Scotland's cancer strategy: services and support evaluation
Findings from an evaluation of cancer treatment services and support in Scotland. Specifically it looks at experiences of patient access and engagement with cancer treatment and support in rural and island areas, and in areas with higher deprivation.
Chapter 7. Physical and mental health and emotional wellbeing – evaluation findings
This chapter firstly explores how physical and mental health and emotional wellbeing challenges hindered timely access to, and effective engagement with, cancer treatment services. It then covers factors that helped patients to cope with cancer both physically and mentally.
Key findings
- Comorbidities and later presentation were more common in more deprived areas with patients experiencing treatment delays while other conditions were addressed first. Staff had experienced patients in more deprived areas being less likely to seek help for side effects, because they were accustomed to living in poorer health or did not want to bother staff.
- The mental health impact of cancer treatment was evident across interviews and was heightened for those with pre‑existing mental health conditions.
- Support from family and friends was crucial to patient experience. Strong support networks were linked by staff to quicker recovery from treatment. Staff reported doing more to support patients who did not have a support network. Peer support was valued by some patients as helping them to cope during treatment, though others found support groups to be ‘too negative’ or ‘too daunting’ to attend.
- Access to prehabilitation and rehabilitation varied. Some areas had a more structured approach to prehabilitation than others. There was a general sense that there was a lack of resources for this in rural and island areas.
- Where in place, CNSs and SPoC staff (in some areas) provided ongoing clinical and low‑level emotional support and signposted to wider services (such as ICJ, Maggie’s Centres or local third sector organisations). However, referral processes varied, raising concerns that some patients missed out on wider support. There were particular barriers in accessing clinical psychology services due to long waiting lists, and a gap in support for patients post-treatment.
- Factors that encouraged take-up of support services included repeated offers from trusted individuals at various points in the journey, offering individual appointments, and increasing outreach.
Impact of comorbidities on experiences of treatment
As noted in the rapid evidence review, it is well known that late diagnosis and presence of comorbidities impact treatment options and outcomes and that this particularly affects patients in the most deprived areas of Scotland. This experience was echoed by staff and patients in this evaluation.
Staff in more deprived areas explained that it can take longer to start cancer treatment if another condition needs to be addressed first, and that delays are compounded if a patient has multiple conditions that require coordinated input from a number of specialists. A patient with chronic obstructive pulmonary disease described how it took several months to determine whether they could have surgery, during which time they became very worried that the cancer had spread. Staff further noted that they had seen treatment delays in cases where a patient with dementia was unable to confirm their own identity and their carer did not have any identification documentation or paperwork with them either.
Another issue was delayed care for the side effects of treatment. As noted in Chapter 4, staff found that patients in more deprived areas with comorbidities were less likely to seek help for side effects because they were accustomed to living in poorer health and may not recognise when to seek help or know how to do so.
Staff also commented that some patients in more deprived areas were reluctant to seek help because they felt staff were already very busy.
“We sometimes have people sitting at home going, ‘well, you know, I didn't think it was worth phoning’ or ‘I didn't want to be a bother Doctor, you're all very, very busy.’ - Staff, more deprived area
Some areas have a helpline for patients to contact about urgent cancer treatment side effects. However, staff in more deprived areas noted that patients can find it difficult to describe their symptoms over the phone and that it is expensive to wait on the phone which is a barrier for patients on low incomes.
While the emotional impact of treatment was a theme across interviews, patients with existing mental health conditions described a particularly strong impact on their mental health. For example, a patient said that chemotherapy had reduced the effectiveness of their antidepressants and sleeping tablets and that the GP was not able to give them a stronger prescription. This contributed to a mental health crisis which they felt unable to seek treatment for because they were afraid that their cancer treatment would be stopped. Another patient described how they felt increased anxiety each time there was a change in their treatment. They were not aware that they could reach out to their CNS for support and would have liked them to have periodically checked in about how they were coping.
Staff further noted that some patients with existing mental health conditions could find it more difficult to attend appointments and were less likely to tell family about their diagnosis in order that they can provide emotional support.
“What I do find as well, obviously not generalising for everyone, but people who have had previous mental health conditions or live with poor mental health often, I feel like, I've had people that have not even told their family that they have a cancer diagnosis. They're hiding, you know […] [I had a patient who] didn't want his family to know that he had cancer so then the emotional support wasn't there because they didn't know what was happening.” - Staff, more deprived area
Staff had also experienced that patients with problematic substance use struggle to abstain in order to be able to have treatment. A doctor in a more deprived area who reported that their team provided a great deal of support to patients said they would phone patients the day before a test to ask them to stop drinking, for example. Substance use among family members could also influence patient decisions. A patient said they had refused to take strong painkillers during their recovery from surgery as a family member had experienced drug dependency.
For patients with existing physical health conditions, travel to appointments was also more difficult (which has been explored in more detail in Chapter 5 above).
Coping with cancer treatment
Key aspects of their treatment journey that patients found more difficult included: taking in the amount of initial information provided, waiting for treatment to begin, travel to and from appointments, and recovery post-treatment, particularly where patients were worried about recurrence. Staff had found that patients without a support network or who had recently been bereaved, and patients with young children tended to struggle more in their journey. Several factors had helped patients to cope which are explored further in this section.
Support from medical professionals
Experience of early appointments had made a difference to patient outlook. Some patients described feeling more positive about their journey after being provided with more information or reassurance about the care they would receive.
“She [the consultant] put our minds at ease by saying ‘I'm not letting you go yet. We are going to keep you here for a good while longer’, which was very reassuring for my partner sitting listening to it and, you know, it kind of perks you up yourself.” - Patient, rural and island area
In some areas, CNSs and SPoC staff were a key source of ongoing clinical and low-level emotional support for patients during their journey. They would also refer patients to wider support services (see section on wider support services below). Some staff have the capacity to proactively check in with patients which they appreciated. However, there was a perception among some patients that CNSs were very busy, so they were reluctant to contact them.
“I remember the day she [support worker] phoned, I don't know if it was just the relief of somebody who you felt you could offload to a wee bit, but she was really, really good. They [CNS team] were really quite good throughout. I didn't have a lot of engagement with them after my surgery, probably because I didn't feel like I needed it because I was quite fit and active, which led to quite a quick recovery. And I think in the back of my mind, knowing the high number of cases of cancer patients that are with way more issues than I felt I had, I was kind of reluctant to contact them too much. But that's not to say I didn't feel I could contact them." - Patient, rural and island area
Staff in rural and island areas noted that there was a perception that Macmillan CNSs were only for patients receiving palliative care which was a barrier to taking up support. However, they felt that this perception was changing due to word of mouth with patients sharing positive experiences, advertising of their service and because they now have a more advanced and expanded role in clinical settings and in the community. In a more deprived area, there was a related concern that Macmillan branding on the ICJ service was a barrier for the same reasons, with some patients thinking that staff were calling to ask for a donation (ICJ is discussed further below in the section on wider support services).
Support network
Support from family and friends was a key facilitator to the take-up of treatment, and for helping patients cope with treatment. Strong community connections was a theme in both rural and island and more deprived areas.
Family and friends would help patients during their journey by providing emotional support; driving patients to appointments; helping patients understand their treatment or encouraging them to attend appointments; and helping with household tasks such as shopping and cooking. However, as noted in Chapter 5, it was not always possible for a patient’s support network to provide this type of support if they received treatment away from home. Some patients also had family members with a medical background who had helped them to research treatment options or who had provided reassurance that they would help with complications if needed.
Support from family and friends was important throughout a patient’s cancer journey, but particularly in the mid to late stages of a treatment cycle, when patients feel more physical and mental effects. During treatment some patients in rural and island areas have to spend weeks at a time away from home and their support network. This was a difficult time and staff would try to signpost to local support services for some support.
Some patients said they had felt guilty relying on family and friends or did not want to burden them. This tended to be older patients living in rural and island areas who needed help to travel to appointments or collect prescriptions, and women who were used to caring for others.
Staff had experienced that patients without a support network struggle more to care for themselves and, at the same time, that patients with a strong support network tend to recover more quickly. While staff reported a lack of social care resource contributing to delayed discharge from hospital, a lack of a support network was also a factor. Where patients did not have a support network, or did not take up offers of wider support (explored further below in the section about wider support services), staff said they would do more to support them by checking in more regularly.
Patients particularly valued the support from people who had lived experience of cancer. This might be from family and friends, informal conversations with other patients or a peer support group. Patients described how hearing from other people had helped them realise that it was possible to live with cancer or that they gained a different perspective when they heard from people they perceived as dealing with a more serious condition.
Patients in rural areas who had been diagnosed through a screening programme reflected that they regularly met the same people in clinical settings. This helped them to provide informal emotional support to each other, as well as offer practical advice e.g. on what to bring to feel more comfortable during treatment. Staff and patients noted that medical professionals may not be aware of or think to highlight these practical things. At the same time, some patients had experienced ‘survivor guilt’ when friends they had made had died.
There were barriers to take-up of more formal peer support groups (i.e. organised through a third sector organisation). While some patients had had a very positive experience, others felt that support groups were too negative or that it was too difficult to go to a setting with strangers when they were feeling unwell. To help address this, in some areas SPoC staff offered to attend support groups with a patient for the first time. Some patients had also benefited from support groups after treatment when they felt more able to talk about their experiences. Staff in rural and island areas reflected that patients diagnosed with rarer cancers were less likely to have the opportunity to benefit from this type of peer support where there are fewer people with the same diagnosis.
Prehabilitation and rehabilitation
Staff across case study areas acknowledged the importance of prehabilitation and rehabilitation to patient outcomes.
Staff said they would make patients aware of the importance of exercise and cutting down smoking and drinking, and encourage early take-up of support services. However, awareness of support available was felt to vary among staff and some areas had more structured pathways for prehabilitation than others (see Chapter 2).
While not specific to supporting patients in rural and island and more deprived areas, a staff member who had had cancer themselves highlighted how it can be difficult to approach conversations about prehabilitation in the early stages when patients are coming to terms with their diagnosis.
“Just from my own experience of having cancer myself, I think I would have been totally outraged if anybody had offered me prehab, because your world is upside down and the last thing you want at that point is somebody telling you to exercise and to eat properly and stuff like that, you know. So whilst I totally, as a professional, really accept the value of it, personally, I think that's probably a big hindrance.” - Staff, rural and island area
This perception of the relative importance of prehabilitation compared to anti-cancer treatment is discussed earlier in Chapter 5 in relation to distance to support.
In another area, staff described how prehabilitation was built into the cancer pathway and all the health professionals would emphasise its importance, which helped encourage patients to take it up.
“The reason that works is because you make that part of the cancer treatment pathway so patients accept that it’s in their best interest. It's part of the process, it's part of the treatment. It's not a cherry on a cake. where, you know, ‘that's great, you did it thanks very much’. It’s ‘this will actually make a difference here's how this fits in and this is our plan for you’. You know, it's like saying you're going to get surgery, you're going to get this and then this follows on.” - Staff, more deprived area
Patients more commonly reported having been offered rehabilitation support after treatment. This included referrals to physiotherapy, occupational therapy, dietetics, audiology and clinical psychology. Support offered depended on the pathway and treatment received. Patients who had had surgery were particularly positive about the difference physiotherapy had made to their recovery, with some also reflecting that they valued having another professional to provide low-level emotional support.
“I remember what [the physio] tells me, the words, I'm not fighting this thing, I'm dealing with it. 'You're an inspiration'. He just uses the right keywords. He knows his stuff and he'll remind me how poorly I was at the beginning and how far I've came. He's very, very good" - Patient, rural and island area
However, as noted, in Chapter 2, there was a general lack of prehabilitation and rehabilitation services, particularly for patients in rural and island areas. Staff also reflected that it is easier and more affordable for patients in more affluent areas to access gyms and personal trainers to help with their recovery.
Wider support services
There were wider support services that could help patients cope during treatment. These included ICJ, Maggie’s Centres, and local third sector organisations (see case study areas - key characteristics). Patients used services at different times depending on their needs and when they were made aware of what was available. This section explores barriers and enablers to take-up of this wider support.
Availability and accessibility
Lack of service capacity and long waiting lists were a barrier. There were particular issues with a lack of clinical psychology support, which was mentioned as a barrier across case study areas.
A lack of counselling services was also a barrier in some areas. Some patients had benefited from BUPA talking therapy sessions offered via Macmillan. However, this was no longer available due to funding pressures. This resource was reported to have been particularly valuable for patients in rural and island areas who did not have in-person support nearby. The closure of Cancer Support Scotland, which had provided mental health and wellbeing support for patients, had also contributed to a reduction in services.
Maggie’s centres offer a range of support services, which patients had found beneficial. However, travel was a barrier for patients in rural and island areas and more deprived areas, in terms of both cost and distance. Staff suggested there was a perception that patients who live relatively close to large urban areas could easily travel to support centres, which was not always the case, due to the travel challenges described earlier in Chapter 5 in relation to journeys for patients in more deprived areas.
While there were online resources and support groups, some patients felt more comfortable discussing their experiences in person or were not computer literate. Other access barriers included timing of support groups not being suitable for patients working office hours.
To help improve accessibility, there were some calls from staff for more local support options. Some services had recently made efforts in this area. For example, in one more deprived area, staff had visited a local community centre which allowed them to reach individuals they might not otherwise have done.
“I went I was out of this community centre and there was, like, 30 men in this room playing darts and snooker and I thought ‘Ah, this is actually what I need to be doing. […] Not going to do a talk, but literally just sitting there.” - Staff, more deprived area
A lack of post-treatment support was a common theme for patients in both more deprived and rural and island areas. A patient described how she felt abandoned after her treatment finished and began to struggle with anxiety about the possibility of her cancer coming back. She used an analogy of being on a bus during treatment, with the conductor being medical staff taking her to where she needed to go, and then being suddenly dropped off the bus when she was finished.
Another patient highlighted a specific gap in clinical psychology support for patients who are waiting for breast reconstruction surgery post-surgical treatment.
"In order to have reconstruction you have to see the psychologist, but to be told you're not getting reconstruction, you don't. Which I could not fathom the logic for because you're still having the surgery to remove the breasts, you're still going to be left with all this horrific scarring and all the body image issues, but there's no support there, which I found really, really bad." - Patient, rural and island area
ICJ staff said that they continue to support patients who get back in touch with them post treatment.
Awareness
CNSs and SPoC staff played a key role in making sure patients were aware of wider support services, by signposting or making referrals. GPs were also involved in making referrals to clinical psychologists. As discussed in Chapter 6, there were concerns that patients miss out on support because of a lack of staff awareness or because they do not think to refer patients. This was a particular issue for ICJ.
In a more deprived area, a key gap in support was identified for patients who were diagnosed via emergency surgery. A staff member described how, in their pathway, these patients do not have access to a CNS or SPoC staff who can ensure patients are aware of support and coordinate referrals. These patients tended not to be seen again by the oncology team until they had recovered from surgery and had been referred for further treatment.
Recommendation 15: In line with the People and Prevention Principles in Scotland’s Health & Social Care Service Renewal Framework9, improve access to and availability of both emotional and psychological support, particularly after treatment. If there is a member of staff responsible for their care (Recommendation 8), they could determine whether a patient requires support after treatment and make the referral. Consider whether new or improved processes are needed to connect patients diagnosed via emergency surgery to the relevant cancer pathway.
Encouraging use of wider support services
Even where support was available and offered, participants did not always take it up. Some felt they already had enough help from family, friends or clinical teams, or were comforted by their faith. Others believed that support should go to people with what they perceived to be ‘greater need’. For example, a patient felt that they did not need support as they had only had surgery whereas others would have had radiotherapy or chemotherapy.
Other barriers included a perception that support groups catered more for older people, and that patients did not feel comfortable attending on their own (as noted above in relation to the support network). A patient whose memory had been affected by treatment said that he was cautious about seeking support too, because he is likely to forget about appointments, and does not want to waste staff time. Further, where ICJ operates via the local authority, emails coming from a council address was a barrier for patients who had previously had a negative relationship with the local authority.
Staff and patients described the importance of re‑introducing offers of support at various points, as needs may have changed, and encouraging take-up. Staff observed that older adults and men, in particular, could see accepting help as a weakness, although they felt this attitude was shifting. Staff observed that uptake had improved when they emphasised that taking support was part of looking after oneself during treatment, not a sign of failure, and where reassurance came from trusted clinicians or peers with a similar background.
In areas with higher deprivation, staff recommended increased outreach from support services such as Maggie’s centres to help counter a perception that activities are more for the middle class. While hospices can offer counselling services or respite for carers, there was a perception that services were only for patients at the point of end-of-life care. Again, some staff felt that more outreach and advertising could help encourage use of these services.
In rural and island communities, some participants worried about being seen at a local group or encountering someone they knew, despite reassurances about confidentiality.
“Because I live in a rural area, there's more chance that you're going to know of people's experiences. And I felt the desire to not be seen as an invalid or somebody who was complaining. So I think I was a wee bit self-conscious.” - Patient, rural and island area
Services that offered individual appointment slots reported engaging a broader mix of patients, who would not otherwise have attended a group setting. One setting had continued offering one-to-one appointments after seeing increased engagement during the pandemic.
"It was May 2022 before we could reopen our doors to a drop-in service so what we kind of realised from our figures and everything and our engagement during that period of time was that the diversity of people who were engaging was huge, bigger than we’d ever seen before […] people in the community who would probably never have come in if you hadn't guaranteed them that private appointment.” - Staff, rural and island area
Figure 7.1 illustrates a patient’s experience of physical and mental health and practical issues. It shows key aspects of their journey and how these relate to the dimensions of the COM-B model of behaviour change.
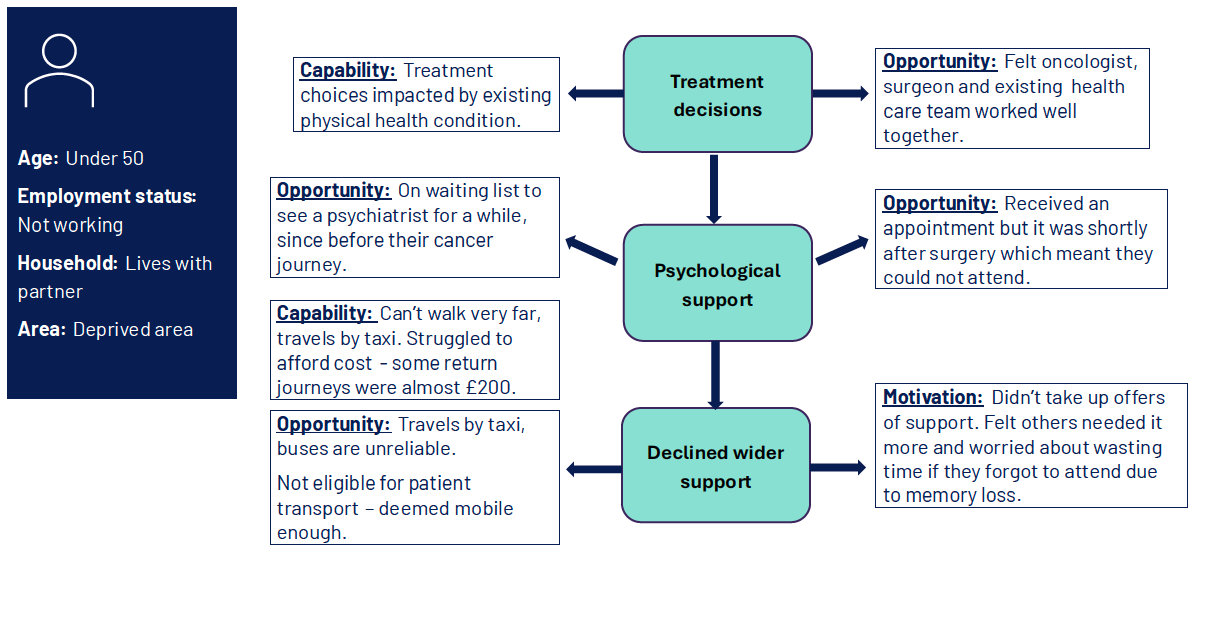
Diagram showing three stages of a patient’s journey and relevant COM-B dimensions
Patient characteristics
- Age: Under 50
- Employment status: Not working
- Household: Lives with partner
- Area: Deprived area
Stage 1: Treatment decisions
- Capability: Treatment choices impacted by existing physical health condition.
- Opportunity: Felt oncologist, surgeon and existing health care team worked well together.
Stage 2: Psychological support
- Opportunity: On waiting list to see a psychiatrist for a while, since before their cancer journey.
- Opportunity: Received an appointment but it was shortly after surgery which meant they could not attend.
Stage 3: Declined wider support
- Capability: Can’t walk very far, travels by taxi. Struggled to afford cost - some return journeys were almost £200.
- Opportunity: Travels by taxi, buses are unreliable. Not eligible for patient transport - deemed mobile enough.
- Motivation: Didn’t take up offers of support. Felt others needed it more and worried about wasting time if they forgot to attend due to memory loss.
Contact
Email: socialresearch@gov.scot