National Centre for Remote and Rural Health and Care: evaluation
The report is an evaluation of the National Centre for Remote and Rural Health and Care.
Inaugural Phase Targets
The targets for the National Centre’s Inaugural Phase under the Education and Training theme and their overall progress are as follows.
Targets achieved:
- 12 remote and rural (R&R) practitioners funded and supported to complete new Rural ANP level 11 programme.
- 15 rural practitioners were funded to study the MSc programme in 2023.
- An additional 12 were funded and began the programme in 2024.
- New Remote and Rural GP and Rural Practitioner Educational Supervisory Hub established with a range of accessible training and information resources available.
- 1,671 users accessed the Rural Supervision Hub in the National Centre’s first year.
- 12 multiprofessional training sessions
- The National Centre has delivered 32 education and training sessions since October 2023 (14 in 2025, 16 in 2024 and 2 in 2023).
- Gap analysis of training resources
- This scoping review took place throughout the 24/25 year and has informed the planning of the upcoming Rural Leaders Programme, due to begin November 2025.
- Gap analysis completed for existing range of primary care remote and rural education and training resources. CTH completed and Series of Learning events completed including training needs analysis, that has informed diary of events over the last 12 months.
Targets progressed:
- Action plan designed for 5% increase in multidisciplinary primary care undergraduate student placement in remote, rural and island areas per year and evaluation report produced.
- An action plan to support an increase in placements has been delivered.
- Engagement with NMAHP (Nursing, Midwifery and Allied Health Professions Development Framework), HEI and NHS colleagues is ongoing
- Work to identify rural primary care practices most suitable for undergraduate placements.
- The new education and training funding awards are intended to support placements.
- Design and delivery of a new set of learning resources to meet identified needs of dispensing practice staff in R&R areas.
- The National Centre developed bespoke training to address challenges for general practices operating dispensing services. This is due to launch by March 2026.
- Identification and production of 3 priority programmes for Digital/TEL Advanced Technology adaption.
- The June 2025 draft delivery plan sets out this ambition, but further updates are unclear regarding how far along these programmes are.
The intended outcomes from setting and achieving these targets were to produce standardised, efficient training and supervision, as well as to improve access and skills development for the remote and rural workforce.
The inaugural phase has delivered substantial progress on Education and Training, with several targets achieved and others still underway. The commitment to fund 12 remote and rural practitioners for the MSc Rural Advanced Practice programme was met and exceeded, though the long-term impact of this investment will require monitoring. The Remote and Rural Supervisory Hub is operational and has attracted significant use, indicating strong demand for accessible resources.
Other objectives remain in progress. Work to increase undergraduate placements has begun, supported by an action plan and stakeholder engagement, but measurable outcomes are not yet available. Similarly, bespoke training for dispensing practice staff is under development and scheduled for launch by March 2026. While the Centre has delivered more multiprofessional training sessions than planned, and completed a gap analysis to inform future programmes, the identification and delivery of priority digital learning initiatives is still to be finalised.
Summary of National Centre Activities
Since its establishment in October 2023, The National Centre has positioned education and training as a cornerstone of its mission to strengthen healthcare delivery in remote, rural and island communities. Activities under this pillar have included:
- Development of tailored educational resources: The National Centre has produced online modules, guidance documents and case studies designed for rural practitioners, focusing on clinical practice, leadership and service design. These resources aim to address challenges such as professional isolation and limited access to specialist support. For example, an elearning module on menopause was launched and a case study from Dumfries and Galloway on integrating paramedics into primary care.
- Webinars and virtual workshops: These sessions have provided opportunities for knowledge exchange and professional development, with over 1,000 participants recorded across over 30 events (as of June 2025). Topics have included workforce sustainability, integrated care models, and leadership in rural settings. Sessions were delivered online to maximise accessibility for geographically dispersed practitioners.
- Training pathways and Continuing Professional Development (CPD) support: Initiatives have targeted early-career professionals and those transitioning into rural roles, aligning with recruitment and retention objectives. The National Centre has worked to embed these pathways within NES frameworks to ensure consistency and recognition.
- Collaboration with NES and health boards: The National Centre has partnered with health boards to ensure training content reflects workforce needs and policy priorities. This collaboration aligns with Scotland’s GP Recruitment and Retention Action Plan (2024–2026).
These activities have been made accessible primarily through the National Centre’s website and promoted via established communication channels, including email outreach and professional networks.
Reflections
Engagement and Accessibility
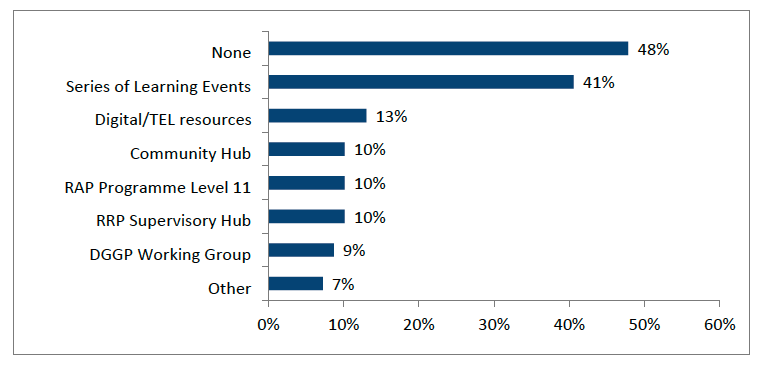
Since the establishment of the National Centre, engagement with education and training activities has been mixed. Almost half of survey respondents (48%, n=73) indicated that they had not accessed any of the National Centre’s education or training activities, highlighting a potential gap in awareness of activities as well as a lack of relevance for certain professional groups. (Figure 3.1).
Amongst survey respondents, the most widely accessed National Centre initiative was the Remote and Rural Health & Care Series of Learning Events, used by 41% of respondents (n=73). Other activities saw lower uptake: 13% accessed digital and technology-enhanced learning resources 13%, 10% accessed the Remote & Rural Practitioner Supervisory Hub (RRP Supervisory Hub), 10% participated in the Rural Advanced Practitioner (RAP) Programme (Level 11),10% used the Community Hub and 9% engaged with the Dispensing GP Practices Education Programme Working Group (DGGP Working Group). A small proportion (7%) reported engaging with other activities not listed.
As was set out in the National Centre’s delivery model, the primary means of accessing the resources was online (83%, n=38), while smaller proportions engaged through blended learning or working groups (Table 3.1). Participants consistently praised the accessibility of webinars and the flexibility of online formats, describing them as “a lifeline” for those working in geographically isolated areas.
| - | % |
|---|---|
| Online | 83 |
| Blended | 23 |
| Self-directed learning | 37 |
| Working group | 26 |
| Other (please specify) | 9 |
However, gaps remain. Stakeholders highlighted limited provision for non-clinical staff and secondary care teams and some expressed frustration at the lack of tailored content for allied health professionals. Notably, secondary care is currently outwith the scope of the National Centre’s work.
Timing was also cited as a barrier, with several participants noting that clinical commitments made it difficult to attend live sessions. These findings suggest that while the National Centre has succeeded in reaching its core audience, further work is needed to broaden engagement and ensure inclusivity.
Feedback and Impact
Feedback from those who took part in the National Centre’s educational activities has been broadly positive. Participants valued the relevance and practicality of resources, with many reporting direct application of learning to their roles.
Examples included improvements in clinical decision-making, enhanced confidence in managing complex cases and strengthened leadership within multidisciplinary teams. One practice manager described using leadership training to restructure rota systems, while others noted that webinars reinforced the importance of integrated, community-linked models of care.
“The National Centre resources have reinforced the importance of multi-disciplinary and community-linked care in rural settings. While they haven’t fundamentally changed how I deliver patient care day-to-day, they have strengthened my confidence in advocating for more joined-up and sustainable models that would benefit our patients.”
“I think a lot of it is valuable workshops and webinars on improving clinical skills and competency, maybe confidence… one of the challenges of sort of working in rural remote areas is that often a healthcare professional is competent, they know what they’re doing, but they lack the confidence to do it without specialists and helpers behind them.”
Beyond individual practice, education initiatives have supported organisational improvements, including quality improvement projects and service redesign. Stakeholders emphasised that these activities are not only building skills but also fostering a culture of continuous improvement in rural health systems.
Application of Learning
Evidence from interviews demonstrates that learning has been applied in diverse ways. Clinicians reported integrating new knowledge into advanced practice roles, district nursing and minor injury care. Others described using insights to inform research projects, develop collaborative networks and mentor colleagues.
The National Centre’s funding awards (Chapter 4) have enabled 14 practitioners to pursue specialist training, research projects, professional development and publication opportunities. One GP was funded for a point-of-care ultrasound fellowship, which was described as “life-changing” for patient care in remote settings.
“The events and resources have allowed rural GPs to connect, share examples, and discuss what works in our different contexts. This is especially important when you are one of very few GPs working in an isolated practice. It has created a sense of shared experience and collective learning that we don’t often get otherwise.”
The National Centre’s Year 1 Progress report notes that in its first year of awards, uptake was lower than expected due to issues related to practitioner time and research confidence. A total of five awards were granted from October 2023 to October 2024.
Educational activities have also contributed to broader system improvements, influencing recruitment strategies and resilience initiatives at community level. However, stakeholders noted that feedback loops into policy remain underdeveloped, limiting the visibility of system-level impacts.
Barriers and Challenges
Despite positive feedback from those who engaged, barriers to accessing or delivering rural-specific training remain. The most common challenges reported were lack of time and training that did not fully align with individual needs. Limited awareness of available opportunities was also highlighted, alongside a perception among some respondents that the trainings offered were not sufficiently relevant or engaging.
A smaller number mentioned issues such as unsuitable formats, lack of supervision and resource constraints for delivering training. While many participants reported no significant barriers, these findings suggest that for some, the main challenge is awareness rather than accessibility.
“Lack of education relevant to needs of AHPs [allied health professionals]- appears very Nurse/ Medical focussed.”
“I've generally either been too busy or I haven't known about them.”
Stakeholders also noted that reliance on Turas[4] for hosting resources limits visibility for those outside formal NHS networks. A public-facing platform was widely recommended to maximise engagement and ensure equitable access.
Looking Ahead
Stakeholders identified clear priorities for the future of The National Centre’s work. These include:
- Expanding educational provision to encompass secondary care and multidisciplinary teams.
- Developing mentorship and peer-learning models to complement formal training.
- Embedding evaluation mechanisms to track outcomes and inform continuous improvement.
- Co-designing content with rural practitioners to ensure relevance and cultural fit.
- Improving visibility and communication - particularly through public-facing platforms beyond Turas.
Assessment of progress
The Education and Training pillar has been central to the National Centre’s inaugural phase, with notable achievements alongside areas where progress remains partial or delayed. Several headline targets have been met or exceeded. The commitment to fund 12 remote and rural practitioners for the MSc Rural Advanced Practice programme was surpassed, with 15 practitioners supported in 2023 and a further 12 commencing in 2024. This represents a significant investment in advanced clinical skills for rural contexts, though the long-term impact on workforce sustainability and patient outcomes will require ongoing monitoring.
The establishment of the Remote and Rural GP and Practitioner Supervisory Hub marks another key success. With over 1,600 users accessing the Hub in its first year, this initiative demonstrates strong early demand for accessible supervision and learning resources. Similarly, the delivery of multiprofessional training sessions has exceeded expectations, with 32 sessions delivered since October 2023 against an initial target of 12. These sessions have provided opportunities for knowledge exchange and skill development across a range of topics, including leadership and integrated care models.
Other targets remain in progress. The action plan to increase undergraduate placements in remote and rural areas has been completed, and engagement with higher education institutions and NHS partners is ongoing. However, measurable outcomes, such as the actual increase in placements, are not yet available. Bespoke training for dispensing practice staff is under development, with launch scheduled for March 2026, and work to identify and deliver priority programmes for digital and technology-enhanced learning has yet to be finalised.
Engagement data highlights mixed uptake. While some initiatives, such as the Supervisory Hub and webinars, have attracted significant participation, survey evidence indicates that nearly half of respondents had not accessed any of the Centre’s education or training activities. Barriers include limited awareness, time constraints and perceived gaps in relevance for non-clinical staff and allied health professionals. Stakeholders also noted that reliance on Turas as the primary hosting platform restricts visibility for those outside formal NHS networks, reinforcing calls for a public-facing platform to improve accessibility.
Feedback from participants has been broadly positive, with many reporting improvements in confidence, clinical decision-making and leadership skills. Examples include the application of learning to rota redesign, quality improvement projects and advanced clinical practice roles. However, feedback loops into policy remain underdeveloped, limiting the visibility of system-level impacts. Stakeholders emphasised the need for stronger evaluation mechanisms to track outcomes and inform continuous improvement.
Looking ahead, priorities for any future phase include expanding educational provision to encompass secondary care and multidisciplinary teams, developing mentorship and peer-learning models and embedding co-design approaches to ensure relevance and cultural fit. Improving communication and visibility, particularly through platforms beyond Turas, will be critical to broadening engagement and addressing current gaps.
In summary, the inaugural phase of Education and Training has delivered tangible benefits, strengthening skills and connectivity among rural practitioners. While progress against several targets is commendable, challenges remain around inclusivity, awareness and the timely delivery of digital learning initiatives. Addressing these issues will be essential to maximise impact and ensure alignment with the Centre’s long-term objectives.
Contact
Email: socialresearch@gov.scot