Scotland's cancer strategy: services and support evaluation
Findings from an evaluation of cancer treatment services and support in Scotland. Specifically it looks at experiences of patient access and engagement with cancer treatment and support in rural and island areas, and in areas with higher deprivation.
Chapter 3. Person-centred care – evaluation findings
This chapter explores person-centred care and the extent to which it promotes effective engagement with clinical cancer treatment. It considers person-centred care in practice in more deprived and rural and island areas, exploring what it looks like, its importance to patients and challenges to supporting it. The Cancer Strategy includes an ambition for patients to receive person-centred care, which places them at the heart of their treatment and support journey, taking into account their individual preferences and circumstances. As noted in Chapter 1, this was one of the reasons behind the introduction of the Single Point of Contact (SPoC) initiative.
Key findings
- Having a single member of staff to build relationships with patients and consider their holistic needs was viewed as the main facilitator to the delivery of person-centred care and supporting access to, and engagement with, treatment.
- Where in place, CNSs were central to this, acting as the main point of contact, consolidating understanding of treatment options, providing emotional support, signposting to other services, and advocating for patients. However, access to a CNS varied between and within health boards depending on cancer treatment pathways.
- The Single Point of Contact (SPoC) model also supported person‑centred care, though its operation differed. In some areas it functioned largely as an inbound triage phone line while in other areas SPoC staff proactively contacted patients from diagnosis and undertook elements traditionally associated with CNS roles.
- Workforce capacity was the main challenge to delivering patient-centred care. Where CNSs or SPoC staff were absent or stretched, this impacted on services’ ability to build a holistic picture of a patient’s needs and the timeliness of addressing patient queries.
The provision of person-centred care
Person-centred care relies on staff building relationships with patients to gain an understanding of their holistic circumstances and needs in order that these can be considered, as far as possible, during treatment decisions. The main professionals involved in patients’ cancer treatment were consultant oncologists, surgeons and radiologists, CNSs and wider nursing staff (e.g., those delivering chemotherapy or providing in-patient care) and, in some cases, SPoC navigators.
The role of Clinical Nurse Specialists
Where CNSs were in place, this role was particularly key in the delivery of person-centred care. The CNS was typically the main point of contact and had the opportunity to build a relationship with patients. They took on a number of roles (as highlighted at relevant points throughout this report) including: consolidating patient understanding of their treatment and treatment options, answering their questions, providing emotional support to patients, and signposting them to other services. They typically acted as an advocate for patients, and a link between them and other medical and support staff involved in their care.
However, access to CNSs was not equitable and varied both between and within health boards and pathways, but not having any CNS support in a particular pathway was raised more in rural and island areas. Where they were not in place, staff described this as a gap in their service which was considered to impact patient experiences. Inequity was thought to be related to funding, although it was noted that decisions as to which cancer pathways had CNSs were not always transparent.
"So, I think the Scottish Government target is that all patients with cancer should have access to a cancer nurse specialist, but very few of the haematology patients have access to a cancer nurse specialist. So I think it makes the journey of going through cancer treatment and the complexities of that or the logistics of it and the psychological burden more difficult for patients in [health board]." - Staff, rural and island area
Where CNSs were not available, staff noted that consultants would tend to pick up the duties undertaken by CNSs elsewhere, adding to their workload but also potentially negatively impacting patient experiences in cases where they did not have the time to get to know the patient and understand their wider circumstances in the same way that a CNS would.
"So, because there's no CNS, that means that the consultants are doing work that a CNS would normally do. So maybe things that relate to logistics around scans, transport, phone calls. Yeah, giving out information about Maggie’s and referrals to Maggie’s and all these sorts of things. It's all done by medical staff. So if we had CNSs who could do some of that work, it would free up some of our time to do other work there." - Staff, rural and island area
In other areas, CNSs had upskilled and had expanded their role, enabling them to take on duties that freed up other clinicians.
"I think we've changed our role, we've advanced our role as Clinical Nurse Specialists. So, about three quarters of the team are now Advanced Nurse Practitioners, we're all prescribers. We're much more involved in the acute side of things within hospital and community." - Staff, rural and island area
Staff also noted that, across health boards and pathways, the level of support that CNSs were able to provide varied according to their caseload. There was a suggestion that greater support was provided in rural and island areas due to the smaller population and resultant caseload.
The role of Single Point of Contact
As described in Chapter 1, SPoC aims to enhance existing services by providing dedicated person-centred support through the cancer pathway. Again, SPoC was not available across all pathways and areas. Chapter 1 also highlights the variation in the operation of SPoC. In some areas, it acted largely as an inbound telephone triage service for patient questions or concerns while, in some rural and island case study areas, the SPoC role involved proactive, face-to-face contact with patients from the point of diagnosis, taking on some duties that would previously have sat with the CNS, and providing the opportunity to build relationships with patients.
Facilitating person-centred care
Having a single member of staff to build relationships with patients and consider their holistic needs was viewed as the main facilitator to the delivery of person- centred care. It was clear the value they could add by having an overview of the patient circumstances.
As noted above in relation to the provision of person-centred care, CNSs were most commonly the main point of contact for patients. On the whole, both patients and staff were extremely positive about the role they played. They were described as going ‘above and beyond’, particularly for patients who required extra support (which was often the case in both more deprived and rural and island areas).
“But I think once you're sort of going through all the treatment and you sort of realise the difference that it actually makes to whether or not you survive, the people who are fighting your corner, you know, the whole team approach now. I watched older relatives who have had cancer and the way that treatment works now is so different. […]. You need people who are there to get you through this and who are on your side and fighting your corner with you as much as the drugs and the training of those people is so incredibly important." - Patient, rural and island area
“You can't phone up a consultant. Consultant secretaries are busy, busy. But the cancer nurse, you feel like you'll phone her and she will get back to you. So that's important. […] To have that one person kind of responsible for being someone who you can phone that will respond. That's a dedicated job […] But you feel if you phone and it's a different person just giving you robotic answers, you wouldn't feel you're getting quite the same service than someone that understands because they know you. It's quite good.” - Patient, more deprived area
"The clinical nurse specialist relationship with the patients is usually very strong and people do go above and beyond, you know, to support more vulnerable patients. And I've had a lot of good feedback from those patients to say, you know, ‘so and so has phoned me to remind me of this appointment and they've managed to move this for me because I can't do this or I can't do that’ so I think that there is a recognition that some patients do need extra support." - Staff, more deprived area
Staff considered the presence or otherwise of a CNS in a department as a significant factor in the level of support provided to patients. Establishing relationships with patients at an early stage was considered particularly valuable.
“I think that's where the role of a nurse specialist comes in, who can pick up the nuances and then probably have another conversation with the patients to understand where they're coming from, understand what they've taken from that consultation, understand what restrictions they think are upon them, let the patients know what support is available to them as they go through the treatment. So it's not just that they're doing it by themselves, it is the fact that they will be supported all the way through.” - Staff, more deprived area
"It's really transformed the support we can give patients because we're involved in their care very, very early on. […] It's a time of high distress and high emotion, and we're now able to be there very early on. It's had the biggest impact on cancer services than anything else that's happened in the last few years." - Staff, rural and island area
"I think there's a clear difference in our specialties that have Clinical Nurse Specialists support, because they're just so vital and we've struggled to justify getting them in some specialties, but we're getting there now. […]." - Staff, rural and island area
One staff member also described the positive impact of having a CNS on their unit’s performance measures, which they felt supported the cost-effectiveness of the role.
Reflecting the inequity of access, some patients did not have access to a CNS or SPoC and others reported that they had a CNS but had not been able to build a relationship with them, for example because they were not aware they could phone them with questions. Patients in these circumstances spoke of the difference they felt it could have made to their treatment journey to have someone supporting them throughout.
"If somebody was allocated that you knew, they knew your history, they were part of your journey, they were part of your team, somebody who's been part of your journey from day one, not somebody who's just randomly been sent out to you, who, at your worst, you have to suddenly start relying on and you don't have that relationship with." - Patient, rural and island area
Where SPoC had been implemented to include proactive patient contact, views were also positive about the impact on patient support, with it being described as ‘more holistic’.
Challenges
The main challenge reported in the provision of person-centred care was staff resource. As noted previously, not all pathways in all areas had CNSs or SPoC staff in place and, where they did, caseloads were often substantial. Indeed, CNSs themselves spoke of feeling restricted in the extent to which they felt able to offer the support to patients that they would like to. Factors that had contributed to their increasing workload included the increased incidence of cancer, and the fact people were living longer with it, and the expansion of their role to include greater responsibilities. They did not feel that the workforce had grown in line with the increased caseload. In some cases, there was only one CNS and staff raised particular issues for patient support when they were on leave or off sick.
Workload challenges were reflected in patient experiences, with some patients reporting difficulty reaching their CNS, which they recognised was due to their workload.
"She's [CNS] not always able to get back to me that day and I fully understand, but I can also understand that some patients want to talk to their nurse now. You know, they're going through a lot of trauma and they want someone to talk to." - Patient, rural and island area
It was suggested that increasing the number of CNS posts would be the best way to address these challenges.
“I suppose, in terms of the patient numbers, people with cancer diagnosis is going up all the time. So, in order to ensure that there's equity right across the board for patients in all different cancer groups, would need more staff." - Staff, more deprived area
Where SPoC had been implemented in pathways, CNSs typically reported a positive impact on their workload.
"My phone used to ring hundreds of times a day, and you can't keep. You know, it's distracting, and you have to carry your phone in case somebody needs you, but it's distracting when it's ringing up. So it's taken away a lot of that stress and stuff for me because, you know, you're not thinking, oh, who's phoning me? What? Wonder what that message is. And, you know, they. And they can deal with some of the simpler issues." - Staff, rural and island area
While this had supported the reduction of the CNS workload, there were still challenges. For example, in set-ups where the primary role of SPoC was to triage patient calls, staff relayed reports of patients being frustrated at not being able to speak directly to their CNS and having to tell their story to someone they didn’t know, arguably making their care less person-centred.
“[SPoC workers] manage the calls for the CNSs. It can be helpful, but patients get frustrated because they're trying to contact the CNS and instead they have to speak with someone they don't know. It's also frustrating for the support workers at [our service] because they have to go through the same long winded message whenever they need to contact the CNS, so they usually email or teams CNS instead on behalf of patient.” - Staff, rural and island area
An alternative view was that it is preferable for the patient’s calls to be answered by someone rather than reaching an answerphone.
"I think a real boost for patients knowing that when they phone, the likelihood of the phone being answered is greater than how it might have been when it was just the nurse specialist having the answer there." - Staff, rural and island area
One staff member also raised a concern about patients phoning SPoC rather than her directly. She described that, previously, patients may have phoned to check appointment details but often go on to open up about other concerns that were on their mind. The move to SPoC, she felt, may mean that the emotional support previously provided by CNSs over the phone does not exist to the same extent.
These challenges provide support for models in which the SPoC role involves a greater level of patient contact where individual staff can build relationships with patients. However, there was a view that staff in this role should have a level of clinical training.
"I don't think there's any point in having [clinically] untrained staff. I feel quite strongly about that. I think over the years, services have been cut to the detriment of healthcare. There is an argument, you know, to care for somebody, you don't have to have a medical degree or a nursing degree or anything like that. But actually, to see the full picture. I feel you do [need to have clinical training]." - Staff, rural and island area
In one rural and island area, SPoC professionals were trained as nurse associates, meaning they had some clinical training that expanded the role they were able to have with patients to include patient observations. This had facilitated the introduction of a seven day nursing service which provided a layer of reassurance to patients that they could always contact a medical professional even at weekends. A staff member in a different area also highlighted that SPoC training can also include emotional and psychological support.
*Recommendation 8: In line with the People Principle in Scotland’s Health & Social Care Service Renewal Framework[9] (person-centred care), provide each patient with a named individual who will build a relationship with them and support them through their cancer journey. While this evaluation found that CNSs (or SPoC staff with clinical training) are well suited to this role, where this is not feasible, learn from examples of good practice e.g. approaches that ensure full use of varied health and social care teams.
Figure 3.1 illustrates a patient’s experience of person-centred care. It shows key aspects of their journey and how these relate to the dimensions of the COM-B model of behaviour change.
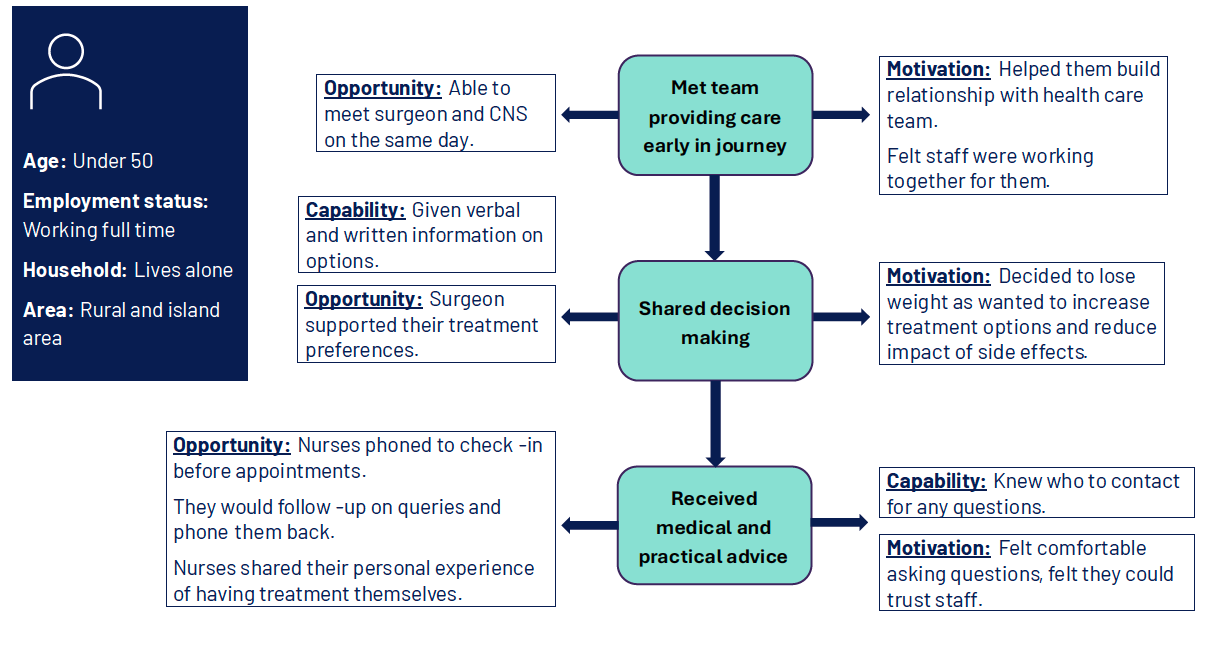
Diagram showing three stages of a patient's journey and relevant COM-B dimensions
Patient characteristics
- Age: Under 50
- Employment status: Working full time
- Household: Lives alone
- Area: Rural and island area
Stage 1: Met team providing care early in journey
- Opportunity: Able to meet surgeon and clinical nurse specialist on the same day.
- Motivation: Helped them build relationship with health care team. Felt staff were working together for them.
Stage 2: Shared decision making
- Capability: Given verbal and written information on options.
- Opportunity: Surgeon supported their treatment preferences.
- Motivation: Decided to lose weight as wanted to increase treatment options and reduce impact of side effects.
Stage 3: Received medical and practical advice
- Opportunity: Nurses phoned to check-in before appointments. They would follow-up on queries and phone them back. Nurses shared their personal experience of having treatment themselves.
- Capability: Knew who to contact for any questions.
- Motivation: Felt comfortable asking questions, felt they could trust staff.
Contact
Email: socialresearch@gov.scot