Quality prescribing for chronic pain: guide for improvement 2026-2029
Chronic pain, defined as persistent pain lasting beyond three months, can significantly impact quality of life, affecting physical and mental wellbeing. This guide supports clinicians and people living with chronic pain, using a person-centred approach to pain management.
6. Chronic Pain in Society
6.1 Understanding chronic pain
6.1.1 Prevalence and distribution of chronic pain
38% of adults reported chronic pain (pain that persisted for more than three months), in the Scottish Health Survey (2022). Chronic pain is more common in women, and with increasing age. It is associated with social deprivation, and with a history of adverse childhood experiences, among other factors.[6]
Chronic pain rarely occurs in isolation: 75% of people with chronic pain experienced at least one other long-term condition, and those with pain at three or more sites had an average of three other co-morbidities. These commonly include mental health disorders, heart disease and/or respiratory disease. Chronic pain can affect anyone, of any age, from any background, with or without other apparent ill health.
6.1.2 Definitions of chronic pain
Everyone experiences pain, and can describe it intuitively, but may find it challenging to define. Pain is defined by the International Association for the Study of Pain (IASP) as “an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage.”
Pain
Based on IASP:
- Pain is always a personal experience that is influenced to varying degrees by biological, psychological and social factors.
- Pain and nociception are different phenomena. Pain cannot be inferred solely from activity in sensory neurons.
- Through their life experiences, individuals learn the concept of pain.
- A person’s report of an experience as pain should be respected.
- Although pain usually serves an adaptive role, it may have adverse effects on function and social and psychological well-being.
- Verbal description is only one of several behaviours to express pain; inability to communicate does not negate the possibility that a human experiences pain.
Chronic Pain
Chronic pain is defined by the Word Health Organization (WHO) as “pain that persists or recurs beyond three months”, this period being taken to represent ‘normal tissue healing time’.1
Chronic pain is further categorised into:
- chronic primary pain
- chronic pain in one or more anatomical regions that is characterised by significant emotional distress or functional disability, and that cannot be explained by another chronic condition. Examples include fibromyalgia, complex regional pain syndrome, non-specific low-back pain
- chronic secondary pain
- cancer-related
- post-surgical or post-traumatic
- musculoskeletal
- visceral
- neuropathic
- headache or orofacial pain
Assessment and treatment must always be person-centred and appropriate to the relevant clinical situations, though there are many commonalities between these groups.
An alternative, mechanistic, categorisation of pain that directly determines prescribing decisions is:[7]
1. Nociceptive pain: Pain arising from actual or threatened damage to non-neural tissue, and caused by activation of nociceptors
- Pain from physical damage or potential damage to the body
2. Neuropathic pain: Pain arising as a direct consequence of a lesion or disease affecting the somatosensory system
- Pain when an injury or medical condition damages the nervous system or prevents it from working properly
3. Nociplastic pain: Pain arising from altered nociception despite no clear evidence of actual or threatened tissue damage causing the activation of peripheral nociceptors or evidence for disease or lesion of the somatosensory system causing the pain
- Pain that arises from altered sensation in the absence of damage to tissue or the nervous system
Note that an individual may experience two or more different types of pain, no matter how they are categorised.
6.1.3 Acute and chronic pain
Acute pain is generally present to provide a warning of danger, or notification of injury. It prompts us to take evasive or curative action and is therefore healthy and lifesaving. In contrast, the definition of chronic pain implies that, as pain has persisted beyond tissue healing time, it is a pathological condition, providing no useful purpose.
However, longer-term pain may be providing longer-term protection, prompting more gradual, sustained rehabilitation. Long-term pain is often associated with long-term tissue damage, as is the case with osteoarthritis.
Characteristics of chronic pain may arise before the three-month period has passed. Complex Regional Pain Syndrome, for example, has its onset soon after (often relatively minor) injury and is characterised by a heightened overall response to the pain.
Recent studies have shown that how individuals respond to acute pain is important in determining the longer-term experience. This response is influenced by:
- genetics
- other biological factors
- psychological factors, including previous experience of pain, stress, and childhood adversity6
The way in which acute pain is managed can have an important effect on long-term outcomes. This is clear, for example, in peri-operative care, where good, multi-modal post-operative analgesia is associated with reduced risk of chronic post-surgical pain and analgesia use. The British Pain Society state: “The principle of multimodal analgesia is that improved pain relief can be achieved by combining analgesics with different mechanisms of action that work synergistically” and “Multimodal analgesia also includes non-pharmacological elements, which may be low risk, have potential analgesic benefits and may reduce both the necessary dose and possible adverse effects of drugs used.” [8] The postsurgical model is an important one to consider for the transition from acute to chronic pain.
In the peri-operative period, several factors are important when providing high-quality and effective pain relief and preventing long-term pain and analgesia use:
- Clear expectations, before surgery, of the likely extent and duration of pain can lead to healthier experiences and responses to post-operative pain
- Long-term analgesic use after surgery is influenced by the pattern of use during hospital care
- Clear expectations, after surgery, regarding the likely need, duration, and strength of analgesia will set realistic expectations for the individual after discharge from hospital
- Carefully-managed reduction and cessation of analgesic prescribing after discharge from hospital will reduce long-term use
- Placing an emphasis on functional recovery, which is facilitated by analgesia, will reduce the expected need for analgesics, and optimise quality of life
Good peri-operative pain relief in hospital is facilitated by appropriate staffing who understand the factors and are person-centred; a dedicated Pain Team is an effective way to address this need. A high-quality approach to planning, implementation and review of peri-operative analgesia supports good analgesic management. This facilitates good use of multimodal analgesia, including regional techniques where they are clinically indicated.
Effective and timely communication is key to successful pain management following discharge from hospital. This supports prompt, effective and equitable practice. Plans and expectations for analgesic management should be made clear and effectively communicated to both the individual and their GP. This may be facilitated by electronic prescribing systems which allow the expected duration of treatment to be described e.g. hospital electronic prescribing and medicines administration (HEPMA) bundles. Once a person has been discharged, ongoing communication between them and their care team can help optimise their recovery and guide further support as required.
6.1.4 Causes of chronic pain
Chronic pain can arise through many causes. These include:
- back pain (most common)
- arthritis, and other musculoskeletal diagnoses
- post-surgical pain
- diabetic neuropathic pain
- headaches
- fibromyalgia
- visceral pain (for example from endometriosis)
In many cases no definitive diagnosis can be reached.
6.1.5 Impact of chronic pain
The impact of chronic pain is extensive at the individual level, influencing all aspects of life and health.[9] This includes:
- physical and mental health
- the ability to work
- undertaking activities of daily living
- reduced physical activity
- negative effects on self-confidence, social functioning and self-identity
The relationship is often bi-directional - for example chronic pain can lead to depression, which heightens the experience of chronic pain.
There is also adverse impact on people's families, their work, the health services, and on society. In the United Kingdom it was estimated that primary care management of chronic pain accounted for 4.6 million general practice appointments per year, equivalent to 793 whole time general practitioners.
6.1.6 Goals of managing chronic pain
The medical model of treating pain – now considered insufficient in chronic pain – required diagnosis of the underlying cause and identification of the appropriate medicines to effect pain relief. The WHO Analgesic ladder was devised for treatment of cancer pain, and although widely used, was never validated in other types of pain. At the outset of treatment it is important that individuals with chronic pain and healthcare professionals recognise that complete relief of chronic non-cancer pain is often unrealistic. This issue led to the NHS campaign in England, Painkillers Don’t Exist. Even when effective analgesia can be achieved, more recent evidence suggests that it is not always the best thing – for example, anti-inflammatory medicines might actually cause chronic back pain by reducing the natural inflammatory/immune response in the acute phase. Breakthrough pain is associated with cancer, life-limiting conditions and end-of-life where background pain exists, and acute episodes of more severe pain may be experienced. In non-malignant chronic pain, the concept of breakthrough pain is poorly understood and it may not be a helpful concept to use.
A person-centred approach to pain management considers the biopsychosocial approach. This considers the person experiencing pain in the context of:
- their background (family, culture, occupation, financial circumstances, etc)
- their beliefs about pain and health
- fears
- expectations
- previous experiences of pain
- causes and its treatment
- other aspects of their physical and mental health
The goals of assessment and management are to understand the impact of pain on the person's life and for them to live as well as possible with the pain, balancing the potential harms of treatment with the potential benefits.
This requires multi-dimensional assessment, multi-disciplinary treatment approaches, and working in collaboration with the person in pain.
Identifying the clinical and social demographic factors associated with chronic pain may provide opportunities for prevention or early identification of risk with a view to minimising overall impact. This may offer limited help for individual patients, but could inform priorities in wider society, such as promoting reduction in health inequality.
6.1.7 Potential harms associated with pain treatments
As with any medicine, adverse effects of analgesics exist, and can outweigh benefits. Opioids are associated with a long list of potentially serious adverse effects that often limit their use. These include drowsiness, constipation, nausea, respiratory depression, immune dysfunction, dependency and sexual dysfunction, among many others. Both tolerance and the paradoxical phenomenon of opioid induced hyperalgesia can lead to escalating doses and harms while also actually making pain worse.
Opioids are associated with problematic substance use, dependency, and death, with opioid-related deaths in Scotland rising fourfold between 2000 and 2020. Prescribing rates of opioids are falling in Scotland (since publication of the SIGN Guideline, Management of Chronic Pain in 2013) and Scottish Government Quality Prescribing Guide for Chronic Pain 2018). However, this is gradual. Opioids remain an important cause of morbidity and mortality.
Gabapentinoids (gabapentin and pregabalin), indicated for treatment of neuropathic pain, were initially considered relatively safe. However, side effects are increasingly being recognised, including drowsiness or somnolence, dizziness, nausea, weight changes (abnormal appetite), cognition speech problems, ataxia and respiratory depression. These frequently limit their tolerability.
Pregabalin can impact foetal development, and similar considerations may apply to gabapentin. Advice for health professionals can be found in the MHRA Pregabalin Drug Safety Update.
These medicines can be misused and are increasingly associated with drug-related deaths in Scotland.[10] Gabapentinoids are associated with serious long-term harms (including overdose and major trauma).[11]
Adverse effects of analgesics can be exacerbated by:
- polypharmacy (especially with opiates, other analgesics and/or sedatives)
- alcohol use
- smoking
- problematic substance use
- mental health conditions
There are additional risks arising through the use of non-prescribed analgesia, for example taking medicines that are prescribed for others, or sharing between family and friends or obtaining illicit drugs. In these cases, there is no opportunity to assess risks and therefore the likelihood of harm is greater.
All healthcare professionals should consider the risks of any prescribing, before prescribing decisions are made, in partnership with the individual. Any decisions need to be supported by early and ongoing review. The benefits and limitations of treating chronic pain with medication is discussed in more detail in chapter nine.
6.2 Health inequalities in chronic pain
6.2.1 Addressing Health Inequalities
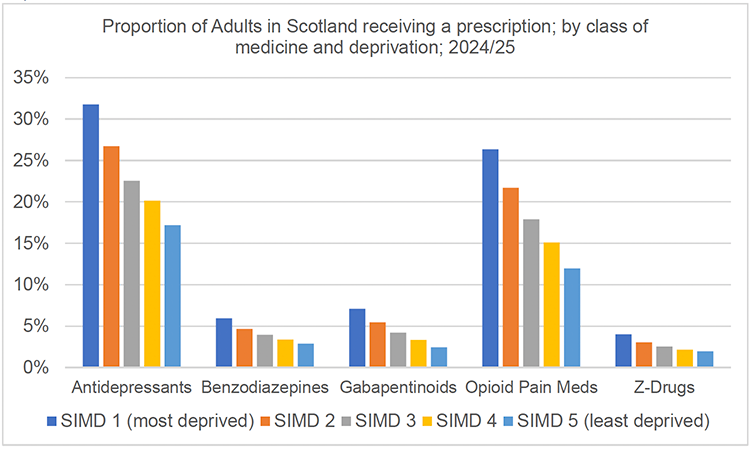
Chronic pain occurs more often among socially, economically and historically marginalised groups.[12],[13] Chronic pain prevalence in adults ranges from 50% in the most deprived Scottish Index of Multiple Deprivation (SIMD) areas to 29% in the least deprived areas.[14] Prescribing data for medications commonly used for pain shows higher levels in areas of deprivation, as demonstrated in Chart 1 below.
While the main drivers of health inequalities lie outwith healthcare, our services and the way they are delivered play important roles. In this small section we raise awareness of health and healthcare inequalities and connect to emerging evidence on effective ways of mitigating inequalities in healthcare. This section is supported by Appendix A where fuller explanations and literature citations are given, including the intersectional nature of health inequalities i.e. that health inequalities can be more fully understood by exploring factors beyond only socioeconomic deprivation.
Scotland has high levels of health inequalities,[15] with poorer areas experiencing worsening health. Health inequalities are ‘unjust and avoidable differences in people’s health across the population and between specific population groups’.[16] There are many possible reasons why chronic pain is experienced inequitably including:
- the complex nature of chronic pain
- the understanding of chronic pain as a defined diagnosis
- the subjective and invisible nature of pain
- the relationship that pain has with distress, trauma and mental health conditions
6.2.2 Actions on Health inequalities
In the context of undertaking medication reviews, approaches to care can be adopted to account for some of the factors that maintain inequalities. If any service improvement approaches are being undertaken, accounting for equitable care should be considered, and Appendix A contains further details of supporting literature and resources to help.
Approaches to consider in delivering care include:
- Raising healthcare professional (HCP) education and awareness of health inequalities, driving factors, impacts on individuals and the limitations of tackling inequalities solely through healthcare
- Consideration of additional support that might be needed to reduce barriers at service interfaces e.g. support mechanisms to help attendance at specialist appointments or care coordinators
- Continuity, building relationships and trust in delivery of care is helpful in particular for marginalised groups. Service design aspects to consider: continuity in timetabling, personal lists and longer consultations
- Improving healthcare professionals’ understanding of power imbalance – understanding that different groups may hold different levels of power that influences consultations, and can inhibit people asking questions that matter, leading to over-medicalisation
- Health literacy involves a functional understanding of any health condition. It supports the ability and opportunity to implement management and to navigate health systems. To promote health literacy within healthcare, use verbal communication strategies, accessible information, easy-to-navigate services and flexible care
- Trauma-informed approaches to health service provision are typically service-wide with connections to trauma treatment options. In consultations it is important to give space to develop trust and for people to tell their stories; fostering individual choice and control, and being sensitive and aware of cultural, historical and gender-related issues
- Welfare and financial inclusion – HCPs can routinely enquire about money worries and signpost patients to welfare resources e.g. Citizen’s Advice Bureau
Contact
Email: EPandT@gov.scot