandyford GIC for psychology assessments as previously. Psychology staff at NHS Highland have been working their way through the backlog of patients who were on the Sandyford waiting list, and this process has recently been completed. One staff member previously anticipated that the process would be significantly quicker: “once those last patients on the Sandyford waiting list have been cleared, that is when we will start to see our waiting times reduce.” Another staff member noticed an immediate improvement to the current waitlists after in-housing psychology assessments. They said “I can't even begin to say how much it's made a difference for patients, the people who are being seen by psychology now were referred for psychology like at the end of last year, not two years ago.” Staff now feel confident that these new changes in working will help decrease waiting times, which without the SG funding, would not have been possible. Staff wellbeing has also improved as a result:
“I think it's really interesting to see how a very small amount of money in the right hands can make a difference…and will continue to make a difference. I know…from speaking to staff that they are feeling much more supported and have more people that they can get peer support from as a result of it.”
The GIC has since developed stronger relationships with secondary teams across NHS Highland, in particular with Psychology and Endocrinology services, enabling faster communication and better patient support.
5.8 Impacts of Funding on Patient Outcomes
Waiting Lists and Patient Numbers
Official statistics in development reported by Public Health Scotland (PHS) found that, as of 31 March 2024, there were 94 people waiting for an initial outpatient consultation at NHS Highland adult gender services.[82] The number of people waiting had increased by 25% between 30 June 2023 and 31 March 2024. During this period, NHS Highland adult gender services received 55 new referrals for outpatient appointments. While not forming part of the official statistics in development, NHS Highland GIC confirmed that it was supporting 179 patients, with 99 people on the waiting list, as of May 2024.[83] In response to a questionnaire carried out as part of this evaluation, the GIC reported that waiting list numbers had not yet changed significantly since the allocation of SG funding, which they attributed to the inclusion of individuals previously referred to Sandyford for psychological assessment in Highland GIC’s waiting list numbers, in addition to the recruitment and training requirements of Psychology. The GIC anticipates that once these individuals (now being managed locally) have been assessed, the waiting list will reduce in number.
Service User Impacts
In July-August 2024, a survey was sent to users of gender identity healthcare services across Scotland, to enquire about their experiences. It comprised a mix of open and closed questions. The survey received 74 responses. A total of three out of 74 respondents to the survey indicated that they were either currently accessing, on a waiting list, or had in the past accessed services at NHS Highland GIC. Two of these respondents were currently accessing services, while one was currently on a waiting list to access the service. Table 2 below provides a summary of responses.
| Current status | No. | % |
|---|---|---|
| Currently accessing services | 2 | 67 |
| On a waiting list | 1 | 33 |
| Have accessed services in the past | 0 | 0 |
| Total | 3 | 100 |
| Has your overall experience with your GIC been a positive or a negative one? | No. | % |
| Positive | 2 | 67 |
| Negative | 1 | 33 |
| Neither positive or negative | 0 | 0 |
| Total | 3 | 100 |
| Since the allocation of additional SG funding (from Dec 2022), have you noticed any changes in how gender identity services are delivered in your area? | No. | % |
| Yes | 1 | 33 |
| No | 2 | 67 |
| Don’t know | 0 | 0 |
| Total | 3 | 100 |
| If you are being seen by a GIC, do you feel that you have a say over the gender identity care you are receiving? | No. | % |
| Yes | 2 | 67 |
| No | 1 | 33 |
| Don’t know | 0 | 0 |
| Total | 3 | 100 |
As Table 2 shows, out of three survey respondents, two indicated that their overall experience with the GIC had been a positive one, while one described it as negative. Positive aspects cited by respondents included an excellent standard of care, and the presence of supportive and understanding staff at the GIC:
“I've been very lucky. NHS Highland is brilliant for gender care.”
“[E]veryone I spoke to at the Raigmore GIC [was] great, understanding and supportive.”
Less positively, all respondents expressed a desire to see shorter waiting times, with two describing in some detail the lengthy and at times arduous processes they had been through in their attempts to access different aspects of gender identity healthcare. As described by one respondent:
“A long and tortuous process, even setting aside the extra 3+ years resulting from covid [...] My fairly consistent experience throughout the process has been of very little proactive help with all the practical organisation of so much out-of-area consultation and treatment - most of the time I have had to invent the wheel anew for myself.”
Only one of the respondents said they had noticed changes in how gender identity services were delivered in their area since the onset of additional SG funding in December 2022, with the other two saying they had not observed any differences. For one, this was because they had still been on the waiting list at the time the additional funding had been allocated and so was not able to compare services before the funding to after, while another said that the main difference that they had noticed during this period was the impact of “Covid delays” on some aspects of treatment.
Finally, two of the three respondents expressed a feeling that they did have a say over the gender identity care they were receiving. Looking to the future, ideas expressed by respondents as to how gender identity healthcare in the NHS Highland area could be improved included more links between the GIC and relevant charities and the provision of additional staff and resources to reduce waiting times for different aspects of care.
The additional interviews conducted with survey respondents shed further light on some of the issues raised above. Some interviewees felt that they were lucky to have comparatively short waiting times in NHS Highland in comparison to other services.
“I first spoke to gender services in maybe September [2020]. So it's a really short waiting time comparatively in the Highlands. So it was maybe six or seven months later, they said that they were happy to progress things [...] the gender doctor was amazing. I felt like she had just heard it all before, and that was such a nice feeling … So I felt very reassured by her. And I felt that she was OK with the fact that I didn't really have any idea of what I wanted, I had no idea about a destination. And I felt that she was very willing to just let me see how things progressed, but be there along that journey.”
One interviewee contrasted the positive, welcoming and inclusive approach adopted at staff at the Highland GIC, compared to other NHS clinicians they had consulted:
“the GP and psychiatrist and CPN [community psychiatrist nurse] … I felt fear from them, like anxiety and fear. And it felt more about them than it did about me. It felt more about them not knowing what to do and them not being experienced, and therefore it felt like they were kind of panicking then sort of thinking, oh no, this is just another thing that we thought we had a handle on this person, and now you're just throwing something completely different into the mix. So it felt like it was overwhelm, a lack of knowledge, rather than concern about me, and so I felt quite rejected by that.”
Fortunately, for one interviewee, they felt they received the care they needed and were “lucky because the access to Highland services is so good.” The service user expressed how easy it was to contact the GIC and receive their help, whereby they could “just phone them up” and the receptionist would answer their queries and arrange for other colleagues to follow-up with information and support. Another interviewee expressed their appreciation of staff going above and beyond, in order to support their wellbeing, recalling how one clinician at the GIC:
“would just call me, maybe every couple of months on her way home from work. Because things were really rough [for me], it wasn't a great time. So she would just sort of check in every so often and say, we're just waiting for this or that appointment, and she gave me loads of different signposting stuff like, like Facebook groups. She tried to find out different things that I could get involved in. That was really useful because I wasn't coming at it from being part of the community.”
However, interviewees were also aware that their positive experience with NHS gender identity services was not necessarily universal, and that within their peer groups they had heard many stories of others being fearful of disclosing their mental health issues to clinic and secondary staff, in case it resulted in their treatment being halted:
“People are terrified about how bad their mental health is when they're waiting for gender services. They might say a bit, but they hide so much because they're frightened they're not going to get the treatment if they're honest. You hear people being frightened to say to their surgeon, I've got top surgery next week, but I'm really struggling with self-harm and this and that. But I can't tell anybody because they won't give me top surgery ... So it's a really polarising feeling, like you've got to pretend that you're OK in order to get the services, but you're also not OK and that's why you need it. It's a really difficult balancing act. I don't know how much the professionals really understand that.”
One interviewee also made suggestions about how to improve support for patients on waiting lists for their initial assessment and different gender identity treatments, including the proposal for a collective care class for trans and non-binary patients, similar to for instance antenatal classes offered to pregnant women:
“I feel like there's a gap for peer-led NHS services … if you did, say, six-week courses for people that are new on waiting lists, or people that are going for a particular type of surgery, then it could be guided by staff, and you’d develop support networks for people going through the same experience. I think it would be useful for people who may be on a similar journey [and] good for people’s mental health and help people to cope with the waiting times … I’ve been involved in amputee group therapy groups [in my job] and you get people in and they're all doing it together. And that's what works.”
Finally, one respondent to the survey of third sector organisations carried out as part of this research reflected positively on the impact of the funding on patient outcomes in the Highlands, citing Highland GIC as an example of a GIC which has “managed to cut waiting lists considerably, which has been really positive.” The respondent felt this had been achieved by “changing the skill mix of staff at the clinics and using MDTs, which means they are impacted less by staffing shortages and able to recruit from a wider range of healthcare practitioners.” As a result, the respondent observed that “trans and non-binary people seem to be feeling positive about the direction of travel” at the GIC. This view was reiterated in an interview with another third sector representative, who felt that NHS Highland has been successful in decreasing the waiting list.
5.9 Structural and systemic issues
One of the issues experienced by NHS Highland, in relation to their funding allocation, was the short timeframe allotted to initially spend the money in year one. The first batch of SG funding came through in December 2022, leaving the clinic three months - from January until March - to spend it. This inadvertently prevented the clinic from using it for recruitment due to the short timeframe. While staff were pleased to receive government funding, concerns and questions were raised about what happens to Highland GIC services once the temporary, finite amount of funding runs out.
Additionally, further issues arose around the topic of gender identity healthcare for clinicians. As one member of staff pointed out, “there’s a lot of good, competent clinicians out there [but] people are fearful that gender [is] so different and they can’t,” which, as highlighted at various points throughout this report, leads back to broader issues of a lack of formal training and education around gender identity healthcare.
Issues around staff recruitment and retention and training converge with systemic challenges around specialism gaps and staff support. As one member of staff reported, “a priority for me is about supporting the staff.” When staff leave and take their expertise and knowledge with them, it leaves gaps in experience, with existing staff attempting to fill them. “I’m trying to use my skills to try and create a sort of supportive environment,” one staff member relayed, “because happy staff is going to mean happy service users… I think it’s something that's overlooked time and time again.”
However, there is also an awareness amongst staff members of the potential fragility of GICs in Scotland given that they are relatively small, new and under-resourced, and with that there was a strong desire reported to be proactive in addressing structural and systematic issues to ensure the long-term sustainability and viability of the GIC.
“People say, oh, well, that's [the GIC] not really very important, you know? And I did have one of my medical colleagues go, ‘well, when you retire, the gender clinic might just not exist anymore if you’re not around’, just taking a very laissez-faire attitude like it wasn't prioritised at all. But our service manager has made sure that was never going to be the case, that we had to find a way to make it work. Which has been brilliant.”
In interviews, clinic staff raised initial “concerns about service resilience and patient safety as the standalone Speciality Doctor is due to retire in 2024”, leading to concerns around the “failure to establish succession planning for the service result[ing] in potential dissolution of the service within NHS Highland.” However, the clinic was able to build support from the NHS Highland Health Board to ensure the future sustainability of the service, aided by the SG funding that increased the visibility of the clinic within NHS Highland and enabled the GIC to hire a new clinical lead in the summer of 2024 to ensure the viability of the service.
The GIC has been putting the necessary systems and structures in place to put the GIC in a strong position going forward. A range of actions were reported such as increased support from the NHS Board as a result of the SG funding; developing clinical governance structures and gender identity sub-groups within existing NHS teams; inserting GIC agenda items on NHS team discussions; in-housing endocrinology and psychology services within NHS Highland so they are not reliant on other GICs to provide these services; developing stronger relationships and outreach with GPs with the goal of creating shared care agreements in NHS Highland; developing closer relationships with local and national third-sector organisations; and providing training and education for NHS teams and the public at large.
5.10 Conclusion
To help evaluate the effects of SG funding on services at NHS Highland GIC, we have developed a bespoke Theory of Change for NHS Highland, shown below. This is based on the main ToC presented at the start of this report, and then tailored to NHS Highland based on its aims for the SG improvement funding, the activities they have since undertaken, and the outcomes these changes are leading to. Situation:
- Wider structural context (high demand for services, long wait lists, overstretched staff, lack of specialists)
- Consideration of local context (largely rural catchment area; historic referral links to Sandyford / Grampian GICs; need for succession planning)
- Fostering collaboration / relationships (relationships with third sector, clinics, GPs)
Inputs:
- Total of £161k SG funding allocated to NHS Highland over 2022-25 to improve services
- Use of this funding by NHS Highland to support activities, by:
- Creating a multidisciplinary team within the service
- Involving NHS Highland endocrinologists/ psychologists with the service
- Increasing nursing capacity / admin support
Activities:
- NHS Highland implementing service improvement plans:
- Carry out psychological assessments
- Increase collaboration between NHS Highland teams across the patient pathway
- Build partnerships with 3rd sector
- Provide training to newly recruited staff
- Establish GIC succession planning
Preconditions:
- Robust data & evidence
- Specialised training on gender identity for GIC staff and general training for mainstream NHS staff
- Safe and fulfilling workplaces
- Local, regional and national leadership
- Empowered and resourced staff, able to confidently make decisions
- Shared care GP agreements
Outcomes:
- Changes to meet the needs of patients (improved wait times, improved assessment processes, new MDT model)
- Changes to understanding of systems (stronger connections with 3rd sector, staff training, increased engagement with primary care)
- Changes to governance of systems (streamlined patient processes, management of admin workload)
Impacts:
- Realistic Medicine vision:
- Empowered patients, Personalised Care, Informed Decisions, Joined Up care
- GIC-specific:
- Accessible, inclusive services (including pre-service support), educated workforce, sustainable and well-funded services, good governance, strong networks, mainstreamed care, reduced inequalities
Data collected for this case study suggest that the SG funding for NHS Highland has led to positive outcomes for the GIC. Operating a service with a skeleton staff before the funds were allocated, the funding has enabled the GIC to create an MDT within the service, to bring endocrinology and psychology services in-house within NHS Highland, and to increase nursing time. The team was able to create a dedicated online chat service and offer ‘Near Me’ online video appointments to help mitigate challenges experienced by rural service users. The SG funding was also used to establish stronger third sector relationships, and has enabled the GIC to conduct psychological assessments (instead of referring patients to Sandyford for initial appointments) and endocrinology care (whereby it had previously outsourced this to NHS Grampian). Importantly, staff attribute greater visibility within the NHS Highland Health Board to the receipt of SG funding, which has enabled the creation of stronger governance structures around the clinic, and has fostered support from key teams across NHS Highland, including senior managers and clinicians who have advocated for the GIC. This has led to increased collaboration amongst NHS Highland teams across the patient care pathway, and has strengthened GIC succession planning.
These activities are aligned with the goals set out in the NHS Highland proposal for SG improvement funding, and the data suggest that the SG funding has had a positive impact on outcomes, including waiting times and patient care. Respondents to the survey and interviews expressed their appreciation of the comparatively shorter waiting times to access services at the clinic, the inclusive and accessible support offered by staff to patients, and the high quality of services offered by the GIC overall. Interviews with staff also suggest that the SG funding has had a positive impact on staff satisfaction and wellbeing, including the provision of staff training and development.
While NHS Highland has been able to effect positive changes in service delivery, they also still face certain obstacles that have hindered their ability to make all of their intended improvements to services. Staff interviewees raised concerns about challenges to recruit and retain staff (owing to fixed-term contracts and the general lack of specialists in gender dysphoria), the absence of a Shared Care Agreement with GPs, and the lack of overall education around gender identity amongst the mainstream NHS workforce - issues that are common to GICs across Scotland. Furthermore, service users felt that waiting times to access different treatments could be shorter, and more support could be offered (for instance, through NHS-run peer-support classes for people waiting for different treatments) to help forge social bonds amongst groups of patients going through similar experiences, and thereby to support their mental health.
These issues may be addressed by putting all preconditions in place for outcomes to be met, in particular with regard to training for staff and shared care. Furthermore, outcomes may be strengthened if leaders at the local (GIC), regional (Board) and national (SG/NHS Scotland) levels put in place a number of best practice learnings - which are elaborated on in full towards the end of this report - around continuous improvement, collaboration and partnerships, long-term core funding (to enable the creation of full-time and permanent posts that are attractive to candidates), clinical governance, staff training, and shared care with GPs. Interviews with GIC staff suggested staff shortages over the long-term would be aided by broader shifts in education and culture, such as including gender identity in the core curricula of university nursing, psychology and medical degrees, and fostering an information awareness raising campaign amongst the public to reduce fear and uncertainty about services. Meanwhile, interviewees were pleased that a new Transgender Care Knowledge and Skills Framework was being developed, which would provide learning opportunities for staff within clinics and across the NHS. These changes may further enable NHS Highland to strengthen positive service outcomes for patients and staff.