Scotland's cancer strategy: services and support evaluation
Findings from an evaluation of cancer treatment services and support in Scotland. Specifically it looks at experiences of patient access and engagement with cancer treatment and support in rural and island areas, and in areas with higher deprivation.
Chapter 5. Travel and transport – evaluation findings
This chapter explores travel and transport-related factors and how they promote or hinder timely access to, and effective engagement with, clinical cancer treatment services and wider support. It considers key themes and associated challenges and facilitators for people living in more deprived and rural and island areas of Scotland.
Key findings
- Distance to treatment was a significant challenge for patients in more deprived and rural and island areas, often resulting in long travel times and, in some cases, influencing treatment decisions.
- Travel to appointments was particularly difficult for patients with pre-existing mobility issues.
- Availability and reliability of public transport options exacerbated travel difficulties, impacting access and patient experience.
- Limited parking availability caused patients stress, though designated cancer centre spaces at one hospital improved this issue.
- Third sector-run transport services were available across the case study areas and helped overcome travel barriers for some patients. However, provision of these services was variable within health board areas.
- Transport organised by the NHS to treatment in other health boards helped some patients in rural and island areas overcome barriers to attending their appointments. However, provision was somewhat inconsistent. In terms of patient transport within board, there were strict eligibility requirements.
- Travel created a significant financial burden for patients from both more deprived and rural and island areas.
- The way that appointments were organised exacerbated travel challenges for some patients. For example, patients often had various scans and appointments scheduled on different days. An important facilitator, which improved patient access and experience of treatment, was appointments being arranged to minimise the number of journeys required.
- While patients tended to accept a certain amount of travel was necessary for medical treatment, even if it was a challenging experience for them, travel to support services was a more significant barrier to access for patients in both rural and island and more deprived areas.
Distance to treatment
Journeys to hospitals for cancer treatment and associated medical appointments, such as consultations and scans, were a significant challenge for patients in both more deprived and rural and island areas. A key reason for this was the distance that patients were required to travel to appointments, which was further exacerbated by other travel-related challenges discussed in this chapter.
Journeys from rural and island areas
Patients in rural and island areas often had to travel significant distances to receive treatment outwith their own health board, sometimes involving several day-long round trips to attend one short appointment, or several weeks away from home for treatments such as radiotherapy, which are received on consecutive days. Due to the geographies of the rural and island areas, appointments delivered within board still often necessitated journeys of several hours to and from appointments.
Although staff felt that, most often, travel challenges could be managed, and that generally patients took up treatment that they considered was to their benefit, they shared some examples of travel considerations affecting patients’ decisions around receiving treatment. For example, a staff member explained that some patients started off travelling for treatment, but decided at a certain point that it was too much for them to manage. A patient interviewed shared a similar personal decision, describing his “terrible journey” to his second round of chemotherapy, with his wife having to drive a significant distance to collect him in foggy and icy conditions. These travel challenges had been a factor in his decision to stop chemotherapy after the second round.
“I was supposed to do four rounds of chemotherapy after the operation, but decided for a couple of reasons not to do the last two - one was the effect of chemotherapy on me and other one was the difficulty getting there and back to the [the cancer centre].” - Patient, rural and island area
There was a view among staff in one of the rural and island areas that decisions about travel depended on people’s stage of life, illness, and perception of their ability to cope with the combination of treatment and travel.
There was a level of acceptance from patients that living in a rural or island area inevitably involved more travel for appointments.
"We've grown up here travelling, so we're used to jumping in the car and going forever. And even when you're sick, it's something that you're used to. It's not like a big deal.” - Patient, rural and island area
However, it was evident from both staff and patient interviews across the rural and island case study areas, that travel was a primary challenge in receiving treatment, and a significant stressor. Having to organise and travel these long journeys impacted patients’ experience of treatment, increasing their mental load at an already psychologically difficult and overwhelming time.
"I think that's what causes the most stress to most of the patients, to be honest. It's not the actual treatment itself, it's how they're going to get there. And will they get there on time? You know, will they get there on the day they're meant to go there? What if their treatment's delayed? What impact will that have?" - Staff, rural and island area
As well as having concerns about how they would physically get to treatment, patients worried about other aspects of the journey, particularly when not driving themselves. This included whether they would have access to a toilet on route or if they would be able to get assistance if they were not feeling well. The journeys required for those in rural and island areas were felt by staff to be particularly difficult for patients with caring responsibilities for children or other relatives, for patients lacking a support network, and for patients who were frailer and/or older.
The distance to treatment also meant that if appointments were arranged or cancelled at late notice, it was difficult for patients to attend. For one patient in a rural area, a late notice change of appointment to a hospital further away, which they had no way of getting to, coupled with communication issues with staff, resulted in them missing two appointments and receiving a letter telling them their treatment would be stopped due to lack of cooperation.
Journeys for patients living in more deprived areas
While the length of journeys required by patients in more deprived case study areas were typically shorter, physically getting to appointments was still a significant challenge. Some patients had to travel out-of-board for scans, or for radiotherapy. For example, one patient discussed having to travel an hour and a half for specialist treatment, and travelling the night before for early morning appointments.
Staff discussed that some patients were not used to travelling outwith their local area and found it extremely anxiety-inducing to consider doing so, to the point that it put some off receiving treatment.
"I'm often surprised at the patients who don't want a potentially curative treatment because they don't want to come to [city within health board] for four weeks, Monday to Friday." - Staff, more deprived area
It also led to some patients delaying their treatment in the hope of being able to access it at a hospital closer to them. For example, a staff member from a more deprived case study area shared an anecdote of a patient who had refused to travel to the city for a biopsy and waited to see if she could receive it closer to home, which resulted in her only option being palliative care.
Similar anxieties were evoked for patients receiving appointments within board, which in some cases still involved significant journeys across the city, on multiple forms of transport, and into unfamiliar areas. Staff from one case study area noted that travel to appointments was particularly difficult and overwhelming for patients with pre-existing mental health issues such as anxiety or agoraphobia. A patient from the same area explained they had not left the house in five years before their diagnosis. They managed to attend treatment by taking taxis to appointments but found this very difficult.
Availability of public transport
Travel was particularly difficult for those without access to a car or someone (e.g. a family member or friend) to drive them. In rural and island areas, this was in part due to the lack of provision of public transport options such as ferries and planes, which were said to have worsened over recent years. For example, one patient explained that a flight stopped being run during her treatment, meaning she thereafter had to take the ferry and stay overnight. Staff noted that the newer replacement flights were much smaller, making it difficult for patients to book a seat. Patients were also competing with commercial passengers for spaces on flights and ferries, causing particular difficulties during summer. This was said to be particularly stressful when patients received last minute appointments. A staff member explained that they had spoken to the local ferry provider about this issue and had been assured that there would always be a couple of spaces available, but this had not always been the case in their experience.
Ferry and flight timetables not aligning with patients’ appointment times also led to long and sometimes uncomfortable waits at airports or ferry terminuses, and additional overnight stays for some patients if they could afford it. In some areas there was a lack of availability of transport on specific days of the week – for example, on Sundays – meaning some patients could not manage to go home at weekends in between weeks of radiotherapy treatment. There were also accessibility issues raised, related to patients’ health and mobility. For example, the small planes flying from rural and island areas were described as being cramped, uncomfortable, and unsuitable for those in wheelchairs.
In more deprived areas too, depending on where patients lived, there were issues with access to public transport. Staff and patients noted that living in an urban area did not necessarily mean there were direct public transport links to the hospital. Often patients had to take several forms of public transport to get to their appointment and, in some cases, they relied on taxis. However, staff explained that this could also present practical challenges, as taxi drivers were sometimes reluctant to take passengers with mobility issues, due to concerns about health and safety issues when helping them in and out of the vehicle.
Reliability of public transport
Furthermore, even where public transport was available, there were issues with its reliability, which caused delays to some patients’ treatment and created significant stress. This was an issue in rural and island areas in particular, where planes and ferries were susceptible to delays and cancellations due to weather conditions – there was a view that this was worsening and would only continue to worsen in future, due to climate change. Travel plans having to change last minute created difficulties for patients in establishing whether they could find alternative means to travel to treatment. In some cases, patients were already waiting at the airport before they found out their flight was cancelled and their whole plan would have to change. This exacerbated other issues in terms of transport availability – for example, a patient may be able to book a different flight to treatment in the event their original flight was cancelled, but may not be able to book on to a flight back on the same day, and have to stay overnight.
“On the week that I would have received treatment, the flight was cancelled twice in the same week… the added stress that it brings when you’re geared up for the treatment, or you’re geared up to have a procedure, whether that be a scan or an appointment with a consultant, it’s not conducive to maintaining mental health that’s required to cope with everything else that goes with it.” - Patient, rural and island area
Staff explained that unreliable public transport delaying patients’ journeys also sometimes caused issues with prescription expiry, e.g. chemotherapy or blood transfusions, which delayed treatment.
Parking issues
For those patients with access to a car, or somebody to drive them to appointments, there were issues with finding a parking space due to hospital car park capacity. The parking situation at several hospitals was described as “stressful” and “horrendous” by patients, and was highlighted by staff too. Patients said they had to arrive much earlier than their appointments to try to get a parking space, or park far away from the hospital. ICJ staff explained that they could help some patients apply for Blue Badges so they could access designated parking spaces closer to the hospital. However, finding an accessible parking space was still difficult.
One hospital was highlighted as having designated Cancer Centre parking spaces, which made a positive difference for patients receiving treatment there. The fact that car parking was free at hospitals across Scotland was also welcomed.
Impact of mobility issues and side effects
Travel to appointments was particularly difficult for patients with pre-existing mobility issues. As discussed above in relation to the availability of public transport, this created issues in using public transport, as well as taxis, in some cases.
Travel challenges were also exacerbated by the exhaustion and physical side effects patients experienced from treatment. Staff from rural and island areas explained that the travel involved may seem manageable for patients at the beginning of their treatment, but as it progressed, and they begin to feel physical side effects, it became more difficult.
"[My patient] really underestimated the effect that travelling [can have] while you're on cycle four, five or six of chemo, when you're not well anyway, and then you're having to travel on these flights, [stay in] hotels, it’s really, really challenging. To the point my patient, when they were offered a further palliative chemo, declined it because she they just could not tolerate the travel". - Staff, rural and island area
Some patients also found it anxiety-inducing to be around other people on public transport and were worried about picking up illnesses when they were already unwell. Staff sometimes advised them not to take public transport if they were immunocompromised. As well as causing stress, concern about mixing with other passengers led to some patients taking measures which made their journey more uncomfortable. For example, a patient shared that when taking the ferry to treatment, they had requested that they could stay in their car, which had been cold and uncomfortable. Whether or not passengers could stay in their car on the ferry was also dependent on space availability on the ferry and had to be requested in advance. Staff in one rural and island area shared that the local ferry provider facilitated a better experience for patients through a service where, if they had advance notice, they would drive patients onto the ferry in a minibus, drop them off at the lift, and make sure they got off safely at the other end.
Not feeling well enough to travel also meant that some patients had longer stays away from home – for example, staying at weekends in between radiotherapy because they did not feel well enough to travel home. There was a sense among both staff and patients in rural and island areas that patients had to be healthier to cope with treatment when living in those parts of the country as a result.
Patient transport options and community transport
Patient transport
Transport organised by the NHS to treatment in other health boards helped some patients in rural and island areas overcome barriers to attending their appointments. However, provision was somewhat inconsistent. For example, staff from one rural area explained that transport for radiotherapy and chemotherapy was provided, but not for surgery or other appointments such as pre-operative consultations and scans. This caused significant stress if patients had morning appointments and sometimes prompted them to decide to book a hotel the night before (which they had to pay for themselves). Patients also could not then drive themselves home after surgery, so had to rely on a friend or family member. Furthermore, when transport such as minibuses were provided, this did not always fully mitigate travel challenges, as patients still had to travel to the pick-up point. Some staff felt that there should be more of an onus on health boards to provide better transport support.
"Having the treatments available is fantastic, but we need to be able to get patients there without them being out of pocket and without them having to risk changing or delaying their treatment because of it." - Staff, rural and island area
In terms of patient transport within board, there were strict eligibility requirements – it is generally provided for those with a certain severity of mobility issues, but not for those who struggled to get to hospital for other reasons such as anxiety, lower level mobility difficulties, lack of access to public transport, being immunocompromised, or not being able to afford other forms of transport. One patient from a more deprived area explained that they had a “bad leg” and were barely able to walk around the corner without getting out of breath due to their health, which meant they were unable to take the bus to appointments. They asked for help from the patient transport team but were “refused point blank” because they were considered to be mobile enough. The patient explained this did not affect their decisions around treatment and they managed to get to all of their appointments because they knew that was their only option if they wanted to live. However, they ended up out of pocket paying for numerous taxis back and forth to appointments across the city. Other patients shared similar experiences of struggling to travel due to conditions such as arthritis, but not being eligible for patient transport.
“We're not always great in terms of people who maybe don't have a very pronounced disability, but it does impact on their ability to access services or to travel independently, etc. There's not always the resource to support that.” - Staff, more deprived area
One staff member described it as a “fight” to access patient transport. Others noted that sometimes patients’ requests were denied because they were not able to sufficiently articulate why they needed patient transport. Staff from a more deprived area also said that if patients had a family member who could drive them, even if that person was unavailable, they would be considered lower priority need.
Furthermore, for those who were eligible for patient transport, there were difficulties associated with the experience. For example, a patient from a more deprived area explained that they had to be ready to be picked up hours before their appointment due to being the first person to be collected, and that there was a lack of consideration as to how long one was able to sit for – nurses had recommended to them that they should only sit in a wheelchair for an hour a day. Patients also sometimes ended up sitting at the hospital for hours depending on how the timing of the transport lined up with their appointment time. Staff from a more deprived area highlighted that there were added complications for patients with medical needs such as tube feeding and medication to take during their journey. Additionally, patients could not take a family member with them on patient transport.
When patients had to go into hospital at late notice, staff in a more deprived area said they could organise an ambulance, but that took several hours no matter the urgency of the situation. Occasionally, when their patients faced significant challenges in getting into hospital, staff had been able to authorise private taxis.
Community/volunteer transport
Third sector-run transport services were available across the case study areas and helped overcome travel barriers for some patients. For example, one patient shared a largely positive experience of a local charity picking her up and taking her to hospital (she had found out about the service from her nurse). Another patient’s GP service had access to volunteer drivers, which she acknowledged she was very lucky to have.
“Someone came to pick me up to take me to the clinic and I know that this is an individual circumstance for this area that I live in and it doesn't happen everywhere. So I am extremely lucky having this diagnosis where I live.” - Patient, rural and island area
In one of the rural and island areas, there was a cancer support centre, heavily supported by a local independent charity, which funded transport for patients and made a significant difference in addressing the travel barrier in their part of the region. ICJ staff noted that befriending services were also useful for some people who needed support with getting to appointments.
Organising volunteer transport for patients was something that the ICJ team helped patients with in some cases. However, they were limited by lack of availability. Staff explained that provision of volunteer transport services was variable within health board areas, with patients’ access being dependent on where they lived. Services also had to be pre-booked, so challenges remained when appointments were cancelled or rearranged at late notice. Furthermore, ICJ staff in one area said that specialist taxis which they could organise still cost patients a significant amount in some cases. The taxi service was also said to be unreliable due to the lack of capacity to meet demand.
ICJ staff in a rural and island area voiced concern about what would happen if volunteer transport services were to further reduce or stop running and felt there should be more encouragement of community transport scheme development.
“I've heard people say, you know, ‘I just felt like a pest’ or, you know ‘I'm having to ask my neighbour again’. So I don't know whether we need to be looking at encouraging social enterprise, volunteer led things. But again, they need money, they need training, they need support.” - Staff, rural and island area
Cost of travel
Cost of travel was a significant issue for patients in both rural and island and more deprived areas.
Rural and island areas
Patients incurred costs from long journeys to and from treatment (e.g. public transport or petrol costs) and overnight stays. Accommodation for those in rural and island areas travelling out of board for treatment was subsidised in some cases. However, patients and staff explained that it was not nearly enough to cover costs. For example, in one area, patients were entitled to £60 per night for accommodation, but in reality this could cost around £300 per night, with patients sometimes needing to be away for weeks at a time. Staff highlighted that the health board’s travel policy had not been reviewed since 1997. The level of subsidy also varied for patients within the same health board depending on which hospital they were visiting for treatment. For example, ICJ staff in a rural and island area explained that patients seen at the Beatson can stay at a nearby hotel with costs covered by the NHS, but this is not the case for treatment at some other hospitals. Furthermore, staff noted that travelling from one board to another, e.g. a flight, was typically well-subsidised, but costs of transport at the other end, such as taxis to and from the hospital, could still be significant and were paid for by the patient.
In some cases, hospital accommodation was provided. However, staff from a rural area explained that patient accommodation was only available for people who lived a certain distance away from treatment, meaning they could end up making a 100-mile round trip every day for radiotherapy. Additionally, some patients felt uncomfortable staying in the shared accommodation provided, so they paid for self-catering accommodation or a hotel.
Staff in rural and island areas thought that the majority of people travelled for treatment that was going to benefit them, but that the financial impact of this was often a concern and could lead to issues down the line for patients – for example, due to them taking out credit cards and getting into debt to pay their travel costs. One staff member said they knew of patients who had slept in their car due to the cost of accommodation. When patients had to stay away from home for treatment, they also incurred costs for meals and travel around the city.
There were additional costs to having a family member or friend accompany patients to treatment, or visit them in hospital. Staff in a rural area explained that there had been a “clamp down” on the escort policy and, when being transported by their health board, patients were expected to travel on their own unless they had a disability (the policy used to be that you could have an escort if you had a diagnosis of were expecting a diagnosis, so it was in line with other parts of Scotland.) Furthermore, when patients stayed overnight in hospital, after surgery for example, costs were incurred from their relatives having to pay for their own accommodation. One patient from a rural and island area shared that they had been able to afford to rent a caravan and book a campsite for their family when going to another board for treatment, but acknowledged the difficulties that others in a more difficult financial position would face. Staff said that some patients decided not to go for treatment because they were not granted an escort and could not afford to bring somebody with them.
"[The new escort policy] has caused huge distress. Huge distress. I've even had, like, elderly people say, 'well, I just can't go. I'm not going. I'm just not going to go because I can't do it'”. - Staff, rural and island area
As discussed in Chapter 4 and Chapter 7, having a support network is important for patients’ emotional wellbeing and comprehension in appointments, so not being able to bring someone with them can negatively impact patient experience.
More deprived areas
Although travel costs tended to be significantly less for patients from more deprived areas than for those living in rural and island areas, it was still a significant barrier – particularly for people on lower incomes. Bus or taxi fares across the city, often to multiple appointments on different days added up (see below in the section on organisation of appointments).
"I've had numerous patients have expressed that actually they don't have the financial means to even get the bus down to ourselves." - Staff, more deprived area
Patients described spending money on taxis that they could not actually afford, because they had no other transport options. For example, a patient from a more deprived area explained that he had to get taxis to and from treatment because he had no access to a car and was not mobile enough to take the bus (though he had not been eligible for patient transport). He had to travel outwith the city on one occasion for a follow-up scan which cost him £100 each way, and would have cost even more had he not known the taxi driver personally. The cost of taxis had a “terrible impact” for him financially and meant he had to keep borrowing money to cover the costs. Staff noted that cost of travel was a particular issue in emergency situations, when patients did not have anybody to drive them into hospital, but could not afford a taxi.
In terms of mitigating this barrier, ICJ helped patients and families apply for bus passes, particularly where they were eligible based on age or disability (though bus was not always a suitable mode of transport for patients e.g. due to mobility issues or in emergency situations, as already discussed). Sometimes patients could claim back expenses for travel. While some patients found this process straightforward, others found it stressful having to organise their receipts and submit the form when they were already exhausted and struggling to think straight. Furthermore, some patients did not have the money in the first place to pay for transport and claim it back. ICJ staff from one area suggested that, where the health board does cover travel costs, this should be paid by the health board up front rather than people having to claim back. There was also a lack of awareness of entitlement to compensation. For example, one patient from a more deprived area who had to travel outwith their board for treatment, said they had spent £5,000 on travel and were not aware they could claim this back until it was too late. Furthermore, staff noted that patients were often reluctant to discuss their financial difficulties and sometimes waited until the point that they were really struggling, before telling anyone. Generally, staff felt that when treatment was within board, there was a lack of support with transport costs.
Organisation of appointments
The way that appointments were organised exacerbated travel challenges for some patients. As discussed, in some cases, appointments were arranged for early in the morning which meant that patients from rural and island areas had to travel the evening before and stay overnight to be able to attend. Patients also discussed choosing to travel the night before appointments which they could theoretically make on the day, due to worrying about potential transportation issues.
Additionally, patients often had various different scans and appointments scheduled on different days, necessitating multiple journeys and further exacerbating their stress about logistics, and financial costs. This was particularly an issue when patients were accessing treatment in health boards that had cancer services spread across a number of hospitals.
“I had a chap the other day who was, I think he was visiting every hospital in [the city] for his treatment. He didn't have a lot of money and it was difficult for him to get there... I think that's difficult.” - Staff, more deprived area
As well as the additional cost involved in travelling to multiple hospitals, patients explained that it made the experience more overwhelming.
“You're already feeling vulnerable from your diagnosis and then it's like, oh my gosh, I've got to go to here, there and everywhere kind of thing." - Patient, more deprived area
As discussed in Chapter 2 in relation to equitable access to treatment options, staff also noted that often cancer treatment centres are located in the more affluent areas of the city, meaning longer journeys for patients in more deprived areas
Arranging appointments according to travel needs
An important facilitator, which improved patient access and experience of treatment, was appointments being arranged to minimise the number of journeys required (see discussion of appointment coordination in Chapter 2). In some cases, this meant organising appointments on the same day where possible. In other cases, this was about arranging appointments to fit in with transport times. CNSs in one of the rural and island areas felt that coordinating appointments around people’s travel needs was “one of their biggest roles”, and in one of the more deprived areas, the SPoC navigator was described as playing a key role in working with CNSs to organise CT scans and treatment on the same day. Patients shared examples of staff accommodating their needs. For example, one patient living in a more deprived area was originally due to have scans at a hospital far away from them, but their consultant arranged for the appointments to be moved to a closer hospital to minimise time and taxi costs. A patient from a rural area was able to have their blood tests done locally, which they said was very helpful, and another explained that their local oncology unit arranged their appointments to align with bus times.
“If I have an appointment in local hospital in [other health board], the oncology unit know that I come in on the bus… then I have an appointment made for 12, midday, and I get there usually at about quarter to 12.” - Patient, rural and island area
Staff being generally accommodating and reassuring patients if things went wrong with their travel arrangements was also positively received.
“Normally it’s not a big deal, [but] when you're already ill, having to get trains and ferries before the ones you need, to make sure that you're not missing appointments starts to get really challenging. And the teams at all the hospitals were so understanding about that and said that they would never turn me away if I was late or something had gone wrong. I was always just to phone them.” - Patient, rural and island area
Some patients, however, felt it had been assumed that they would be able to get themselves to appointments, and that proactive support and awareness of travel difficulties was lacking. This tended to be more the case for patients in more deprived areas, and for patients from rural and island areas who were travelling within their own health board.
As discussed in Chapter 2, phone or video appointments had helped mitigate travel challenges to some extent.
Distance to support, prehabilitation and rehabilitation
While patients tended to accept a certain amount of travel was necessary for medical treatment, even if it was a challenging experience for them, travel to support services was a more significant barrier to access for patients in both rural and island and more deprived areas. Patients often felt it was too much to deal with the journey for non-essential appointments. While sometimes support services were based in the same hospital as they were receiving treatment, patients did not necessarily have enough time or energy to attend before making their journey home.
“Most of the support services, like sort of the Beatson, it's a long way. The parking at that hospital is horrifically brutal. It's not too horrendous by train, but it's quite expensive to do. So I didn't really use an awful lot of the services that were over the water because it was already costing me enough to travel for the essential appointments and even things like access to wigs, wig fittings.” - Patient, rural and island area
Staff also noted that they felt patients were less likely to travel for prehabilitation or rehabilitation appointments which were often considered to be supplementary, rather than key appointments.
Recommendation 11: In line with the People Principle in Scotland’s Health & Social Care Service Renewal Framework and the Population Principle in Scotland’s Health & Social Care Service Renewal Framework[9], facilitate ease of travel for patients by:
- Reviewing travel expense policies to ensure these, as far as possible, reflect the cost of travel and meet the needs of patients. Consider whether it is possible to expand entitlement to an escort. Ensure all patients are aware of, and understand, travel expense policies.
- Considering whether any improvements can be made to appointment scheduling to better consider patient travel needs.
- Working collaboratively with Regional Transport Partnerships and other partners to co-design and implement transport options which support people to access treatment.
- Exploring how free parking at hospitals can be improved, perhaps through designated spaces.
- *Encouraging the setup of more volunteer transport for patients in both rural and more deprived areas.
- *Working with ferry companies/airport operators to accommodate patients’ needs e.g. having dedicated space for those worried about coming into contact with other passengers.
Figure 5.1 illustrates a patient’s experience of cross-health board travel. It shows key aspects of their journey and how these relate to the dimensions of the COM-B model of behaviour change.
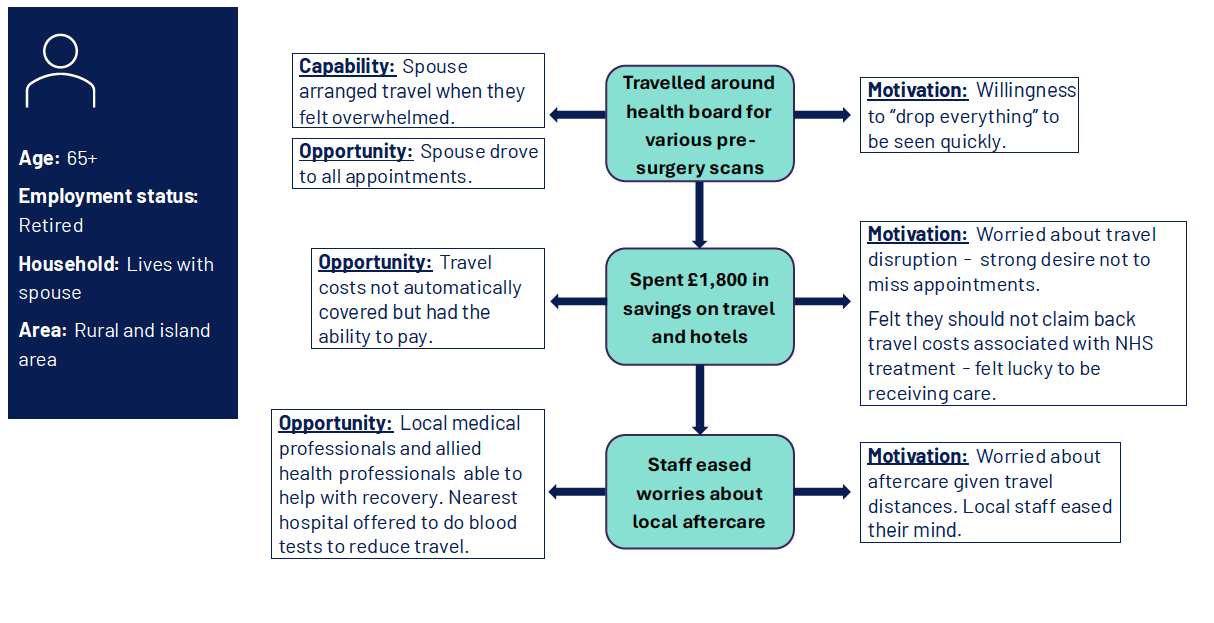
Diagram showing three stages of a patient's journey and relevant COM-B dimensions
Patient characteristics
- Age: 65+
- Employment status: Retired
- Household: Lives with spouse
- Area: Rural and island area
Stage 1: Travelled around health board for various pre-surgery scans
- Capability: Spouse arranged travel when they felt overwhelmed. Opportunity: Spouse drove to all appointments.
- Motivation: Willingness to “drop everything” to be seen quickly.
Stage 2: Spent £1,800 in savings on travel and hotels
- Opportunity: Travel costs not automatically covered but had the ability to pay.
- Motivation: Worried about travel disruption - strong desire not to miss appointments. Felt they should not claim back travel costs associated with NHS treatment - felt lucky to be receiving care.
Stage 3: Staff eased worries about local aftercare
- Opportunity: Local medical professionals and allied health professionals able to help with recovery. Nearest hospital offered to do blood tests to reduce travel.
- Motivation: Worried about aftercare given travel distances. Local staff eased their mind.
Contact
Email: socialresearch@gov.scot