Quality prescribing for chronic pain: guide for improvement 2026-2029
Chronic pain, defined as persistent pain lasting beyond three months, can significantly impact quality of life, affecting physical and mental wellbeing. This guide supports clinicians and people living with chronic pain, using a person-centred approach to pain management.
5. Introduction
5.1 Scope of this guidance
This guide aims to provide a practical resource for practitioners helping people who live with Chronic Pain. Communication and non-pharmacological approaches are often central to achieving good results for patients, and these are explored in detail. Where medicines are used there should be an optimal balance between therapeutic effects and side effects of the medication, with an emphasis on non-pharmacological approaches.
5.2 What is chronic pain and why is it important?
Chronic pain, defined as persistent pain lasting beyond three months, [1] can significantly impact quality of life, affecting physical and mental wellbeing. In Scotland, the Scottish Health Survey (2022) indicates that approximately 38% of adults live with chronic pain. The prevalence of chronic pain is significantly higher in areas of socioeconomic deprivation.
There is a complex interplay between the social determinants of health and chronic pain, which require carefully considered management to achieve good outcomes. Medication reviews, focusing on what matters to the individual using a person-centred 7-Steps approach, are key to supporting people manage chronic pain and address the factors that influence their health.
With this guidance, we aim to support prescribers navigating the complexities of chronic pain management, particularly given the risks of adverse effects, dependency and the association with polypharmacy.
5.3 Methodology
This guide was developed by the collaborative efforts of a multidisciplinary team of clinicians, academics, experts by experience, patient groups and policy makers from across Scotland, from Scottish Government and NHS Scotland.
This document is intended to support good clinical practice and it is complementary to SIGN 173.
We have provided an indication on the strength of recommendations and guidance, which indicates the type of evidence that the recommendation is based on. The categories follow SIGN guidance terminology, categorising recommendations as strong, conditional or a good practice point.
- Strong: interventions that 'should/should not' be used for most people, based on evidence of high quality.
- Conditional: interventions that should be ‘considered', but the evidence is of low/mixed quality, or there is a risk of harm which should be balanced against the potential benefit.
- Good practice points: generally accepted practice, therefore it is unlikely that research would be conducted to confirm this. These good practice points are supported by the expert writing group.
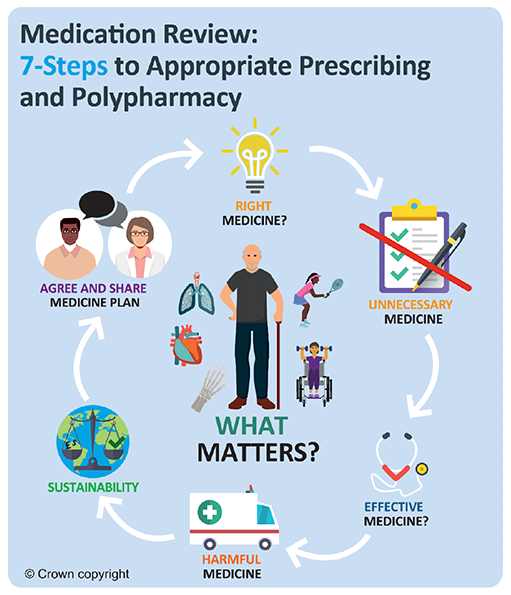
5.4 7-Steps Medication Review Process
The person-centred 7-Steps review process starts by matching therapeutic objectives to current life priorities with the individual. This is illustrated in Figure 1 below. This initial discussion guides decision-making in subsequent steps that consider medication need, effectiveness, and safety before a therapeutic plan and follow-up strategy are agreed upon.
Applying the 7-Steps as part of a holistic medication review has the potential to address all six dimensions of quality in health care: efficacy, safety, efficiency, timeliness, equity, and acceptability.[2] Although the 7-Steps approach was primarily designed to be applied at the point of medication review to correct inappropriate prescribing, its principles may equally be applied when initiating new medicines, to prevent inappropriate prescribing, or when a patient moves across transitions of care. This may result in reducing the dose or stopping a medication completely, although this should not be the primary objective of a medication review. Addressing unmet needs may include starting new medications.
The 7-Steps methodology has been developed to reflect a review focused on chronic pain.
5.5 7-Steps methodology
| Steps | Process | Person specific issues to address |
|---|---|---|
|
1. Aims What matters to the individual about their condition(s)? |
Review diagnoses and consider:
|
|
|
2. Need Identify essential drug therapy |
Identify essential drugs (not to be stopped without specialist advice)
|
|
|
3. Does the individual take unnecessary drug therapy? |
Identify and review the continued need for drugs
|
|
|
4. Effectiveness Are therapeutic objectives being achieved? |
Identify the need for adding/intensifying drug therapy to achieve therapeutic objectives
|
|
|
5. Safety Does the individual have or is at risk of ADR/ Side effects? Does the person know what to do if they’re ill? |
Identify individual safety risks by checking for
Identify adverse drug effects by checking for
|
|
|
6. Sustainability Is drug therapy cost-effective and environmentally sustainable? |
Identify unnecessarily costly drug therapy by
Consider the environmental impact of
Water pollution |
· Identify and review medicines of low/limited clinical value e.g. lidocaine plasters, nefopam |
|
7. Person- centredness Is the person willing and able to take drug therapy as intended? |
Does the person understand the outcomes of the review?
Ensure drug therapy changes are tailored to individual’s preferences. Consider
Agree and communicate plan
Ask person to complete the post-review PROMs questions after their review |
Agreed plan
|
5.6 Sustainability
NHS Scotland has set a target of becoming a net zero health service by 2040 and the plans for this are outlined in the NHS Scotland climate emergency and sustainability strategy: 2022-2026. This commitment was made in response to the recognition that climate change is currently the greatest global health threat of this century.
The professional leadership bodies in Scotland recognise the scale and the importance of the climate and ecological crisis, and the catastrophic effect on human health of not acting urgently and decisively. Therefore, in June 2022, the Royal College of General Practitioners Scotland published a joint statement with the Royal Pharmaceutical Society and the Scottish Academy of Medical Royal Colleges and Faculties to show commitment to reducing the environmental impact of prescribing and medicines.
Medication is by far the most common form of medical intervention for many acute and chronic conditions with around 280,000 items prescribed every day in Scotland. Approximately 25% of NHS carbon emissions is accounted for by the use of medicines and this can be reduced by:
- improving prescribing and medicine use, taking a value-based approach
- tackling medicines waste including medication reviews
- preventing ill health, and considering non-pharmacological approaches
- improving infrastructure and ways of working[3]
Approximately 10% of medicines are thought to be inappropriately prescribed and the Department of Health and Social Care’s National overprescribing review report outlines the importance of review, ensuring appropriate prescribing, to improve patient care, support the NHS, and reduce carbon emissions.[4] Research estimates between 30 to 50% of medications prescribed for long-term conditions are not taken as intended. [5] Medicine taken incorrectly, or not taken at all, is a potential risk to patients and leads to medicine wastage and contributes to the financial and carbon burden of the NHS.
It is therefore important that what matters to the person is taken into consideration, alongside a shared decision-making approach which takes into account their needs, preferences and values, to aid adherence. To ensure outcomes from medication are optimised, and prescribing is appropriate and safe, the 7-Steps medication review process provides a clear structure for both the initiation of new and the review of existing treatments and places an emphasis on ‘what matters to the individual’.
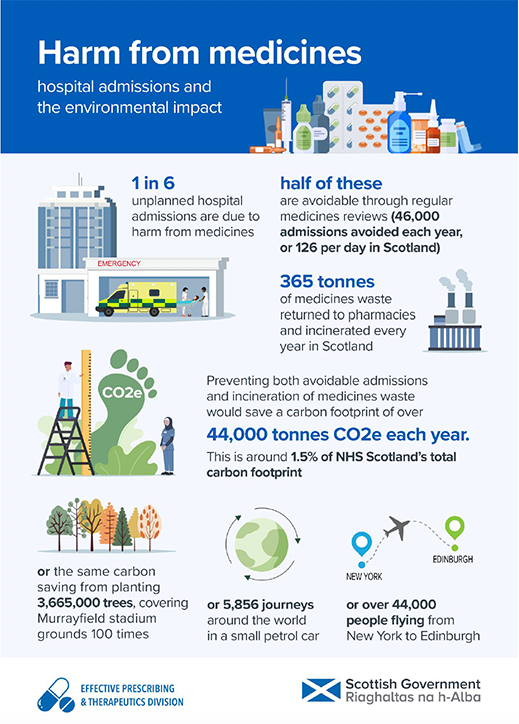
In Scotland every 10 days a 10-tonne truck of medicines waste (from community and hospital pharmacies) is transported for incineration. There are multiple associated costs with incineration of medicines waste including the transport costs, incineration costs, the environmental impacts and the direct costs of the unused medicines.
One in six unplanned hospital admissions are due to harm from medicines and half of these are preventable. Environmental impact from hospital admissions includes patient and visitor travel, medicines and use of goods and services whilst in hospital.5 (see Figure 2 below).
Ensuring appropriate prescribing and initiation of medicines and undertaking regular person-centred medication reviews can reduce waste and reduce harms associated with medicines use. This can benefit the individual by ensuring the effective use of medicines whilst reducing the NHS carbon footprint.
Reducing waste from medicines has a double carbon benefit by minimising:
- upstream emissions e.g. in distribution
- downstream emissions, with fewer medicines for disposal
Pharmaceuticals in waste water
The One Health Breakthrough Partnership highlights that medicines not only have a significant carbon footprint but can also lead to water pollution and loss of biodiversity. Every oral dose of a medicine is converted to a metabolite or excreted unchanged and 30-100% enters our wastewater system which cannot effectively remove all traces. The occurrence of pharmaceuticals in the environment is of global concern and the extent of their risks and impacts on human health and biota is growing. There is already evidence that they can affect aquatic wildlife, increase microbial resistance and enter the human food chain.
Pharmaceutical residues have been found in the environment as a result of production and formulation, patient use, use in agriculture and food production, and from improper disposal of medicines. Everyone should be encouraged to avoid flushing medication down the toilet or drain, and to return medicines to community pharmacies for safe disposal.
NHS health boards are responsible for providing a service whereby patients can return unwanted and out of date medicines to community pharmacies. Through local contractual arrangements, funded by the local board, pharmacy contractors are required to accept returned waste medicine from patients. Each pharmacy is allocated a specific number of waste bins and receives regular uplifts of these bins. Once collected, the health board is responsible for ensuring its disposal by incineration.
This guidance supports reducing inappropriate prescribing by recommending:
- person-centred decision-making
- providing guidance and support
- more alternatives to medicines, such as physical and social activities and lifestyle change
- regular 7-Steps medication review
Contact
Email: EPandT@gov.scot