NHS Scotland redesign of urgent care: second national staging report
This is the third of three reports assessing our urgent and unscheduled care - redesign of Urgent Care Programme.
4. Findings
4.1. NHS Scotland Management information findings
The focus patient population for the RUC programme is a sub-group of patients who historically presented to A&E services (ED/ MIU), who may be safely managed through alternative patient pathways.
4.1.1. High Level Summary
Activity and Time related performance summary for NHS Scotland. (Note data caveat section below and related focus group feedback sections).
1. The public and patients have responded to the messaging to increase contact for urgent care needs through increased use of NHS 24 111 (call demand and contact records) as envisaged by the RUC programme.
2. This is evident by the marked increase in NHS 24 111 call demand and contact records (ED, Mental health and COVID-19), most significant Monday - Friday in routine hours/ in-hours (IH), with a smaller increase for OOH demand Monday - Friday. Total call demand has increased to a much greater extent compared to patient contact records.
3. Patient disposition from NHS 24 contact records to GP OOH, GP IH, SAS and A&E services as defined by total activity is similar or increased compared to historical patterns (June - August 21 and June – August 19). These pathways all include COVID-19 activity. GP, particularly OOH, should be considered with COVID-19 activity which demonstrates increased activity, due to potential workforce overlap.
4. Patient disposition activity from NHS 24 111 to self-care/other is similar to historic patterns.
5. SAS (attended and conveyed) activity is broadly similar to historical levels. The non-attended component is increasing (almost double historical levels), requiring on-ongoing review.
6. NHS 24 111 to FNC disposition activity has increased over time since the introduction of FNCs and has stabilised in recent months.
7. The level of patient activity through the RUC - FNC pathway is relatively small (circa 400 patients per day across Scotland). Based on exploratory linked analysis approximately half of those referred to FNC are seen in A&E services and half offered alternative care. This varies by NHS Board.
- 8. The FNC pathway in its current format may reduce total A&E services demand by approximately 5% of patients per annum across Scotland, as defined by patients being managed by the RUC - FNC pathway who do not attend A&E services. See point 9 below.
- 9. Considering the overall activity of the RUC pathway, including all referral routes to A&E services suggests a lesser impact on the overall RUC pathway (see 3 and 8 above).
- 10. Overall, A&E services (planned/unplanned) activity is similar to historic activity. Self-presenters are lower than in 2019 and remain the major group attending A&E services; this needs to be taken into context with point 9 above. Planned attendances are currently approximately 5% of total A&E services activity.
- 11. Patient admission to total A&E services attendance ratios are very similar to historic values at approximately 27%.
- 12. Performance, based on time stamp data:
- For NHS 24 111, call responsiveness has deteriorated and remains a challenge at weekends and OOH Monday - Friday in particular.
- For patients accessing the RUC-FNC-A&E services pathway (approximately 150-200 per day) the available time stamp data (patient journey time, which excludes NHS 24 111 call response times) appear efficient. Improved and more complete data to better understand scheduling versus immediate onward referral of FNC-A&E services is needed.
- Performance against the 4-hour emergency access standard has deteriorated. Delays on transfers of care (delayed discharges) are increasing and may be contributing to the decrease.
- Ambulance handover times have deteriorated. This is likely related to the decline in the 4-hour emergency access standard which may reflect reduced flow for patients who require hospital admission.
- 13. Paediatrics data is very preliminary as only 3 months' data are available for comparison. There has been an increase in NHS 24 111 contacts, with evidence of increased referrals to GP OOH and FNCs as expected, predominantly Monday - Friday. FNC activity remains relatively stable at approximately 50 patients per day, with 22% being referred to A&E services.
- 14. Mental health was not part of phase 1 of the RUC Programme but early data shows patterns similar to adult non-mental health patients. Notably, mental health patients have a higher number of contacts per episode.
4.1.2. Data caveats for both adults and children
- The RUC programme launch coincided with the second wave of the COVID-19 pandemic, with on-going effect.
- Data does not consider case acuity, complexity, outcomes, or workforce challenges.
- The pandemic and associated public health interventions continue to influence urgent care services for both COVID-19 and NON-COVID-19 related healthcare.
- COVID-19 activity is included in all relevant touchpoints including Primary Care. Note that it is understood a proportion of patients being referred through the pathways have non-COVID-19 related symptoms, e.g. respiratory.
- Primary care In-Hours data are not routinely available; urgent work is under way to resolve this.
- GP OOH activity includes all consultations directly related to a case contact. For example, one case may have several consultations.
- FNC data quality and completeness problems remain for disposition and time stamp data.
- Analysis is on-going for patient journey times and contacts.
- A&E services data quality and coding requires further improvement.
- Data periodicity (patterns) highlight the importance of temporal analysis. Urgent and unscheduled care varies by day or time of week. This is important for analysis and design of systems. If analysed together, data may be misinterpreted.
- Paediatric total numbers are less than adults with a shorter time period since Go-Live (June 2021). Data should be interpreted with caution until more data points become available.
4.1.3. Approach across key touchpoints in the patient journey
Analysis was and continues to be compiled by Workstream 1 Data and Monitoring Group (see Appendix D for group membership). The group produces monthly RUC data reports, and an earlier Prioritisation Paper[11] outlined data recommendations and priorities.
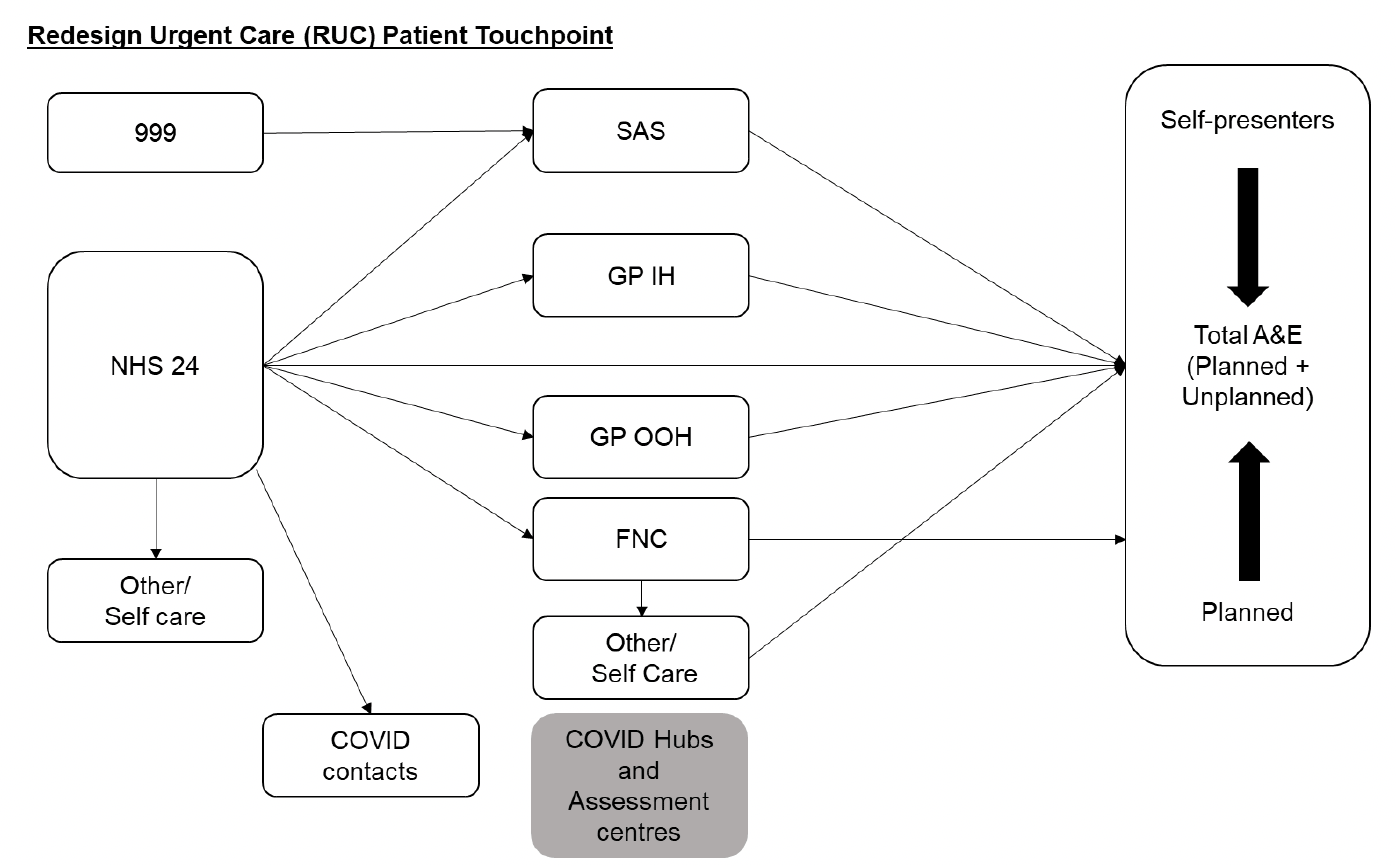
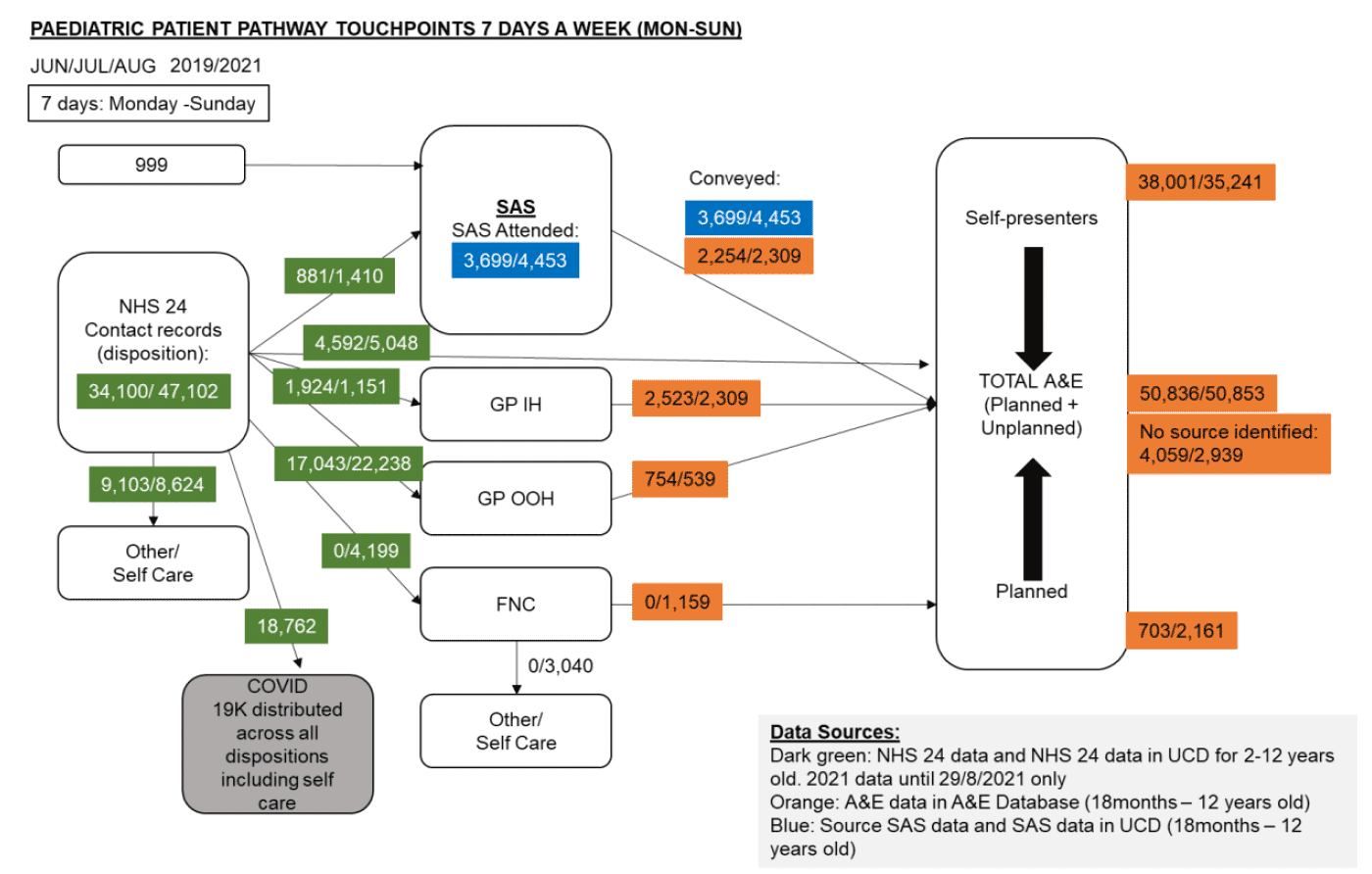
This section includes quantitative management information data collated through the Evaluation Advisory Group (EAG) and supported by PHS and stakeholders. This section shows activity, performance and time stamp data based on patient touchpoints (Figure 2). Activity and demand data covers the period from January 2019 to end of August 2021 (including RUC National Go-Live on 1 December 2020).
The diagram in figure 2 displays the various touchpoints through the RUC patient pathway. Patients can access the RUC pathway by dialling 999 or contacting NHS 24. From there, dependent on the nature of their condition, the patient can be referred onto a number of services including but not limited to Scottish Ambulance Service, Primary Care GP (in-hours/out-of-hours), Flow Navigation Centre (FNC), or COVID Hubs and Assessment Centres. The patient can then either be referred back to their GP, given self-care advice or if necessary advised to attend A&E services if required.
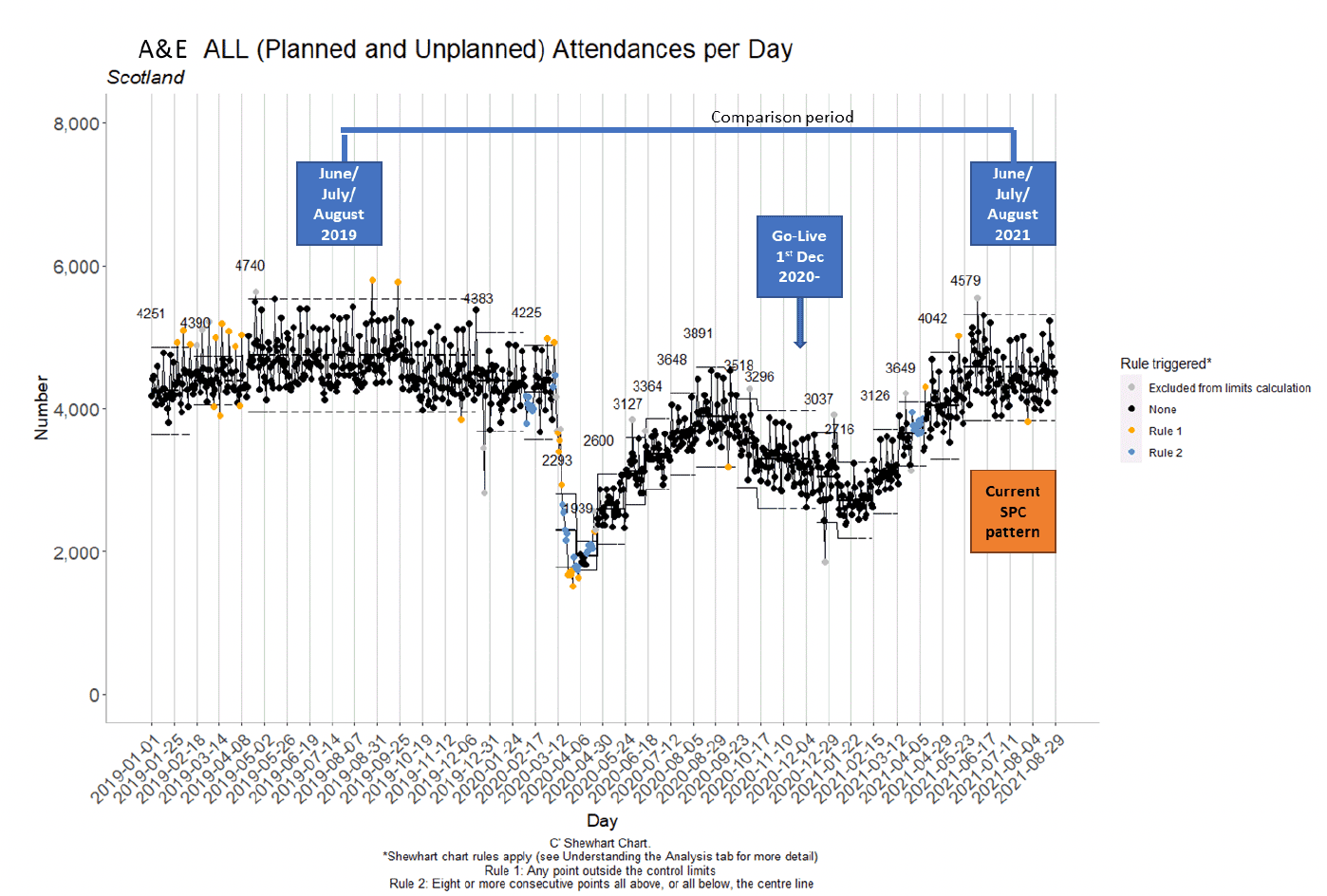
Statistical Process Control (SPC) charts, as recommended by NHS Scotland and NHS Improvement (Making Data Count, 2018[12]) are used as the main analytic approach (example in Figure 3). They highlight process change and patterns at Scotland and board level. Supporting comparative data is provided (as appropriate) between Jun - Aug 2019 with Jun - Aug 2021 (also the current SPC pattern period referred to in this section), as these two periods are broadly stable. Daily data is used to improve understanding of demand patterns to support service provision.
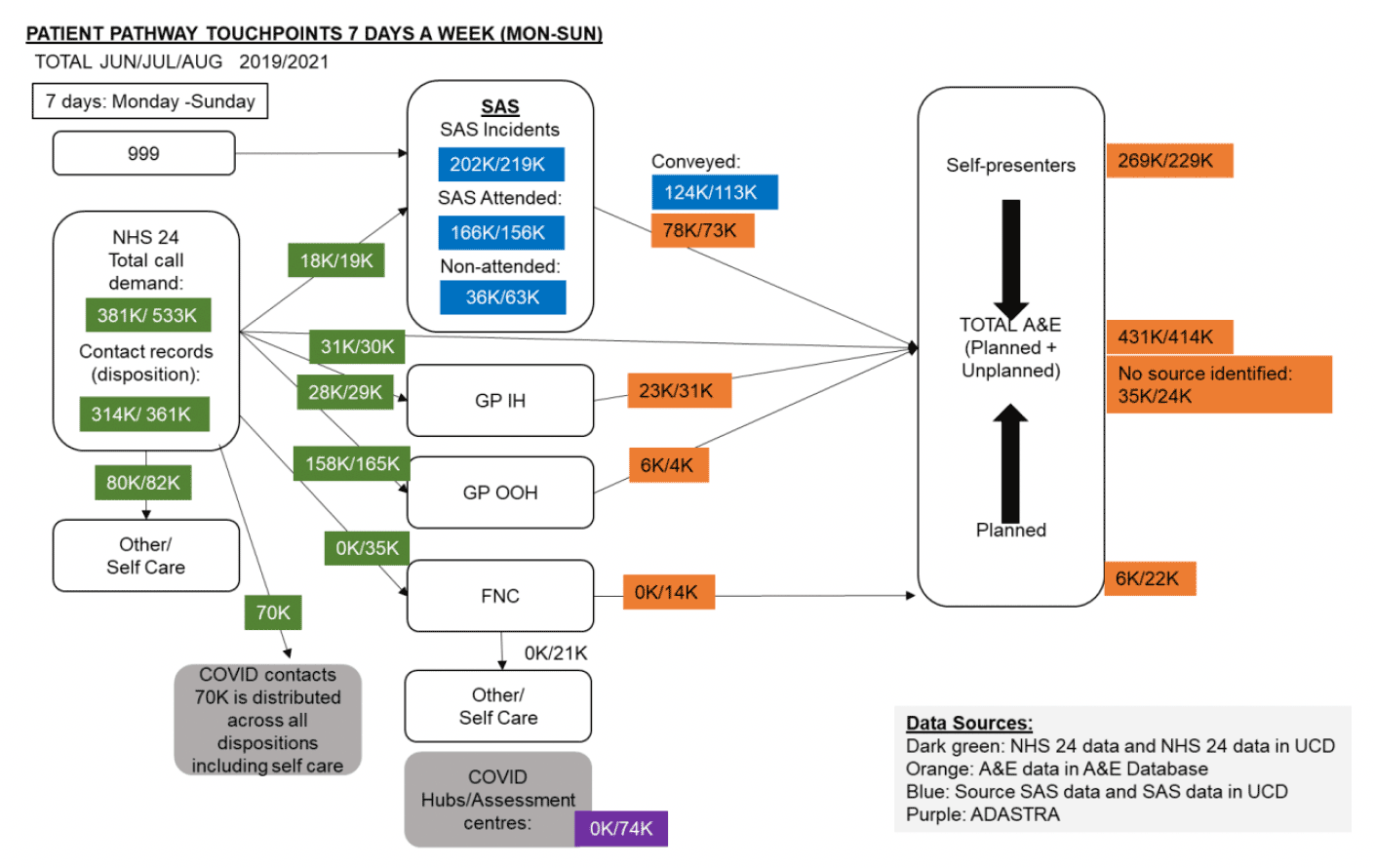
4.1.4. Data findings for touchpoint comparison between June - August 2019 to June - August 2021 for Monday-Sunday (Figure 4). Monday-Friday and Saturday-Sunday (Appendix E). This expands on the summary findings above.
- The public have responded by calling NHS 24 111 more frequently (call demand increased by over 40% comparing 2021 to 2019), as envisaged. Mostly in-hours Monday - Friday.
- Contact records (calls answered, a case record created) have increased to a lesser extent, approximately 15 - 20%. For this group it is estimated contacts may be 10 - 15% higher representing repeat calls as part of the same episode of care.
- Contact record disposition in 2021 is 46% to GP OOH (50% 2019), 23% to Other/self-care (25% 2019), 10% to FNCs, 8% direct to A&E services (10% 2019), 8% to GP IH (9% 2019) and 5% to SAS (6% 2019). Of all 2021 NHS 24 111 contact records, 19% had a COVID-19 tag.
- Total A&E services (planned + unplanned) activity in 2021 is approximately 4% lower than 2019.
- Self-presenters are 15% lower than 2019 and continue to be the major group attending A&E services.
- Patient admission to total ED attendance ratios remain similar to historic values at approximately 27%.
- For all A&E services attendances (excluding self-presenters), SAS contributes 27% (29% 2019), GP IH 8% (5% 2019), NHS 24 111 7% (7% in 2019), planned attendances 5% (1% 2019) (approximately two thirds from FNCs), FNCs 3% and GP OOH 1% (2% 2019).
- Planned attendances have increased from 1% to 5%. This is related to FNC referrals and improved A&E services coding. There remains a need to better understand scheduling, time to appointment, time to completion & comparison with non-planned attendances and further improve A&E service coding.
4.1.5. Understanding the impact of the RUC pathway on A&E services attendances (Using June-August 2019 and June-August 2021 data)
- Figure 4 shows the total number of patients in June to August 2021 against June to August 2020 at each touch point in the RUC Pathway.
- Total A&E services attendances (planned and unplanned) reduced by 17K compared to 2019 (annualised 68K).
- Self-presenting attendances are reduced by 40K, compared to 2019 (annualised 160K).
- Total planned activity to A&E services is 22K (16K higher than in 2019), of which 14K (or 56K annualised) can be attributed to the FNC referral pathways.
- There has been an increase in Primary Care referrals to A&E services by 6K (annualised to 24K).
- A potential impact of the RUC pathway on A&E services self-presenting attendances, given the current context and taking into account the increase in planned activity and increase in Primary Care referrals, gives a potential net benefit effect between 48K to 74K per annum. The FNC component of this would equate to 28K annually.
- NHS 24 111 self-referral patterns are similar to historic levels.
- One area that requires further evaluation is the interaction between NHS 24 111 and Primary Care (both IH and OOH), in relation to patients being referred onwards to A&E service.
4.1.6. The Scotland Data Table August 2021 (Appendix F) (with predicted activity related to the RUC pathway) focuses on SPC analysis and recent trend data.
Appendix F shows the envisaged impact of the RUC Programme on activity against current data. Percentage change data is a time point comparison (August 2021 and August 2019) using SPC and touchpoints. Individual NHS Board summary data (Appendix G).
4.1.7. Time related system variation (Periodicity (Scotland Data Table August 2021))
4.1.7.1. NHS 24 111
- Data periodicity shows 4 patterns of NHS 24 111 activity: Monday - Friday in-hours 0800-1800, Mon-Fri OOH (1800-0800), weekends and public holidays. Public holiday activity is stable over the last 32 months.
- Total call demand and contacts increased in line with RUC planning. Call contacts activity has markedly increased Monday - Friday in-hours, with smaller increase OOH and weekend activity stable. NB:10 - 15% of calls are repeat calls, not generating a new contact.
- NHS 24 111 to A&E services referrals are higher Monday - Friday compared to 2019. Referrals to SAS are higher Mon-Fri.
Other patient touchpoints including GP OOH, A&E services attendances and emergency admissions also show Mon-Fri/weekends periodicity.
4.1.8. Performance (Scotland Data Table August 2021)
4.1.8.1. 4-Hour Emergency Access Performance
Performance for August 2021 76% compared to 89% in August 2019.
4.1.8.2. SAS to A&E services Turnaround Times
Turnaround times have been increasing since 2019, with a further increase from April 2021 (August 2019 30 minutes versus August 2021 41 minutes), impacting available crew hours.
4.1.8.3. NHS 24 (111) Time to Answer (TTA) & Call Abandonment Rates (Appendix H)
- Response times have three main patterns which relate to call volumes, day of the week, and public holidays. Weekend and public holiday activity is greater than Monday-Friday for both current and historical patterns of activity.
- TTA and call abandonment rates have increased and remain challenging particularly OOH's and at weekends.
- This analysis does not consider call complexity, repeat callers or staffing levels. Note, average handling time (AHT) has increased over time since January 2020.
4.1.8.4. RUC/Flow Navigation Centre/A&E Services Pathway (exploratory analysis)
- The NHS 24 111 call process was re-designed from a potential call back option, to responding to all calls as quickly as possible in one contact episode and put in place early 2020 to improve the patient journey (pre 1 December 2020 national RUC Go-Live date). This impacts on comparative historical data interpretation.
- FNC referred activity represents 8-10% of all NHS 24 111 contacts.
- Exploratory data linkage suggests approximately 50% of FNC activity is referred to A&E services.
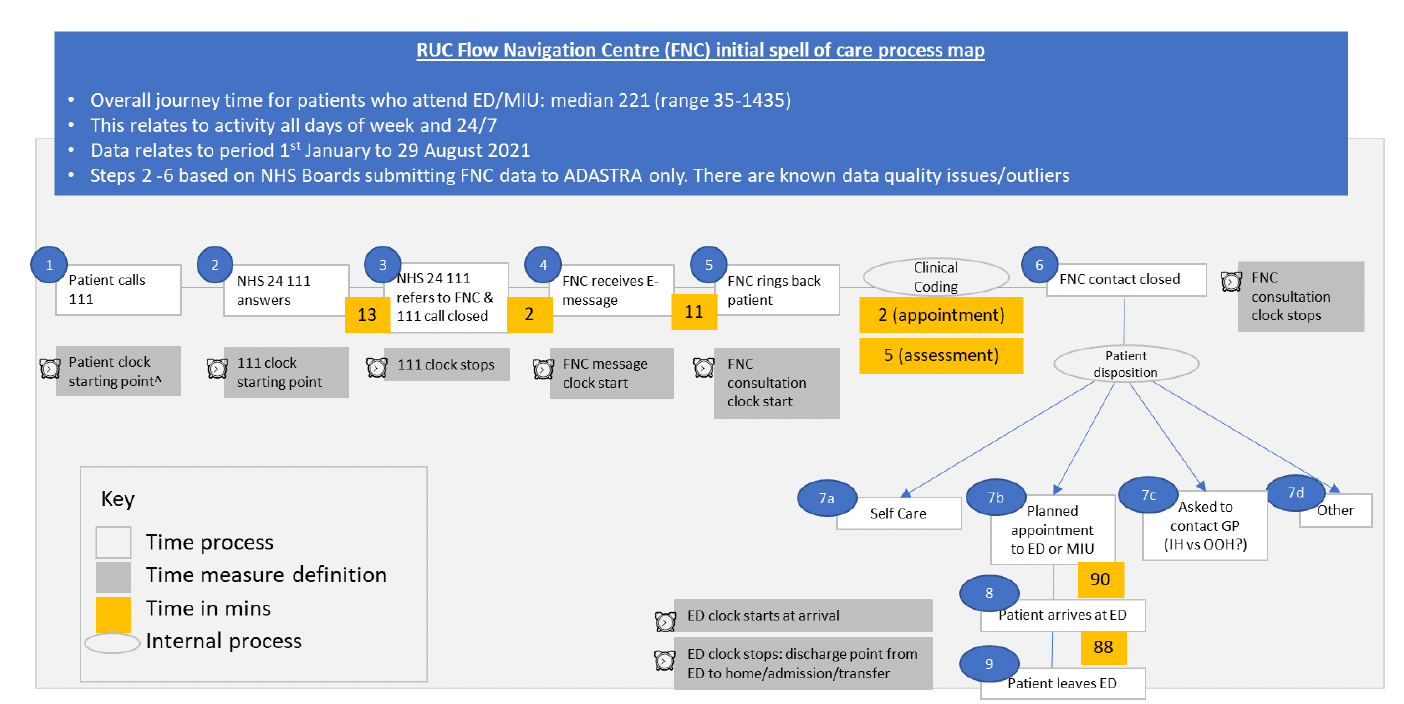
4.1.9. Time stamp data (Figure 5) process map (excludes NHS 24 111 call response time)
- Median total journey time to A&E services discharge 221 minutes (upper 95th percentile 1186).
- Median time from end of FNC consultation to being seen in A&E services is 90 minutes. This is part of on-going work at NHS Board Level to understand the proportion of patients referred immediately versus a planned appointment.
4.1.10. Near Me Utilisation as part of FNC pathway (operational in 11/14 NHS Boards)
- Between December 2020 and July 2021, across NHS Scotland Near Me consults accounted for 13% of FNC contacts.
- Average call duration for a Near Me consult in Scotland was approximately 6 minutes.
4.1.11. Paediatrics (age 18months – 12 years)
Data is preliminary as RUC paediatric programme only went live June 2021. Available data awaits final validation and therefore there may be some minor variations. For most touchpoints data, total patient numbers are relatively low compared to adults and the SPC charts suggest activity is not stable yet.
4.1.11.1. Data findings for Paediatric touchpoints for total activity for the period. Comparison between June-August 2019 to 2021 for Monday-Sunday (Figure 6), Monday-Friday and Saturday-Sunday (Appendix I)
- NHS 24 111 call contact records (calls answered and a case record created, with disposition) have increased by 38%, when comparing June-August 2021 to 2019. Note: as per for adults, repeat calls for same episode are not included. The increase occurs Monday-Friday.
- Of all NHS 24 111 contact records (47K), 40% had a COVID-19 tag, which is higher than adults.
- Total paediatric NHS 24 111 referrals to FNC were 4,199, representing 9% of all NHS 24 contact records, of which 75% of contacts are Monday-Friday.
- Since July 2021, NHS 24 111 to FNC data appears relatively stable at approximately 50 referrals per day, with 11 (22%) of this group being referred to A&E services from FNCs.
- There is a small increase to GP OOH as expected; this is most evident Monday-Friday.
- Total A&E services activity is similar to historic levels, although self-presenters as a group are slightly lower.
Figure 6 shows the total number of paediatric patients (children aged 12 and under) in July to August 2021 against June to August 2019 at each touch point in the RUC Pathway.
4.1.12. Mental Health
The Mental Health pathway is not part of this formal evaluation as it was not part of Phase 1 RUC Programme. A high-level summary position is represented here:
- NHS 24 111 contacts, GP OOH and SAS attended have remained stable since September 2020.
- A&E services attendances gradually increased in 2021 but remain below historical levels.
- Marked differences between mental health and physical health related calls to NHS 24 111, with those calling for mental health being 5 times more likely to be frequent callers.
- Mental health patients are 10 times as likely to have patient journey with 5 or more steps compared to general population contacting NHS 24 which is likely to reflect complex needs.
4.2. Equity of Access
This section is split into three parts, showing different studies, as it was important to monitor to avoid a negative impact of RUC implementation on equality of access to urgent care services.
4.2.1. Age and Deprivation index and ethnicity (Appendix J)
These data compare August 2021 to 2019 by monthly average.
- The pattern of access by age and index of deprivation for NHS 24 111, SAS and A&E services attendances is similar to historical organisational patterns.
- For NHS 24 111, SAS and A&E services attendances the pattern of use is similar with the Socio-demographic group 1 (most common) and Socio-demographic group 5 (least common). The pattern of service use by age differs historically for these three services. Consistent with increased NHS 24 111 activity, there has been a small increase in NHS 24 111 contacts across all age groups.
- NHS 24 111: most common age groups (by 5-year band) are 0-4, 80-84 and 85+, recent data is similar though 0-4 and 85+ contacts may be less.
- SAS incidents: increase with age and most common age bands are in the > 65 age groups; this is unchanged.
- A&E services attendances: The most common age groups (by 5-year band) are 0-4, 75-79, 80-84 and 85+; this is unchanged.
- Ethnicity data remains suboptimal. Across Scotland it is only recorded for 70% of A&E services attendances, with variation across health boards. 92% of attendances, where recorded as Scottish or Other British.
4.2.2. Equity of Access, following RUC implementation (Appendix K)
PHS have completed a more in-depth analysis looking at age, sex and level of deprivation. These were broken down into 3 age bands (under 18, 18-64, 65+), 5 quintiles and male/female gender. Analysis undertaken for four different urgent care access pathways (A&E services self-presentations, A&E services attendances, OOH contacts and NHS 24 111 calls).
For the purposes of this analysis different time periods were used which differs from the daily time point analysis in section ii above.
- There was no evidence of differences in A&E services self-presentations, A&E services attendances or total contacts between levels of deprivation. There was evidence of a Scottish Index of Multiple Deprivation (SIMD) gradient for OOH contacts, NHS 24 111 calls (higher percentage drop for levels of use in the most deprived areas) and NHS 24 call terminations (higher number of terminations for more deprived areas).
- There was no evidence of a gender gradient for A&E services self-presenters, A&E services attendances and OOH, except with NHS 24 calls (higher percentage increase for males).
- There was evidence of an age gradient for pathways (higher percentage drop for under 18s) and for NHS 24 call terminations (higher number of terminations for the 18-64 age group).
This initial exploratory analysis is narrow and provides insights but does not seek to give a definitive answer to the question of whether any changes in access have been the direct result of the redesign process or whether they represent an improvement or worsening in equity of access to urgent care following redesign.
The RUC Programme will continue to engage PHS further to fully understand any impact from RUC on equity of access of urgent care.
4.2.3. Groups who are more likely to experience barriers or disadvantage when accessing urgent care services
The RUC Programme commissioned HIS - Community Engagement, to undertake a 'Gathering Views' exercise in May 2021[13], to elucidate what matters to groups more likely to experience barriers or disadvantage when accessing urgent care services by calling NHS 24.
Groups identified from national Equality Impact Assessment (EQIA) included: people with addictions, asylum seekers, refugees, unpaid carers, disabled people, those from minority ethnic groups, homeless people, LGBT+, elderly, and those living in remote or rural locations.
Participants were asked questions about experience of using the new urgent care service, their feelings about using the service in the future, and how the service might be promoted.
Details of the findings and themes are included in the full report and a summary of recommendations can be found in Appendix L.
4.3. Listening exercise NHS Scotland staff
Between 11th August – 9th September 2021, 12 focus groups were held to engage with a wide range of staff across NHS Scotland to hear their lived experience of the RUC pathway. The focus groups were facilitated by the RUC Evaluation Programme Senior Responsible Officers together with an experienced facilitator, for continuity.
The sessions provided an environment for open and honest conversations, posing two questions about the RUC pathway:
- What works well?
- What needs to be improved?
There were 112 attendees, from across the territorial NHS Boards, NHS 24, SAS, National Education Scotland (NES) and professional bodies. The approximate split between clinical (including those in leadership and management), management and/ or programme roles was approximately 60:40.
Thematic analysis identified some clear and consistent messages. However, there were also areas of differences or inconsistencies.
To note:
- Attendees in leadership and management roles tended to be more positive about acceptability, progress and impact. Although support for the RUC programme was broad based, there were notable exceptions, with caveats expressed by some professional groups, particularly regarding implementation challenges.
- Tendency for conversations to focus on the FNCs rather than the whole pathway, with more limited feedback about the initial patient journey from first point of contact.
- SAS were not formally part of Phase 1 implementation, although they were actively engaged in focus group conversations.
- It was difficult at times for attendees to distinguish between urgent, emergency and unscheduled care, which may reflect their lived experience. It also highlights the complexity of the care system and that change in one part of the system may have impacts and consequences in other parts of the system.
- Attendees consistently commented on the difficulty of understanding the impact of the RUC pathway during the changing dynamics of the COVID-19 pandemic.
Findings are presented as key themes and where appropriate at touchpoints in the patient journey to enable read across to the management information presented.
4.3.1. Workforce
Significant concerns were expressed about the sustainability and resilience of the workforce, posing a substantial risk to the delivery of urgent care services.
We heard about reduced staff morale, tired staff coping with the ongoing effect of the COVID-19 pandemic. This includes staff who are still redeployed from key change management and patient experience roles and concern about staff ability and capacity to engage in ongoing change.
There was an overall sense of skilled and experienced staff being moved around the urgent /unscheduled care system. Some on are temporary/short term contracts, with many NHS Boards supplementing the short-term National funding posing a risk to sustainability of current services. Frequent short-term sickness and absence is compounding longer-term vacancy factors.
4.3.2. RUC Pathway Touchpoints
4.3.2.1. Urgent care access
Staff told us that they feel there is far greater potential for people and carers to access self-care advice via NHS Inform and Community Pharmacies as a first point of contact.
4.3.2.2. NHS 24
Staff were positive about the creation of safe space conversations between NHS 24 and NHS Boards, as a forum to build relationships and trust and for mutual problem solving. However, there were concerns about:
- managing surges in demand and the impact of backlog in call answering on system flow, overall waiting times and user experience
- the number of 1-hour and 4-hour pathway dispositions
- the numbers of people referred to self-care
- the level of understanding of local provision and geography, especially in remote and rural communities.
4.3.2.3. Flow Navigation Centres (FNCs)
There is wide variation across NHS Boards in the way FNCs are functioning, including:
- core operating hours
- dedicated clinical resource. Staff described differences in the level of dedicated clinical staffing especially in smaller NHS Boards, where SCDMs often have other clinical commitments, especially out-of-hours. In some instances, SCDM slots are voluntary and often reliant on the same people.
- assessment and SCDM roles. Staff described differences in competence, confidence and the professional regulations governing staff in assessment and clinical decision-making roles. The role is largely undertaken by ED Consultants, GPs and Advanced Nurse Practitioners but staffing models and skill-mix varies and it is unclear whether this is in line with clinical need.
- where FNCs operate with limited face-to-face contact with members of the FNC delivery team there may be less opportunity for team building, learning, collaboration and shared risk taking.
Clinical staff highly valued professional to professional calls and clinical decision support offered through FNCs, to discuss clinical risk and identify safe alternative pathways. However, there is a need to further widen the access and support for more professional-to-professional discussions.
The use of digital (remote) consultations was felt to improve clinician and patient confidence, effective clinical decision making and provides more patients with appropriate alternative care pathways. Digital consultations may be under-utilised, possibly because of time pressures, ease of access and user confidence.
Planning and scheduling of urgent care is gaining acceptance but needs to progress at scale to have impact. There is a need to extend access to, and further invest and develop community-based alternatives and urgent outpatient provision. People referred to A&E services with a scheduled time slot often find they joined the queue on arrival and experienced further delays to their care.
FNCs are diverting some patients to alternative pathways but the actual numbers were perceived to be lower than anticipated and often FNC activity is below available capacity. Some staff talked about the need for FNCs to be effectively resourced to operate consistently and increase productivity, in order to demonstrate impact at scale to provide a more cost effective and efficient service model.
4.3.2.4. Minor Injury Units (MIUs) and Emergency Departments (EDs)
There were differences in feedback about the impact of RUC on local minor injury pathways. Some feedback suggests improved pathways while others report that they had a good minor injury pathway prior to RUC and the new RUC pathway is now more complicated, with longer overall waiting times as patients now have to access A&E services via NHS 24 111 and the local FNC.
A&E services staff described people referred via the RUC pathway arriving later in the day when access to diagnostics is more limited and staffing levels lower, some of whom could have been offered alternative pathways. There are still significant numbers of self-presenters and an overall sense of unmet need and pressure building across the system, especially for musculoskeletal care and longer-term injury.
The feedback is similar for Primary Care IH and OOH, with staff feeling they are managing increasing demand and changes in urgent care health seeking behaviour. There was an unverified sense that some patients may be trying multiple routes to access urgent care for the same episode of care and are being redirected around the care system, resulting in multiple patient encounters.
The urgent care system is presently complicated by ongoing unprecedented COVID-19 services and measures. Concerns were expressed commonly about planning for surge and winter resilience and the need for clarity about national planning guidance.
4.3.2.5. Person-centred redesign
There were examples shared about specific initiatives to improve the pathway for people with urgent mental health needs, working in partnership with the police and non-statutory organisations to provide care closer to home.
There was consistent feedback about people experiencing multiple triage and assessment, highlighting duplication, potential waste and pathway inefficiencies. Resultant waits and delays may erode public confidence, especially if people end up being sent to A&E services when other pathways could have provided more appropriate care closer to home.
Some staff talked about the need to understand the added value of each step in the urgent care journey and the collective investment in NHS 24 and FNCs.
Some NHS Boards are considering a more whole-system approach, integrating FNCs with other services including GP OOH and Social Care with the potential to create a more flexible, responsive and cost-effective urgent care model.
Staff described opportunities to develop regionally based provision, in collaboration with NHS 24 and SAS. It was suggested that collaboration between smaller NHS Boards, could possibly generate economies of scale and more efficient and cost-effective workforce solutions.
4.3.2.6. Digital infrastructure, data and information
There were differences in opinion about how well the different elements of the digital infrastructure work. There are challenges with system interface and intra-operability issues; staff training, working across multiple screens and systems and risk with multiple data entry.
This also impacts on ability to have accurate data and information for improvement and to manage whole systems demand and capacity.
There is a need to accelerate the development of the (electronic) single shared care record and access to the clinical portal, especially important to work effectively with SAS and Community Pharmacies.
4.3.2.7. Public messaging and confidence
There was consistent feedback from staff that in their experience of how public messaging about urgent care has changed it is unclear and there is a need to align national campaign and locally nuanced messages relevant to the local care system.
To build local public understanding and confidence, there needs to be a common understanding, consistent communication and signposting by all staff at patient touchpoints in the pathway.
There were also expressed concerns that current public messaging is creating an unrealistic expectation for 24/7 access, with insufficient expectation of scheduled care provision as 'the norm', driving up demand across the whole care system, not just NHS 24.
4.3.2.8. Transformational change
There was support for the intent and principles of the RUC pathway, which has been largely seen as a catalyst for change and focused necessary attention on creating alternative options to A&E services attendance. However, concerns were expressed by some about RUC, particularly implementation challenges. Partnership working across multidisciplinary and multi-agency teams is perceived as having improved communications, building relationships and trust.
There is however a tension experienced between what staff describe as a nationally-mandated approach, driven at pace and a more-lengthy journey of transformational change, creating the culture for the scale and duration needed to fully achieve the RUC ambition.
Transformational change takes time and support, including local improvement, change management and organisational development. Robust local feedback loops are needed to help staff understand the impact of changes in practice. National networking opportunities are welcomed to more widely share learning across NHS Boards, clinical teams and professional groups.
NHS Boards are still working through phase 1 operational and clinical change. Staff spoke about a sense that some services have been put in place before there was a unified vision of the whole urgent care pathway. Some NHS Boards have taken an improvement approach and using tests of change and incremental development.
Many of the issues were felt to be with implementation of, rather than with the RUC programme itself. However, the perceived primary focus on A&E services might undervalue the role of Primary Care and other community partners. Some A&E services staff expressed views that the apparent prime focus on self-presenting patients was not addressing the main problem they experience of delays in admitted pathways.
There are variations throughout NHS Scotland in how the RUC Programme has been adopted and the scale of ambition, local engagement and improvement focus. Staff from some NHS Boards with fewer urgent care presentations have questioned the return on investment, which prompts questions about economies of scale and opportunities for greater integration on a regional or joint NHS Board partnership basis. Some staff described the broader fundamental change with more widespread inclusion of Social Care and care home independent and third sector partners.
4.3.2.9. Island Heath Boards
Representatives of island NHS Boards (Orkney, Shetland, Western Isles) felt that there was a need to progress RUC in the broader context of planning sustainable care services for the unique circumstances and challenges of remote communities.
Island NHS Board staff expressed high regard for the support from NHS Highland that provides their FNC service (from Inverness). However, island-based services (availability of Senior Clinical Decision Makers (SCDMs), diagnostic and treatment facilities) do not match those on the mainland. Urgent care protocols and pathways must closely align with the actual availability of SCDMs, the range of accessible services and diagnostics capability.
A clear view was expressed of the importance of taking a system wide approach, including a more proactive approach to anticipatory care. There are opportunities to collaborate to provide 24/7 services across the islands, building public confidence and managing care expectations.
Moving forward, many staff felt the need to clearly build and articulate the vison for local people and create a positive narrative about widening access to optimal urgent health and care provision closer to home.
4.4. Review of RUC - FNC pathway in Greater Glasgow and Clyde
To gain greater insights into the effectiveness of the RUC pathway and the experience of users, a pathway review was prototyped and tested in NHS Greater Glasgow and Clyde (NHS GG&C).
Between 30 August 2021 and 5 September 2021, a 25% sample from approximately 400 patients and carers (age range 5-88 years) who accessed care through NHS 24 and who were referred to the FNC were identified for clinical review of the appropriateness of the pathway. The sample was a timed series across the hours of operation of the FNC (10.00-22.00) within a 7-day period.
104 of the 105 patient records sampled were identified as appropriate for referral to the FNC. One person was more suited to referral to Primary Care services and was referred accordingly.
The onward referral of patients is shown in figure 7. Most patients (57%) were scheduled to attend A&E services and 36% to self-care or other services.
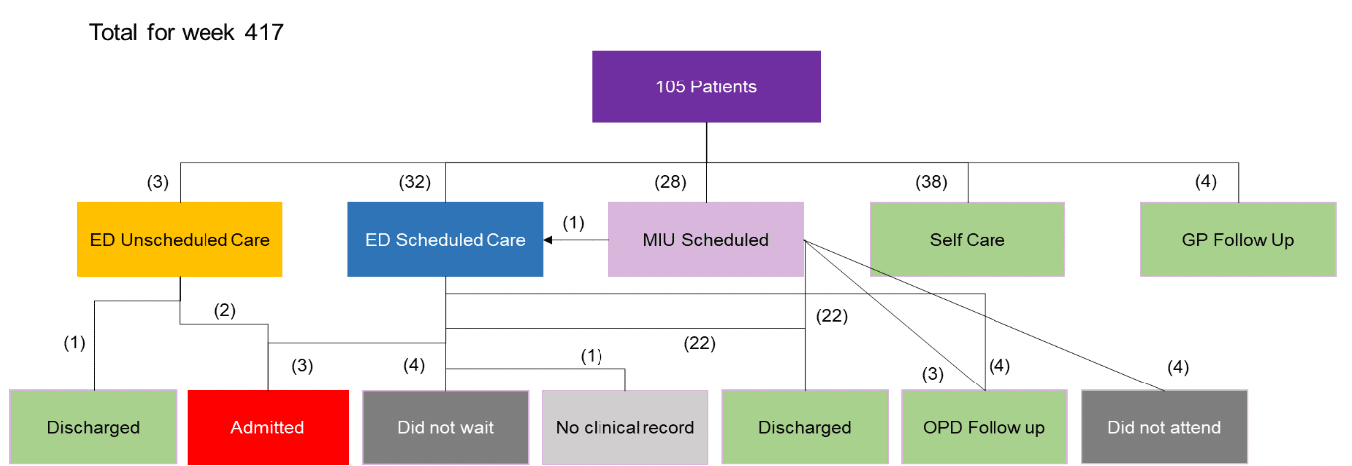
51 of 105 individuals with referrals to all areas, participated in a follow up telephone questionnaire by NHS GG&C Patient Experience team to understand their experience of RUC.
There was wide variation in the length of time from the start of triage at NHS 24 to the end of treatment for patients not admitted (range 29-20 hours) with the 10 longest waits for patients with care scheduled for the following day. It was not possible to capture call waiting times at NHS 24.
The following themes were identified from telephone questionnaires in order of most common:
1. Efficient pathway
2. Effective care
3. Good communication from professionals in the pathway
4. Long waiting times negatively affects patient experience at all points of the journey
5. Positive person-centred approach
A full report[14] of the patient pathway review, including recommendations for improvements in the review process can be found on the CfSD website.
4.5. Patient Experience
In the absence of comprehensive and comparable patient data from NHS Boards a review of the numbers of positive and negative posts to Care Opinion[15] has been undertaken for April – September 2021 and the same period 2019 pre the COVID-19 pandemic and launch of RUC. See Figure 8.
| Month | Positive | Negative | Total |
|---|---|---|---|
| April 2019 April 2021 | 42 32 | 4 2 | 46 34 |
| May 2019 May 2021 | 51 42 | 2 9 | 53 51 |
| June 2019 June 2021 | 31 42 | 6 8 | 37 50 |
| July 2019 July 2021 | 34 31 | 6 14 | 40 45 |
| August 2019 August 2021 | 31 36 | 3 11 | 34 47 |
There has been a slight increase in the proportion of negative comments this year, which largely relate to time delays and staff attitudes or communication. These data will be kept under continuous review.
4.6. Right Place, Right Care, public messaging campaign
As part of the Urgent and Unscheduled Care - RUC Programme, Scottish Government commissioned the Right Care, Right Place public messaging campaign in winter 2020. The campaign aims to raise awareness of the new process to access urgent care with a view to diverting the approximate 20% of people that self-present at A&E services, to more appropriate NHS services for their care needs.
The first campaign ran from the end of November 2020 until end of March 2021 in what was described as a soft launch, with local messaging and a national door drop in January 2021. Evaluation of this period demonstrated that digital, press and local communications campaign have been effective and fostered high levels of engagement.
The communication toolkits were updated based on the findings and shared with NHS Boards to use locally.
Field work for the second campaign was undertaken in May 2021 and the campaign ran during July and August 2021. An evaluation of the campaign to date was carried out in August – September 2021.
Overall, the campaign performed well, with recognition exceeding average campaign levels and the campaign is reported as being clearly understood. Key findings from the evaluation are:
- People who recognise the campaign are more likely to call NHS 24 111
- Fewer people now see NHS 24 as an OOH service and awareness has risen that NHS 24 is available 24/7 – this is higher for people who recognise the campaign
- People with children and people who have underlying health conditions are more likely to recall the campaign
- Older people and males were less likely to have seen the campaign but recall levels are good
- 41% of people claim to have acted on the campaign messages – the most likely action to call 111 instead of attend A&E services
- Satisfaction levels for NHS 24 and A&E services are high
The key recommendations were to continue with the current media strategy. People who have seen the campaign through four or more communication channels are more likely to act positively and next steps are to proceed further with a multi-channel approach, using posters, TV, radio and social media.
Contact
Email: RedesignUrgentCare@gov.scot