Realistic Medicine - Doing the right thing: Chief Medical Officer annual report 2022 to 2023
Chief Medical Officer's (CMO) third annual report, and the seventh on Realistic Medicine. It reflects on the challenges our system is facing and asks professionals to practise Realistic Medicine, in order to deliver value based health and care and a more sustainable system.
Appendix 1: The Health of our Nation
Introduction
Good health can allow people to more easily play an active role in their communities and the economy, promoting prosperity and enabling individuals, communities, and society to flourish. As set out in the introductory chapter, several challenges currently pose a threat to our population's health and healthy life expectancy. A recurring but important theme has been that of health inequalities, which are widening and require urgent action to be taken.
This appendix describes the health of our nation using select data and intelligence on the burden of disease. It briefly summarises some of the key negative and positive drivers of our population's health, concluding with some headline "calls to action". It is not exhaustive in its representation of available data, but serves to illustrate some key points that are worthy of noting.
Is our health improving or getting worse?
As described in an earlier chapter on health inequalities, life expectancy has begun to decline for those living in our most deprived areas. Similar trends are observed in healthy life expectancy, which captures the number of years lived in good health, helpfully distinguishing quality from quantity of life.
Overall healthy life expectancy increased markedly between 1995 and early 2010s, but then declined by approximately 2 years between 2011 and 2019. A greater decline (of around 3.5 years) was observed among people living in the 20% most deprived areas. Women in the most deprived fifth of areas are now estimated to live fewer than 50 years in good health, compared with over 70 years in the least deprived areas (Figure 1).
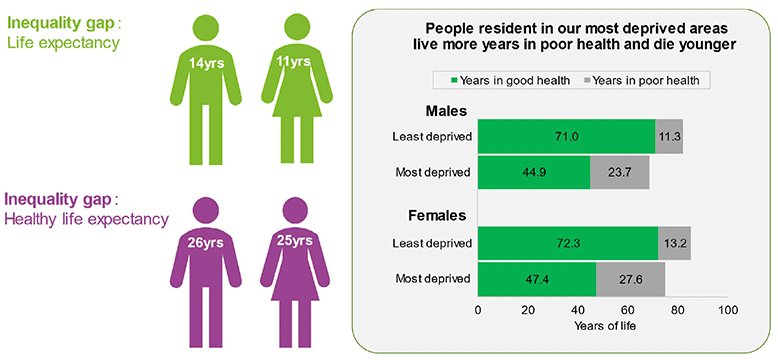
Source: National Records Scotland
What health conditions affect our population?
To understand what is preventing people in Scotland from living longer lives in better health, we can look at those conditions causing the most "healthy years of life lost" to ill health and early deaths. This can be measured using Disability-Adjusted Life Years (DALYs). Figure 2 shows the fifteen conditions causing the highest number of DALYs in Scotland in 2019. It shows in red the size of the burden that is attributable to deprivation – this is the reduction we would see if everyone experienced the same mortality and morbidity as those in the least deprived fifth of the population. It can also be seen that many of the leading conditions in 2019 – heart disease, drug use disorders, lung cancer and chronic obstructive pulmonary disease – were also the leading drivers of absolute and relative inequalities in the disease burden.
Areas coloured red show the size of the burden that is attributable to deprivation
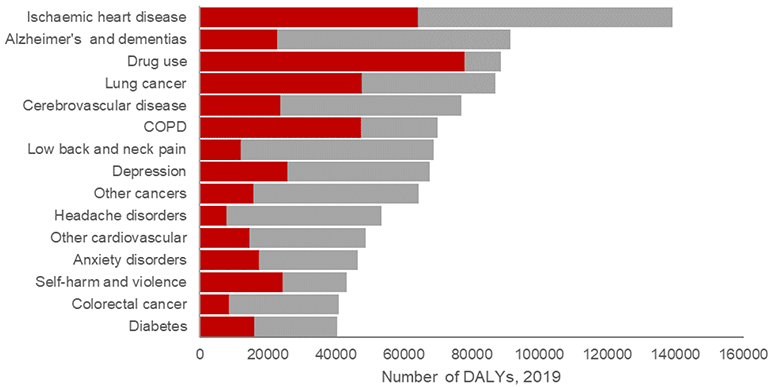
Source: Pre-pandemic inequalities in the burden of disease: a Scottish Burden of Disease study, Wyper et al.
Ischaemic heart disease contributes the most to disease burden with around 7% of men and 4% of women in the 2021 Scottish Health Survey reporting they had ever had IHD. Cancer is also an important cause of morbidity and mortality; currently for the lifetime risk of developing cancer, it is estimated that 2 in 5 (40%) people in Scotland will be diagnosed with some form of cancer. These diseases are linked to Scotland's high prevalence of associated risk factors, including smoking, poor diet, and physical inactivity. In addition, mental health conditions such as anxiety and depression substantially contribute to Scotland's poor health with recent analysis indicating that levels of psychological distress have been worsening since around 2015 in the working population.
Of significant increasing concern is the steep rise in drug misuse deaths from 6.2 per 100,000 in 2001 to 25 per 100,000 in 2021. This has been driven by the increase in deaths in the most deprived areas to 64.3 deaths per 100,000 people in 2021, which is over 15 times higher than in the least deprived areas.
What is negatively affecting our health?
Austerity and cost-of-living
The economy matters for population health. From 2012, average mortality rates and life expectancy in Scotland (and many high-income countries) stopped improving. Mortality actually increased and life expectancy declined for people in our most deprived areas. Over the last ten years there has been growing unease about the long-term health implications of the global economic recession following the financial crisis in 2008, and the subsequent austerity measures implemented in many countries. National responses to this major economic downturn varied substantially but, in many cases led to extensive reductions in public expenditure, including cuts to central and local government budgets, welfare services and benefits.
This is of course compounded by recent price inflation that has substantially increased the cost of living. Rising energy and food bills are seeing people having to make difficult choices about how they spend money, with healthier choices, such as affording to do recreational activities or buying fresh produce, often made more challenging or impossible. Adverse mental health consequences from the increased cost of living have also been reported, with a recent poll of Scottish adults showing one-third feeling stressed when thinking about their financial situation in the past month and three quarters being concerned about not being able to maintain their standard of living. Significantly, more than half (52%) of adults in Scotland were at least a little worried about being able to afford food over the next few months, rising to 69% of those aged 18 to 34.
COVID-19
The pandemic has accentuated the circumstances negatively impacting our health. The unintended but unavoidable consequences of the measures introduced to manage the COVID-19 pandemic has negatively impacted the population's social and economic circumstances. This has included loss of income or employment, disruption to education, and reduced social contact and support across our communities. Changes in the ability to play freely and be active, and in access to healthy foods may have contributed to the increase in the risk of obesity seen among Primary 1 children in 2020/21, which although improved had not returned to pre-pandemic levels in 2021/22. People were also not affected equally. During the UK-wide lockdown in early 2021, a survey showed that young adults (18-29), compared to other age groups, reported the highest levels of distress, the highest levels of loneliness and the lowest life satisfaction scores. A study of the mental health and wellbeing of students within Scottish colleges suggests the effects on mental health wellbeing are continuing.
During the early phases of the COVID-19 pandemic there was a substantial decline in the number of people who received most types of healthcare (including cancer diagnoses, primary care monitoring of chronic diseases, planned operations, screening programmes, dental check-ups etc). Much of this decline was to create capacity within healthcare settings to deal with people who were seriously ill from COVID-19, and this likely saved many lives as a result. However, it is also likely that many people who would otherwise have benefited from healthcare did not, either because they felt that they shouldn't be a burden on services, or because services became less accessible. This meant that a substantial amount of unmet healthcare need built up in the population. Some of this is now seen in waiting lists for treatment, but some also will be appearing as people with more advanced disease and conditions than would otherwise have been the case. For example, reductions in the take up of blood pressure medication may have contributed to a higher than expected number of deaths from cardiovascular disease.
What is positively affecting our health?
Minimum unit pricing
Scotland was one of the first countries in the world to legislate a minimum unit price for alcohol. Following its introduction in 2018, alcohol use in Scotland has fallen. Implementing alcohol minimum unit pricing legislation has also made a positive contribution to tackling deaths, and inequalities in, alcohol-related health harms, although the scale of harm remains high and entirely preventable.
Reduction in smoking prevalence
Smoking prevalence in Scotland has fallen to its lowest ever level (11% of the adult population). Yet inequalities persist. Just 5% of adults living in the least deprived areas of the country smoke, compared to 24% of those living in our most deprived communities. Scotland has implemented world leading tobacco control legislation for over a decade, including banning smoking in public places, putting tobacco out of sight at point of sale and banning smoking in prisons. As a result, we have seen massive improvements in smoking in pregnancy and large falls in the exposure of children to second hand smoke with consequent positive impacts on infant and child health.
In 2021, the proportion of children exposed to second-hand smoke in their own home was significantly lower than in previous years
- 12% in 2012
- 6% in 2019
- 2% in 2021
Source: Scottish Health Survey 2021.
Prevention and early intervention
There are many examples of preventative actions that have already helped achieve major improvements in health. For example, the Human Papilloma Vaccine (HPV) has reduced the development of high-grade cervical abnormalities (a pre-cursor of cervical cancer) by 89% and Scotland's Childsmile programme has halved the rates of tooth decay in children since 2003.
What can we do to improve our health?
The causes of ill health are indeed complex and inter-related so there will be no simple solutions or quick fixes. We also know that on account of our ageing population, the overall burden of disease is projected to increase. Therefore, accepting the status quo is untenable for our health and care services which are already pressurised. To do nothing is a choice, and one that we cannot allow to become the default. Throughout this report I have indicated what we can do to change our current course and the key actions are summarised below.
Invest in prevention
A strategic and systematic approach to embedding prevention across the health and care system is needed. This will not only enable people to live healthy fulfilling lives but is essential to ensure the future sustainability of the health and care system. For this reason, the Preventative and Proactive Care Programme is a key component of our National Care and Wellbeing Portfolio.
Health in all policies
As illustrated throughout this report, healthcare is not the main contributor to population health with other policy areas playing a greater role. To improve future health and reduce future demand it is important that we ensure decisions in all other policy areas, be it housing, fiscal or employment, are designed to support good health, including mental health. This approach is key to enabling us to improve the wider determinants of health.
Leave no-one behind
Although deprivation is inextricably tied to poorer health outcomes, the needs of populations with other protected characteristics should also be considered or they too risk being left behind. These include persons with disability, ethnic minorities, older people, children and the homeless. Scotland's Equality Evidence Strategy will help deliver better equality evidence that is essential to informing our understanding of what is happening in the lives of all of Scotland's people, helping the people who need it most. Evidence has also emerged that young to middle-aged men in Scotland may be particularly vulnerable due to their declining engagement with health services and greater risk of poor future health through reduced earnings potential.
Take a life-course approach
Early childhood development and the school years play a crucial role in determining future health, and are affected by a range of influences including biological factors and social, environmental, and economic conditions. Improvements and reductions in inequality in child development are possible through action across these influences, including health in pregnancy, family income and access to parental leave, early years education and surveillance and targeted intervention for developmental concerns.
Reduce health harms
As seen with minimum unit pricing, positive health changes are possible over a short space of time when working with the private sector to reduce the price of and availability of unhealthy products. Addressing the commercial determinants of health has potential to impact a wide range of risk factors affecting health, from policies to prevent gambling harms to reducing marketing and access to high fat, salt and sugar foods and drinks.
Improve healthcare delivery
Now, more than ever, there needs to be a focus on ensuring services are used equitably and sustainably to meet the needs of the people of Scotland as well as those of our future generations. As our system recovers from the pandemic our primary focus must continue to be on achieving outcomes that matter to the people we care for. Our vision for delivering Value Based Health and Care sets out how we can achieve this.
Also, Scotland's first data strategy for health and social care sets out how we will work together in transforming the way that people access their own data to improve health and wellbeing; and how care is delivered through improvements to our systems.
Implement co-benefits from tackling the climate emergency
As described in Chapter 4 and the NHS Scotland climate emergency and sustainability strategy, taking action on the climate emergency will also result in wins for health outcomes. We must maximise these co-benefits in a proactive response to climate change.
Take a public mental health approach
Improving the mental health and wellbeing of the population of Scotland is a priority and requires a proactive and preventative approach across all levels of the system. This includes addressing both the root causes of poor mental health and strengthening the factors that boost positive mental wellbeing, in active partnership with relevant communities. The Scottish Government policy prospectus published in April 2023 commits to improve mental health and wellbeing support by 2026. Also, initial responses from the consultation on the new Mental Health and Wellbeing Strategy for Scotland were published in February 2023. These results have been used to inform the new Mental Health and Wellbeing Strategy and Delivery Plan published in the summer of 2023.
Contact
Email: realisticmedicine@gov.scot