Scotland's cancer strategy: services and support evaluation
Findings from an evaluation of cancer treatment services and support in Scotland. Specifically it looks at experiences of patient access and engagement with cancer treatment and support in rural and island areas, and in areas with higher deprivation.
Chapter 6. Wider financial and practical issues – evaluation findings
This chapter explores wider financial and practical factors and how they promote or hinder timely access to, and effective engagement with, clinical cancer treatment services and wider support. It considers key themes and associated challenges and facilitators for people living in more deprived and rural and island areas of Scotland.
Key findings
- Having to take time off work to undergo cancer treatment, and the associated loss of income, was a key challenge faced by patients, particularly in more deprived areas. This sometimes impacted their decisions around which treatment(s) to take up or caused patients to return to work too early.
- Patients, particularly those in more deprived areas, reported struggling with living costs such as food, heating and clothes while undergoing cancer treatment.
- Fitting cancer treatment around caring responsibilities was identified as a challenge, practically and emotionally, for patients in both more deprived and rural and island areas.
- Some patients also faced challenges with housing while undergoing cancer treatment – for example, because their cancer symptoms or treatment side effects meant that their living situation was no longer suitable for them.
- The main way in which staff felt they could help patients financially, was to make sure they were in receipt of all the benefits they were entitled to. This involved referring patients for benefits assessments and advice and helping them to complete benefits applications. However, some patients in difficult financial circumstances had their applications rejected – several times, in some cases.
- ICJ teams across the case study areas were generally felt to have had a positive impact for patients that they had supported. However, the referral process into ICJ differed across case study areas which staff felt impacted the extent to which they reached patients who would benefit from support.
- Some patients also faced motivational barriers in asking for, or accepting, financial support. Support offered proactively by clinicians and staff in ICJ teams was a facilitator in patients being able to access support with financial and practical issues.
- Staff who were proactive in arranging financial support for patients (e.g. ICJ staff and CNSs) highlighted the lack of available options. For example, staff were frustrated that a previously available Macmillan Cancer Support grant had been cut.
Challenges
Loss of earnings
Having to take time off work to undergo cancer treatment, and the associated loss of income, was a key challenge faced by patients, particularly in more deprived areas. Staff felt that most patients took up treatment despite the financial impacts, but that their decisions around which treatments to take were sometimes influenced. For example, patients sometimes chose not to have radiotherapy, or not to have chemotherapy after surgery, which could improve their outcomes, due to the amount of time off work that would be required. Staff mentioned that some patients had to rely on Statutory Sick Pay which was a “drop in the ocean” compared to their usual income, and caused significant financial stress. Those who were self-employed or on non-permanent and/or zero-hour contracts were highlighted as being particularly vulnerable to loss of earnings. For example, a patient from a more deprived area who was self-employed said he was offered three treatment options and tried to choose the one that would involve the least amount of time off work. Another self-employed patient said it had crossed his mind to not have surgery due to loss of earnings (though he did end up taking the treatment). A staff participant from a more deprived area shared an example of one of their patients who felt they could not afford the time off work to have another hospital admission in order to get a feeding tube which had been recommended to them as a preventative measure after their treatment. Staff highlighted that the time required for treatment, and associated financial costs, were particularly difficult for patients with childcare needs.
Farming communities in rural and island areas were also identified as being particularly vulnerable to the financial impacts of undergoing treatment. Staff explained that farmers sometimes tried to minimise their hospital visits during lambing season or opted against treatment if they could not afford to pay someone to look after their stock.
Staff also discussed that patients often rushed back to work, which sometimes negatively impacted their recovery. This issue was echoed by patients who described their experiences of going back to work before they were really ready, because they could not afford not to.
“I then rushed back because I couldn't afford to go on zero wages… My employer gave me a phased return over eight weeks, but we’re a very small team… so it was very much ‘hit the ground running’ when you come back. And even now, a year on, I still struggle. Like yesterday I spent most of the day in bed working from home because I was really struggling.” - Patient, more deprived area
Undergoing cancer treatment also had lasting negative impacts on earnings for some patients, due to cancer symptoms or treatment side effects continuing to limit their physical capabilities. For example, a patient from a more deprived area was still struggling a year post-surgery due to the physical demands of her job, which restricted the number of shifts she could take. Another patient shared that he had been working full time before his diagnosis, but was only working part time afterwards – he felt impacts of the loss of income and was no longer able to do the things he used to do. Furthermore, staff discussed that some patients had needs, post-treatment, that were difficult to meet while at work. For example, they explained that those who had upper gastrointestinal cancer surgery typically needed to eat something every couple of hours in order to receive the nutrition they need, but struggled to do so in some jobs or work environments. Staff noted that such patients often returned to work too early and consequently struggled to maintain their weight, negatively impacting their recovery and their mental health.
While some patients’ employers had been supportive of their needs for time off work and accommodations when they returned, others felt they had lacked understanding.
“I appreciate they've got to provide a service, but a bit of humanity, I think, at times, and a bit of recognition that, although cancer is gone at the moment, the repercussions of this treatment are significant.” - Patient, more deprived area
Staff noted that some patients were pressured into early retirement due to ill health or unsupportive employers.
Recommendation 12: Raise awareness among employers about the impacts of cancer treatment (particularly the ongoing effects on health post-treatment), their duties under the Equality Act 2010[12], and how they can support staff. Create or signpost to existing guidance and have a means of ensuring it is implemented.
Living costs
Patients, particularly those in more deprived areas, reported struggling with living costs while undergoing cancer treatment. One patient, who was on universal credit and receiving no wages, said she was barely able to afford her house payments each month. She was not sure how she would have managed without financial support from her adult children.
“If it wasn't for my adult kids, I don't know where I would have been, because I was in such a financial crisis that they helped pay some of the bills.” - Patient, more deprived area
Paying for heating was identified by both staff and patients as being a particular issue, especially because, when receiving active cancer treatment, patients sometimes needed to keep their houses warmer than usual. When they struggled to do so, this risked negatively impacting their recovery. The cost of food was also challenging for some patients from more deprived areas and was something that staff identified as impacting recovery outcomes. Staff acknowledged that they often recommended patients to eat certain types of healthy food which they might struggle to afford or to access if they were using food banks, and highlighted particular issues faced by patients with specific dietary needs. For example, some patients required a blended or fortified diet including foods such as full cream milk, butter and cheese. When patients had cultural or religious dietary needs, this was said to add another layer of difficulty.
A staff member also highlighted the challenges faced by patients in temporary accommodation. They gave an example of a patient who was a refugee living in a hotel with only a kettle in his room. Food was provided to him, but was not appropriate for his poor appetite and he could not afford to buy extra provisions.
Staff noted that being tired from treatment made it harder to cook, and that patients on lower incomes were less likely to be able to afford ready meals, which could make their lives easier.
"It's all these little things that sort of bubble under the surface that can make things very challenging for patients, particularly if they haven't got a lot of financial security." - Staff, more deprived area
Patients also discussed not being able to afford new clothes which they needed due to treatment side effects such as weight changes or incontinence.
Struggling to afford living costs also exacerbated practical challenges around organising and attending treatment. For example, one patient who had to stop working and claim universal credit and adult disability payment (ADP) had to get rid of their car as they could no longer afford to run it. This meant they could not drive themself to and from appointments and led to knock-on transport challenges. Staff from a more deprived area also noted that some patients did not have enough money on their phones to answer calls about appointments.
Patients discussed the added stress that their financial situations caused at an already emotionally difficult time. For example, one patient from a more deprived area spoke about their worries that their family would not be able to afford their funeral in the future. They were receiving ADP which could have helped pay for taxis to and from treatment, but instead they were saving it for their funeral. Another patient shared that her financial struggles had led her to isolate herself because she felt she could not afford to go out and socialise.
Caring responsibilities
Fitting cancer treatment around caring responsibilities was identified as a challenge, practically and emotionally, for patients in both more deprived and rural and island areas. Staff discussed that it was difficult for patients to make care arrangements so that they could travel for treatment. A staff member from a rural and island area was not aware of anyone completely refusing treatment for this reason, but thought it was a factor in some patients’ decisions - for example, in choosing surveillance over treatment, or treatments that require less time away from home.
"I think sometimes if we might have a choice between a treatment that requires an overnight stay or something… if you've got an older couple where one person has dementia and the other one's having cancer treatment, then yeah, it can affect people's choices." - Staff, rural and island area
A staff member from a more deprived area similarly felt that patients sometimes prioritised their caring responsibilities over their own cancer treatment.
“I think very much sometimes the cancer is not always their main issue that's going on in their lives. They may have other problems as well. They are the main carer for another person, whether it be a child or whether it be another member of their family. And they don't tend to put themselves first, they'll put the person that they're caring for as the primary sort of goal of support at a detriment to themselves.” - Staff, more deprived area
Difficulties in arranging relatives’ care were also raised in patient interviews. For example, a patient who was a full-time carer for their spouse had to pay for a private nursing home while away for radiotherapy, as they were unable to find respite care. Leaving loved ones for extended periods of time was also highlighted as being emotionally difficult for patients. A staff member highlighted the importance of realistic medicine in these circumstances, to ensure the person’s individual circumstances were considered in treatment decisions.
Housing
Some patients also faced challenges with housing while undergoing cancer treatment – in some cases, because they did not have a permanent address. Staff from a more deprived area shared an example of a patient who was living in temporary accommodation where they did not feel safe leaving their belongings, meaning they could not pick up their full nutritional supplements prescription.
“They didn't feel safe leaving their suitcase in the temporary accommodation, so whenever they went anywhere, they had to take their whole suitcase with their belongings on the bus. I couldn't then give them the supplements on prescription because they wouldn't have been able to carry it and would have had to have then carted that with them every time they went anywhere else as well. So, you know, all these kinds of barriers that you just wouldn't ever imagine." - Staff, more deprived area
Other patients struggled because their cancer symptoms or treatment side effects meant that their living situation was no longer suitable for them. For example, patients sometimes struggled with stairs. In these instances, staff referred them to occupational therapy for support. In one of the more deprived areas, ICJ were able to facilitate quicker access to occupational therapy and housing adaptations due to their links with the local authority.
Overcoming financial challenges
Support with claiming benefits
The main way in which staff felt they could help patients financially, was to make sure they were in receipt of all the benefits they were entitled to. This involved referring patients for benefits assessments and advice, and helping them to complete benefits applications. Patients tended to be referred for this support by CNSs and ICJ staff (who also helped with applications themselves sometimes). Organisations that provided the help included Macmillan, Maggie’s Centres, Citizens Advice Bureau, and other local patient information and support services. In one of the rural and island areas, Macmillan had a partnership with the Citizens Advice Bureau. The team was based within a hospital and was highlighted by staff and patients as being a “fantastic” source of support.
Patients from various case study areas shared experiences of receiving support to help apply for ADP, Universal Credit, and Pension Age Disability Payment, which had made a significant difference in some cases. For example, one patient from a rural and island area who received help with filling out ADP application forms, said it had relieved financial pressure.
"Well, I'm not struggling now. I was struggling to have enough money to pay all the bills like council tax and rent and things like that. And now, although I'm not rich by any stretch of the imagination… I'm not sort of scraping the bottom of my bank account at the end of each month." - Patient, rural and island area
ICJ staff highlighted that they were limited in what they could do to help those who were already not working and/or were already in receipt of ADP, as a cancer diagnosis did not lead to an ADP increase. Furthermore, a staff member noted that there were actually fewer financial benefits available for patients with curable cancer than for those with incurable cancer who were eligible for benefits that were not means tested.
Barriers to accessing benefits
Despite the support provided with applications, some patients in difficult financial circumstances had their applications rejected – several times, in some cases. They expressed feeling let down by Social Security Scotland, and discussed the stress of appealing their cases.
"The only thing I feel has made it harder for me is [lack of] help financially. That is the only thing I feel that I've been let down with. Other than that I think that the nurses and everything else and ICJ… I feel that they were a great help… yet with Social Security Scotland and the ADP I really feel let down there." - Patient, more deprived area
It took several months for some patients to hear the outcome of their benefits applications, and even when they were accepted, that was followed by a difficult waiting period for the benefits to come through. A support organisation in one area noted that they were “whitelisted” with Social Security Scotland which meant they had escalation routes, facilitating quicker benefit application processes and answers to queries.
Referral to ICJ
ICJ teams across the case study areas were generally felt to have had a positive impact for patients that they had supported. Staff conducted HNAs with patients and linked them to financial and practical support where needed, along with providing some emotional support (see Chapter 7). However, staff expressed that they were not reaching everyone in need. The referral process into ICJ differed across case study areas (see Chapter 1 for more on this), which staff felt impacted the extent to which they reached patients who would benefit from support.
ICJ staff in one rural and island area where they proactively reached out (over the phone) to patients with a diagnosis, thought this helped them reach patients who would not seek support themselves. This ICJ team also followed up with patients after twelve weeks to find out if they needed further support.
“The ICJ, I think, has been a Godsend to a lot of people because a lot of people will not walk in and ask for help. We are being proactive and reaching out to them. So I think that makes a difference.” - Staff, rural and island area
The health board had a Cancer Tracker staff member who was responsible for tracking all patients with certain types of cancer that are routinely tracked in a database. Once a month, the ICJ team received a spreadsheet of everyone in the area with a diagnosis of a tracked cancer. However, some cancer types were not tracked, and so staff thought it was likely that some patients were being missed.
By contrast, in other areas, the responsibility lay with individual clinicians to refer patients into ICJ, or for patients to self-refer. ICJ staff expressed concern that some patients who could benefit from their support were not being referred. They discussed that clinicians may get a false impression of a patient’s circumstances, as people often put on appearances for medical appointments and did not necessarily share information about their wider circumstances.
"I think we need to be all singing from the same hymn book. ICJ is in the Cancer Strategy and, as such, we should be a part of what every nurse is offering to patients in terms of support. There shouldn't be any gatekeeping about when a patient needs to be referred. Everybody should be referred at some point and if the nurse is unsure of that, of whether that person's [already] been referred, refer them again and again and again… It's up to the person whether they take it up or not. - Staff, more deprived area
There was an identified need for greater cohesion and collaboration between different services in several case study areas, and improved advertising of ICJ to patients. ICJ staff noted that some GPs and CNSs were still unaware of the service, and that greater communication of the service was required. Staff in one area mentioned that they specifically had lower engagement from people from more deprived areas, and struggled to engage minority ethnic patients (which they thought could partly be due to cultural barriers in relation to accepting help).
Some case study areas had tested a blanket referral system which staff felt had worked well. In one area, it used to be that everyone who got a cancer diagnosis received a letter informing them of the ICJ service, and another reminder letter six weeks later. Staff highlighted that it was useful for patients to have a physical information sheet about the service that they could refer back to. However, the letters were stopped, which staff believed was due to cost-saving measures. Another health board had carried out a test of change whereby ICJ received blanket referrals from staff for patients in one pathway. This worked well and staff mentioned plans to roll this out across additional pathways.
Recommendation 13: In line with the People Principle in Scotland’s Health & Social Care Service Renewal Framework[9], improve awareness among healthcare staff, such as GPs and CNSs, and referral processes for support services for patients, including ICJ.
The time of signposting or referral to ICJ was identified by staff as being an important factor in levels of uptake. There was a view that overwhelm at the point of diagnosis was a barrier to some patients taking up support at that stage, and that it was also too early for some patients to realise that they may benefit from support. In areas where all new patients used to be sent letters about ICJ, staff reported that there was not a massive uptake immediately after diagnosis, but that they noticed more uptake after prompting people six weeks later. A staff member from a different area similarly reported that some people sought support much later down the line, up to a year after their diagnosis.
Motivational barriers to accessing financial support
Some patients also faced motivational barriers in asking for, or accepting, financial support. Staff noted that some had the attitude of ‘don’t bother the doctor/nurse’, or were embarrassed to share that they were struggling financially. It was also evident from patient interviews that, despite significant financial struggles, some patients felt they were not deserving of support. For example, a patient from a more deprived area did not accept a grant from Macmillan because they thought that other people were worse off than them. This was despite them describing travel as having had a “terrible” financial impact as they had to keep borrowing money to pay for taxis.
“There’s people a lot worse off than me, with the state of the country just now, so they need that more than me.” - Patient, more deprived area
A different patient, from a rural and island area, did not claim back the £1,800 that they spent on travel and hotels because they explained they would have ‘felt bad’ about doing so and were just grateful to have received free treatment.
Proactive offers of support and encouragement to accept help
A facilitator in patients accessing support with financial and practical issues, was the support being proactively offered to them, by clinicians or ICJ. In some cases, staff felt this helped overcome motivational barriers in terms of patients feeling embarrassed to ask for help, or that they did not deserve it. Some patients interviewed shared a similar perspective, discussing that they probably would not have known about available support, and would not have asked for it, if they were not directly made aware of it or encouraged to take it up. Likewise, some patients who had not accessed any financial support felt they would have been more likely to take it if it was directly offered to them.
Availability of financial support
Staff who were proactive in arranging financial support for patients (e.g. ICJ staff and CNSs) highlighted the lack of available options. Previously, a Macmillan grant was available and was considered by staff to have helped many of their patients. It was a one off payment, typically of around £200 - £350 for people who met specific financial criteria (low income, and savings of under £1,000) and could be used for anything, such as food and heating bills. However, the grant was stopped as of April 2025, to much frustration among staff.
“Macmillan used to offer a grant as well… you could get that money and that was yours to do whatever you wanted with, which was a really good resource. During COVID times it was increased… which again was a lifeline for so many patients who were struggling financially. That’s completely pulled.” - Staff, rural and island area
Regardless, the eligibility criteria to access the grant had been a barrier for some patients. For example, a patient shared that she had not been eligible due to the amount of savings she had, but she had now used them up and was worrying about paying bills. However, patients (from both more deprived and rural and island areas) who had received the grant before it was cut, described how it had helped them cope with expenses including travel costs; electricity costs; keeping afloat until universal credit payments were received; electric blankets, and pyjamas to take into hospital. While the grant had not covered all of these costs for patients, it had helped at a difficult time.
Other avenues for financial support included Scottish Welfare Fund grants, but staff noted that this had very strict eligibility criteria.
“We do explore all areas and look at kind of grants and things, but these are becoming less accessible as well now.” - Staff, more deprived area
Staff in one rural and island area noted that there were small third sector grants available, and a support centre funded by a charity in another area had started its own £250 grant when the Macmillan one ended.
In terms of heating costs, ICJ referred patients to Home Energy Scotland for small grants or energy advice, and made sure patients had already accessed support available through their housing association, where relevant. However, this support consisted mostly of advice and very small grants. Staff noted that there was even less that could be done for private renters. Some patients who owned their homes reflected on the importance of them having had critical illness insurance, which helped them pay their mortgage and cope financially. However, this was not widely discussed, suggesting that not all patients had this insurance.
Staff also linked patients up with other third sector support services that provided help for those in difficult financial situations, such as food banks. However, stigma around accessing these services remained a barrier for some. For example, one patient described how, when offered a referral to a food bank, they had put the phone down because they were so offended.
"I wouldn't have went. I would never have went to a food bank. Never, never, ever would I have went...I shouldn't have to.” - Patient, more deprived area
ICJ staff also noted that, although they could make outward referrals to support patients, they were reliant on other services following through and providing the support.
“Once the referrals are made, it's not my job to make a decision on whether they get something. So, for example, I could refer into transport services and that, but they could decline. You know, the benefits team, they could say, ‘well, actually, no, you're not entitled to this, we can't make this application for you’. I could say to people, ‘I'm going to refer you for this, that, and the next thing’ but ultimately it's up to the person that I refer to or the service to decide what's going to happen." - Staff, more deprived area
Recommendation 14: In line with the People Principle in Scotland’s Health & Social Care Service Renewal Framework[9], increase and promote financial support for patients who need it to help with costs incurred (e.g. travel, accommodation, heating) and to cover loss of earnings. Facilitate prompt receipt of available support. Minimise need for patients to pay in advance if they cannot afford to. Raise awareness of critical illness cover among the general population to help cover relevant costs.
Figure 6.1 illustrates a patient’s experience of financial and practical issues. It shows key aspects of their journey and how these relate to the dimensions of the COM-B model of behaviour change.
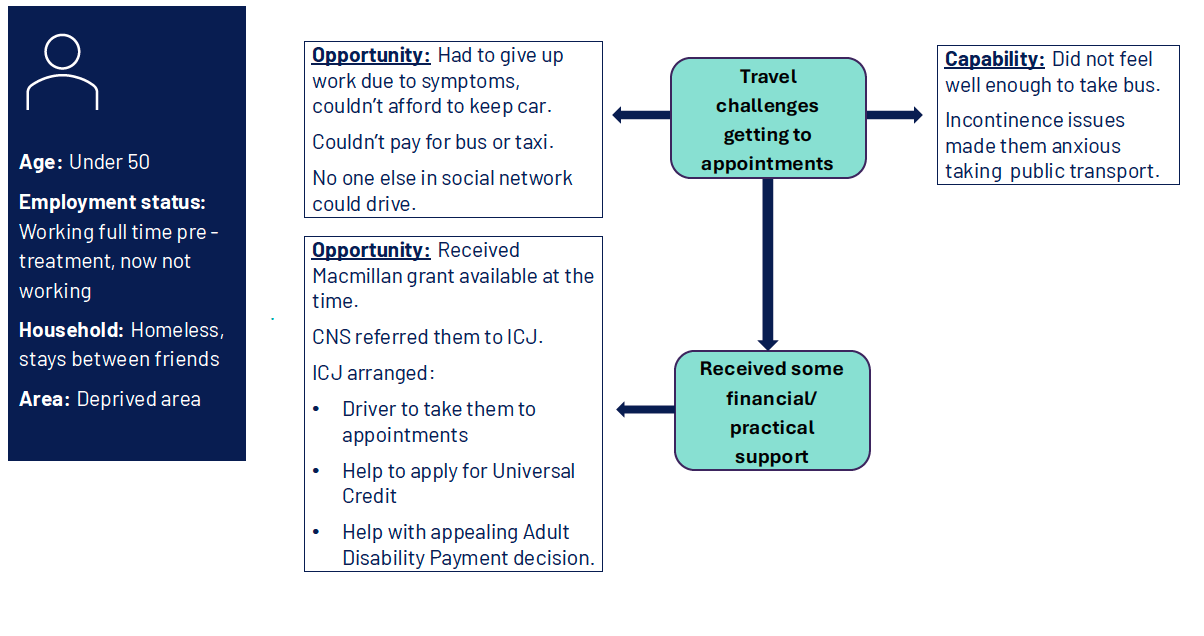
Diagram showing two stages of a patient’s journey and relevant COM-B dimensions
Patient characteristics
- Age: Under 50
- Employment status: Working full time pre-treatment, now not working
- Household: Homeless, stays between friends
- Area: Deprived area
Stage 1: Travel challenges getting to appointments
- Opportunity: Had to give up work due to symptoms, couldn't afford to keep car. Couldn't pay for bus or taxi. No one else in social network could drive.
- Capability: Did not feel well enough to take bus. Incontinence issues made them anxious taking public transport.
Stage 2: Received some financial/practical support
- Opportunity: Received Macmillan grant available at the time. Clinical nurse specialist referred them to Improving the Cancer Journey. Improving the Cancer Journey arranged:
- Driver to take them to appointments
- help to apply for Universal Credit
- help with appealing Adult Disability Payment decision.
Contact
Email: socialresearch@gov.scot