Realistic Medicine - Doing the right thing: Chief Medical Officer annual report 2022 to 2023
Chief Medical Officer's (CMO) third annual report, and the seventh on Realistic Medicine. It reflects on the challenges our system is facing and asks professionals to practise Realistic Medicine, in order to deliver value based health and care and a more sustainable system.
Chapter 3: Health inequalities: Turning the Tide
Health inequalities in Scotland
These are health inequalities – defined as, "systematic, avoidable and unfair differences in health outcomes that can be observed between populations, between social groups within the same population, or as a gradient across a population ranked by social position".
In Scotland, as in other countries, the levels of health experienced by different groups of people are not equal. People with lower incomes, or who are socially disadvantaged in other ways, consistently have poorer health. Those experiencing poverty, deprivation, racism and discrimination come into contact with every aspect of our health and care system. The theme of health inequalities has featured in my two previous reports. In this report, I am keen to focus attention not only on the role of healthcare but on aspects of wider socioeconomic policy in targeting the underlying core determinants of health. In the previous chapter I spoke of a value based approach to delivering health and care. This includes equitable care that is delivered in the right way, by the right person at the right time. Getting this right means that we are including and engaging effectively with those most at risk of poor health in our society. Getting this right means we all need to play a role.
Health inequalities trends
The extent of health inequalities in Scotland has varied over time and tracks changes in wider social and economic inequality. For instance between the 1920s and 1970s, mortality differences across the United Kingdom declined. During this period the welfare state was built, state pensions were introduced and the NHS was created. Income and wealth inequalities fell, and the power between social groups was more equal. Subsequently these trends reversed as economic policy changed, inequalities in income and wealth widened, and the balance of power became more unequal.
The initial stages of the COVID-19 pandemic exposed the underlying socioeconomic inequalities in society, and brought greater focus to the long standing racialised health inequalities that exist in Scotland. This led to a further widening of mortality inequalities in 2020-21. These dramatic changes are captured in the figures below. Here we can see the rise in all-cause mortality rates for both men and women in Scotland, but also that those in the most disadvantaged populations are accelerating at a faster rate.
In the Health Foundation report, Leave no one behind, amongst the important data it displays, the most alarming signals suggest that the fortunes of those living in our most deprived communities are becoming detached from the rest of society. The effects of the pandemic, the current crisis in living standards and the growing impact of the climate emergency are further compounding this gap. This strongly suggests that those with agency who can act must do so for the collective good.
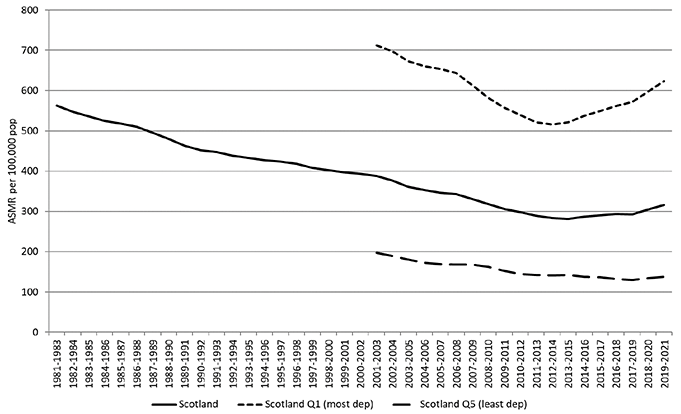
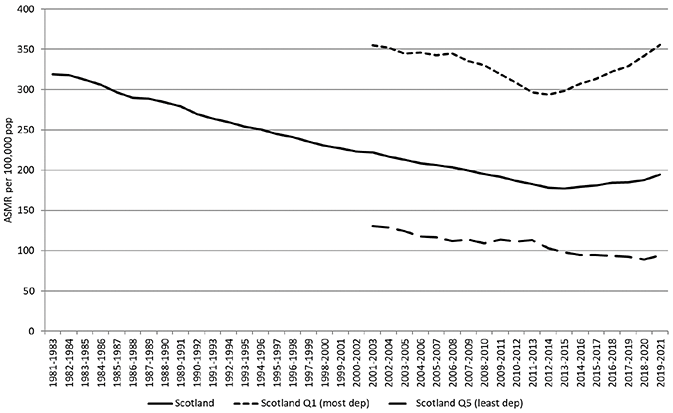
Source: Changing mortality rates in Scotland and the UK 1981–2021
What causes health inequalities?
Everyone's health is affected by many different influences over the course of their lives including early years experiences, schooling, employment, physical and social environments and the quality and accessibility of public services. These influences are affected by the economic and other resources that individuals can draw on.
Racism and discrimination or disadvantage, perceived relative status and the extent to which people feel in control of their life all affect health. These psychosocial influences affect mental health and lead to adverse health behaviours, but evidence also shows that they can affect physical health through changes in cortisol and other mediators. This wear and tear on the body is known as allostatic load, which accumulates as an individual is exposed to repeated or chronic stress.
There is also a cumulative life course effect. Children in families with more resources are likely to have more positive experiences growing up. This will both directly benefit their health and equip them to gain further social and economic resources, continuing to benefit them throughout their life.
Taken together, the breadth of these influences means that reducing health inequalities cannot just focus on addressing individual diseases or risk factors but must tackle the 'fundamental causes' driving inequalities. The fundamental causes are the underlying inequalities in income, wealth and power between social groups. They lie beyond the healthcare sector or decisions made by individuals and are the most important factors in explaining why and how inequalities in health change over time.
Between 1981 and 2011 the average mortality rate for the whole population continued to improve. From 2012, average mortality rates and life expectancy in Scotland (and many high-income countries) stopped improving. Mortality actually increased and life expectancy declined for people in our most deprived areas. Over the last ten years there has been growing unease about the long-term health implications of the global economic recession following the financial crisis in 2008, and the subsequent austerity measures implemented in many countries. National responses to this major economic downturn varied substantially but, in many cases led to extensive reductions in public expenditure, including cuts to central and local government budgets, welfare services and benefits.
The figure below illustrates how the fundamental causes of inequalities influence health, leading ultimately to the health outcomes that we see.
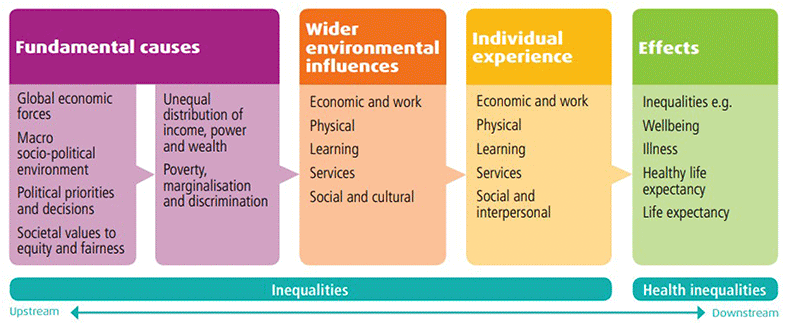
Source: Public Health Scotland
The importance of income as a key fundamental cause affecting multiple health outcomes and determinants is shown in a recent report from Public Health Scotland on health impacts of the rising cost of living in Scotland. Rising costs due to inflation effectively reduce household incomes. These impacts will not be felt equally across the population. They will disproportionately affect low-income populations, disabled people, older people, minority ethnic people and rural populations with long term effects on children. The supporting system model shows how these factors interlink to impact population health.
Turning the tide
Socioeconomic drivers provide much of the benefit in supporting us to live healthy lifestyles, and often in healthcare we are dealing with the consequences of health inequalities, rather than targeting underlying causes. However, our ability to enable people to continue in, or return to, employment for example has both individual and societal benefit that assists in reducing inequality and is a critical dimension of healthcare. Worryingly, the latest Labour market overview for the UK, published by ONS in May 2023, noted an increasing trend of people who were economically inactive due to ill health. This is a record figure for the UK. Targeted support to enable people to return to employment, during and following periods of ill health, including the development and maintenance of robust occupational health services should be considered important to improve this worrying trend.
The evidence-based Marmot framework describes a set of principles, first set out by Professor Michael Marmot in Fair Society, Health Lives in 2010 and updated in a 10 years on report. These aim to improve health and wellbeing and reducing health inequalities through coordinated efforts to affect the conditions of everyday life and reduce socioeconomic inequalities. These 'building blocks', or determinants, of health include good early years; good education; good work; good income; healthy places; tackling discrimination and racism; environmental sustainability, and good ill health prevention.
In the Marmot Review 10 Years On, Professor Marmot expanded on the conceptual model of explaining health inequalities and the strategies to target the structural drivers of inequities in power, money and resources. I want to emphasise the additions of addressing structural racism and tackling climate change as priority areas in our approach to reducing health inequalities. These domains are heavily interlinked and require dedicated, proactive resource to ensure a just and fair transition in the way we work, live and thrive together.
This figure gives a visual representation of how health and social care services contribute only 20% of the modifiable determinants of health, with the social, economic and environmental factors (50% collectively) being the primary drivers of our health and wellbeing. Although simplified for illustration purposes, the main message is that health and care services alone are not the solution to reducing health inequalities.
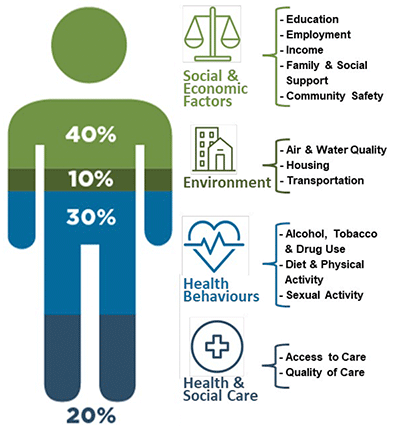
*Diagram adapted from Bookse et al., 2010 and King's Fund – A Vision for Population Health – Used for illustrative purposes.
Health services do, however, make an important contribution to reducing health inequalities by supporting action focused work on prevention, early detection, and early intervention and treatment. They ensure equity across the whole pathway of care, recognising that disadvantaged groups experience disproportionately poorer access and outcomes. In thinking of the role that NHS Scotland and its professionals play in contributing to the reduction of health inequalities, a systematic approach becomes essential.
Inclusive data collection
Inequity in vaccine uptake would risk perpetuating or even worsening existing inequalities if people who needed the most protection were unable to access vaccines easily. The introduction of the COVID-19 vaccination programme offered an opportunity to help address inequalities experienced by ethnic minority groups and people from more deprived areas.
From November 2021, people attending for COVID-19 vaccination were asked their ethnicity. Data was also collected through the online booking portal and national helpline . Analysis of the Winter 2022 influenza and COVID-19 vaccination uptake at 29 January 2023, showed ethnicity has been assigned to over 93% of the eligible COVID-19 records and to 90% of eligible influenza records. This has greatly improved Scotland's ethnicity data.
Having better data on vaccine uptake by ethnicity and areas of deprivation has helped NHS Boards tailor their vaccination delivery models. This has included producing an NHS Explainer video, offered in a variety of community languages, to provide answers to questions such as whether the vaccine is halal.
To ensure all communities had access to clinics, NHS Boards used a variety of trusted community venues to administer vaccines, such as African Churches, and worked with local religious and community leaders to disseminate relevant and accurate information.
Having improved ethnicity data has led to targeted actions based on where there is the greatest need, including the commissioning of qualitative research to understand what barriers exist to vaccination within specific groups with low uptake. The insights from this research have informed local approaches to reducing barriers to vaccination.
Data on deprivation has also been used to inform the vaccination programme, including through the strategic locating of clinics within areas of high deprivation to reduce barriers to access, such as cost of travel.
Ethnicity data collection is being extended to other vaccines. With more robust and complete data, we can improve our understanding of health inequalities and subsequently inform approaches to address them, with the aim of increasing vaccine uptake and reducing the risk of harm amongst low uptake communities. Ensuring inclusion is embedded throughout vaccination programmes is a critical principle of our approach.
We must continue to coordinate efforts within health and social care and also work across other sectors to address the wider determinants described above. It will take continued cross-Government working to address climate change; improve outcomes for children and young people, including child poverty and The Promise; and support a transition to a wellbeing economy through community wealth building efforts.
1. An advocate for change for the most disadvantaged groups
Health care professionals are having to adapt their role to an ever more complex environment. The impact of the economic realm on health outcomes, the links between planetary health and human health, and the recovery process following a global pandemic have shifted perception on the role healthcare professionals are playing in advocating for global health and wellbeing. I think it is extremely important we give time and consideration to this. Our voice can amplify the priorities and concerns of communities who have become marginalised or alienated in society, and we can work with these communities to increase their agency.
The Health of the Nation appendix to this report highlights the unmet healthcare needs of our population following the COVID-19 pandemic. These impacts will disproportionately affect people and communities most at risk, and will increase future health inequalities if not addressed. It is important that efforts to address pressure on services and help us catch up with backlogs also recognise the needs of the communities we care for and address barriers to care. We can do this by practising Realistic Medicine. In doing so we can direct resources away from services that are wasteful, less cost-effective, cause harms, are not valued by the people we care for and do not reduce inequalities.
Addressing the existing inequalities means delivering healthcare in accordance with need. Currently, healthcare services are either accessed equally across social groups despite differences in need, or disproportionately by those whose needs are lower. There are many reasons for this, including:
- people not feeling worthy of NHS resource;
- barriers to obtaining appointments and accessing services;
- a fading trust in services and providers;
- cost, time, caring or employment barriers; and,
- services being more stretched in areas with greater needs.
This may suggest a need for targeting of services to geographical areas of deprivation, but this can be stigmatising, and many people affected by inequalities do not live in these areas. A better alternative is to apply 'proportionate universalism' whereby everyone has access, but with more service provision for populations with greater needs. NHS services can also link patients to other services such as welfare advice to support them with other needs.
Meeting communities' needs
Gypsy/Travellers face some of the starkest inequalities in healthcare access and outcomes in Scotland. Key barriers to improvement in health outcomes include a lack of trust between Gypsy/Travellers and healthcare professionals; difficulties registering with GPs and dentists; low (health) literacy levels, lack of awareness of their rights and discrimination.
To help improve health outcomes for the Gypsy/Traveller community, Scottish Government funded MECOPP (Minority Ethnic Carers for People Project) to recruit and train Gypsy/Traveller community health workers (CHWs) to provide support, information and advocacy for their community on a wide range of health and social care issues. As gypsy/travellers themselves, the CHWs are trusted by their community and have personal knowledge and awareness of the issues and challenges they face. This has resulted in individuals and families feeling safe and confident to approach CHWs for help and support, and to discuss their health concerns.
Low uptake of cancer screening, as well as general communication with health professionals around women's health were identified by the CHWs as issues of concern. The CHWs worked closely with the NHS Screening and early detection teams to ensure they were aware of current advice and early detection pilots. CHWs were able to provide information to healthcare professionals around gypsy/traveller culture, and on barriers the community can face when accessing information and support. CHWs have successfully reached over 150 Gypsy Traveller women to provide early detection information and inform healthier lifestyle choices in a culturally appropriate way. This included running a women's only group at a gypsy traveller site on cancer screening and awareness. Cultural sensitivities and barriers were accommodated, such as inviting female-only health professionals to speak with community members. This informal opportunity encouraged the women to discuss health issues they hadn't felt comfortable speaking about before.
The sessions helped educate women on available healthcare and dispel long held cultural concerns around procedures like smear tests. More specifically, the session facilitated a CHW to support two women to register for smear tests (also accompanying them to the appointments). It also highlighted a lack of awareness relating to availability of vitamin supplements for babies and young children. This led to the CHWs working directly with the local NHS Board to establish a way to distribute vitamins for under 3's on two local authority gypsy traveller sites. All attendees were also given culturally appropriate information to share with their peers.
Scottish Government continues to work with the MECOPP and NHS Boards to learn from the gypsy/traveller community health worker project to support sustained improvements to access, experience and outcomes in health for the gypsy/traveller community.
2. Facilitating inter-agency dialogue
Building on the advocacy role of the health and care profession, comes the opportunity to gather wider professional groups or agencies to engage around the needs of patients and communities. Whether a local health centre or a hospital, the physical buildings representing health have a strong connecting power. They can become meeting places for important discussions. Effective multiagency working requires a multidimensional approach to an individual's needs that is person centred, outcomes focused and supports complex needs. Done well, the language of care focuses on the person in need of help, and deals with alleviating suffering rather than just sickness or disease. This furthers the case of ensuring that biometric and biographical care are considered in balance in order to provide a holistic response.
Money matters
Welfare advice and health partnerships (WAHPs) integrate local authority or third sector welfare rights and money advice services into healthcare services. Embedded in 150 GP practices across Scotland – including practices which cover our most deprived communities – welfare rights officers provide advice on income maximisation, social security, debt resolution, housing, and employability issues, as well as representation at tribunals. As a member of the multi-disciplinary primary care team, the Welfare Rights Adviser can access patient records with informed consent, to prepare medical reports for GPs to authorise. These reports are used to support applications for benefits and to help address debt, housing and employability issues.
Many people trust their GP, and placing WAHPs within Practices can help reach people with money worries and people who traditionally don't access mainstream advice services. WAHPs have the potential to reach people before they come to a crisis point which might otherwise have brought them into contact with traditional advice services.
In the first year, more than 8,000 people accessed the WAHP service, with twice as many appointments taking place in person compared to telephone discussions. The financial gain for people using the service has totalled almost £6.2 million. Encouragingly 85% of those accessing the service to date have been new users. WAHP are reaching people who have not yet engaged with traditional advice services. The Partnerships are helping to ease pressure on GPs and primary care services, allowing them to focus on the care and treatment of the people they care for while dedicated advisers support their social and economic needs.
3. Community wealth building as anchor institutions
The NHS can contribute to addressing these fundamental causes through its role as an Anchor institution, where the impact of the NHS on local economies can be harnessed to contribute to reducing economic and social inequalities.
The value of our institutions is not only in their physical presence but also in the people who work there, the links to other community institutions, and the use of land and assets for collective good. The NHS plays a key role in contributing to the employment of local people and the procurement of local services.
The NHS has the largest single budget controlled by the Scottish Government. Using this money to best effect to deliver high quality and effective healthcare, and to reduce economic and social inequalities, is critical.
Decisions about the location of services can ease access for patients and staff, facilitate active travel and use of public transport, and contribute to reducing inequalities. The actions in the NHS Scotland climate emergency and sustainability strategy support this through the use of Community Wealth Building tools towards a wellbeing economy. Finally, NHS organisations can work in partnership with local authorities and others to advocate for actions addressing the wider determinants of health inequalities.
Anchor institutions are large organisations which have significant presence in a local community, and significant power to distribute wealth and assets within that community through deliberate decisions to recruit and procure locally, and to ensure land and assets are used to the benefit of the local community.
They are called 'anchors' as they are deeply rooted in their community, having been in situ for a long period of time, and being unlikely to move in the near future.
4. Shaping policies that impact on wellbeing
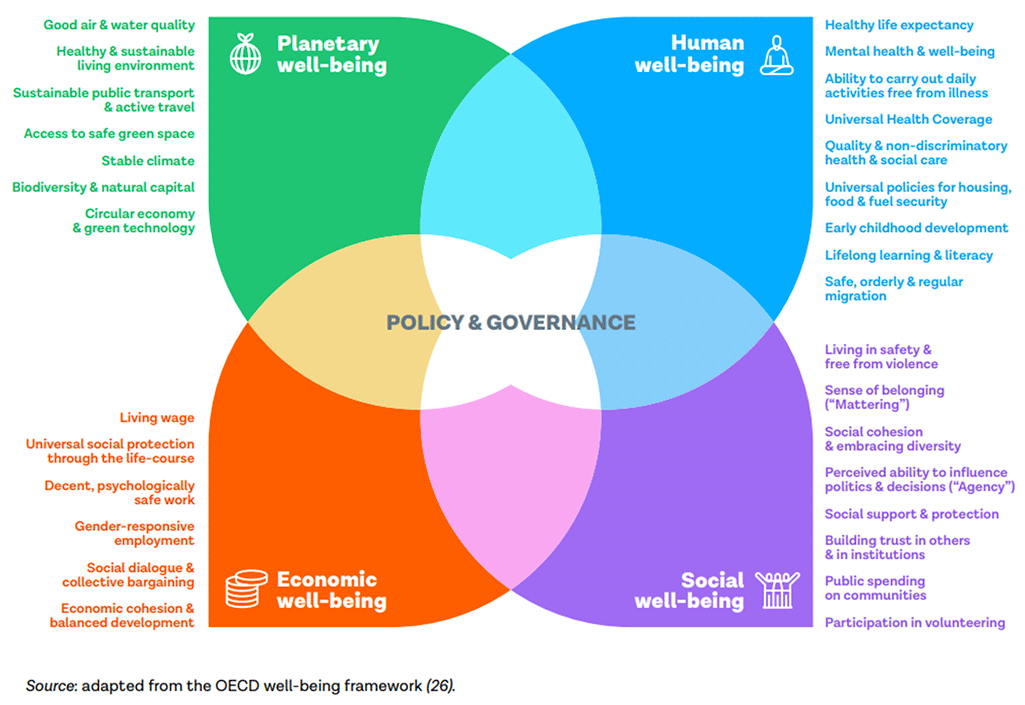
Scotland set out its aspirations to become a wellbeing economy in 2018, to create a thriving economy that works for everyone and promotes innovation and fairness. In this sense, wellbeing is defined as "living well" and is about "how we're doing as individuals, communities, and as a nation – and how sustainable that is for the future". This approach is being pioneered in Scotland in partnership with other Wellbeing Economy Governments around the world, including Iceland, Finland, Wales and New Zealand.
Wellbeing economies are economies that prioritise human, social, planetary, and economic wellbeing, which constitute the wellbeing "capitals". These include important assets such as trust, social cohesion, participation, environmental sustainability, and quality employment, which are crucial for developing healthy, fairer, and prosperous societies where people can thrive. Promoting population wellbeing is key to reducing the burden on health systems, to enable sustainable and resilient health care. This cannot be achieved in silos, and requires many sectors of our society working together to support each other. The move to create a wellbeing economy should help ensure economic policies contribute to achieving health and social outcomes in an equitable way. The NHS can play an important part in this by delivering appropriate, high-quality health services to populations with the poorest health, making full use of its potential as an anchor institution, and working with partners to help address the underlying fundamental causes.
This move to a wellbeing economy is reflected in the National Strategy for Economic Transformation and there are many different policies being developed and implemented to support this approach. These include: increasing the Scottish Child Payment to reduce child poverty; taking a Community Wealth Building approach in local authorities; implementing the Fair Work Framework to improve employment conditions; and increasing the range of assets in public and democratic ownership. Importantly, from a healthcare perspective, the health and wellbeing of individuals and communities become national indicators of the wealth of Scotland's people. As a country, we are investing in a transition to environmental sustainability and have committed to doing so in a way that tackles inequality.
A whole family approach
Glasgow has the highest levels of children living in poverty of any Local Authority in Scotland. Feedback from service providers and families suggests that the current support system is difficult to navigate for families and professionals.
Good quality early intervention and preventative holistic family support are essential to reduce preventable ill health, tackle the adverse effects of child poverty, and close the gap in life expectancy. General practice holds a unique position within communities as a provider and enabler of care and support, without stigma or referral criteria, and as an advocate for individuals and communities.
The Scottish Government is providing Glasgow City HSCP with funding, from 2023-2026, for a new programme of multi-agency Whole Family Support through General Practice.
Initially, the programme will be developed in a small number of deprived practices. As well as joining up existing services, the programme will introduce new family nurture and empowerment roles and other evidenced-based support for well-being services. It will include components for families with children from pre-school to secondary school age who are in/at risk of poverty and poor health outcomes, including:
- making every contact count, so that consultations with families do not just address the clinical issues presented, but are the starting point for social, psychological and economic support; and,
- outreach with families on practice lists who are not using or under-using primary care to ensure the right type of support for them. Outreach is critical as many who need care and support do not know how to, or cannot effectively, access services.
By working with families, the programme will address the health and wellbeing of children, parents and other caregivers, supporting people to remain socially connected (e.g. building links with community supports, helping them to maintain relationships) and economically active (e.g. helping people to stay well can help them participate in work). New multidisciplinary teams will be in place by autumn 2023 and the programme will be evaluated over 2023-26.
5. Building a Health in All Policies approach
This chapter has highlighted that the main drivers of health and health inequalities lie outside of healthcare – in fact, health is affected by policies and decisions in all sectors. This means that to improve health and reduce inequalities we need to work across policy areas to ensure all policies are designed to maximise benefits to health and prevent any risks to health. This is an approach called 'Health in All Policies'.
Policies to reduce inequalities in income, wealth and power are crucial, since health inequalities are unlikely to reduce without effective actions at this level. I am keen to see the development of Health in All Policies framing as we move through this period of NHS Reform and Recovery to a stronger preventative model investing in healthier populations at both local and national levels.
Health in All Policies is promoted by the World Health Organisation as a preventive approach that tackles the underlying determinants of health. A common way to achieve Health in All Policies is by applying Health Impact Assessment (HIA). HIA is a structured, partnership approach that uses public health skills and evidence to assess the potential impacts of policy proposals and identify changes that would improve these impacts. In Scotland, HIA has been used in policy areas including housing, transport and many others. Public Health Scotland has recently established a HIA Support Unit to build capacity to use this approach. I am keen to encourage my public health colleagues and wider partners to draw on this resource and to work together using the Health in All Policies approach more consistently. This will help us to create the positive building blocks needed to improve health and reduce health inequalities across Scotland.
Conclusion
Recognising the role that healthcare plays in tackling health inequalities is essential, but it is only the first step in realising the potential and opportunity for improvement offered by collective and collaborative action across the whole system. It would be easy to become pessimistic in the face of these challenges, but there are significant opportunities for the Scottish Government and other public and private organisations in Scotland to achieve important shifts in the trends of health inequalities. In moving from our current position, it is imperative that each of these sectors and organisations realise the contribution that they can make individually and collectively to reducing structural inequalities that persist across the country. Only by doing this, and by reducing the alienation of those communities and people who have not yet been fully reached, will health inequalities begin to reduce across Scotland.
Contact
Email: realisticmedicine@gov.scot