Family Nurse Partnership: 10 year analysis
To mark the first ten years of the Family Nurse Partnership in Scotland, we have undertaken a review of data from the programme over this time.
Section 3: Maternal Outcomes
This section uses data about clients who completed the programme (graduates) only, unless stated otherwise. Data for those that left prior to completion is excluded as the data is incomplete. Data is collected at various points in the FNP journey and is collated across all graduates from the programme's inception to the 31st March 2021. This analysis does not include the data from the pilot of FNP.
Summary – Maternal Outcomes
- More than half (54%) of FNP graduates smoked at some point during pregnancy (including before they knew they were pregnant). This decreased to a third (32%) two weeks after enrolment and a slightly lower proportion again (28%) by 36 weeks gestation.
- At 12 months post-birth, over a third (37%) of FNP clients reported that they currently smoked cigarettes. A higher proportion of clients living in the most deprived areas (40%) smoked at 12 months post-birth, compared to 26% in the least deprived areas
- In recent years the majority of FNP clients had not consumed alcohol (68%) or taken drugs (94%) during pregnancy[xiii], including before they knew they were pregnant.
- Of clients who were sexually active, 90% reported using birth control at 6 months post-birth. However this decreased at 24 months post-birth (79%)
- Almost a third (31%) of FNP clients reported experiencing a second pregnancy by 24 months post-birth of their first child. Overall, 13% of FNP clients had a live birth within 24 months of the birth of their first child.
- The proportion of FNP graduates in education post-birth increased from 9% in full-time education 6 months post-birth to 14% in full time education 24 months post-birth. This varied with age, with the youngest clients more likely to be in education than those over 20 years.
- Overall, over one in ten (12%) clients who graduated from FNP were in paid employment at 6 months post-birth, however this increased to one in four clients (25%) by 12 months post-birth and almost a third (30%) of clients by 24 months post-birth. Those aged 20 years and older at enrolment were more likely to be in paid employment than younger clients.
- FNP clients in work and/or education post-birth increased across all age groups, SIMD quintiles and regions from one fifth (20%) at 6 months post birth to two fifths (40%) at 24 months post birth.
- The majority of FNP clients lived in local authority or housing association housing, and the proportion living in this type of accommodation increased slightly from 60% at 6 months post-birth to 65% at 24 months post-birth.
- At each stage post-birth, around 40% of clients were single, 30% were living with their partner and/or married or in a civil partnership, and 30% were in a relationship but not living with their partner.
Young mothers represent one group that are at particular risk of engaging in health behaviours that can lead to poorer health outcomes. There is a strong association between teenage pregnancy and social deprivation[41], meaning that younger mothers may struggle financially, live in poorer housing and have lower educational attainment [42,43]. Behaviours like smoking and physical inactivity often begin in youth and are closely aligned with social deprivation[44], and young mothers may leave school early or move away from the parental home, leaving them at risk of isolation due to inadequate social support[45].
The evidence also indicates that younger mothers tend to have poorer perinatal health outcomes (later engagement with services, lower birth weights, less likely to breastfeed, higher infant mortality and higher rates of postnatal depression)[46]. Further to this, mothers aged under 20 are at a 33% increased risk of stillbirth and a 75% increased risk of neonatal death compared to mothers aged 30-34[47].
Alongside this, young mothers are also more likely to experience poorer mental health and are at a higher risk of mental health issues, such as postpartum depression, in the first three years after giving birth than older mothers. Postpartum depression can have long-term consequences for both the mother and child[48].
FNP has been implemented in many countries in the 45 years since its inception. There have been demonstrable programme effects on a range of child and maternal outcomes. However, FNP is not delivered in the same context to the same clients in every country, although the target client group overall usually comprises of first time mothers with an idetified need. Furthermore, the context within which the programme is delivered can have a bearing on the outcomes achieved. In particular the health care setting in which the programme is delivered is a key consideration in the intepreatation of outcomes achieved by FNP in the country context.
The Early Intervention Foundation's Guidebook[49] provides a summary of the evidence base for the Family Nurse Partnership programme and has provided an established evidence rating (Level 4+) of improving a variety of child and parent outcomes, including attachment security in the short term, children's early language development and reduced risk of preventable death in early adulthood.
In the five randomised control trials (RCTs) conducted to date in countries that have implemented FNP, the following maternal outcomes have been show to be affected by FNP in two or more trials[50]:
- Reduced smoking (at childbirth) (Elmira, Denver and Dutch Trials)
- Increased attempted breastfeeding (between childbirth and child age two) (Memphis and Dutch Trials)
- Improved home environment (child age two) (Memphis and Dutch Trials)
- Improved self-efficacy (child age two) (Memphis and English Trials)
- Reduced domestic violence (child age 2-6) (Memphis and Dutch Trials)
Smoking, Drug and Alcohol Use
Smoking in Pregnancy
Tobacco smoking is associated with adverse pregnancy outcomes because smoking during pregnancy harms both the mother and her baby. Prenatal smoking is thought to account for an estimated 20 to 30 percent of cases of low birth weight (<2500g), and also increases the risk of shortened gestation, respiratory distress syndrome, and sudden infant death syndrome. Babies born with lower-than-average birth weight are more likely to get infections and have other health problems. Even after controlling for alcohol use, socioeconomic status, maternal height, maternal weight and years of education, smoking has been implicated in long term effects such as poor cognitive performance on achievement tests and decreased physical growth.[51]
Over the past two decades, smoking among pregnant women has declined by about 60–75% in high-income countries[52]. In Scotland in 2000, approximately 29% mothers smoked while pregnant. By 2021 this figure had dropped to 13%[53]. However, generally Scotland reports higher rates of smoking during pregnancy than many other European countries[54].
In Scotland overall, the proportion of women recorded as current smokers at the time of their booking appointment has steadily decreased since 1997/98, falling from 30.7% of those with a known smoking status to 13.1% in 2020/21. In 2020/21 a further 14% were former smokers at the time of their booking appointment, whilst 72.9% had never smoked. However, smoking rates are not equitable accross all age ranges and deprivation quintiles. Nationally, in 2020/21 almost a quarter (24%) of mothers in the most deprived areas (SIMD 1) were smokers at the time of their antenatal booking, which is more than double the rate of all mothers in Scotland (13%). Women aged under 25 years were approximately three and a half times more likely to be a current smoker at booking than women aged 35 and over[55].
There are many factors associated with smoking during pregnancy such as socioeconomic status (low educational attainment and deprivation), white ethnicity, higher level of nicotine dependence, lack of social support, having a partner who smokes or other smokers in the home, using alcohol during pregnancy, culture, high levels of stress, and mental health conditions including depression and past-year psychiatric symptoms[56,57].
Overall, more than half (54%) of FNP graduates had smoked at some point during pregnancy (including before they knew they were pregnant). This decreased to around one in three clients (32%) being a current smoker 2 weeks after enrolment onto the programme and a slightly lower proportion (28%) by 36 weeks gestation.
When compared to the findings in the Building Blocks trial[58] about FNP in England (which combined data from self reported smoking and urine analysis) the findings showed that 55.6% of FNP clients were smokers in late pregnancy and 51.6% of the control arm were smokers in late pregancy (about 34 to 36 weeks gestation).
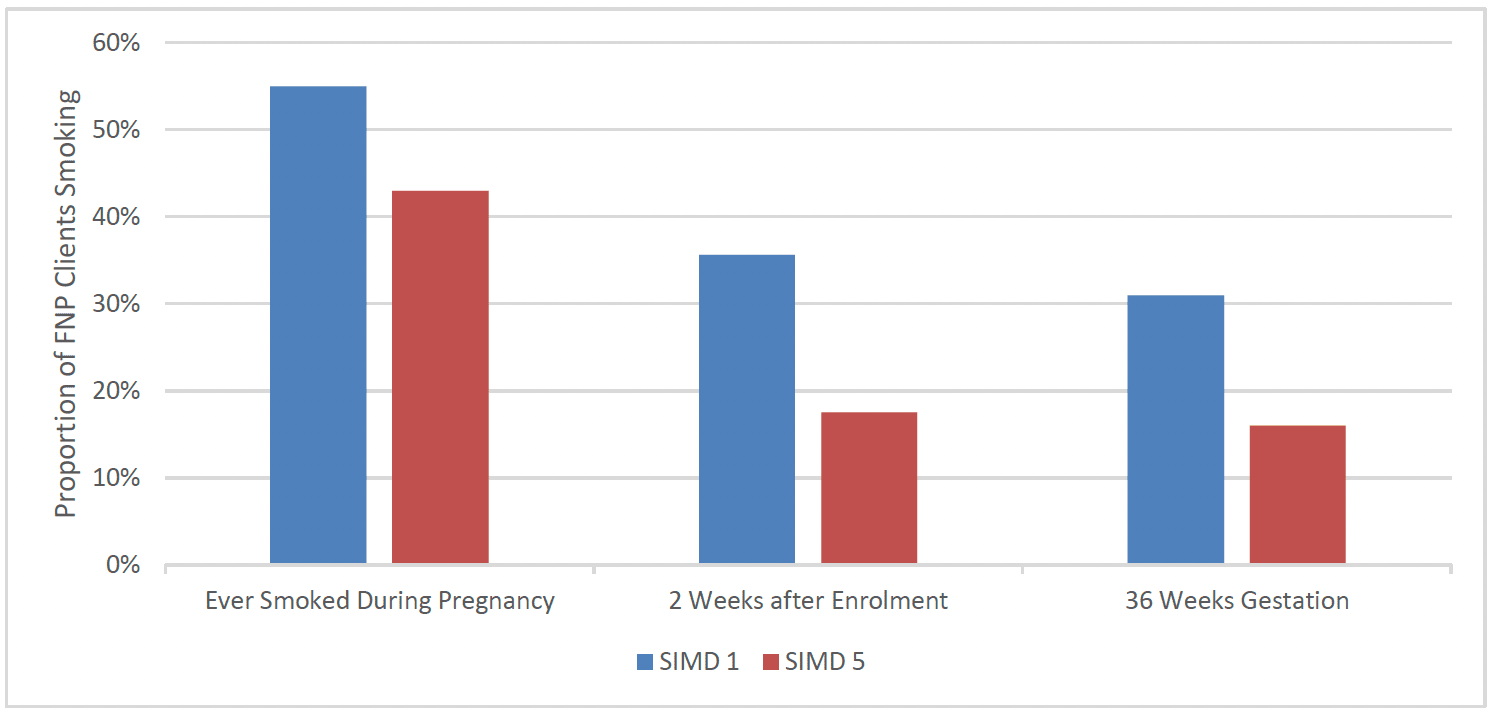
There was evidence of differences by social deprivation, although this was not as marked as that seen in the general population, with over half 55% of clients in the most deprived areas reporting having ever smoked during pregnancy, compared to 43% of clients in the least deprived areas. This gap widened at subsequent stages of pregnancy, with clients in the most deprived areas almost twice as likely (31%) to smoke at 36 weeks gestation, as clients in the least deprived areas (16%) (Chart 17).
Clients who spoke English as their primary language were more likely to smoke at each time-point than those who did not. Over half (55%) of clients who spoke English as their primary language reported having smoked at all during pregnancy, compared to 43% of clients who spoke a primary language other than English, with a similar reduction in smoking between the two groups at subsequent time-points.
There was a similar proportion of clients in each age group smoking at each timepoint.
Smoking was slightly less prevalent at each time-point in the West of Scotland, with 50% reporting having ever smoked during pregnancy, 28% at 2 weeks after enrolment and 24% at 36 weeks gestation, compared to 54%, 32% and 28% at these respective time-points among all FNP clients.
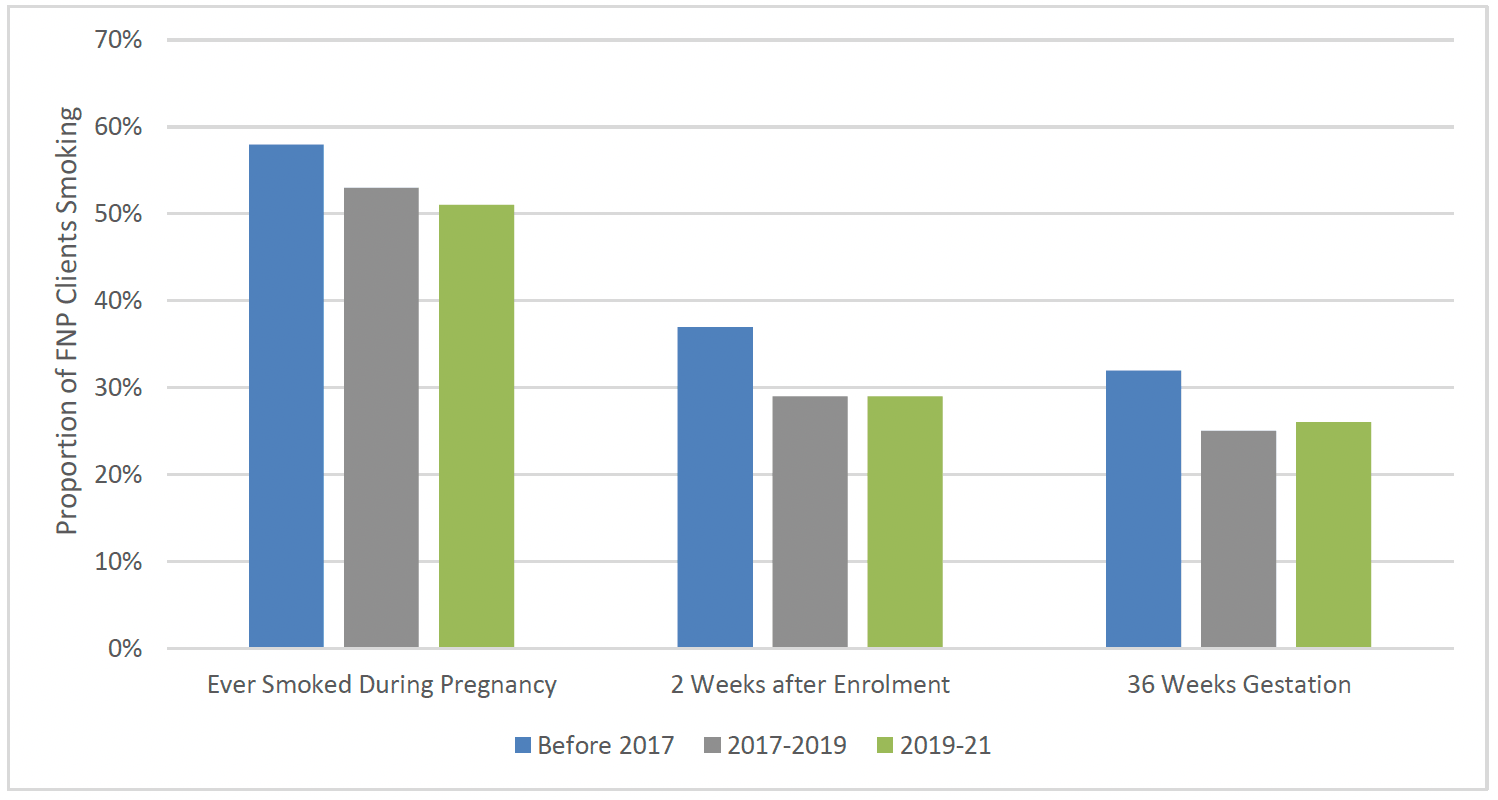
Smoking was also slightly less prevalent for clients entering FNP in more recent years, in line with decreases in smoking more generally. For clients who went on to graduate between 2019-21, 51% reported having ever smoked during pregnancy, 29% at 2 weeks after enrolment and 26% at 36 weeks gestation. For clients who graduated prior to 2017, 58% reported having ever smoked during pregnancy, 37% at 2 weeks after enrolment and 32% at 36 weeks gestation (Chart 18).
Postnatal Smoking
Studies have shown that while high proportions of mothers stop or abstain from smoking during pregnancy, a high proportion relapse from 6 to 12 months postpartum. A study in the US in 2016 showed 58% of those that had stopped smoking begin to smoke again postnatally[59,60].
The evidence shows that having a supportive partner is particularly important in stopping smoking during pregnancy[61]. Pregnant women with partners who are active smokers find it harder to quit and are more likely to relapse, especially during the postnatal period[62]. Themes central to smoking cessation in pregnancy at an individual level were perception of risk to baby, self-efficacy, influence of close relationships and smoking as a way of coping with stress. At an interpersonal level, partners' emotional and practical support, willingness to change smoking behaviour and role of smoking within relationships were important[63].
At 12 months post-birth, over a third (37%) of FNP clients reported that they currently smoked cigarettes (Chart 19). A slightly higher proportion of clients aged 17 and under at intake (41%) smoked at 12 months after birth, compared to 35% aged 18-19 and 37% aged 20 and over.
Smoking rates at 12 months post-birth were also higher amongst clients who spoke English as a primary language at intake (38%) when compared to those who did not (31%).
As with smoking during pregnancy, a higher proportion of clients living in the most deprived areas (SIMD 1) (40%) smoked at 12 months post-birth, compared to 26% in the least deprived areas (SIMD 5). Smoking rates at 12 months post-birth were also higher in the East of Scotland (41%), compared to the North (37%) and West (34%) of Scotland. As with smoking during pregnancy, there appeared to be a reduction in the proportion of FNP clients smoking 12 months post-birth over time. Just over one in four (42%) of the group graduating before 31 March 2017 smoked, compared to 34% graduating between 2017-2019 and 35% of those graduating between 2019-21.
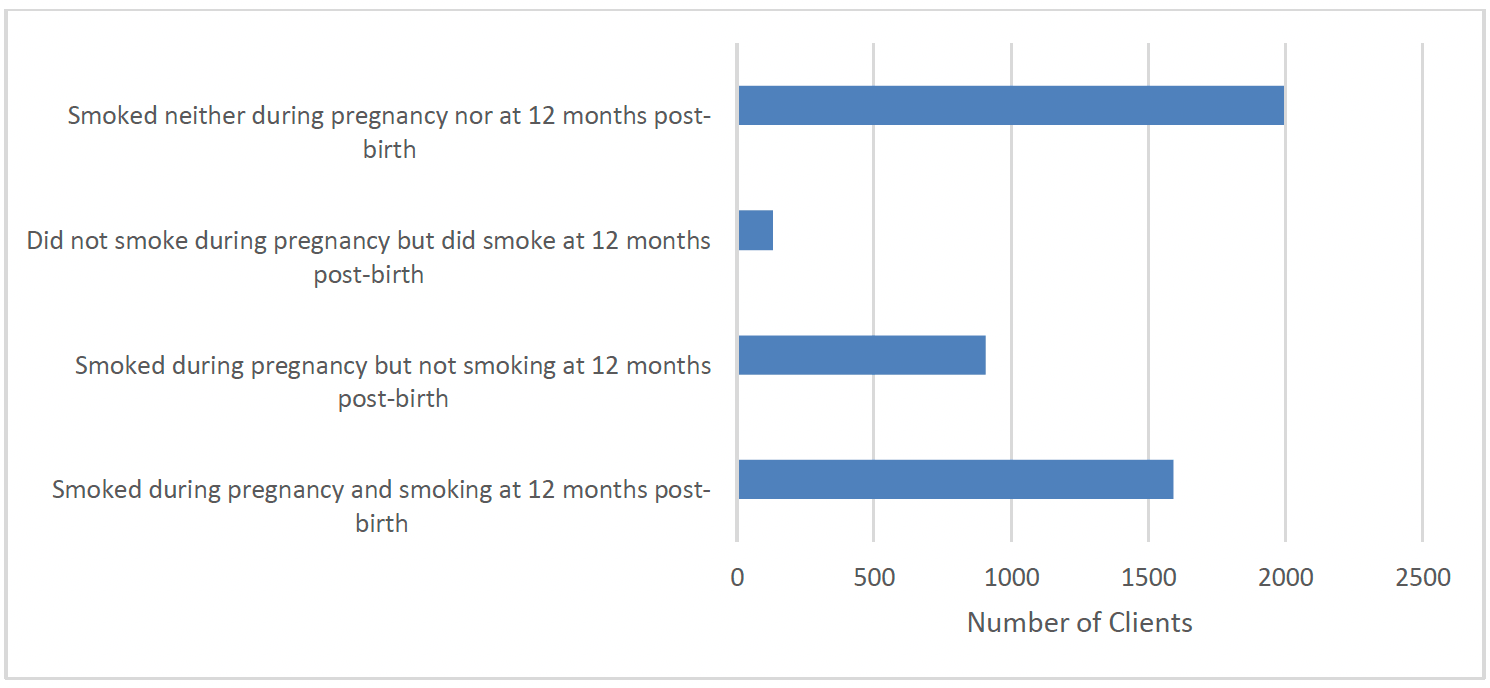
Of clients who reported having smoked at any time during pregnancy, the majority (64%) smoked at 12 months post-birth, while one in three (36%) had ceased smoking. The vast majority (94%) of clients who did not report smoking at all during pregnancy also did not smoke at 12 months post-birth.
Alcohol Use
The health risks of drinking alcohol while pregnant are well documented. Drinking in pregnancy can increase the chances of miscarriage, pre-term birth and low birthweight, and may lead to life-long harm to the foetus. Higher levels of drinking increase risks[64,65]. A baby's brain and body develop during the entire pregnancy. Alcohol can affect this development and result in a number of lifelong physical, emotional and developmental difficulties including fetal alcohol spectrum disorder (FASD)[66]. The UK Chief Medical Officers guidelines[67] state that pregnant women or those who think they could become pregnant should not consume any alcohol immediately prior to or during pregnancy.
Within the Scottish maternal and infant nutrition survey in 2017[68] younger respondents were more likely than older respondents to report avoiding alcohol or drinking infrequently before they became pregnant. Nearly two-thirds (64%) of respondents aged 19 and under[xiv] reported that they never drank alcohol compared to less than half of those over 35 years (45%).
The Growing Up in Scotland study[69] found that mothers living in the most advantaged circumstances were more likely to say they consumed alcohol during pregnancy[xv]. In birth cohort 2 of Growing Up in Scotland, 34% of those in the highest income quintile consumed alcohol while they were pregnant, compared with 11% of mothers in the lowest income quintile. These findings were also found when children were 10 months: main carers in the highest income quintile were more likely to drink alcohol than those in the lowest income quintile. However, parents in the lowest income quintile were over twice as likely to drink five or more units on a typical drinking day compared with those in the highest income quintile (45% compared with 20% respectively), indicating more alcohol being consumed per drinking day among those in the most deprived groups.
Data on alcohol use in the Turas FNP system was limited to clients enrolling onto the programme in the most recent years (2019 onwards), so limited analysis is available.
Where there was data available, clients were asked at 2 weeks after enrolment onto FNP whether they had consumed alcohol at any time during their pregnancy, including before they knew they were pregnant. Of the 1750 clients for whom this data was collected, the majority had not consumed alcohol during pregnancy (68%), while 567 clients (32%) reported having consumed some alcohol. However, clients were also asked at this time-point how many units of alcohol they had consumed in the prior 7 days and almost all (99%) reported having not consumed alcohol, with just 13 clients reporting that they had consumed alcohol in the last 7 days. This was also the case when clients were asked the same question at 36 weeks gestation – only 11 clients reported having consumed alcohol in the last 7 days when asked at this time-point.
Clients were also asked, 2 weeks after enrolment, how many units they had drunk the last time they were at a night out or party (including before their pregnancy). Of the 1660 clients for whom valid data was collected for this question, 572 clients (34%) stated that they had not drunk alcohol, 475 clients (29%) stated that they had consumed 6 units or less, 265 clients (16%) stated that they had consumed 7 to 10 units, 263 clients (16%) had consumed 11 to 20 units, and a small group of clients (85 clients, 5%) had consumed more than 20 units.
Drug Use
In 2019/20, drug use was recorded in 1.6% (769) of 47,767 maternities[xvi] in Scotland[70]. Where maternal drug use was recorded, the drugs most often used during pregnancy were cannabis, cocaine and opiates . The rate of maternities with drug use recorded was highest in the under 20 age group (52.0 per 1,000 maternities).
In 2019/20, the rate of maternities where drug use was recorded was over five times higher in the most deprived neighbourhoods in Scotland than in the least deprived neighbourhoods[71],[xvii].
Data on drug use amongst the FNP data system clients was limited to clients enrolling onto the programme in the most recent years (2019 onwards) due to issues with data migration from previous FNP systems.
Clients were asked at 2 weeks after enrolment onto FNP whether they had taken any drugs in the previous month. Of the 1750 clients for whom this data was collected, the majority had not used drugs in the previous month (94%), while 111 clients (6%) reported having used drugs in the previous month. The most common drugs used were cannabis (96 clients) and cocaine (15 clients).
Clients were also asked at 36 weeks gestation whether they had taken any drugs in the previous month. Of the 1511 clients for whom this data was collected, 96 clients (6%) reported having used drugs in the previous month. Again, the most common drugs used were cannabis (80 clients) and cocaine (13 clients).
Birth Control, Subsequent Pregnancies and Births
Birth Control
In Scotland, young people under the age of 25 experience the greatest burden of sexually transmitted infections (STIs), and young women aged 20-24 years experience the highest rate of abortion care, suggesting unplanned conception. Research has shown that for adolescents, use of a long-acting reversible contraceptive (LARC) method (intra-uterine device (IUD) or contraceptive implant) is associated with better spacing of pregnancies.[72]
Condoms are still the most commonly used form of protection against STIs and unintended pregnancies by young people in Scotland. Over the last five years, however, there have been strong indications that fewer young people than before are accessing free condom services, or LARC[73].
The prescribing rate for new insertions of a LARC (an implant, IUD, intra-uterine system (IUS), or contraceptive injection) has been significantly impacted by the COVID-19 pandemic across all NHS board areas, decreasing from 54.3 per 1,000 women in 2019/20 to 32.1 per 1,000 women in 2020/21[74].
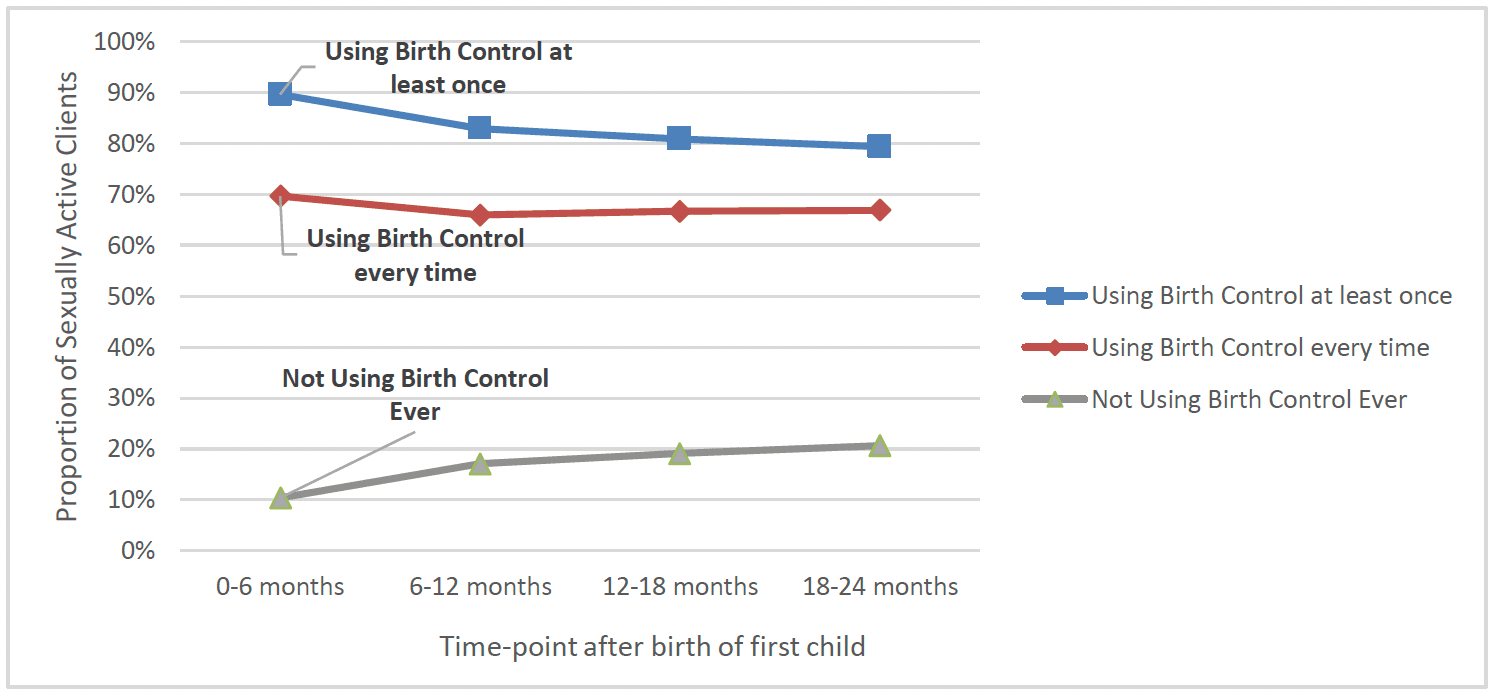
FNP clients were asked about their use of birth control over the previous six months and at six month intervals after birth. Of clients who were sexually active, 90% reported using birth control at 6 months post-birth. However, this decreased at 24 months post-birth (79%). Overall, the proportion using birth control every time they had sex remained relatively stable at around two thirds of clients (Chart 20). Birth control use at each time-point was broadly similar across demographic groups, geographically, and over time.
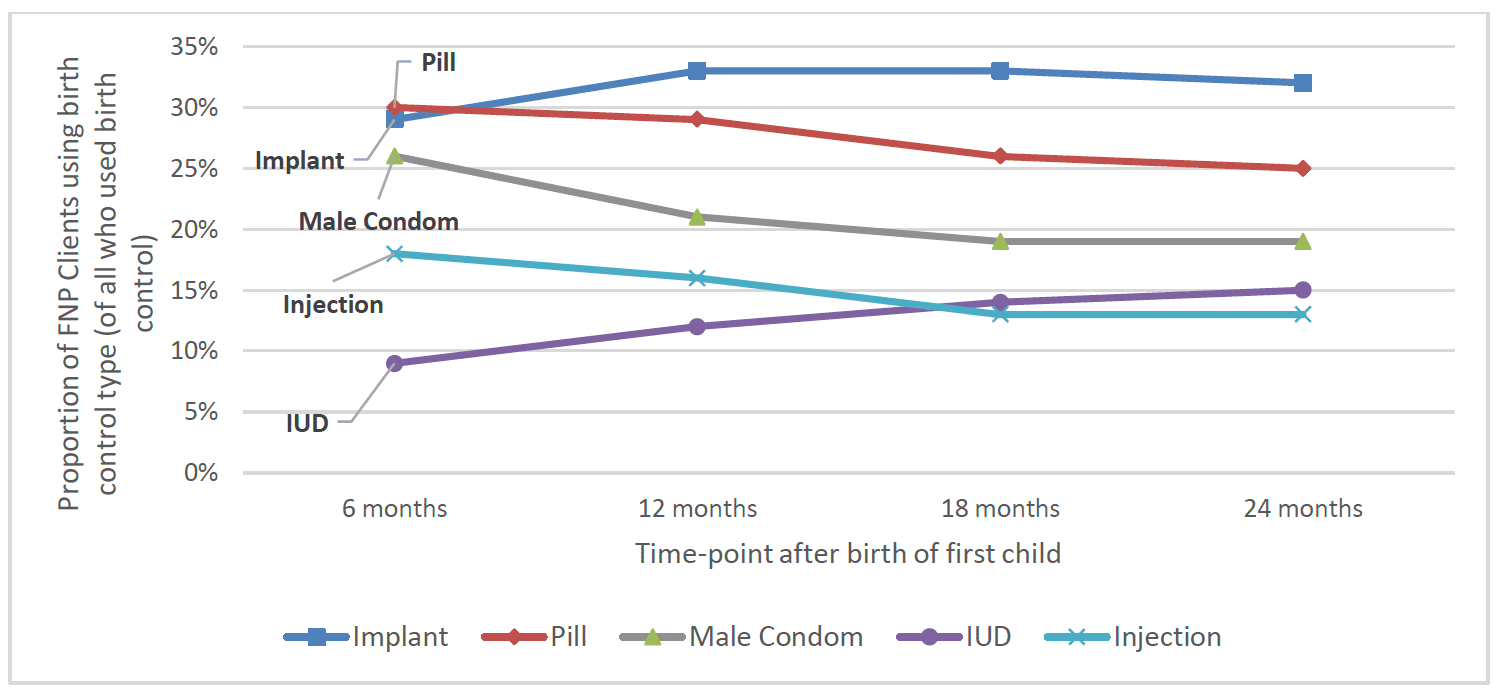
The most common forms of birth control used were the contraceptive implant (around a third of those using birth control used this at each timepoint) and combined oral contraceptive pill (around 30% used this at six months post-birth, though this decreased to around 25% by 24 months post-birth). The male condom was another commonly used birth control method, though use of this decreased from 26% at 6 months post-birth to 19% at 24 months post-birth. The next most commonly used birth control methods were IUD and contraceptive injection, with around 10-15% of those who used birth control using these at each time-point (Chart 21).
When viewing the proportion of all FNP graduates using LARC forms of birth control, a similar proportion of FNP graduates overall were using these at 6 months post-birth (46%) and 24 months post-birth (44%).
Between 2015-16 and 2020-21, the proportion of the overall FNP client group using LARC at 6 months decreased (from 50% to 43%) as did the proportion using LARC at 24 months (from 49% to 42%). This is possibly partially attributable to the composition of the FNP client group including an increasing number of mothers aged 20 and over in later years, of whom a smaller proportion used LARC at 6 months and 24 months (44% and 39% respectively), when compared to mothers aged 17 and under (52% and 48% respectively).
Of the small group of clients who were sexually active but did not use birth control at 6 months post-birth, most did not have a reason stated for not using birth control. However, the reduction in overall birth control use at subsequent time-points appears to correspond with an increase in clients who were either pregnant or trying to conceive. By 24 months post-birth 298 clients were pregnant and 116 were trying to conceive (around 10% of the client group overall).
Subsequent Pregnancies
Rapid, repeat pregnancy (i.e. within two years) is associated with an increase in adverse health outcomes[75]. An early repeat pregnancy has also been associated with a number of negative short-term consequences in the areas of education, employment, and welfare dependency[76].
Scottish data (2011) shows that approximately 25% of mothers aged under 20 will have a subsequent conception within two years (with around 7% conceiving again within one year). Percentages for under 18s are similar (24.9%), however rapid subsequent pregnancies amongst those aged under 16 are notably lower (5.9%).[77]
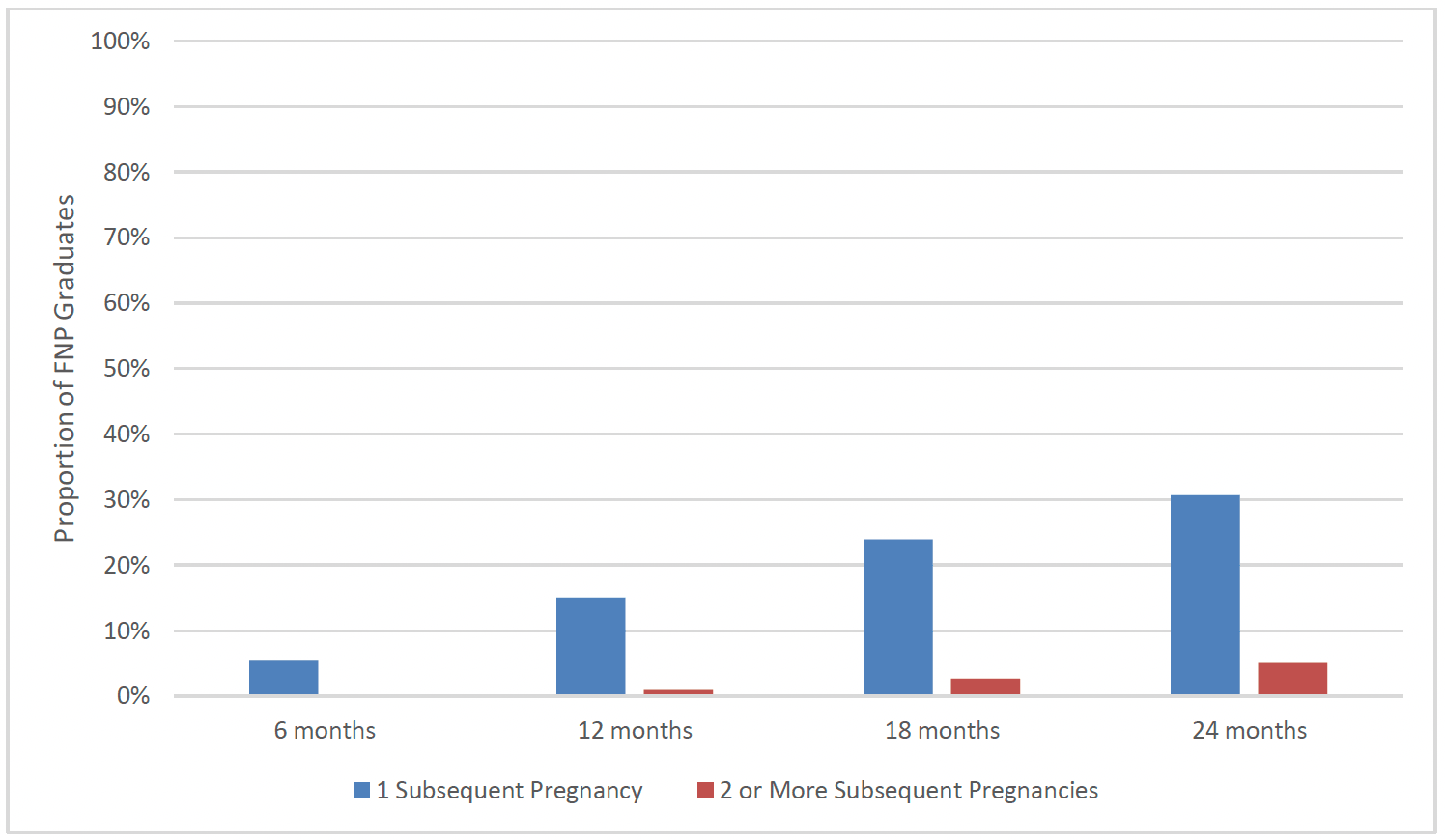
FNP clients were asked about whether they had experienced subsequent pregnancies at 6, 12, 18, and 24 months after the birth of their first child. Around one in twenty (5%) FNP clients had at least one subsequent pregnancy within 6 months. This increased to 15% by 12 months post-birth, around one in four (24%) clients by 18 months post-birth, and almost a third (31%) of clients by 24 months. By 24 months post-birth there was a small group of clients (5%) who had experienced more than one pregnancy since the birth of their first child (Chart 22).
These proportions in the Scottish FNP data are lower than similar data from England. The Building Blocks trial in England showed that 50% of mothers in the FNP group and 55% of the control group reported having had another pregnancy within 24 months[xviii], compared to 31% of FNP clients that reported a subsequent pregnancy to their nurse in Scotland.
There was little difference in the proportion of clients by age or by geographical region experiencing a subsequent pregnancy, and there was no clear correlation in the proportion of clients experiencing a subsequent pregnancy over time. A slightly higher proportion of clients in SIMD 1 (33%) and SIMD 2 (36%) at enrolment had experienced a subsequent pregnancy than those in SIMD 5 (29%). A higher proportion of clients who were in neither employment or education at enrolment experienced a subsequent pregnancy (36%) than those who were either paid employment or education (27%).
A slightly higher proportion of clients who spoke English as their primary language at intake (24%) had experienced a subsequent pregnancy by the time their child was 18 months old than those who did not (19%). The proportion of clients who did and did not speak English as their first language at intake experiencing pregnancy by 24 months post-birth was largely similar, though a higher proportion of clients who spoke English had experienced 2 or more pregnancies by this time-point (5% vs 1%).
Of clients who experienced a subsequent pregnancy, just under one third (31%) were single at 24 months post-birth, while 35% were in a relationship and living with their partner and 34% were in a relationship but not living with their partner.
Overall, one in five (20%) of clients who were using LARC at 6 months post-birth had reported a subsequent pregnancy by 24 months post-birth, compared to 42% of clients who were not using LARC at 6 months.
Subsequent Births
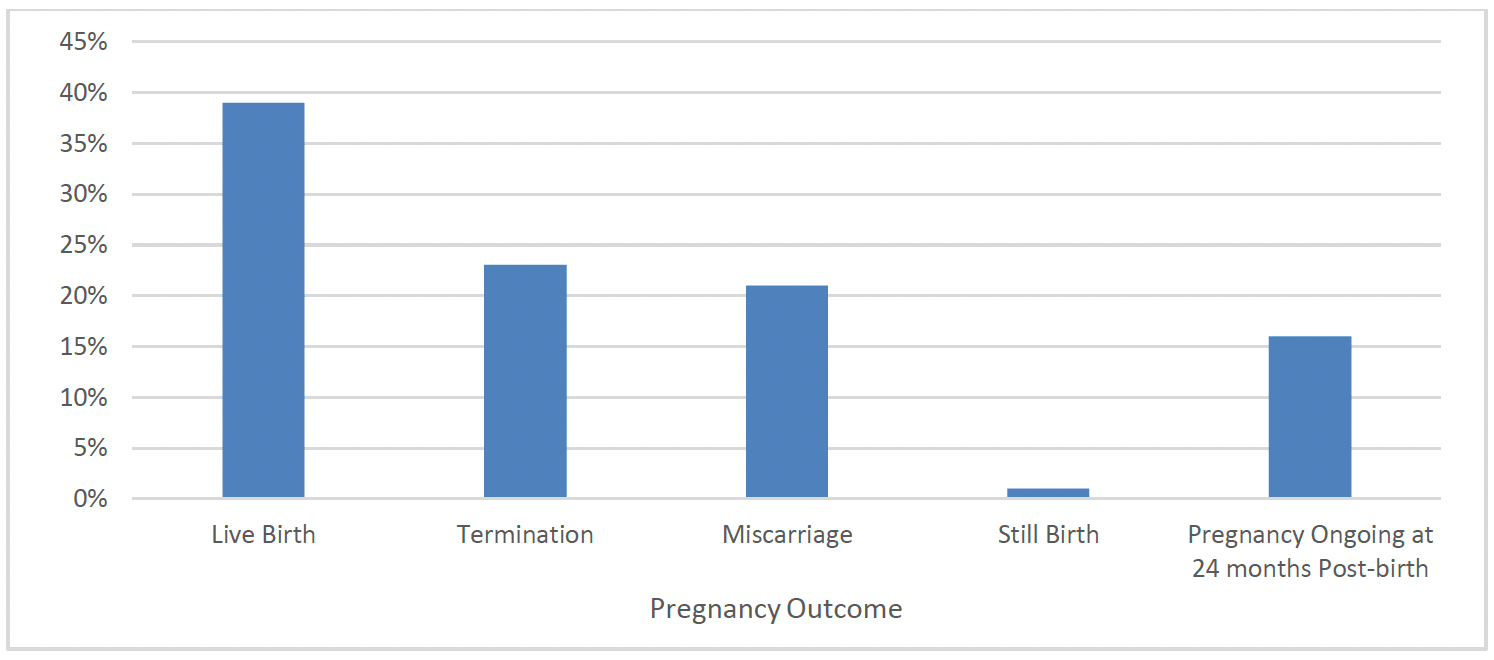
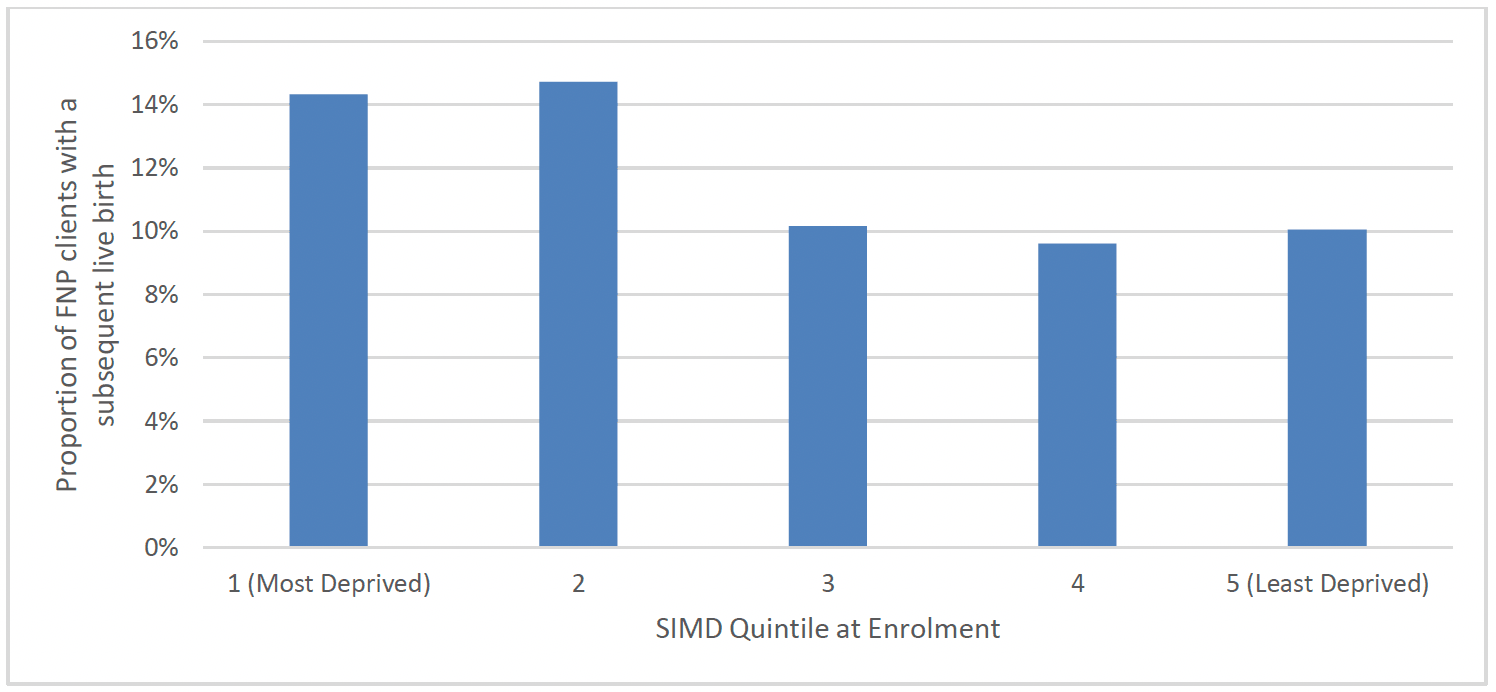
Overall, 13% of FNP clients had a live birth by 24 months after the birth of their first child. Therefore, of the subsequent pregnancies experienced by FNP clients up to 24 months post-birth, around two in five (39%) resulted in live births, representing 628 clients having subsequent live births. One in five pregnancies resulted in termination (22%), and one in five (23%) resulted in miscarriage, and the majority of the remainder of pregnancies (16%) were still ongoing at the time of graduation from FNP (Chart 23).
The proportion of FNP clients who had a subsequent live birth was broadly similar across client age groups. Clients from the most deprived areas (SIMD 1) (14%) were slightly more likely to have a subsequent live birth by 24 months than those from the least deprived areas (10%) (Chart 24). A higher proportion of clients who were in neither employment nor education at enrolment experienced a subsequent birth (16%) than those who were (10%). The proportion of FNP clients having a subsequent live birth was broadly similar for clients who did and did not speak English as their primary language at intake and over time.
Of clients who experienced a subsequent pregnancy, around a quarter (24%) were single at 24 months post-birth, while 40% were in a relationship and living with their partner and 33% were in a relationship but not living with their partner.
The rate of subsequent births differed when comparing these rate with use of LARC. 6% of clients who were using LARC at 6 months post-birth had reported a subsequent birth by 24 months post-birth, compared to 19% of clients who were not using LARC at 6 months.
Education, Work, Housing and Relationships
Education and Work
Evidence shows that education and engagement with learning are key interventions that help young people to plan for their future – including pregnancy and parenthood. Supporting young mothers and fathers back into school or learning environments is important for preventing a rapid subsequent pregnancy and ensuring better outcomes for mother and child. Evidence suggests that a focus on employment and provision of jobs and higher earning for young mothers is associated with improved long-term self-sufficiency[78].
Findings from Growing up in Scotland in 2014[79] showed that 72% of mothers aged under 20 had a household income amongst the lowest 20% of all family incomes at 10 months after giving birth. By comparison, the same was true for 40% of mothers aged 20 to 24 and just 12% of those aged 25 or older. At all age points, mothers aged under 20 were significantly more likely than other mothers to be in the lowest income quintile. Mothers under 20 were considerably more reliant on state benefits and tax credits than are older mothers. This position remained as the child aged.
Findings from Growing up in Scotland[80] also showed that more mothers aged under 20 had qualifications at Higher Grade level or above when their child was aged six than they did when their child was aged two. Although acquisition of qualifications increases as their child grows, even when their child was aged 6, mothers aged under 20 at the time of their child's birth remained the group least likely (by a significant margin) to have these qualifications[81].
As well as being captured at intake onto FNP, information on clients' education, work and relationships was captured throughout their time on the programme, at 6 months, 12 months, 18 months and 24 months post-birth.
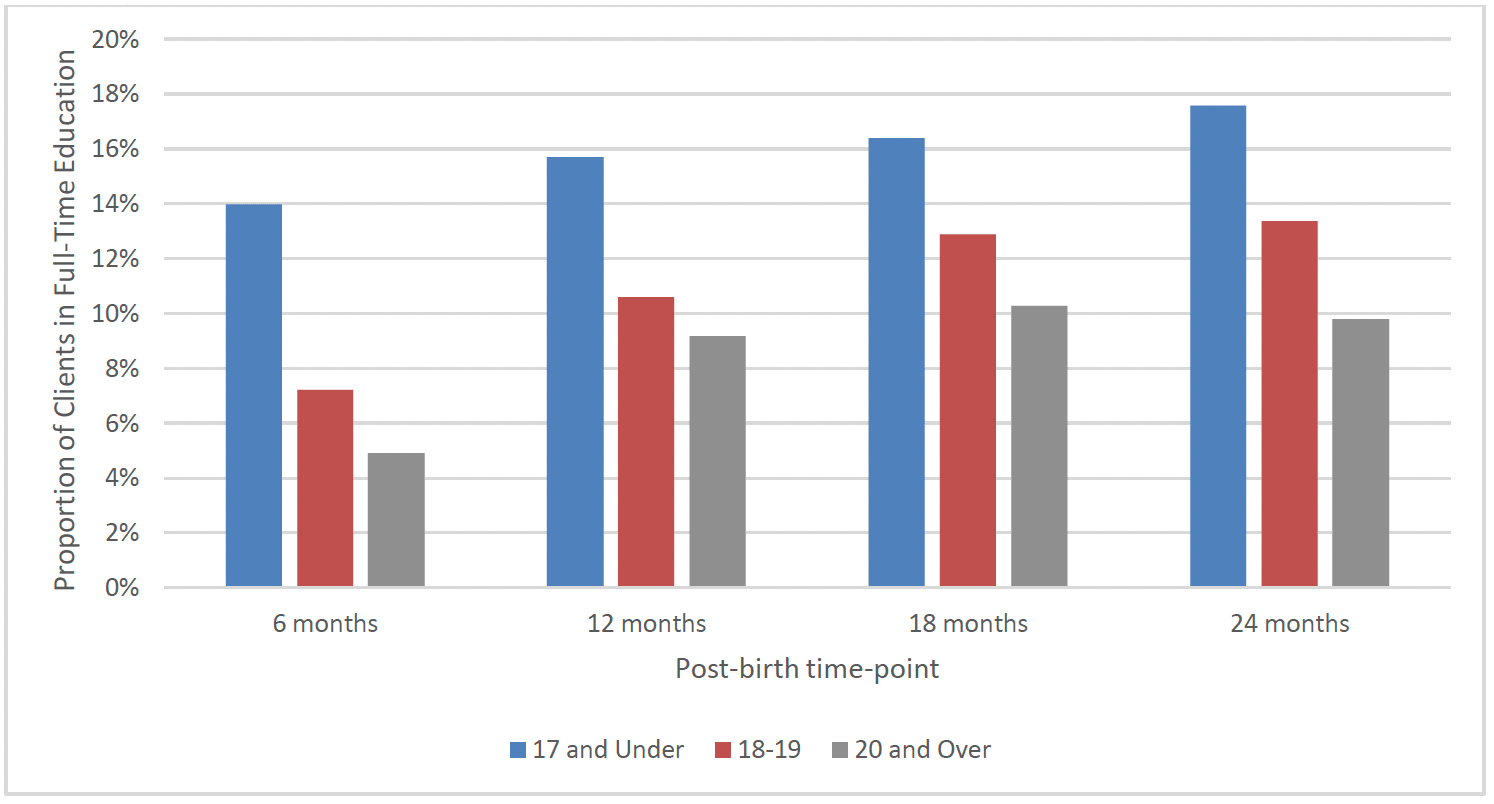
The proportion of FNP graduates in education post-birth increased from 9% in full-time education at 6 months post-birth to 14% in full time education at 24 months post-birth, as detailed in Chart 25 below. This trend of increasing educational attendance can be seen across all age groups with the youngest age groups more likely to be in full time education and the older age groups more likely to be in employment as shown below.
At 6 months post-birth there was a similar proportion of FNP graduates from the most deprived areas (9%) and the least deprived areas (11%) who were in full-time education. The proportion of clients in full-time education increased across all SIMD quintiles by 24 months post-birth, with 14% of clients in the most deprived areas in full-time education at this time-point, compared to 18% from the least deprived areas. There was a similar proportion of graduates in full-time education at these time-points in each region of Scotland.
The findings from Growing Up in Scotland showed that at 10 months, 21% of mothers under 20 were employed (either full-time or part-time) compared with 55% of those in their early twenties and 83% of those aged 25 or older. As the child ages, mothers aged 25 or older remain most likely to be in employment and mothers aged under 20 remain least likely. Employment levels amongst mothers aged under 20 do increase over time, however, whilst for other groups they remain similar, so that by the time the child is age six the gap is narrower than at age two.
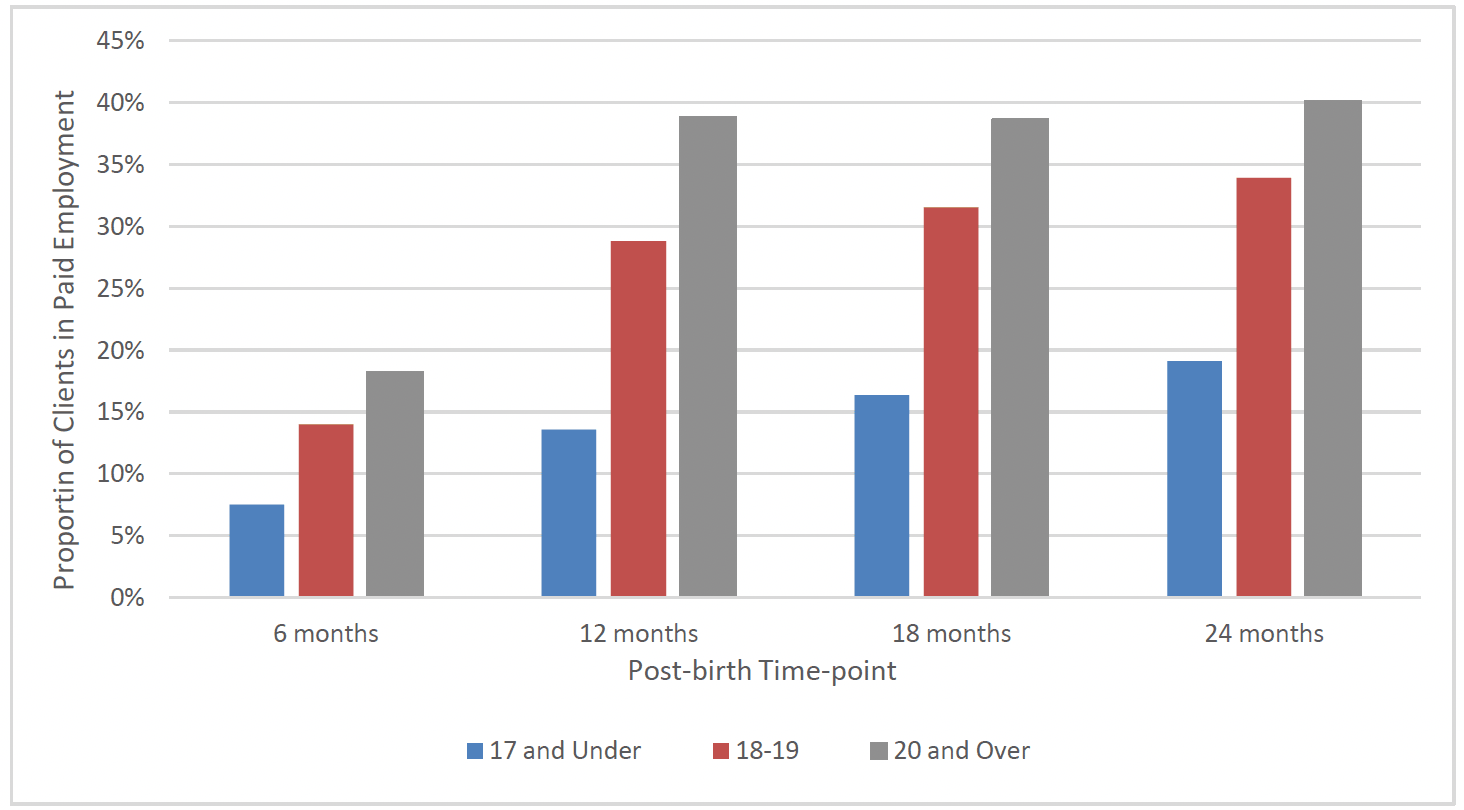
Overall, over one in ten (12%) clients who went on to graduate from FNP were in paid employment at 6 months post-birth, however this increased to one in four clients (25%) by 12 months post-birth and almost a third (30%) of clients by 24 months post-birth. The proportion of clients in paid employment increased across all client age groups between 6 months and 24 months post-birth: increasing from 8% to 19% of clients aged 17 and under at enrolment, 14% to 34% of clients aged 18-19 years and 18% to 40% of clients aged 20 and over (Chart 26).
There was also a differential in the proportion of clients from the most and least deprived areas in paid employment at subsequent time-points post-birth. While the proportion of clients from the most deprived areas in paid employment increased from 10% at 6 months post-birth to 25% at 24 months post-birth, the proportion of clients in the least deprived areas in paid employment increased from 16% at 6 months post-birth to 48% at 24 months post-birth. By 24 months post-birth there was a higher proportion of clients from the North of Scotland (35%) in paid employment when compared to those from the East (29%) and West (27%) of Scotland.
Taken together, those in work or education post-birth increased across all age groups, SIMD quintiles and regions: from 20% in work and/ or education at 6 months post-birth to 40% at 24 months post birth.
Housing
At each post-birth time-point, the majority of FNP clients lived in local authority or housing association housing, and the proportion living in this type of accomodation increased slightly from 60% at 6 months post-birth to 65% at 24 months post-birth. Most of the remaining clients either lived in privately rented or in privately owned accomodation.
The proportion of clients living in temporary accomodation was relatively stable between post-birth time-points at 3-4%. The proportion of clients who were registered homeless was only consistently captured on the data system for clients entering FNP in more recent years, but from the avaiable data it appears that the proportion of clients who were registered homeless was relatively stable at subsequent post-birth time-points at 4-5%.
This is similar to the findings in Growing up in Scotland that the majority of mothers aged under 20 lived in social rented housing and were the group most likely to do so. The figure increased over time with a corresponding decrease in the proportion living in owner-occupied housing. Mothers aged under 20 were more likely than older mothers to live in the most deprived areas. The gap between them and those aged 25 or older did not change over time.
Relationships
Findings from Growing Up in Scotland showed that when the child is aged 10 months, mothers aged under 20 were less likely to be living with the child's biological father. The figures differ starkly by age. 30% of mothers aged under 20 live with the child's father compared with 56% of those in their early twenties and 89% of those aged 25 or older. By the child's sixth birthday, mothers aged under 20 were still more likely than older mothers to be lone parents. However, a significant number who were lone parents when the child was aged two had partners by the child's sixth birthday.
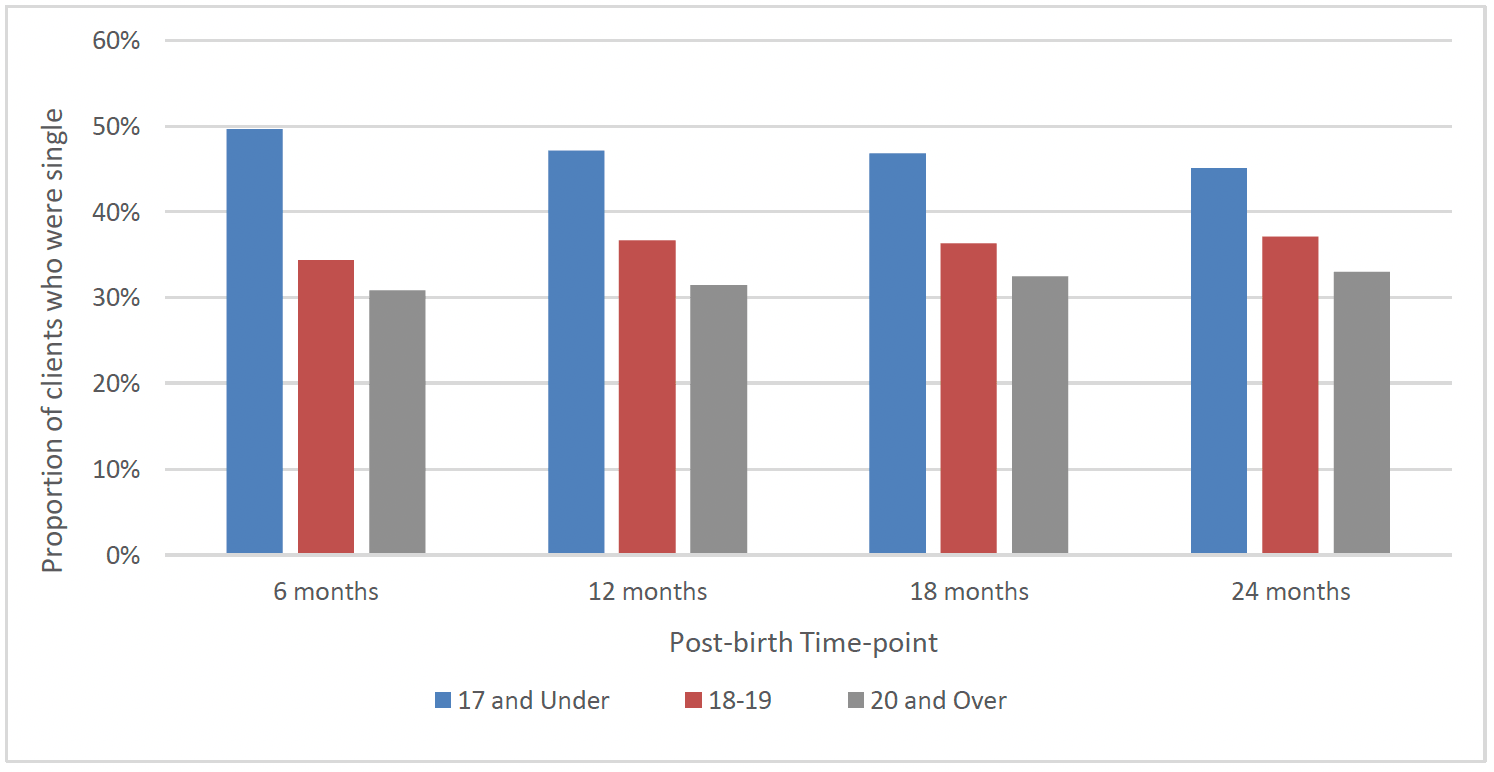
The proportion of FNP clients who were in a relationship was largely stable between post-birth time-points. At each stage, around 40% of clients were single, 30% were living with their partner and/or married or in a civil partnership, and 30% were in a relationship but not living with their partner. At each stage, a higher proportion of clients aged 17 and under were single than other age groups, though this gap narrowed slightly over time (Chart 27). There was no clear difference in the proportion of clients from the most and least deprived areas who were single at 6 months and 12 months post-birth. There was, however, a slightly higher proportion of clients from the most deprived areas who were single at 18 and 24 months post-birth (41% at both time-points), when compared to those from the least deprived areas (36% at both time-points).
Contact
Email: Justine.Menzies@gov.scot