National Centre for Remote and Rural Health and Care: evaluation
The report is an evaluation of the National Centre for Remote and Rural Health and Care.
Chapter 6: Leadership and Best Practice
The Leadership and Best Practice pillar aims to raise the profile of rural healthcare and promote models of excellence through collaboration and innovation. This pillar focuses on building leadership capacity, sharing effective practice and connecting Scotland to national and international networks. The following section reviews achievements and ongoing work to strengthen leadership and knowledge exchange in remote and rural health systems.
Inaugural Phase Targets
The National Centre’s targets for its Inaugural Phase work in Leadership and Best Practice are as follows.
Targets achieved:
- Establish new national and international R&R networks for engagement and knowledge exchange
- The National Centre established the National Network for Engagement and Knowledge Exchange on R&R Research and Evaluation in Scotland, the National Centre R&R Recruitment and Retention Stakeholder Engagement Network.
Targets progressed:
- Design and delivery of 5 practice model projects that promote improved delivery of R&R Primary Care healthcare delivery.
- The National Centre has designed four practice model projects, at different stages of delivery:
- Scoping and creating the Rural Leadership Course, due to begin in November 2025
- The Community Training Hub Pilot for knowledge exchange, education and training resources, the site for which was complete by September 2025.
- Paramedics in Rural Primary Care, a case study for which was published in March 2025.
- Rural Advanced Practice MSc, which was planning for its third cohort as of September 2025.
- The National Centre has designed four practice model projects, at different stages of delivery:
The Leadership and Best Practice pillar has achieved some key milestones while others remain in progress. The National Centre successfully established national and international networks for engagement and knowledge exchange, creating platforms to share learning and strengthen collaboration.
Progress has also been made on practice model projects, with four initiatives underway: the Rural Leadership Course (due to launch in November 2025), the Community Training Hub Pilot (site completed by September 2025), a published case study on paramedics in rural primary care, and continued delivery of the Rural Advanced Practice MSc. These developments indicate strong foundations for promoting models of excellence, though full delivery of all five planned projects will be required to meet the inaugural phase target.
Summary of National Centre Activities
Since October 2023, The National Centre has been focussing its leadership and best practice efforts on building networks for knowledge sharing and collaboration and developing its rural leaders programme.
- Joining National and International Networks: The National Centre mapped out national and international networks to share knowledge and good practice, models of education delivery, recruitment, retention, research and education. Engagement is ongoing with international locations including Australia, New Zealand and the USA.
- Additionally, The National Centre established new rural networks to drive collaboration, knowledge exchange, and innovation in remote and rural healthcare: the Recruitment and Retention Stakeholder Network, the Research and Evaluation Network and Education and Training International Network, which engage over 250 stakeholders across Scotland and internationally.
- Preparing for the Rural Leaders Programme: The National Centre is planning a rural leadership education opportunity to enhance service sustainability and workforce capacity in remote and rural settings. They completed a scoping exercise of rural leadership education courses, a stakeholder survey and have been planning the programme based on the findings of this work. This was due to launch in November 2025, making the impacts out of scope for this evaluation.
Reflections
The evaluation considered awareness of and involvement in leadership and best practice work led by the National Centre.
Awareness
Awareness of ongoing work under this pillar was low compared to the others.
Half (50%) of survey respondents said they were aware of work starting in the National Centre on rural leadership, while the other half (50%) were not (Table 6.1). And just under half (47%) were involved in or aware of national or international rural and remote networks for knowledge sharing or collaboration. Only one in nine (11%) were involved in National Centre leadership working groups or practitioner model projects.
| - | Yes (%) | No (%) |
|---|---|---|
| Awareness of work starting in the National Centre on rural leadership | 50 | 50 |
| Involved in or aware of any national or international rural and remote networks for knowledge sharing or collaboration | 47 | 53 |
| Involved in any National Centre leadership working groups or practitioner model projects aimed at improving primary care delivery | 11 | 89 |
Network involvement
Some of the networks mentioned by respondents include the Rural GP Association of Scotland (RGPAS), the remote rural and island researchers Teams network, World Organisation of Family Doctors (WONCA), European Rural Isolated Practitioners Association (EURIPA), the NES Remote and Rural and Islands Researchers Microsoft Teams Channel and the Contact Help Advice and Information Network (CHAIN).
One stakeholder described how The National Centre has successfully been getting Scotland involved in international networks for knowledge sharing, such as the CHAIN network:
“[National Centre representative] was key to the development of the CHAIN network. thinking how you could have those conversations. And the idea of the CHAIN network is about dissemination of information.”
They went on to explain the significant long-term value from being involved in these international networks, emphasising that benefits will continue to be realised into the future:
“One thing is, especially with WONCA or EURIPA, is you're in the conversation. And then that sparks off, future ideas, people working into groups. So, within EURIPA, we've just set our research priorities and so then we're setting up collaborative teams to take it forward.”
Model projects
The stakeholders who said they had been involved in The National Centre’s leadership working groups or practitioner model projects were asked what those were. Respondents mentioned the Rediscover the Joy of General Practice evaluation, the Education and Training Funding awards and the Paramedics in Rural Primary Care work with the Scottish Ambulance Service.
Benefits from engaging with this work included connecting with new colleagues or services, sharing examples of good practice, applying new models or ideas in one’s work, influencing change locally and gaining more confidence in a leadership role.
One stakeholder, who has not been directly involved, but has been following The National Centre’s work online, described how they were hoping to adopt some of the approaches they learned about in their own area, including the Paramedics in Rural Primary Care.
“Some of the things related to minor injuries, which will be something that we might try and approach in the same way as has been done as a pilot in Dumfries and Galloway. So there, the paramedics are changing from being just acute here to being more involved in the training in chronic conditions, long term conditions.”
They also spoke about the value in the National Centre’s work in disseminating information and sharing examples of strategies working in places facing similar challenges. They specifically mentioned some of the ongoing work in recruitment and retention and remote imaging work in Shetland:
“We want to try and attract carers into the area. Some of that relates to, we need to give better housing, more affordable housing, different type of housing, and we need to look at how other areas around that are more remote are managing things…Interested in the remote use of imaging X-rays in Shetland, some projects like that going on. And they're not impossible to try and implement with a bit of effort, so these are things we're interested in.”
International profile
One of the National Centre’s goals is to become an international leader in rural healthcare. International survey respondents and interviewees from the USA and Australia commended the National Centre for its progress in this area. In addition to getting involved in international networks for knowledge sharing, one participant spoke about an opportunity they had to visit Scotland learn about the work the National Centre has been doing and promoting some of their strategies and care models back in their home country.
They spoke with gratitude about how supportive colleagues from the National Centre have been in helping them accomplish this, including National Centre colleagues coming to speak with representatives from their home government, particularly about the Dispensing General Practice and non-doctor prescribing work.
Respondents who worked in other countries, including Australia, the United States, England and Wales, confirmed they thought the National Centre was making good progress on building their international profile and positioning Scotland as a leader in rural healthcare.
Rural leaders programme
A few stakeholders, primarily those who worked at NES, said they were aware of ongoing work to develop a rural leadership programme. The National Centre first did scoping work to identify existing leadership courses and launched a rural leadership survey in January 2025 to Centre stakeholders. They also advertised this on NES platforms and social media to gather views on what stakeholders would like to see in a rural leadership course for Scotland. Additionally, they created a working group of rural healthcare leaders to develop the course, the pilot for which is due to launch towards the end of 2025.
At the time of the evaluation interviews, the course was still being developed, but some ideas were to use action learning sets with real examples of challenges of what senior rural leaders are facing. Mentorship and support for leaders on the course was also a key consideration mentioned.
However, most stakeholders who did not work at NES/the National Centre were unaware of this work.
Support for work in leadership and networks
While awareness of leadership and network activities was lower than awareness of ongoing work under the other pillars, stakeholders were very supportive of work being done to strengthen networks and leadership opportunities in rural areas.
Many emphasised the value of having practitioner networks for those working in remote or isolated areas where there may be limited support available in the immediate vicinity. One healthcare professional shared the importance of peer support in their work in getting advice and assurance on the unique challenges faced when providing care in remote and rural areas:
“Peer support is really important when you're working on your own. You want to be able to discuss this with somebody else and say, what do you think? Have I done this right?”
Similarly, mentorship networks, particularly for new or early career practitioners in isolated places, was suggested as something which could aid in recruitment and retention, instilling confidence in healthcare providers and providing support where it’s needed:
“They're in a rural community. It's hard going if you've got no support. And it's thinking about how you can get that, in a way, a mentorship scheme going. So that they can mentor them into the places. And if they get worried there's somebody they can phone.”
One stakeholder said that they thought remote and rural networks should also be made accessible for students and unpaid carers, as those doing these types of work would also benefit from greater support:
“I think a remote and rural network for healthcare students - and I'm focused on students. It shouldn't just be for students. When you think about this more widely, where are the networks to support care workers? Where are the networks to support unpaid careers? Just because these people are professionals, they're part of networks, but why can't anybody that works in healthcare or indeed in remote and rural locations, why shouldn't they have a supportive network?”
The importance of confident leadership in rural areas was also mentioned by many stakeholders, particularly when considering the bespoke challenges rural practitioners could experience compared to those working in urban centres, including having to make decisions under high pressure with fewer resources:
“Recognising how do you lead a team in a low resource environment? How do you lead a Team when you don't have backup 15 minutes away, 5 minutes away?”
“Highlighting the differences in [rural] leadership [compared to urban] and I think courageous decision making. Having the confidence to say, ‘yeah, we need to do this’. It should be highlighted a little bit more because [remote practitioners] probably have to make more clinical decisions without any other support than any other area.”
One healthcare professional specified this is especially the case for district nurses, who provide care in homes:
“[District nurses] don't have access to the Internet, they don't have access to mobile phone coverage. They might not even have access to hot water or electricity in some of the houses. They are so remote and rural that they are not going to get help within a few hours…There is a very high pressure, and you need to be confident in what you're doing to provide that service because you are it and you are the only backup.”
Underscoring the importance of strong leadership in rural healthcare, stakeholders offered a few suggestions for work which the National Centre could support to facilitate this. One described a developing a leadership pathway to identify and support clinicians who are interested in becoming leaders to build the confidence and skills they need:
“There needs to be an intentional pathway to develop leaders in rural, remote and island communities while they're still clinicians but who have expressed an interest in being a manager one day or a director or even just a supervisor … more than just a webinar, an intentional programme of leadership development.”
This suggests that the work being done to develop the rural leaders programme described above could be more widely communicated amongst stakeholders to increase awareness and allow for broader input.
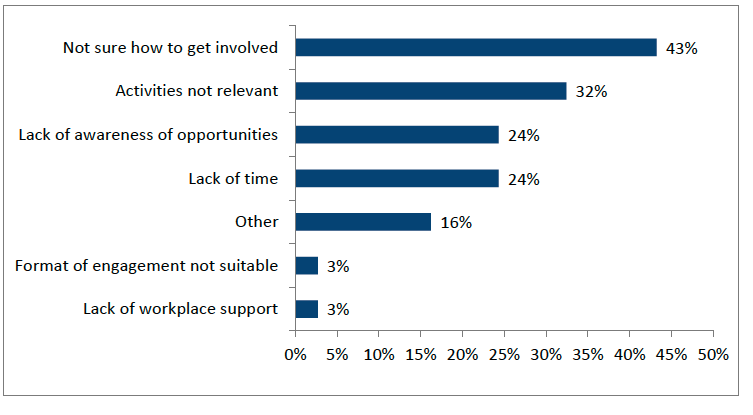
Barriers
The evaluation also examined some of the factors underlying the low engagement with the National Centre’s leadership or network activities. The most cited barriers were not being sure how to get involved or not seeing relevant activities (Figure 6.1). Lack of time and lack of awareness of opportunities to engage with this work were also frequently identified barriers or challenges to engaging with leadership or network activities.
Looking Ahead
Looking forward, stakeholders suggested the following priorities under Leadership and Best Practice:
- Networking opportunities for students: Provide peer-based support for students who are working, placed or want to work in remote and rural areas.
- Progressing with the Rural Leaders Programme: Establish and promote strong leadership in remote and rural areas.
- Greater mentorship opportunities: Increased support for early-career clinicians in remote and rural areas to improve recruitment and retention.
- Continue joining and fostering rural networks: Remain engaged in conversations nationally and internationally to share best practice in remote and rural healthcare.
- Promoting work in this area: Broaden understanding and recognition of the National Centre’s ongoing work in Leadership and Best Practice, as many stakeholders were unaware of what was happening in this area.
Assessment of progress
The Leadership and Best Practice pillar has achieved some notable successes while other areas remain in development. The National Centre met its target of establishing national and international networks for engagement and knowledge exchange, creating platforms that connect over 250 stakeholders and position Scotland within global conversations on rural healthcare. These networks have facilitated collaboration and shared learning, though evidence of tangible outcomes from international partnerships is still lacking.
Progress on practice model projects has been more limited. Four initiatives are underway: the Rural Leadership Course, scheduled to launch in November 2025; the Community Training Hub Pilot, with its site completed by September 2025; a published case study on paramedics in rural primary care; and continued delivery of the RAP MSc. While these developments represent strong foundations, the full target of five practice model projects has not yet been met, and most initiatives are at early stages, meaning their impact cannot yet be assessed.
Awareness and engagement with leadership and best practice activities remain relatively low compared to other pillars. Survey data shows that only half of respondents were aware of work on rural leadership, and just 11% reported involvement in leadership working groups or practitioner model projects. Barriers include lack of time, uncertainty about how to engage, and limited visibility of opportunities.
Despite this, stakeholders expressed strong support for the National Centre’s efforts to strengthen networks and leadership capacity, highlighting the value of peer support and mentorship for practitioners working in isolated settings. Many emphasised the importance of confident leadership in rural contexts, where decision-making often occurs under high pressure with limited resources.
Looking ahead, priorities include progressing the Rural Leaders Programme, expanding mentorship opportunities, and improving communication to raise awareness of leadership initiatives. Stakeholders also called for networking opportunities for students and unpaid carers, alongside continued engagement in international collaborations to share best practice.
In summary, the inaugural phase has delivered important groundwork for leadership and knowledge exchange, but greater visibility, broader participation, and completion of planned projects will be essential to realise the intended outcomes of this pillar.
Contact
Email: socialresearch@gov.scot