Scotland's cancer strategy: services and support evaluation
Findings from an evaluation of cancer treatment services and support in Scotland. Specifically it looks at experiences of patient access and engagement with cancer treatment and support in rural and island areas, and in areas with higher deprivation.
Chapter 4. Information provision and shared decision-making – evaluation findings
This chapter explores how information provision and shared decision-making impacts on patient experience of accessing and engaging with clinical cancer treatment. The Cancer Strategy has a focus on the use of a realistic medicine approach, key elements of which are patients feeling empowered to have a say in decisions about their treatment, and such decisions reflecting their holistic needs. This chapter focuses on the extent to which patients felt they received accessible information on their diagnosis and treatment and the extent to which both patients and staff felt they were able to reach shared decisions about treatment, including the facilitators and challenges to doing so.
Key findings
- Patients typically described feeling that they did have a say in their treatment. Accessible information was central to this. Patients valued a combination of clear verbal explanations tailored to their circumstances and written materials they could revisit and share with family.
- Having a family member or friend present supported recall and capacity to ask questions, though lack of funding for escorts for patients from rural and island areas could limit the opportunity for this.
- Patients were generally positive about the accessibility of the information provided. However, patients in more deprived areas more commonly described challenges in understanding medical terminology. CNSs and SPoC staff (in some areas) played a key role in patient understanding.
- Some patients wanted more information on what to expect during treatment, particularly the likelihood of potential side effects. Due to perceived gaps in the information provided, some patients felt alarmed by reactions to treatment or felt unsure about when to seek help for the side effects of medication.
- Challenges to shared decision-making included limited staff tools/training for complex conversations and time pressure in busy clinics. Staff reported that patients in more deprived areas tended to defer more to clinicians and were less likely to question their options.
Information provision
Accessible information provision is the first step in facilitating shared decisions about treatment. The extent to which patients were able to understand the information provided on their diagnoses and treatment options, and their experiences of receiving it, was affected by a number of factors, discussed in the remainder of this section.
Format of information
Information about patients’ diagnoses and treatment options was typically provided at consultations with clinicians. In some cases, patients were also provided with written information in the form of leaflets, letters or links to online resources. While there were individual preferences for one format or another, on the whole, patients appreciated the combination of both verbal and written information. Verbal information from clinicians was helpful in that it was specific to their individual circumstances and allowed them to ask questions and clarify understanding while written information enabled them to digest it in their own time and provided something to share with family or friends who had questions.
"I think it needs to be a combination of different things because everybody's uptake of information is different. So, some people are more receptive to verbal communication, other people understand things better when it's written down. So, I think just making sure that, when we're providing communication on potential treatments, it comes in various formats." - Staff, more deprived area
“Well, on paper, that's where I could look over it myself at any time. And then if any of the family were asking, you know, so it was there that I could explain it to them as well, or they could read it themselves." - Patient, rural and island area
This was particularly important as patients often reported feeling overwhelmed in consultations and being ‘unable to take anything in’.
"It's the enormity of your diagnosis that might blur what you actually take in and what you don't take in." - Patient, rural and island area
Staff noted variation in the extent to which written information was provided to patients, specifically that there were more and better-quality resources available for more common cancers than for rarer ones that had more complex pathways.
In addition to consultations and written information, there were also reports of staff offering information to patients in alternative ways, which could help to ease their worries. For example, in a rural and island area, staff reported offering to walk patients around the chemotherapy department in the hospital in advance of their treatment.
The presence of a family member or friend at appointments
As noted above in relation to the format of information, patients reported finding it difficult to take in information during appointments. Having a family member or friend present at appointments was considered helpful in facilitating information recall or to help encourage them to ask questions.
“Again, this is why for me, having my husband come with me to all of those appointments, so there were two of us listening, was really important because I think if you were there on your own, or even if you're older, where you rely on something being written and sent to you, perhaps a little more quickly, it might be more difficult because when you're being told so much information at once, you don't absorb all of it, especially when it's quite tough information.” - Patient, rural and island area
While there were generally no barriers to patients bringing someone with them to appointments, the lack of funding for escorts to accompany patients travelling from rural and island areas (see Chapter 5) was prohibitive for some patients. The provision of video consultations could help in some cases (see Chapter 2).
Medical terminology and accessibility
The use of plain English supported patient understanding of their diagnosis and treatment options. On the whole, patients were positive about the accessibility of the information provided.
“It wasn't cloaked in doctor's talk, if you know what I mean. It was in plain language so that you could absorb what they were trying to tell you." - Patient, rural and island area
However, the use of complex medical terminology as a barrier to understanding was raised more by patients living in more deprived areas.
"Dealing with cancer is hard enough, but with words and stuff you can't even pronounce, that just adds to the stress because… you don't actually understand.” - Patient, more deprived area
"And I just think sometimes the doctors have got the assumption that everybody's medical savvy and they forget to put it in plain language." - Patient, more deprived area
One patient in a deprived area described asking her clinician to clarify some of the language in leaflets she had received and them taking the time to write down what each word meant. She found this very helpful and suggested that the leaflets should be more simply worded in the first place.
Staff also discussed their experiences of supporting patient understanding. They were keen to stress the importance of not making assumptions about patients’ ability based on the area in which they lived and that the most important thing is to tailor information to individual patient needs.
"…not everybody living in a deprived area […] has issues that are related to education or something like that. Sometimes it's just that's where they've ended up because of the circumstances. So, I think to blanketly say that everybody living in a deprived area of [city] doesn't have the ability to comprehend or understand [is not correct]. So, I think, what we need to be sure of is that we are tailoring the information that we give or the advice that we give out, or the access to support to meet everyone's needs."- Staff, more deprived area
It was recognised that information leaflets were sometimes long and contained terminology that was not accessible to all patients. Staff described balancing the challenges of ensuring patients had full details of planned treatment, in order to provide their informed consent, and the time pressures that could preclude staff from being able to go over the information with patients and confirm their full understanding. One staff member noted variation in the length of appointments by cancer type. In her experience, patients with more common lung cancers typically received shorter appointments than those with rarer types due to resource issues.
While there were easy read versions of some materials available, these were felt to be more suited to patients with additional learning needs, and not appropriate for all patients. A staff member also noted that patients did not always admit that they were unable to read, making it difficult for staff to judge their level of understanding.
Examples of ways in which staff were trying to overcome these challenges included piloting using a video rather than written material and sending follow-up personalised letters using lay terminology to describe upcoming investigations and treatment. One staff member also mentioned a service operated by Maggie’s Centres which offered patients the opportunity to attend a session (either in person or online by video) that involved staff talking them through the chemotherapy experience and showing videos of what to expect.
Staff also reported specific barriers for patients whose first language was not English (see discussion about interpreter services in Chapter 2).
Content and level of detail of information
In some cases, patients described feeling that the information provided was lacking in detail on aspects that were important to them, for example, what to expect during treatment. This patient noted that they had discussed the treatment with their surgeon but would have liked more detail in writing and suggested email could have been used.
"It was a little bit thin on detail. Like it said, ‘you're getting this treatment and that treatment starting on the Monday’. […] It would have been better if it had a little bit more detail on it. I think I said to my mum, ‘You know, it looks as though somebody just realised they hadn't sent me anything and quickly bashed up something on the computer and tried to get it in the post as fast as they could because they realised I was coming their way on the Monday so they did their best to try to give me something’. - Patient, more deprived area
Another patient reported a more positive experience of being provided with sufficient detail, and the opportunity to ask questions at the initial appointment, which was very important to her:
"Actually, that, for me was so helpful because I'm a doing person… [If they had] sent me away with that information and no date of when I was going to come back, I think I would have totally cracked. And people being willing to take the time [was helpful]. Because, you know, I probably asked a lot of questions, maybe more than some other people, because knowledge is power to me and that's what reassures me. Tell me what's going to happen if it's really bad, I'll get my head around it.” - Patient, more deprived area
While not always the case, information on potential side effects of treatment, and their likelihood, was seen as a particular gap. Staff thought that this information gap was more likely to negatively impact patients living in more deprived areas who, staff reported, were more likely to tolerate side effects. They felt this may be due to these patients sometimes already having poorer health, or lower expectations of their health, and therefore being less likely to seek support. Health literacy was identified as a barrier in that some patients found it more difficult to recognise that they needed to ask for medical help, and to communicate with professionals about their symptoms.
"You know, I just think maybe people from affluent areas are generally not, you know, their health is better. So if they have anything that makes them feel a little bit unwell, they're much more happy to access the service. Whereas I think if you're used to always being not that well, that they will just almost put up with things rather than ask for help." - Staff, more deprived area
Examples of patients who felt their experience had been affected by a lack of information on side effects included one patient who experienced serious constipation from chemotherapy and would have taken medication to counter this had she understood how bad it would be. Another patient was alarmed by a skin reaction she had experienced as a side effect of radiotherapy, and a third patient had received medication to counter the side effects of chemotherapy but had also experienced side effects of this medication, which she felt had not been explained.
"But nothing was actually discussed with you. They just, ‘Oh, here's your medication, it says on the packet, when to take it’ kind of thing. But nothing was discussed about maybe any side effects. I think they left it for you to read the leaflet that came with the medication." - Patient, more deprived area
Relatedly, one patient reported a lack of information on surgical aftercare. She had an issue with dissolving stitches and had not received any advance information on the potential for this to happen. She knew someone who had received similar treatment privately and had received much more comprehensive information. She was also able to find what she was looking for online, on the website of another health board, suggesting that the information is available.
A staff member acknowledged the challenges for health boards in maintaining in-house personalised and up-to-date materials. They gave examples of third sector materials that they felt to be particularly effective, including the Roy Castle Lung Foundation booklet, which can be tailored to the treatment the patient is having, and Macmillan website materials which are frequently updated with new drugs that become available.
Again, in a similar vein, some patients would have welcomed further information on treatment risks. Two patients who raised this were men in more deprived areas who had experienced post-surgical complications from prostate and bladder surgery and, in hindsight, wished they had been clearer on the risks before going ahead.
Delivery of verbal information
Clinicians’ manner and, in turn, the delivery of information, had a clear impact on patient experiences.
"So, initially, when I had my diagnosis, when I first attended [hospital], I had a really brilliant doctor and I think I just felt I was in such good hands that I very much felt that my interaction with her kind of, I'm not sure how I'd put it into words, but it kind of set the tone for the remainder of my journey because I felt very well informed from the offset, which made a huge difference. She just explained herself very well. I felt really quite well informed at every stage of the journey. And I think maybe that doesn't work for everybody, but for me, that made a huge difference." - Patient, rural and island area
Other patients reported less positive experiences. For example, one patient in a more deprived area described feeling as if he had been told he had cancer in a very matter of fact way and felt that the conversation could have been handled more sensitively.
"It’s the matter-of-fact way they tell you you've got cancer, just like they’re dropping it into a normal conversation, eh?" - Patient, more deprived area
Other patients reported feeling like they were being dismissed, or that their consultant was getting frustrated with them asking clarification questions. One patient also gave an example of having medical students in the consultation room (which she had consented to) and feeling that the consultant focused their communication on the students rather than talking and listening to her. A further patient was upset that a consultant did not apologise to her for keeping her waiting and sat with their back to her during the consultation. Reflecting on such experiences, a patient thought it was important that staff remember they are dealing with people who are scared, and treat them accordingly.
"I think that's the number one thing that people need to actually remember - that you are dealing with someone that is scared [thinking] ‘Am I going to get through this?’." - Patient, more deprived area
Staff acknowledged that there was variation in the manner clinicians had with patients when communicating information to them.
"You get some [consultants] that are very, very good and you get some who don't have such good communication skills.” - Staff, rural and island area
There was a staff view, however, that, on the whole, staff were much clearer and explained things more fully than they would have done in previous years. Examples of good practice included actively encouraging patients to ask questions, drawing diagrams to aid understanding, adapting to patient preference (e.g. not giving too much medical information when someone says they are ‘squeamish’ or being fully upfront with patients who request this). Further detail on patient-clinician interactions, specifically on shared decision-making, is provided later in this chapter.
Recommendation 9: In line with the People Principle in Scotland’s Health & Social Care Service Renewal Framework9, ensure that patients are provided with plain‑language information in more than one format (written, verbal, or digital) at key points in their journey (before, during and after treatment). Consider increased use of video resources showing what patients can expect during treatment.
Follow-up communication
As noted in Chapter 3, one of the roles of the CNS, and in some cases SPoC staff, was to aid patient understanding of information following their initial diagnosis. In practice, this involved them attending appointments with patients and consultants (including video consultations), proactively contacting patients (including running clinics) in the days or weeks following their initial appointment to confirm understanding and answer questions, and being on hand for patients to contact them with any questions or concerns. This proactive contact was valued by patients, who may not have otherwise known who to go to with questions, and CNSs were considered to be particularly skilled in this role, often acting as a conduit between patients and consultants.
“The consultant was a wee bit difficult to understand, not all the conversation, but, you know, there was a few things I didn't quite pick up, but the Macmillan nurse did, and she wrote them all down and the names of, even the names of the chemotherapy you're getting, so everything was written down. And then after the call, the Macmillan nurse went through it all with me and so it did make a huge difference having her with me. Definitely, yeah. All the medical terms I didn't know that I didn't know, she did." - Patient, rural and island area
"Routinely with patients that we see at short notice clinic, and the ones that [have a straightforward cancer diagnosis] - I use the word straightforward, it's never straightforward having a cancer diagnosis - but if they are given information, given their booklet that's personalised to them and they've been to pre-assessment and they're going for surgery, [SPoC] will routinely phone them later in the week just to check in case they've got any other questions as well.” - Staff, rural and island area
Staff noted, however, that, while follow-up contact was welcomed by many patients, some did not want to be reminded of their diagnosis; therefore, they had to be guided by individual patients.
While CNSs played a key role in providing follow-up support to patients, there were also mentions of consultants doing this, with one patient in a more deprived area being pleased that her surgeon had phoned her to check in on her following her surgery.
Reaching shared decisions about treatment
The provision of accessible information, as described in the section on information provision above, was an important first step in facilitating shared decision-making. Other factors also contributed to patients and staff being able to reach shared decisions on treatment that take account of patients’ wishes and wider circumstances. These are discussed in the remainder of this chapter.
Experiences of shared decision-making
Typically, patients described feeling that they did have a say in their treatment. As one patient explained, the decision was taken jointly by themself, their wife and staff.
"Well, they're the experts now. They're not always right but they were very approachable and very easy to talk to. And so I would say it was a joint decision between the four of us (patient, wife, surgeon and CNS)." - Patient, rural and island area
While it was not commonplace for patients to report wanting to have a say in their treatment but not being able to, there were patients who found it surprising to be asked about this in the evaluation and did not see its relevance. This seemed to be because they did not see any reason to not opt for the treatment recommended by medical professionals, who they saw as being much more qualified to make the decision. In some cases, it may have been that treatment options were more limited and they did not have choices, other than to have no treatment.
"They basically said that if you don't get it, you die". - Patient, rural and island area
However, in other cases, it may be that these patients did not have treatment options presented to them as shared decisions.
“I don't think I felt I was deciding what treatment to have. I don't think I was conscious of making that decision. I think I just, I'm not sure if I actively or subconsciously, just accepted what their recommendations were for treatment.” - Patient, rural and island area
"I was offered treatment and then I received it. I don't really understand how anything could have made it more helpful. It was just a case of being told I needed ‘X, Y and Z’ and just getting ‘X, Y and Z’. […] I was just told that this is what would help me in my particular circumstance. And I went with them, I trusted them and I had the treatment, and praise God, I'm better. So I don't really understand, more than that, how I can answer that question. […] And why would I even think that I might know more than these people who are trained to deal with the situation, that I would know better than them and how to treat them?" - Patient, rural and island area
Staff also provided evidence of shared decision-making happening in practice.
"I'd say we're very fortunate with the oncologists and the respiratory consultants that we work with. That's very much their way of working, that their patients are not pushed in a direction that they don't want to go in. They always have options. And even if that option is of no treatment while they're still well enough for treatment, as long as patients have been given full information, have time to discuss it with their families." - Staff, more deprived area
"Unfortunately, I've got a lot of patients who come in younger and younger, and I've got two or three really young patients who are trying every single thing that they can and want to explore every alternative. You know, they're doing their own research and stuff like that. And I think we're very lucky - our oncologist is always very supportive of those patients and, you know, helping them and supporting them and doing whatever they can." - Staff, rural and island area
However, other staff reported that it was more of a mixed picture. A number of challenges were reported, which are discussed below in relation to practical challenges and challenges related to patient beliefs and attitudes.
Facilitators
As described earlier in this chapter, the manner and approach of individual clinicians affected patient experiences. This was particularly true in the case of discussions about treatment options and it was the key factor in whether patients felt they had a say in decisions about their treatment. Features of clinicians’ approaches that facilitated shared decision-making included:
- Where more than one treatment option was available, talking through each option in detail including likely success, risks, recovery timescales and potential side effects.
- "They explained everything, all the different options, and then just left it to me to decide. I think I'd already made the decision as soon as they told me." - Patient, more deprived area
"All the choices were explained to me in great detail by both the breast surgeon and the breast care nurses who spent an hour with me. I think it was just taking me through all the options, just so I was absolutely clear in the decision I was making. So that support was fantastic." - Patient, more deprived area
- Honesty and openness about prognosis with different options, including no treatment, and supporting patients to weigh up quality of life considerations.
- “We always talk about what's wrong and what the potential treatment options are, […] And we always have that, you know, ‘and what if I do nothing?’ conversation as well. And we do invite relatives to come in to support people during their discussions so that they're making an informed decision that suits them and their, you know, their life and their family. We do that quite well on a weekly basis, really. Everybody, you know, we talk through that. So I think where we are, we're very fortunate that it, I think it works well." - Staff, rural and island area
- Encouraging patients to communicate what their main hopes and concerns would be coming out of treatment.
- “But we do ask what their sort of, what their main concern would be throughout treatment and what we can try and do to kind of alleviate that.” - Staff, rural and island area
- Being explicit that the final decision lay with the patient.
- "The oncologist went through the positives and consequences of stopping the chemo early. And she said it was entirely my choice." - Patient, rural and island area
- Offering patients time to consider options and offering further appointments.
- "It's quite easy because surgeons will offer that and you know, it can be either back at the short notice clinic again or it could be a Near Me [appointment] or it could be or a phone call and you know, sometimes a phone call is all that is needed. It's just that reassurance to speak things through again." - Staff, rural and island area
- When asked, providing their view on what they would do if they or a loved one were in the same position.
- “They had a couple of different treatments and a couple of different timescales for the treatment with radio and chemo and it was just with time scale and lifestyle, we decided which one would go for and me asking [consultant] ‘What would you do if it was your brother or your son?’ type of thing, put them on the spot. And it was basically, well, if I didn't do it and it comes back, there is something wrong and what do I do? And it might be worse.” - Patient, rural and island area
- Inviting questions from the patient and their family member/friend.
- "It was given to me as ‘This is what we would propose to do. What do you think about it? Are you in agreement with it?’ and it was open to me to ask any further questions that I might want to ask." [...] "Any medical appointments I've had, I have not been shy to ask any questions I wanted to ask. And I have never found any of the professional people involved to hold back any information from me or to steer me away from the questions I was asking." - Patient, rural and island area
- Listening to patient feedback and requests.
- "That was an amazingly easy conversation to have. And I was taken aback by how amenable the consultant was. He could so easily have dismissed me, he could so easily have been just dismissive of what I was saying, but he wasn't at all. He was great. I explained my feelings, I explained why I felt that might be the situation, and he totally agreed. He wasn’t a bit arrogant or patronising towards me, which I think I possibly, with hindsight, would have expected." - Patient, rural and island area
- Being supportive of patient choices.
- “She [consultant] is an absolute legend of a person and was incredibly supportive of everything.” - Patient, rural and island area
- Offering reassurance that patients can change their minds if they are not coping with treatment.
- "The decision isn't concrete. It's always a bit fluid, and things can stop and start. Patients are told when signing for consent, they can always stop treatment if they want to stop.” - Staff, more deprived area
Practical challenges
While this was not widely raised, some staff did not feel they had received the necessary training and resources to implement shared decision-making effectively. For example, one staff member said that they would welcome further tools and guidance to support discussions and gave an anecdote of a patient interaction where this would have been helpful – the patient had chosen not to take a treatment option and then changed their mind a year later, when their symptoms had progressed, but the original treatment option was no longer suitable due to the stage of their disease and the staff member found this a difficult conversation to manage.
A further practical barrier was a lack of time in appointments for patients to process information and engage in shared decision-making. One staff member spoke of the importance of building trust with patients but noted this could require multiple appointments, which was challenging due to workload.
Challenges related to patient beliefs and attitudes
Deference to medical professionals
It was clear that patients placed a lot of emphasis on clinicians’ views and trusted their professional expertise.
"Well, you've got to trust them, haven't you? They're experts in their field and they know what they're talking about, hopefully. So you go by what they tell you." - Patient, rural and island area
“I took the view that I put my trust and faith into the oncologists, and I believe that was still the absolute right decision rather than trying to research.” - Patient, rural and island area
Staff understood the reasons for this and described that patients found absorbing all the information they were given, and making choices, to be overwhelming.
"If you've just had a cancer diagnosis and you've never had cancer before and suddenly you've been asked to make lots of decisions and you, you know, it's a wee bit like, you know, this is not a subject you've studied before, so how can you suddenly become an expert in it?" - Staff, rural and island area
From a staff perspective, however, deference to medical professionals acted as a barrier to shared decision-making. Staff reported patients, particularly in more deprived areas, often having a 'doctor knows best' attitude that made it difficult to have a good discussion with the patient about proposed treatment risks and benefits. Sometimes this extended to patients not reading information they had been provided.
“Sometimes they are a bit like ‘whatever you say, doctor’, and sign for treatment, without having read all of it.” - Staff, more deprived area
One staff member speculated that some patients may, in fact, take comfort in the more paternalistic, prescriptive medicine model where they are advised by a doctor, making it more difficult to shift to a shared decision-making approach.
"They're often saying, well, ‘Why is the doctor making me decide rather than just telling me what treatment I need?’ Or some people say they don't want anything, but then you find a middle ground.” - Staff, more deprived area.
Staff had also noticed patients in more deprived areas being less aware that they could ask for a second opinion without the doctor being annoyed, and being less likely to push for certain treatment options in the same way as patients in more affluent areas.
"I treat a lot of wealthier people in [city] who know what to ask for, and how to ask for it. And that makes a major difference in someone [compared to] someone who can't do that because they don't know how, or they don't have the language, or they don't feel empowered to do so." - Staff, more deprived area
One staff member working with patients in more deprived areas also spoke of challenges related to doctor biases. She felt that these biases could influence the treatment offered to patients and result in them not receiving the treatment that would be best for them. This was considered particularly problematic given some patients in more deprived areas may be less likely to question doctors’ advice and push for certain treatment options, as reflected in the description of deference to medical professionals earlier in this section. The staff member gave a specific example - in relation to patients’ fitness for treatment - of a patient with lung cancer who was not offered curative treatment due to doctors perceiving her to be less well than she was, as her house was very messy and she didn’t get dressed or out of bed prior to the assessment.
“An example would be, I had this lady who was in her 30s who had lung cancer and a solitary brain metastasis and she was in a very deprived area, house was in a terrible mess. She had a range of children, different ages and she always looked worse in bed than she would ordinarily because she wouldn't get changed, she'd look a bit grubby. When she was visited by people to talk about different treatments, she didn't come across well and […] she ended up not really getting any treatment because everything took so much time and, and she wasn't advocating well for herself. And when we were looking at fitness and performance for all of these things, she came across badly because she didn't put on a good front. You know, she didn't put on a clean top. She wasn't sitting up. But actually, if you're more objective about it, she's okay. Once you work with a group of patients that are like this, you understand that in many ways they are going to look less suitable for treatments. The performance status will be affected by biases. And that is the problem that's going on here.” - Staff, more deprived area
Wider social influences
Patients were also sometimes exposed to information and advice on treatment options from non-medical sources that could influence their decision-making. For example, the views and experiences of family members or friends and unofficial online sources.
Patients who took part in the evaluation did not attribute a great deal of weight to these sources. Although there were those who spoke about what their family or friends wanted them to do, this was typically to take up treatment and patients did not tend to report being persuaded against treatment due to the negative experiences of others or things they had read online. One patient spoke of how a clinician allayed the fears he had, by explaining that his treatment would not be ‘anything like the horror stories he’d heard’.
Staff views were more mixed. While recognising that this was a generalisation, one viewpoint was that patients in more deprived areas were more susceptible to having decisions influenced by the experiences of others (who may not have had the same cancer type and/or who may have had their treatment a number of years ago) and misinformation, as well as a tendency to opt for less aggressive treatment options. Examples of the type of beliefs staff heard were: ‘the chemo killed them’ and ‘if you open them up [via surgery], it spreads the cancer’. Factors felt to be behind these beliefs were a sense of resignation among those in more deprived areas that they had had a ‘good innings’ and that cancer was ‘going to get them at some point’, a lower ability to critically appraise information and, relatedly, being more suspicious of treatment if they were unable to understand the science. One staff member also suggested that patients from more deprived areas were more likely to know someone who had died from cancer (potentially due to later stage diagnosis being more common) and have little hope following their own diagnosis as a result. Staff understood these views given the lower life expectancies in more deprived areas.
“Life expectancy in deprived areas is lower so they don't expect to live long, they don't expect to live to 85…looking at their mums, their gran…a high number of people die at a young age so it is their normal.” - Staff, more deprived area
More generally, staff recognised that experiences of others close to them were valid for patients and that it was understandable that they would inform decisions in some cases, for example when no curative treatment was available.
"I suppose it's their lived experience, really, that will impact their decisions. So, if they have experience within their own families of cancer and cancer treatments, that will impact their decisions. I recently had a 76 year old gentleman who had had what we had hoped was curative treatment for a colorectal cancer, discovered that he had liver metastases and, although he's reasonably fit as he is at the moment, and would have coped with palliative chemotherapy, which may have extended his life a little bit, he's declined referral to oncology because he's lost four siblings over the last 15 years with cancer diagnoses and none of them responded well to palliative treatments. So based on that, he's decided to decline any referral." - Staff, rural and island area
On the other hand, there were staff who felt that patients in more deprived areas were less likely to seek further information and were more likely to defer to the recommendation of the doctor (as discussed at the start of this section).
Cultural influences
Cultural beliefs also impacted patient decisions about treatment. Examples provided related to cultural attitudes towards fertility in African communities, in particular, causing challenges in the treatment of gynaecological cancers, and stigmas attached to stomas in other cultures, impacting on bowel cancer treatment. In other cases, challenges were reported in cultures where the husband is the main contact for the wife’s treatment, making it challenging to understand the patient's perspective and wishes.
Figure 4.1 illustrates a patient’s experience of information provision and shared-decision making. It shows key aspects of their journey and how these relate to the dimensions of the COM-B model of behaviour change.
Recommendation 10: In line with the People Principle in Scotland’s Health & Social Care Service Renewal Framework[9], encourage patient empowerment, including by emphasising that patients can ask questions and have the right to a second opinion. Ensure all relevant staff are trained in shared decision-making and realistic medicine and have resources to support them to have these conversations with patients (including resources to help staff consider cultural influences on decisions around treatment). Conversations should include clear information about treatment side effects.
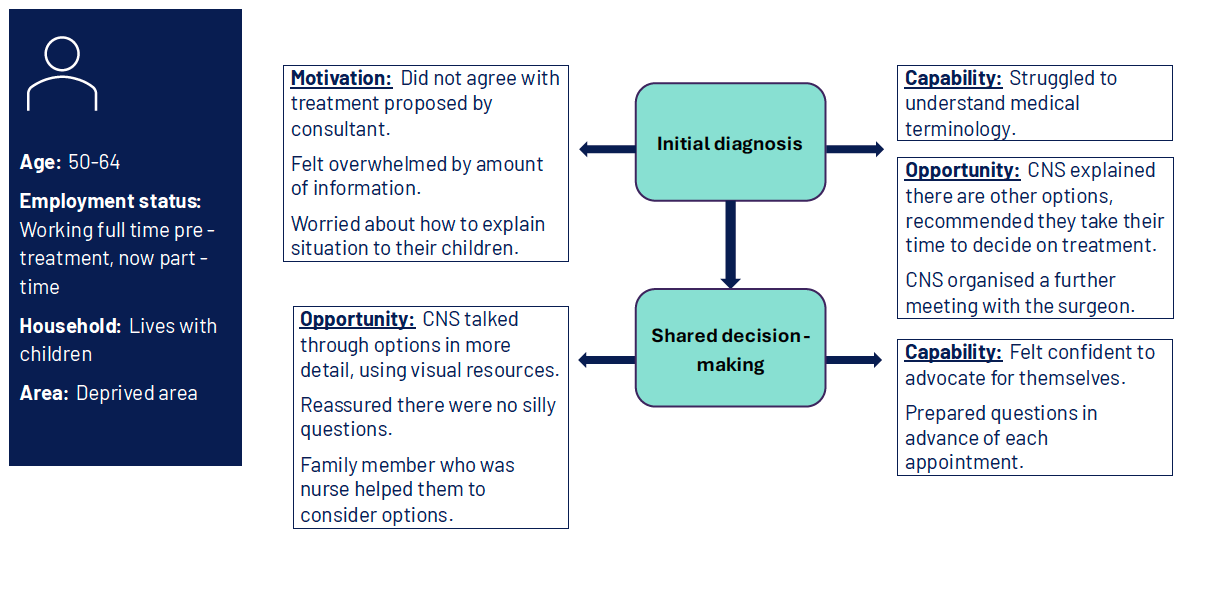
Diagram showing two stages of a patient's journey and relevant COM-B dimensions
Patient characteristics
- Age: 50-64
- Employment status: Working full time pre-treatment, now part-time
- Household: Lives with children
- Area: Deprived area
Stage 1: Initial diagnosis
- Motivation: Did not agree with treatment proposed by consultant. Felt overwhelmed by amount of information. Worried about how to explain situation to their children.
- Capability: Struggled to understand medical terminology.
- Opportunity: Clinical nurse specialist explained there are other options, recommended they take their time to decide on treatment. Clinical nurse specialist organised a further meeting with the surgeon.
Stage 2: Shared decision-making
- Opportunity: Clinical nurse specialist talked through options in more detail, using visual resources. Reassured there were no silly questions. Family member who was nurse helped them to consider options.
- Capability: Felt confident to advocate for themselves. Prepared questions in advance of each appointment.
Contact
Email: socialresearch@gov.scot