Realistic Medicine - Doing the right thing: Chief Medical Officer annual report 2022 to 2023
Chief Medical Officer's (CMO) third annual report, and the seventh on Realistic Medicine. It reflects on the challenges our system is facing and asks professionals to practise Realistic Medicine, in order to deliver value based health and care and a more sustainable system.
Chapter 2: Value Based Health and Care
Introduction
In my opening chapter, I spoke about the four concurrent and interlinked challenges to population health in Scotland. The persistent threat of infection and antimicrobial resistance; the ongoing challenge of improving health with widening disparities at a time of pandemic recovery and rising prices of energy and food; the sustainability of health and social care services to meet not only current demand but that projected by demographic changes to the burden of disease in Scotland over the next 20 years; and the reality of the climate emergency impacting now and falling disproportionately on those who already experience disadvantage in our society.
Our health and social care services are rightly valued by all in Scotland. In recent years, colleagues across health and social care have adapted to the ongoing challenges of the COVID-19 pandemic and every day I see dedicated people continuing to work extraordinarily hard to make a difference and relieve suffering felt by others. However, there is an urgent need to do things differently if we are to be successful in addressing these interlinked challenges and we really wish to improve the lives of the people we care for. It's time to fully adopt practising Realistic Medicine as the way we can contribute to a healthier, more sustainable, fairer Scotland.
The OECD estimates up to 20% of healthcare spending adds no value to those receiving it. To put it another way, up to one fifth of our healthcare resource is potentially wasted and prevented from being used to address unmet clinical need elsewhere. This is a sobering statistic that I have mentioned before, but it is central to reinforcing why we must do things differently. We all recognise waste in our day to day work, for example in prescribed medicines which were not taken, in appointments which were not needed, and in travel to hospital which could have been by video or telephone call. This waste can impact directly on the people we serve, on their time spent accessing healthcare and in the potential harm and suffering from some interventions. This waste also significantly impacts on our environment through the depletion of natural resources, the manufacture and use of unnecessary drugs or emissions from unnecessary travel.
Practising Realistic Medicine to deliver Value Based Health and Care
Health and care systems across the world are thinking about how they can deliver Value Based Health and Care (VBH&C) which focusses on achieving the outcomes that matter to people while using resources wisely.
"Value Based Health and Care delivers better outcomes and experiences for the people we care for through the equitable, sustainable, appropriate and transparent use of resources."
By practising Realistic Medicine we can deliver VBH&C. Through shared decision making we can deliver person centred care. We can support people, and their families, to feel empowered to discuss their treatment options and the associated risks and benefits. We can help manage expectations and enable people to make informed choices, based on what matters to them. Sometimes they might choose different treatments which offer greater personal value. In other cases, they may choose less or no treatment, which helps reduce wasted resources. By identifying and tackling unwarranted variation in health, treatment and outcomes, we can also ensure equity of access for those who need our help the most.
Scotland's Vision for Value Based Health and Care recognises the vital role health and care colleagues play in fostering the culture of stewardship. It's crucial that we focus on achieving the outcomes that matter to the people we care for, reduce waste and improve equity of access to services for our most disadvantaged communities.
I have been greatly encouraged by the support shown by colleagues across the health and care professions for the Vision for Value Based Health and Care that I set out. Its positive reception shows that there is both a recognition of the need and an appetite to act – to do things differently. Through careful and kind care, the pursuit of doing the right thing, it becomes possible to liberate this vision of care and the more sustainable system we all wish to see. I also expect that it will sustain us as professionals too, by reconnecting us to our purpose, helping us provide the kind of care we would like to see and reducing the risk of moral injury.
Inspirational leadership and support
Doing the right thing involves ensuring every health and care professional has the tools to practise Realistic Medicine every day. Delivering our vision will require collaboration and consensus from senior leaders across our health and care system and the ability to provide the data, analytical skills, education, training, measurement and improvement support required to foster the culture of stewardship we need to deliver better value care.
There are already encouraging signs of this collaboration becoming evident. NHS Education for Scotland (NES) have been an important partner in the Realistic Medicine journey and are keen to support development, delivery and access to educational resources, training and tools that are fundamental to practising Realistic Medicine and delivering Value Based Health and Care. I have seen, up close, the commitment of the senior leaders within NES, including the non-executive team, and was extremely encouraged by their enthusiasm and support. We have discussed:
- the possibility of developing and delivering system-wide senior leadership training on Value Based Health and Care and why it matters. This might include training for non-exec directors in NHS Boards to help them fulfil their responsibilities; and,
- NES working with undergraduate and post-graduate education providers to explore whether they can do more to promote Realistic Medicine and Value Based Health and Care in their curricula.
I look forward to seeing NES make further progress in these areas. Meantime, NES has also developed a shared decision making in practice module to support staff across Scotland to apply the principles of Realistic Medicine and shared decision making in their daily working lives. All NHS Boards have been asked to ensure that health and care colleagues complete this training and if you haven't already, I would strongly encourage you to do so.
NES and our delivery partners are also working with the Right Decision Service to develop two new apps that will house the information, training and education resources required to support both professionals and the public to practise Realistic Medicine and both should be ready to use later in 2023.
Shared decision making
Our ambition is to deliver the outcomes that matter to people while optimising the use of available resources. To do this, we must meaningfully involve people in decisions about their care. This excellent example from NHS Lanarkshire shows how shared decision making helps people make better choices about their care:
Understanding complexity and sharing decisions.
The Shared decision making clinic at Hairmyres Hospital has been running for almost 2 years and is helping people make informed choices about their preferred treatment. This case study demonstrates the benefits of the BRAN questions approach, used at the clinic, and focuses on Lorna who has Breast Cancer:
What the surgeon said about Lorna and her treatment options in their referral:
Benefit: Surgery might offer Lorna curative resection of her cancer.
Risks: She will have a 1-5% risk of dying due to this procedure.
Alternatives: If Lorna was not considered suitable for an operation due to her underlying health problems, we could manage her cancer with primary endocrine therapy and still consider surgery further down the line if there was an opportunity for pre-habilitation.
What would happen if Lorna chose not to have surgery?: Lorna has an oestrogen receptor positive breast cancer, which we can potentially control with endocrine therapy. In the long term, data shows patients do better if we operate, but we would potentially be able to keep her breast cancer under control for a number of years on medication alone.
What Lorna said about us: I was worried that my health conditions might make surgery a high risk option for me. They sent me some papers in advance to explain what Shared Decision Making was. I had a breast biopsy which confirmed cancer and I thought I needed an operation. I answered the questions in the letter. This was the way I saw things before I came to the clinic:
Benefit: Surgery might mean becoming cancer free.
Risks: None. I am aware that my COPD and obesity are risk factors during surgery, but I wasn't sure why.
Alternatives: Chemo. Also a new treatment to shrink tumours? – I have seen this on TV.
What would happen if I chose not to have surgery?: I would go through a very lengthy treatment with lower success rate. My chances of becoming cancer free would be less.
My healthcare professionals introduced themselves and we sat in a triangle and shared information. I told them what was important to me and they explained things to me in a way I understood using graphs and pictures, including what the complications of surgery might mean for me.
When they said that my other health problems, in particular my COPD, might lead to a loss of function and independence following surgery - should I come through it ok - this was the trigger for me to opt for hormone treatment instead. I am alone and have no-one to help look after me while I recover. This clinic really helped me understand my options and remain calm.
I would push doctors to help patients who are perhaps not outgoing to please ask these questions, because they really do want to talk like this and it can help you decide what treatment is best for you.
I ask that you encourage the people you care for to use the BRAN questions, so they can be sure of the benefits, risks, alternatives and what might happen if they choose to do nothing, when weighing up their care options. The BRAN questions help people make better decisions about their care, which helps us to optimise resources and reduce waste.
- What are the Benefits?
- What are the Risks?
- What are the Alternatives?
- What if I do Nothing?
Through work supported by the Centre for Sustainable Delivery we are supporting health and care practitioners to practise shared decision making early in care journeys using active clinical referral triage (ACRT) and patient initiated review (PIR). In collaboration with patients, ACRT means information is offered to patients to support their decisions around investigation and treatment, and provision of specialist care is tailored to those who will benefit from it. Patient initiated review offers support for patients to seek further care only when they need it. This reduces waste from routine, often unnecessary, follow up appointments – it respects patients' and clinicians' time, optimises resources and reduces the environmental impact by avoiding unnecessary travel.
National adoption of active clinical referral triage (ACRT) and patient initiated review (PIR)
NHS Boards have been implementing active clinical referral triage (ACRT) and patient initiated review (PIR) for a number of years, but the evidence of impact has previously been captured only at a local level. Using the Centre for Sustainable Delivery's Heatmap approach, it is now becoming possible to understand the benefit of these programmes in six key specialties: Dermatology, ENT, General Surgery, Gynaecology, Orthopaedics, and Urology.
ACRT involves a senior clinical decision maker reviewing referrals at the beginning of a person's wait to establish their most appropriate care pathway. While many people benefit from alternative services, receiving information about their condition or investigations while they wait to improve their health, the Heatmap focusses on people who will not benefit from secondary care.
Between April 2022 to March 2023, these six specialties have managed almost 66,000 referrals by returning to primary care with appropriate advice for people that provides benefit beyond waiting for a clinic appointment, or given the opportunity to 'opt-in' to a secondary care pathway if their condition or circumstances changed. A conservative estimate of providing those 66,000 appointments in NHS services is almost £10 million, based on a £150 per outpatient appointment estimate. This resource can now be used to provide higher value care.
In patient initiated review (PIR), instead of offering people routine return appointments, they are advised how they can quickly come back to secondary care services if and when they need to. While this approach is not appropriate for every person, in the six specialties almost 43,000 patients were added to discharge PIR pathways between April 2022 to March 2023, putting them in control of their own care and increasing access when they need it.
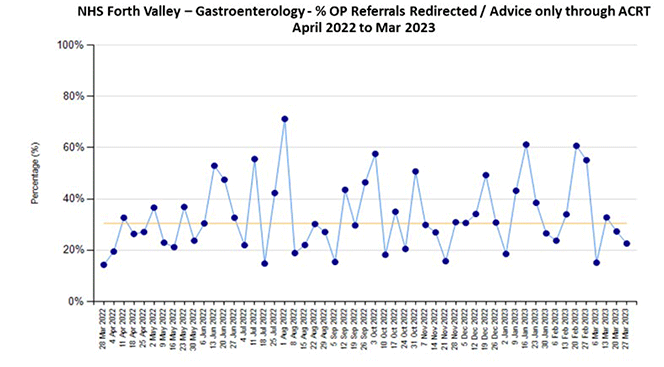
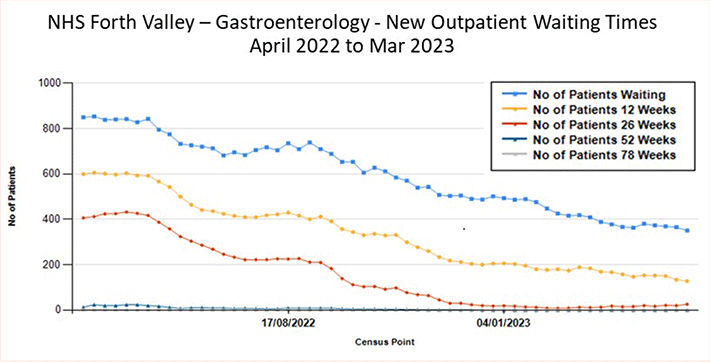
Case study: NHS Forth Valley Gastroenterology ACRT
The Gastroenterology team in NHS Forth Valley have implemented ACRT over the last few years. They consistently average around 30% of people referred being redirected to more appropriate pathways (Fig 1,) and as a result free up capacity in clinics for those people who need them most. The impact has been a 50% drop in the waiting list and 66% drop in waiting times providing quicker access to assessment and treatment for patients. (Fig 2)
Case study: Breast pain pathway
Through 2022/23 the introduction of the breast pain pathway across NHS Fife, Lanarkshire and Forth Valley, showed that 82% of people were able to avoid a face to face appointment and unnecessary imaging, saving them time as well as being able to access more appropriate advice and care. This has enabled waiting times to reduce for urgent suspicion of cancer patients from 7 weeks to under 2 weeks, and from 18 weeks for a routine referral to under 4 weeks. As a result NHS Forth Valley have been able to offer mutual aid capacity to three surrounding NHS Boards.
Outcomes that matter
To deliver high value care we need to ensure we deliver outcomes people value. Personal value means people and families are involved in decisions about their care by health and care professionals who understand and respect what matters to them.
The outcomes that people value
1 in 8 of us cares for someone, and there should be no barriers to getting support, recognition, and quality of life. Improving the Cancer Journey service is part of Transforming Cancer Care, a partnership between Scottish Government and Macmillan Cancer Support which aims to make Scotland the first country in the UK where all cancer patients have access to a key support worker who can provide dedicated financial, practical and emotional support.
Anna was 37 years of age. She was terminally ill. Anna's brother and her sister in law agreed to take kinship care of her 7-year-old son once she passed. With a Link Worker's help, Anna's sister in law was able to consider the challenges ahead and how to deal with them.
A holistic needs assessment (HNA) was completed in partnership with Anna's sister in law. This plan tackled the issues this family faced one by one:
- the Beatson's Specialist Health and Work Service (SHAWS) provided employment advice, and liaised with the carer and her employer, to let them know about rights and entitlement;
- the local Macmillan Advice Works team helped secure benefits allowing the carer to reduce her hours to help care for the child;
- Cancer Support Scotland provided six free sessions of counselling for the carer, to help her come to terms with the situation;
- the Kinship Care team provided the carer with additional funding and the family were supported to move house to accommodate Anna's son; and
- the Macmillan Free Will writing service created a free will for the carer along with resources on helping prepare a child for loss.
Our ICJ service has helped identify over 1,000 people affected by cancer in Renfrewshire with financial difficulties and on average helped raise their income through benefit and employment support by £1,500 per head. In all, the annual total income gain is £1.5 million in three years of service.
"Hi Karen, thank you so much for being the person that you are, honestly my world is pretty grim right now and to know I have you is more than you know right now."
Anna's sister in law
We also need to get better at measuring the outcomes that matter to the people we care for. Historically we have been good at counting episodes of care such as numbers of people admitted to hospital or procedures undertaken. In addition we have mechanisms to measure quality of care but quality is often based on reports generated by the care providers rather than those who have experienced care. We want to make better use of measures of care and outcomes reported by people receiving care. There are areas where good progress has been made to develop and collect patient reported outcome measures or person reported experience measures (PROMs and PREMs). One of the commitments in our Vision for Value Based Health and Care is to promote the measurement of outcomes that matter to people and explore how we can ensure a coordinated approach to their development and implementation. In the future, it may even become possible to evaluate empathy and compassion in consultations and workplace environments using artificial intelligence and sensors that interpret sound waves and body language – innovation that will begin to revolutionise the way we evaluate quality of interaction when providing care.
Unwarranted variation and equity of access
We know provision of health and care can and should vary according to the needs of the population or individuals we care for. But we also know that at times there is variation in care which can't be explained by the needs of the people we care for. Over-investigation and overtreatment lead to unwarranted variation in health, treatments and outcomes, potentially cause harm (all healthcare has risk), and waste precious healthcare resources, which could be better used elsewhere.
There is also underuse of some high value tests and interventions. Failing to deliver care where it is needed can be just as harmful and wasteful as too much treatment and care. This is often linked to inequality of access to services. Failure to deliver the right care, when and where it's needed, contributes to low value health and care because we miss the opportunity to improve outcomes.
Examples of low value care include prescribing of branded drugs where generic drugs are equally effective, or the use of a surgical approach to musculoskeletal problems when physiotherapy will deliver better outcomes with less risk. In many instances a non-medical intervention, for example weight loss or stopping a harmful behaviour, such as smoking, may be the best choice. Evidence Based Practice sits at the heart of Value Based Health and Care, marrying the scientific evidence, professional judgement and patient preference together in balance.
Scottish Atlas of Variation
The Scottish Atlas of Healthcare Variation highlights unwarranted variation in care across Scotland. In 2022, we refreshed maps showing variation in a number of planned care procedures across Scotland and asked health boards to tell us how they used these data to tackle overprovision and underprovision of care.
Scottish Atlas of Healthcare Variation December 2022
Some NHS boards have provided very good feedback on how they used these maps to inform improvement. The Atlas has real potential in supporting professionals to tackle unwarranted variation, however the support structures and processes need to be strengthened to ensure consistency of adoption and impact across the country. In the short term, we will work with Public Health Scotland to :
1. Produce maps that support the areas of national clinical priority such as helping to reduce waiting times.
2. Seek to reduce over-investigation in radiology; radiologists have expressed concern about possible over-testing using some investigations. We will work with them to identify lower value investigations and explore whether we can produce maps that help local clinicians to understand better where overtesting might exist. We expect that supporting improvement activity will reduce over-testing and reduce waste and potential harm.
3. Develop and deliver training and education for clinical teams to help them interpret Atlas data.
4. Develop and implement a formal structure of support from the Centre for Sustainable Delivery to help local clinical teams identify and tackle unwarranted variation.
In the longer term, I expect the Atlas will become an essential tool in achieving higher value care by helping health and care colleagues reflect on their practice and identify unwarranted variation in health, treatment and outcomes across our health and care system.
Sustainability in health and care
The construct of value in health and care includes personal value, with outcomes that matter to individuals. However, our health and care systems are also responsible for planning and delivering care for larger communities, and we call this population (or allocative) value. Population value includes the promotion of health and wellbeing and prevention of ill-health. When we plan for communities we take into account technical value which considers aspects of care provision such as procurement, where we strive to get the best available and effective treatments and devices at the lowest cost. In addition to personal, population and technical value we should also consider the impact of health and care on our wider society, including the environment. We call this societal value.
The climate emergency is a population health crisis, the biggest threat to our health of our time. It significantly impacts societal value because changes to our climate and environment significantly impact on the social and environmental determinants of health, for example, directly through air pollution or extreme weather events, and indirectly due to changing patterns of disease such as vector borne infections. The NHS is a significant utiliser of natural resources and emitter of CO2 and by reducing our carbon footprint we can positively influence societal value not just for now but for future generations.
No matter our role within our health and care system, all of us share the responsibility to limit the impact of the way we practise on our planet and help to address the climate emergency. Efforts must be accelerated to cut greenhouse gas emissions from Scotland's health and care system and become environmentally sustainable. We know too the difference that practising Realistic Medicine can make to reducing waste and optimising use of resources. This year saw the launch of the National Green Theatres Programme which represents the upscaling of the Green Theatres Project from NHS Highland that I presented in my 2020-2021 Annual Report. I'm delighted to highlight this again as an example of environmental sustainability being prioritised to deliver of high quality sustainable healthcare.
Sustainable healthcare in action
Up to 80% of the carbon footprint of the NHS is due to clinical pathways, of which surgical theatres are the most carbon intense part of the hospital and responsible for a huge amount of single-use plastics and pharmaceutical waste.
The National Green Theatres Programme (NGTP) launched in March 2023, is a nationwide development of a pilot project from NHS Highland which recognised that, for healthcare professionals, our work environment could be the main source of our carbon footprint. Grassroots action by a group of committed clinicians on anaesthetic gases, spread by Green Anaesthesia Scotland (GAS) had already delivered a significant reduction in the greenhouse gas emissions from Scottish hospitals. They then developed an Ideal Green Theatre, and looking at pharmaceuticals, systems, equipment and practice asked "What is the best way to provide safe and effective surgery utilising the least resource?"
NHS Scotland climate emergency and sustainability strategy 2022-26 has helped formalise the Green Theatre Programme. Hosted by the Centre for Sustainable Delivery (CfSD), it is focusing on around 50 actions that will help to address carbon emissions, single-use plastics waste, air pollution and pharmaceutical contamination. This work involves collaboration with colleagues in Infection, Prevention and Control, Engineering, Pharmacy, Procurement and Finance, with assistance provided by CfSD if required.
The innovation arm of the NGTP has been developed with the Medical Devices Manufacturing Centre at Heriot-Watt University, accessing and supporting many small start-up companies keen to develop new tools and ways of working with healthcare providers. Pilot projects include the provision of sterile water, removal of microplastics and pharmaceuticals as well as recovery of heat energy from laundry waste water, and a more efficient and low energy system for cleaning surgical instruments.
The National Green Theatre Programme clearly has an important role in helping to embed environmental sustainability in clinical and managerial decision making across NHS Scotland.
Managing risk better
We know that over-investigation and over-treatment can cause harm as well as being wasteful of our healthcare resources. Realistic Medicine encourages us to recommend investigations and treatments that add value, minimise waste and to personalise our approach to what matters to the people we care for, involving them fully in decision making.
One perceived barrier to practising Realistic Medicine, and one that I hear often, is the worry that professionals will be criticised for not offering all available treatments to patients, no matter the judgement of their individual relevance.
To reduce the risk of complaints, some doctors recalibrate their practice by carrying out extra tests and procedures, perceiving that patients are more satisfied when they get extra tests or treatment. This is known as defensive medicine. Primarily, the aim of practising defensively is to protect the doctor rather than to encourage best practice. We have already noted that not all tests, treatment and procedures improve patient outcomes, and what is more likely is that increasing their volume adds to the likelihood of medical errors occurring. For example, a 2019 study found that preventable patient harm affects at least one in 20 patients in a medical care setting, and that harm was mostly related to drug incidents, therapeutic management and invasive clinical procedures.
There is clearly anxiety in parts of the NHS about whether practising Realistic Medicine exposes clinicians to medicolegal action and complaints which might otherwise not arise. In this blog, Michael Stewart, Head of Central Legal Office discusses the relationship between Realistic Medicine and consent. A summary of Michael's advice follows:
The best prophylactic to an informed consent claim is a robust shared decision making process which:
1. puts the patient at the centre of decisions made about their care;
2. encourages clinicians to find out what is important to the patient;
3. treats the patient as an equal partner; and
4. engages the patient in decisions about treatment options to make sure that they are able to decide what is right for them,
It is a process which should encourage people to take responsibility for their own care. It is also a process which the law requires. The Supreme Court justices described such an approach as one which:
'instead of treating patients as placing themselves in the hands of their doctors (and then being prone to sue their doctors in the event of a disappointing outcome), treats them so far as possible as adults who are capable of understanding that medical treatment is uncertain of success and may involve risks, accepting responsibility for the taking of risks affecting their own lives, and living with the consequences of their choices.'
Of course, not all patients will take responsibility in this way. Complaints or actions will continue to be made, many of which may have a legitimate basis. But if appropriate care has been offered or provided using a framework for shared decision making or consent, the validity of that complaint or claim when tested is more likely to fail. In this respect, it is especially important to consider how you can evidence that such a conversation took place.
To the extent that either a consent form or a contemporaneous entry in the records are important means of proving that informed consent took place, it is important to be fully aware of the test for informed consent following Montgomery (a test which is reflected well in the BRAN (Benefits, Risks, Alternatives, do Nothing) questions used by practitioners of Realistic Medicine). The test requires the clinician to make the patient aware of 'any material risks involved in any recommended treatment, and of any reasonable alternative or variant treatments.' It is not enough just to narrate the nature of the risks and benefits of the treatment provided; you should also say something about any reasonable alternative treatments, including the option of doing nothing.
Reflecting on the nature of claims that are frequently seen by Central Legal Office, clinicians are effective at describing the risks of the proposed course of treatment (both during the consenting process and when describing that process in the consent form), but describing the risks and benefits of other treatments is perhaps less well articulated. And it's not difficult to understand why this is so. Time is one of the scarcest resources in healthcare and talking about different treatment options or exploring with the patient whether it makes sense for them to have treatment at all (and then recording that discussion) all take time. However, the conversation itself, and the record that it took place, are the best protection against successful actions being raised.
Michael's legal perspective is important and I welcome his advice. It aligns with doing the right thing, both in the way we should support the people we care for to make an informed choice about the care that is right for them, but also in legal terms. Understanding people's preferences does not mean that we always give people what they want, because we know that there are times when it may not be appropriate or practical for us to do so. This is where consideration of the evidence and our professional judgement becomes important in the conversation. But we should always consider what matters to them and try to compassionately understand how their health and wellbeing fits into the broader context of their lives.
Of further interest when considering the four domains of value in this context, evidence shows that if people are fully informed about the risks and benefits of their treatment options they often choose less treatment, or more conservative treatment.
Conclusion
Modern health and care systems are facing considerable challenge to remain sustainable as practice becomes more intense, wider in scope and necessary for longer as people live more years in ill health. By extending healthy life expectancy and focusing on the prevention of disease, we can preserve the fundamental purpose of universal provision, and remain accessible to all in the longer term. Practising Realistic Medicine is part of how we can work together to support people to live more years in good health, reduce inequalities in health, and support recovery and renewal of services across Scotland. That's why Realistic Medicine, with its focus on delivering Value Based Health and Care, continues to be threaded throughout Scotland's Health and Social Care policy. Six commitments will help us deliver our vision for Scotland. We must:
1. Continue to practise Realistic Medicine as the way to provide higher value care and reduce harm and waste.
2. Continue to engage with the public to promote understanding of Realistic Medicine and its benefits for them and for Scotland. We will work to empower people to be equal partners in their care, through shared decision making, enabling self-management, and promoting health literacy and healthy lifestyle choices.
3. Promote outcomes that matter to the people we care for and explore how we can ensure their proportionate measurement for further improvement.
4. Continue to develop and use effectively tools that enable us all to seek out and eliminate unwarranted variation in access to healthcare, treatment and outcomes.
5. Support the provision of sustainable care in line with the NHS Scotland climate emergency and sustainability strategy by addressing inequalities, promoting greener care pathways and reducing waste and harm; and,
6. Continue to build a supportive and enabling community of practice with a culture of stewardship across Scotland.
To do this, we will continue to collaborate widely, developing an action plan that describes how NHS Scotland will deliver these commitments. Work on the action plan is underway and I expect to publish this in Summer 2023. Meantime, it is important to emphasise that we are not starting from scratch. Value Based Health and Care is already being provided in areas across Scotland and the Vision provides excellent examples of good practice. Many of these I've already had the opportunity to see up close during visits to services, hearing directly from colleagues and the people they care for about the difference it is making. This enthusiasm, to show and celebrate the success of local achievements, has been, for me, a highlight of the last twelve months. We need to build on them, support each other to practise Realistic Medicine and accelerate the provision of this type of care consistently across the country. By doing so, we'll develop the compassionate, sustainable and equitable health and care system that we want and need.
Contact
Email: realisticmedicine@gov.scot