National Centre for Remote and Rural Health and Care: evaluation
The report is an evaluation of the National Centre for Remote and Rural Health and Care.
Chapter 7: Overall Reflections on Progress to Date
Overall Progress Across Pillars
The National Centre has delivered meaningful outputs in its first two years, though progress has varied by pillar:
- Education and Training has been the most advanced area, with several headline targets achieved or exceeded. The funding of rural practitioners for the RAP MSc programme surpassed expectations, and the Remote and Rural Supervisory Hub attracted over 1,600 users in its first year. Multiprofessional training sessions exceeded targets, and a gap analysis informed future programme planning. However, some objectives, such as bespoke training for dispensing practices and digital learning initiatives, remain in development.
- Research and Evaluation has established strong foundations for building a rural evidence base. Academic study programmes and professional development awards have been delivered, supporting 27 MSc participants and 14 small-scale research projects. Evaluation frameworks for key initiatives are in place, but most evaluations are scheduled for completion in 2026. The Rural Practitioner Publishing Award has seen low uptake, and international comparative research outputs are still emerging.
- Recruitment and Retention has progressed more slowly, reflecting the complexity of workforce challenges and systemic barriers. The Rural Recruitment and Retention Stakeholder Network is operational, and pilots such as Making it Work in Skye have generated valuable learning. However, most improvement programmes remain in development, and structural issues, housing, transport and funding models, continue to constrain impact.
- Leadership and Best Practice has achieved its networking target, positioning Scotland within global conversations on rural health. Four practice model projects are underway, including the Rural Leadership Course and Community Training Hub Pilot, but impacts are not yet visible. Awareness of leadership initiatives remains low, and engagement has also been low.
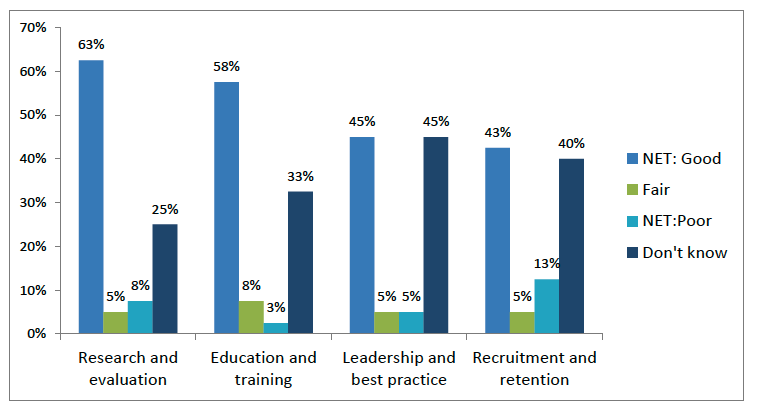
Survey data reflects this mixed picture. Three in five (63%) respondents rated progress in research and evaluation as good or very good, and a similar proportion (58%) said the same so for education and training (Figure 7.1). Ratings were lower for recruitment and retention (43%) and leadership and best practice (45%), with significant proportions selecting “don’t know,” underscoring visibility challenges.
Benefits
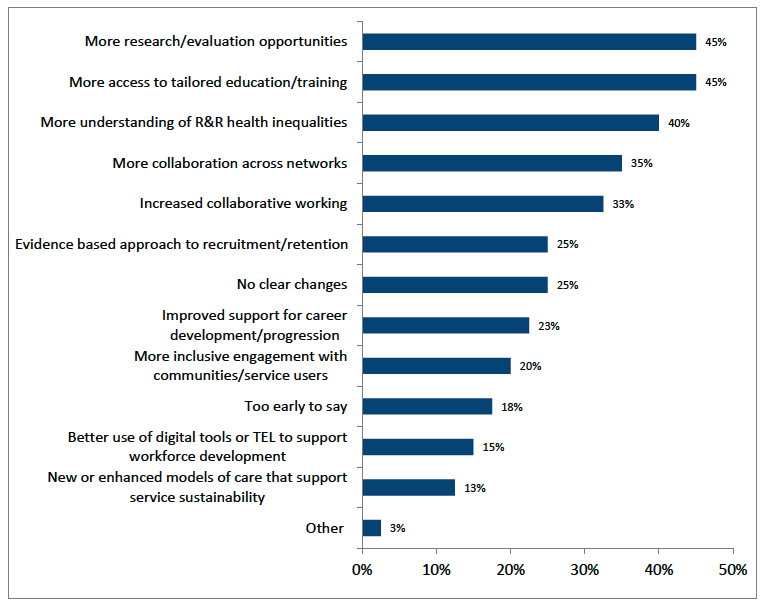
Considering examples of benefits that respondents had personally experienced through the National Centre, nearly half reported expanded access to education and training resources (45%) and increased opportunities for research and evidence-sharing (45%) (Figure 7.2).
Other personal benefits included improved understanding of rural health inequalities (40%) and greater collaboration across networks (35%).
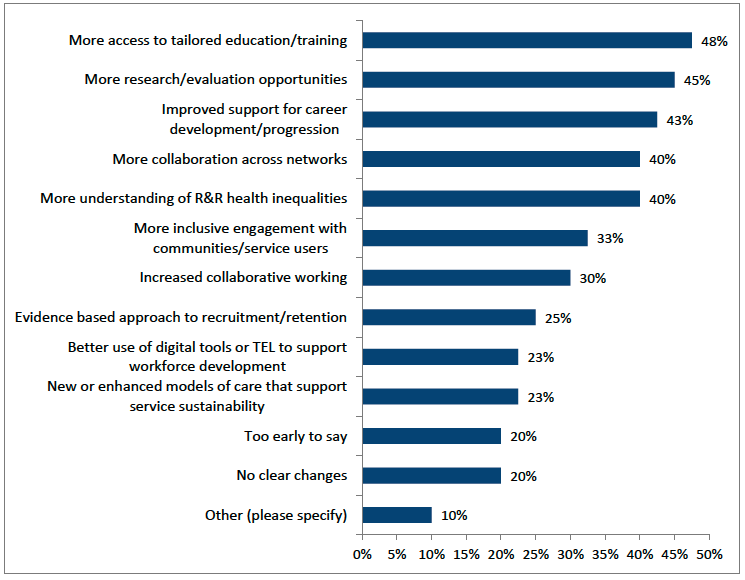
In addition to those experienced personally survey findings show that stakeholders had also observed a range of positive developments on the sector through the National Centre’s activities (Figure 7.3):
- Expanded access to education and training resources tailored to remote and rural health and care (48%).
- Increased opportunities for research, evaluation, or evidence-sharing relevant to rural practice (45%).
- Improved support for professional development and career progression in rural settings (43%).
- Greater understanding of health inequalities faced by remote, rural, and island communities (40%).
- Enhanced collaboration and knowledge exchange across rural health and care networks (40%).
Other areas of perceived progress include more inclusive engagement with rural communities in shaping services (33%), increased collaborative working (30%), and evidence-based approaches to recruitment and retention (25%). Emerging innovations such as new or enhanced models of care (23%) and better use of digital tools for workforce development (23%) were also noted, though these remain at an early stage.
However, one in five (20%) of respondents felt it was “too early to say,” and an equivalent proportion reported “no clear changes”, highlighting the need for stronger visibility and communication about impact.
Personal benefits mentioned in interviews mirrored these trends, with practitioners citing enhanced access to training and research opportunities, stronger professional networks and improved confidence in their roles.
Stakeholder quotes reinforce these findings:
“The Professional Development Awards programme demonstrates how targeted support can enable rural practitioners to access training and research opportunities aligned to their needs.”
Qualitative feedback highlighted the value of targeted support, such as the professional development awards, and the sense of connection fostered by webinars and networks. Examples of these reflections include:
“The co-production of the rural mental health survey with grassroots community members… The development of the Skye Recruitment Group Evaluation Framework is another strong example, providing a practical tool that can be adapted for other rural areas.”
“It's been great to know that you're not alone out there… there’s a willingness to make things better and do research and train you up. Communication was excellent every time I reached out.”
Practitioners described applying learning to service redesign, quality improvement and advanced clinical roles. These developments matter because they begin to address structural challenges, professional isolation, limited CPD access and gaps in rural-specific evidence which have historically undermined workforce sustainability.
However, benefits remain uneven. Engagement has been concentrated among GPs and nurses, with limited reach into pharmacy, optometry, dental and allied health professions. Similarly, while some stakeholders reported applying learning locally, feedback loops into policy and system-level decision-making are underdeveloped.
These examples illustrate that while progress is evident - particularly in education, research, and collaboration - there is still work to do to embed these gains across all pillars and make them visible to a wider audience.
Challenges and Constraints
Despite progress, several challenges persist:
- Visibility and Communication: Many stakeholders were unaware of available resources or unclear about the National Centre’s remit. Reliance on Turas limits reach beyond NHS networks, reinforcing calls for a public-facing portal and proactive outreach.
- Integration Across Pillars: Workstreams have sometimes operated in silos, reducing opportunities for synergy. Stakeholders emphasised the need for a more joined-up approach, with education, research, recruitment and leadership seen as interdependent rather than discrete.
- Inclusivity: Engagement has focused heavily on medical and nursing roles, with insufficient involvement of other primary care professions and community organisations.
- System-Level Barriers: Housing shortages, transport limitations and rigid funding models continue to undermine recruitment and retention efforts, highlighting the limits of what the National Centre can achieve without wider policy interventions.
- Impact Measurement: While outputs are visible, mechanisms to capture and share practical outcomes remain limited, making it harder to demonstrate value and secure ongoing support.
Cross-Cutting Themes
Several themes recur across all four pillars and provide important insights into the Centre’s progress and future direction. First, the inaugural phase has established strong foundations, but visibility remains inconsistent. While credible outputs have been delivered,such as advanced training programmes, supervisory hubs and research networks, many stakeholders are still unaware of these achievements. Improving visibility is therefore critical to translating progress into tangible impact.
Feedback indicates that engagement to date has been perceived as heavily focussed on general practice. Stakeholders consistently called for broader inclusion of other professional groups, particularly pharmacy, optometry, dental and allied health professions, such as dietetics.
Second, stakeholders expressed a need for greater horizontal integration across the National Centre’s pillars. The four pillars were designed as distinct workstreams, yet they are inherently interdependent. Education supports recruitment; research informs leadership; leadership drives retention. Stakeholders repeatedly emphasised that future phases should move away from siloed approaches and adopt a more integrated model. Importantly, staff from the National Centre shared that they have recently adopted a more horizontal, integrated working model, and felt they were already seeing benefits from this shift, including greater opportunities for collaboration and joined up thinking.
Third, community engagement emerged as a consistent priority. Stakeholders called for deeper involvement of local communities and grassroots organisations in shaping solutions, recognising that rural health systems cannot be strengthened without meaningful input from those who live and work in these areas. This includes co-designing interventions and ensuring cultural relevance. As one participant observed:
“You can't get anywhere without engaging with the community… some of them are delivering services because there aren’t any statutory ones. You can’t leave them out.”
Finally, stakeholders expressed strong support for broadening the National Centre’s remit beyond rural primary care. Two in three survey respondents (67%) either strongly or somewhat supported expansion, while only one in ten (10%) opposed this idea. This reflects recognition of the interconnected nature of rural health systems, where boundaries between primary, secondary and social care are often blurred. As one participant noted:
“Sometimes there's a there's a bit of a blurring of boundaries between secondary care and primary care, particularly in rural areas you might get somebody who works in the community but also works in the hospital… it's really important that this work gets expanded to encompass other areas, social care, as well as secondary care and not just rural community primary Health…I think there's so much crossover and intersection with that within rural areas, I think it's really important that we don't ignore these aspects of people's care.”
However, expansion must be carefully managed to avoid diluting the National Centre’s core focus on rural sustainability. Stakeholders emphasised the need for a clear strategic framework and adequate resourcing:
“Primary care is the bedrock of rural health, and we cannot afford to lose focus until the sustainability of rural general practice is secured.”
Several challenges were identified as potential barriers to expansion. Workforce capacity and funding constraints were the most frequently cited (by 53% each), followed by difficulties collaborating across organisations (39%). Other concerns included retention and recruitment of skilled workers, differences in models of care between primary and secondary settings and the complexity of aligning priorities across sectors. These barriers underline the importance of phased expansion, supported by stakeholder engagement and robust governance.
Stakeholders also highlighted factors that would support successful expansion. These included dedicated time and resources for planning and delivery, strong stakeholder commitment and opportunities for international collaboration to share learning. Increased visibility of the National Centre’s work and structured dialogue on secondary care priorities were seen as essential to building consensus and momentum.
Strategic Framework for Future Phases
As the National Centre moves beyond its inaugural phase, there is a clear need to consolidate learning and set out a coherent approach for future delivery. Rather than presenting a rigid blueprint, this section outlines key considerations that should inform the development of a strategic framework for future developments.
First, integration across workstreams must be strengthened. The four pillars -Education and Training, Research and Evaluation, Recruitment and Retention and Leadership and Best Practice - have delivered important outputs, but they have often operated in isolation. Future planning should consider a more horizontal model, where activities are designed as interconnected components of a single programme. This would allow education initiatives to support recruitment, research to inform leadership and leadership development to reinforce retention.
Second, visibility and communication require significant attention. Despite credible achievements, awareness among stakeholders remains uneven. A strategic framework should consider investment in clear, accessible communications and the creation of a public-facing platform to showcase resources, opportunities and impact. This is essential not only for engagement but also for demonstrating value to funders and policymakers.
Third, inclusivity must be a guiding principle. Engagement to date has focused heavily on medical and nursing roles, with limited involvement of pharmacy, optometry, dental and allied health professions. Future planning should consider how to broaden participation and embed co-design with local communities and grassroots organisations, ensuring interventions reflect the realities of rural life.
Fourth, evaluation and impact measurement should be embedded from the outset. While outputs have been delivered, mechanisms to capture and share practical outcomes remain limited. A strategic framework should consider developing indicators for workforce sustainability, service quality and community engagement, alongside processes for feeding learning into policy and practice.
Finally, the framework must acknowledge the structural enablers that underpin rural health systems. Issues such as housing, transport and digital connectivity lie beyond the National Centre’s direct remit, yet they shape the feasibility of recruitment and retention strategies. Future planning should consider how the National Centre can act as an advocate and convenor, working with partners to influence these wider determinants.
Taken together, these considerations point to a future model that is integrated, visible, inclusive, evidence-driven and outward-facing. They also highlight the importance of phased expansion. While there is strong appetite to broaden the National Centre’s remit beyond primary care, this must be managed strategically to avoid diluting core priorities. Potential future phases offer an opportunity to build on progress, scale effective interventions, and position the National Centre as a driver of innovation and equity in rural health and care.
Contact
Email: socialresearch@gov.scot