Potentially hazardous agents in land-applied sewage sludge: human health risk assessment
This report on the risks to human health is part of the research project undertaken by the James Hutton Institute on the impacts on human health and environment arising from the spreading of sewage sludge to land (CR/2016/23).
3.4. Pharmaceuticals and personal care products
3.4.1. Background
Pharmaceuticals and personal care products (PPCPs) are used for health or cosmetic purposes, and include products used on both animals and humans. A diverse collection of thousands of chemical substances can be classed as PPCPs, comprising prescription and over-the-counter medicines, veterinary medicines, fragrances and cosmetics.
Pharmaceuticals are designed to modify biochemical and physiological functions of biological systems in humans and animals – these properties can unintentionally influence the behaviour and fate of microorganisms in the soil or water should their habitats become contaminated with these compounds. Major groups of pharmaceuticals include antibiotics including antimicrobials, antivirals, etc., disinfectants, steroids, hormones and nutraceuticals, as well as their various degradation products. Some pharmaceutical compounds are easily broken down and processed in the human or animal body, whilst in other cases, a significant proportion of the compounds and their metabolites are eliminated through urine or faeces. Through these routes, some pharmaceuticals and their degradation products enter the wastewater stream, and many compounds have been detected in sewage sludge produced by wastewater treatment.
Unlike pharmaceuticals, personal care products such as cosmetics, shampoos and lotions, are directly washed into wastewater during showering and bathing, and hence enter waste water treatment. Many of these compounds and their degradation products have been detected in sewage sludge (e.g. Richardson et al., 2005). Once present in sewage sludge, there are both theoretical and measured pathways by which PCPPs can pass from sewage sludge up the food chain resulting in human exposure (Latare et al., 2014).
Numerous studies report a range of different classes of pharmaceuticals in domestic sewage, including: antibiotics, antiepileptics, anticoagulants, analgesics and anti-inflammatories, lipid regulators, steroidal compounds, cosmetics, psycho-stimulants (Luo et al., 2014). Several studies have showed that the fate and transport of these compounds varies during wastewater treatment, with some compounds completely degraded and some only partly degraded (WHO, 2012).
The half-lives of various PPCPs in sewage sludge applied to land have been investigated by a number of authors. Walters et al. (2010) collated data from a number of previous studies and compared these with their own empirical evidence from pot incubation studies. The results indicated that the 'environmental half-lives' were greater than those from controlled laboratory experiments, as well as values calculated in chemical fate models. This was thought to be due to a variety of factors:
1. Binding of the compounds within the sewage sludge matrix, reducing their bioavailability
2. The presence of complex mixtures that may inhibit microbial activity and limit degradation
3. The water content of the matrix
4. The quantity of readily available nutrients
5. Ambient temperatures
6. Microbial adaptation / acclimatisation to the compounds of interest
7. The initial concentration of the compounds of interest
To compensate for this potential underestimation in fluxes of PPCPs from the multi-media fugacity modelling used in this study (Section 2.2.2), the exposure assessment of the risk modelling has adopted 'reasonable worst case' assumptions that will tend towards over-estimating exposure (see Section 2.2).
Other studies have investigated the uptake of PPCPs from sewage sludge into crops/food chain. For example, Wu et al. (2010) reported findings from a greenhouse experiment in which the uptake of three pharmaceuticals (carbamazepine, diphenhydramine, and fluoxetine) and two personal care products (triclosan and triclocarban) by soybean grown in sewage sludge-amended soil was measured. Carbamazepine, triclosan, and triclocarban were found in both root tissues and above ground plant parts, whereas uptake and translocation for diphenhydramine and fluoxetine was limited. Holling et al. (2012) reported findings from greenhouse studies with Chinese cabbage where sewage sludge was applied at normal agronomic rates. Concentrations of carbamazepine, sulfamethoxazole, salbutamol, triclosan and trimethoprim in soils and crop (shoots and roots) were determined. Sulfamethoxazole was only detected in the roots, whilst the other compounds were found in both roots and shoots. Shargil et al. (2015) found estrone and testosterone in lettuce plants grown in soils amended with sewage sludge at rates equivalent to 500 kg total N ha-1. However, the experimental design suffered from low statistical power and it was not possible to make strong inferences from these data with respect to sewage sludge being a source of estrone and testosterone in the food chain.
Overall, there is an increasing body of evidence showing that certain PCPP compounds introduced to soils via sewage sludge can be taken up by a range of crop plants, and into those parts of the plants that are normally consumed by humans (and animals). Ecotoxicologic impacts are also evident, and while not a direct health impact on humans can be seen as an indication of potential impacts on living organisms, including humans. For example, Carter et al. (2016) showed that earthworms could accumulate a number of pharmaceutical compounds (fluoxetine, carbamazepine, diclofenac and orlistat), while Konradi & Vogel (2013) studied cirpofloxacin, sulfamtheoxazole, ofloxcin and clarithromycin; recommending that the presence of these and other antibiotics in sewage sludge is monitored to mitigate risks of change to soil microbial populations. Toxicity and fate data are still absent (or insufficient) for many emerging substances of concern (Higgins et al., 2010), but risk assessments have already been undertaken for a number of PCPPs.
Previous risk assessments
The Norwegian Food Safety Authority conducted a risk assessment for a number of chemical hazards in sewage sludge, relevant to application of sludge to agricultural land (Eriksen et al., 2009). A total of 14 pharmaceuticals were included in the assessment based on previous investigations undertaken by the Norwegian Pollution Control Authority. The risk assessment used the classical source-pathway-receptor approach, using 12 different exposure routes in order to evaluate the risks to "soil living organisms, the aquatic environment, grazing animals, animals eating feed based on plants from sludge treated soil, children eating soil, and humans consuming drinking water, crop plants and/or meat affected by the use of sludge as soil conditioner" (Eriksen et al., 2009).
The overall conclusion of the risk assessment was that exposure to the hazards considered was likely to be at levels well below predicted no-effect concentration (PNEC) values in most cases and should not constitute a significant risk to humans and biota. The risks of antibiotic resistance were also evaluated, and it was deemed unlikely for most antibiotics analysed, with the possible exception of ciprofloxacin, due of its persistence and mobility in soils. Those compounds recommended for further study as a result of this project are listed in Table 3‑8.
A qualitative assessment by Smith (2009) identified over a dozen PPCPs or classes of compounds present in sewage sludge (Table 3‑8). The main conclusion was that the overall risk to crop yields, animal health, groundwater, surface water, and air quality was low when applying sewage sludge according to European and British regulations. Smith (2009) also identified several "possible risks" to human health and soil fertility from land application of sewage sludge, where "there is some reported evidence that current operational practice may result in a potential impact on the environment on the basis that one or [both] of the following conditions apply: there is uncertainty about the environmental implications of particular sludge components, [and/or] effects may occur under certain extreme 'worst-case' conditions, given the current regulations and codes of practice." In a more recent assessment (Clarke & Smith, 2011), different groups of PPCPs were ranked to determine research priorities on the effects of chemical hazards after land application of sewage sludge. The following criteria were used to develop a priority index ranging from 0 to 11 points, with a higher index representing a higher priority for research and monitoring.
The prioritised list of chemicals is presented in Table 3‑8. Triclosan and triclocarban were given the highest score (7/11), followed by benzothiazoles, antibiotics and synthetic musks. The lowest priority index was given to quaternary ammonium compounds (QACs), steroids, phthalate acid esters (PEAs), and polydimethylsiloxane (PDMS).
| Imperial College Reviews | Danish Risk Assessment | Norwegian Risk Assessment | WEAO Reports | EPA Research Report | CIP2 Sludge Investigations | |
|---|---|---|---|---|---|---|
| Smith 2009(a) | Clarke & Smith 2011(a) | Jensen et al 2012 | Eriksen et al 2009 | WEAO 2010, 2001 | Healy et al 2017 | Gibbs & Jones 2017 |
|
|
|
|
|
|
|
(a) Values correspond to average concentrations in sewage sludge (mg kg-1 DW)
(b) These compounds were not formally risk assessed due to data limitations
3.4.2. Risk Assessment
Chemicals listed in Table 3‑8 were included in the risk assessment if; (i) their primary application was for pharmaceutical or personal care products, (ii) if reliable distribution coefficients were available that satisfied the requirements of the multi-media fugacity models (Section 2.2.2). The full list of pharmaceutical and personal care products (PPCPs), their physico-chemical properties and reference doses (RfD) are listed in Table 3‑9.
| Chemical | Water solubility (mg l-1 @ 25C) | Vapour pressure (mm Hg @ 25C) | Henry's constant (atm-m3 mol-1) | Log KOW | RfD (mg kg-1 d-1) / Uncertainty Factor |
|---|---|---|---|---|---|
| Triclocarban | 2.37x10‑3 (USEPA 2012) | 3.60x10-9 (USEPA 2012) | 4.50x10-11 (NCCT) | 4.90 (USEPA 2012) | 2.50x10-3 / 10000 (HPVIS) |
| Triclosan | 1.00x101(a) (Yalkowsky et al 2010) | 4.60x10-6(a) (USEPA 2012) | 2.10x10-8 (NCCT) | 4.76 (NITE 2012) | 3.00x10-1 / NR (ACToR) |
| Carbamazepine | 1.80x101 (USEPA 2004) | 1.84x10-7 (USEPA 2004) | 1.10x10-10 (NCCT) | 2.45 (Dal Pozzo et al 1989) | 3.00x10-2 / 10000(c) (ToxRefDB) |
| Cyclomethicone 5 (Decamethylcyclopentasiloxane) | 1.70x10-2 (Kochetkov et al 2001) | 3.00x10-1 (ECHA 2015b) | 3.30x101 (NCCT) | 8.06 (Xu et al 2014) | 1.00x10-1 / 10000 (EPA Chem Dash) |
| Cyclomethicone 6 (Dodecamethylcyclohexasiloxane) | 5.10x10-3(b) (Varaprath et al 1996) | 1.69x10-2 (Lei et al 2010) | 2.50x101 (NCCT) | 8.87 (Xu et al 2014) | 1.50x10-1 / 10000 (EPA Chem Dash) |
| Caffeine | 2.16x104 (Yalkowsky et al 2010) | 9.00x10-7 (Emel'yanenko & Verevkin 2008) | 1.10x10-11 (NCCT) | -0.07 (Hansch et al 1995) | 8.00x10-4 / 10000 (EPA Chem Dash) |
| Diclofenac | 2.37x100 (Fini et al 1986) | 6.14x10-8 (USEPA 2012) | 1.55x10-10 (USEPA OPERA) | 4.51 (Avdeef 1987) | 4.00x100 / 10000(d) (Derived from Dietrich et al 2010) |
| Ibuprofen | 2.10x101 (Yalkowsky & Dannenfelser 1992) | 4.74x10-5 (Daubert & Danner 1989) | 1.50x10-7 (NCCT) | 3.97 (Avdeef 1993) | 2.00x10-4 / 10000(e) (Derived from Nallani et al 2011) |
| Atorvastatin | 1.12x10-3 (USEPA 2012) | 6.56x10-10 (USEPA OPERA) | 2.40x10-23 (NCCT) | 6.36 (USEPA 2012) | 1.00x10-3 / 10000(f) (Derived from Richards & Cole 2006) |
| Atenolol | 1.33x104 (McFarland et al 2001) | 1.11x10-9 (USEPA OPERA) | 4.35x10-10 (USEPA OPERA) | 0.16 (Hansch et al 1995) | 1.00x10-3 / 10000(g) (Derived from Zhang & Gong 2013) |
| Erythromycin | 2.00x103(h) (O'Neil 2006) | 2.12x10-25 (USEPA 2009a) | 1.28x10-11 (USEPA OPERA) | 3.06 (McFarland et al 1997) | 1.50x10-3 / 10000 (EPA Chem Dash) |
| Azithromycin | 2.37x100 (USEPA 2012) | 2.65x10-24 (USEPA 2012) | 1.33x10-11 (USEPA OPERA) | 4.02 (McFarland et al 1997) | 1.50x10-3 / 10000(i) (Derived from EPA Chem Dash) |
| Clarithromycin | 1.69x100 (USEPA 2012) | 2.32x10-25 (USEPA 2012) | 1.01x10-10 (USEPA OPERA) | 3.16 (McFarland et al 1997) | 1.00x10-1 / 10000(j) (Derived from Isidori et al 2005) |
| Ciprofloxacin | 3.00x104 (Nowara et al 1997) | 2.85x10-13 (USEPA 2012) | 9.46x10-12 (USEPA OPERA) | 0.28 (Takács-Novák et al 1992) | 1.33x10-1 / 100 (Derived from USFDA max therapeutic dose) |
| Metformin | 1.06x106 (USEPA 2012) | 7.58x10-5 (USEPA 2012) | 7.60x10-16 (NCCT) | -2.64 (USEPA 2012) | 5.00x10-1 / 100 (Derived from USFDA max therapeutic dose) |
| Ranitidine | 2.47x101 (Gerhartz1985) | 2.99x10-9 (USEPA OPERA) | 7.29x10-9 (USEPA OPERA) | 0.22 (USEPA OPERA) | 1.00x10—2 / 10000 (Derived from LD50 in rats Acute Tox) |
| Sertraline | 0.35x10-1 (Drugbank) | 3.36x10-6 (USEPA OPERA) | 1.15x10-6 (USEPA OPERA) | 4.55 (USEPA OPERA) | 1.00x10-3(k) / 10000 (Derived from Richards & Cole 2006) |
| Norsertraline | 1.04x10-6 (USEPA OPERA) | 1.07x10-9 (USEPA OPERA) | 6.43x10-7 (USEPA OPERA) | 4.94 (USEPA OPERA) | 1.00x10-3(l) / 10000 |
| Tamoxifen | 1.67x101 (USEPA 2004) | 3.46x10-8 (USEPA 2004) | 2.21x10-8 (USEPA OPERA) | 6.30 (USEPA 2004) | 4.00x10-5(m) / 10000 (Derived from Cevasco et al 2008) |
| Dipyridamole | 9.22x102 (Human Metabolome Database) | 9.30x10-10 (USEPA OPERA) | 1.21x10-11 (USEPA OPERA) | 2.06 (USEPA OPERA) | 1.68x10-2 / 10000 (Derived from LD50 in rats Acute Tox) |
| Fexofenadine | 2.40x10-2 (USEPA 2004) | 2.56x10-9 (USEPA OPERA) | 2.51x10-8 (USEPA OPERA) | 2.81 (USEPA 2004) | No Tox Data Available |
| Gabapentin | 4.49x103 (USEPA 2012) | 2.94x10-10 (USEPA 2012) | 4.87x10-8 (USEPA OPERA) | -1.10 (Sangster 2005) | 2.00x10-1 / 100 (Derived from USFDA maximum theraputic dose) |
| Levetiracetam | 1.04x105 (Thomson & Montvale 2007) | 3.50x10-6 (USEPA 2004) | 1.77x10-9 (USEPA OPERA) | -0.49 (USEPA 2004) | 6.00x10-1 / 100 (Derived from USFDA maximum theraputic dose) |
| Sotalol | 5.51x103 (Drugbank) | 2.19x10-10 (USEPA OPERA) | 1.25x10-9 (USEPA OPERA) | 0.55 (USEPA OPERA) | 5.00x10-2 / 100 (Derived from USFDA maximum theraputic dose) |
| Benzothiazole | 4.30x100 (Human Metabolome Database) | 1.60x10-2 (USEPA OPERA) | 9.53x10-6 (USEPA OPERA) | 2.05 (USEPA OPERA) | 5.10x10-4 / 10000 (USEPA Chem Dash) |
(a) at 20C; (b) at 23C; (c) Low confidence - derived from USGS screening level; (d) Very low confidence - derived from lowest point of departure from ecotoxicologic study with water fleas; (e) Very low confidence – derived from lowest point of departure from ecotoxicologic study with catfish; (f) Very low confidence – derived from lowest point of departure from ecotoxicologic study with frog larvae; (g) Very low confidence – derived from lowest point of departure from ecotoxicologic study with zebradanio fish; (h) 28C; (i) Very low confidence – assumed the same RfD as Arythromycin; (j) Very low confidence – derived from lowest point of departure from exotoxicologic study with zebradanio fish; (k) Very low confidence – derived from lowest point of departure from ecotoxicologic study with frog larvae; (l) Very low confidence – assumed to have the same RfD as Sertraline; (m) Very low confidence – derived from lowest point of departure from ecotoxicologic study with frog larvae;
Initial concentrations in sewage sludge were set based on the 'realistic worst case' paradigm (WRAP 2016c; Hough et al. 2012). A series of recent reviews documenting measured concentrations in sewage sludge were used and starting concentrations were derived from 90%ile values reported in these data sets (Table 3‑10).
| Chemical (IUPAC) | Concentration in sewage sludge (mg kg-1) | Reference(s) |
|---|---|---|
| Triclocarban (1-(4-Chlorophenyl)-3-(3,4-dichlorophenyl)urea) | 2.21x102 | USEPA 2009b |
| Triclosan (5-Chloro-2-(2,4-dichlororophenoxy)phenol) | 4.74x100 |
|
| Carbamazepine (5H-Dibenzo[b,f]azepine-5-carboxamide) | 2.09x10-2 |
|
| Cyclomethicone 5 (2,2,4,4,6,6,8,8,10,10-decamethyl-1,3,5,7,9,2,4,6,8,10-pentaoxapentasilecane) | 2.58x103 | Harrison et al 2006 |
| Cyclomethicone 6 (2,2,4,4,6,6,8,8,10,10,12,12-dodecamethyl-1,3,5,7,9,11-hexaoxa-2,4,6,8,10,12-hexasilacyclododecane) | 2.58x103 | Harrison et al 2006 |
| Caffiene (1,3,7-Trimethylxanthine) | 4.96x10-2 |
|
| Diclofenac (2-(2,6-dichloranilino) phenylacetic acid) | 6.00x10-5 |
|
| Ibuprofen (2-(4-Isobutylphenyl)propanoic acid) | 2.70x10-4 |
|
| Atorvastatin ((3R,5R)-7-[2-(4-fluorophenyl)-3-phenyl-4-(phenylcarbamoyl)-5-propan-2-ylpyrrol-1-yl]-3,5-dihydroxyheptanoic acid) | 8.73x10-2 | Gibbs & Jones 2017 |
| Atenolol (2-[4-[2-hydroxy-3-(propan-2-ylamino)propoxy]phenyl]acetamide) | 4.76x10-1 |
|
| Erythromycin ((3R,4S,5S,6R,7R,9R,11R,12R,13S,14R)-6-[(2S,3R,4S,6R)-4-(dimethylamino)-3-hydroxy-6-methyloxan-2-yl]oxy-14-ethyl-7,12,13-trihydroxy-4-[(2R,4R,5S,6S)-5-hydroxy-4-methoxy-4,6-dimethyloxan-2-yl]oxy-3,5,7,9,11,13-hexamethyl-oxacyclotetradecane-2,10-dione) | 7.82x10-2 |
|
| Azithromycin ((2R,3S,4R,5R,8R,10R,11R,12S,13S,14R)-11-[(2S,3R,4S,6R)-4-(dimethylamino)-3-hydroxy-6-methyloxan-2-yl]oxy-2-ethyl-3,4,10-trihydroxy-13-[(2R,4R,5S,6S)-5-hydroxy-4-methoxy-4,6-dimethyloxan-2-yl]oxy-3,5,6,8,10,12,14-heptamethyl-1-oxa-6-azacyclopentadecan-15-one) | 1.06x10-1 |
|
| Clarithromycin ((3R,4S,5S,6R,7R,9R,11R,12R,13S,14R)-6-[(2S,3R,4S,6R)-4-(dimethylamino)-3-hydroxy-6-methyloxan-2-yl]oxy-14-ethyl-12,13-dihydroxy-4-[(2R,4R,5S,6S)-5-hydroxy-4-methoxy-4,6-dimethyloxan-2-yl]oxy-7-methoxy-3,5,7,9,11,13-hexamethyl-oxacyclotetradecane-2,10-dione) | 1.38x10-1 |
|
| Ciprofloxacin (1-cyclopropyl-6-fluoro-4-oxo-7-piperazin-1-ylquinoline-3-carboxylic acid) | 6.49x10-1 |
|
| Metformin (1,1-Dimethylbiguanide) | 4.00x101 |
|
| Ranitidine (6.N (2-(((5-((Dimethylamino)methyl)-2-furanyl)methyl)thio)ethyl)-N'-methyl-2-nitro-1,1-ethenediamine) | 9.00x10-2 |
|
| Sertraline ((1S,4S)-4-(3,4-dichlorophenyl)-N-methyl-1,2,3,4-tetrahydronaphthalen-1-amine) | 1.20x100 | Gibbs & Jones 2017 |
| Norsertraline ((1s,4s)-4-(3,4-dichlorophenyl)-1,2,3,4-tetrahydronaphthalen-1-amine) | 7.60x10-1 | Gibbs & Jones 2017 |
| Tamoxifen (2-[4-[(Z)-1,2-diphenylbut-1-enyl]phenoxy]-N,N-dimethylethanamine) | 5.36x10-2 | Gibbs & Jones 2017 |
| Dipyridamole (2-[[2-[bis(2-hydroxyethyl)amino]-4,8-di(piperidin-1-yl)pyrimido[5,4-d]pyrimidin-6-yl]-(2-hydroxyethyl)amino]ethanol) | 2.48x10-1 | Okuda et al 2009
|
| Fexofenadine (2-[4-[1-hydroxy-4-[4-[hydroxy(diphenyl)methyl]piperidin-1-yl]butyl]phenyl]-2-methylpropanoic acid) | 1.70x10-4 | Golovko et al 2014 |
| Gabapentin (1-(Aminomethyl)cyclohexaneacetic acid) | 1.00x10-3 | Writer et al 2013 |
| Levetiracetam ((2S)-2-(2-oxopyrrolidin-1-yl)butanamide) | 1.25x10-2 | Gurke et al 2015 |
| Sotalol (N-[4-[1-hydroxy-2-(propan-2-ylamino)ethyl]phenyl]methanesulfonamide;hydrochloride) | 5.09x10-4 | Radjenović et al 2009 |
| Benzothiazole (1,3-benzothiazole) | 6.44x101 | Harrison et al 2006 |
Combining partition coefficients (Table 3‑9) with initial concentrations in sewage sludge (Table 3‑10) within Equations 2‑6 - 2‑9, it was possible to estimate the concentrations of each PPCP that would remain in soil vs. migrate to soil pore water or soil pore air (Figure 3‑12). Those contaminants with the greatest propensity to partition into the soil pore water are subsequently more likely to be taken up by food crops or pasture, and therefore enter the human food chain.
![This figure indicates the partitioning [ppm] of pharmaceutical and personal care products (PPCPs) between soil amended with sewage sludge, soil pore water, and soil air spaces given initial starting concentrations in sewage sludge (Table 3 10).](/binaries/content/gallery/publications/research-analysis/2021/10/human-health-risk-assessment-potentially-hazardous-agents-land-applied-sewage-sludge/SCT10215481602_g17.png)
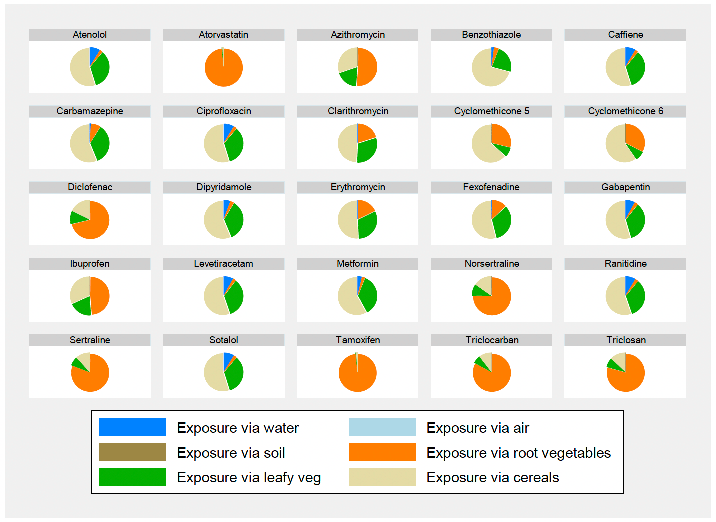
Concentrations of each PCPP in root crops, leafy vegetables, cereal crops, groundwater (private drinking supplies) and volatilisation to air were estimated using Equations 2‑10, 2‑11 & 2‑12. These were related to human exposure by assuming that a proportion of produce consumed was from the locations where sewage sludge was applied, a proportion of the air breathed in was derived from air into which contaminants had volatilised into, and a proportion of the water consumed was derived from a supply into which contaminants had leached. The assumptions made were the same as those made in the risk assessment of organic contaminants are detailed in Table 3‑7. Estimates of exposure for each individual PPCP were then calculated (Figure 3‑13).
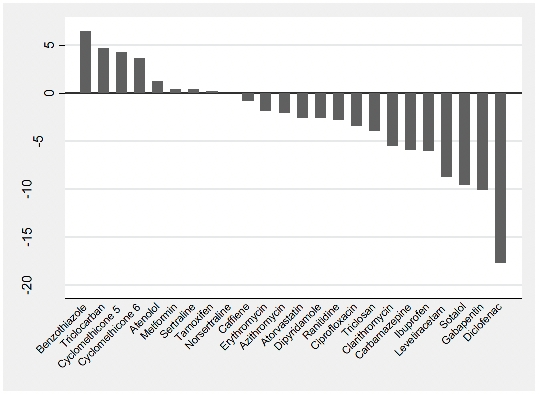
Estimates of exposure (Figure 3‑13) were compared to the reference doses (RfDs, Table 3‑9) in order to derive the Hazard Quotient, HQ as defined in Equation 2‑15 (Figure 3‑14).
Conclusions
Even with 'realistic worst case' assumptions, the majority of the phamaceuticals and personal care products investigated posed no appreciable risk to local inhabitants.
The following PPCPs returned a hazard quotient that was significantly greater than one; benzothiazole, triclocarban, cyclomethicone 5 & 6 and atenolol (Figure 3‑14); suggesting that for the worst case exposure scenarios described above, individuals would experience deleterious health effects due to lifetime exposure to these compounds as a result of sewage sludge application to land. It is interesting to note that for all these compounds, the exposure is dominated by food consumption with consumption of cereals driving the risk from benzothiazole, atenolol and the cyclomethicones (although in all these cases, consumption of leafy vegetables is also important), while root vegetable consumption drives the risk from triclocarban (Figure 3‑13). Therefore these exposures (if found to be real) could be mitigated by restricting the use of sewage sludge to crops for animal feed, e.g. grass and other forage crops. There are also a number of opportunities within the treatment processes to mitigate against these chemicals, with partial reductions readily achieved using anaerobic digestion and thermal hydrolysis (see Table 4‑1)
It should be noted that the RfD for atenolol has especially large uncertainties as it is derived from a point of departure from ecotoxicologic data where fish have been exposed to atenolol in their water environment. This exposure scenario clearly does not represent very well the human exposure pathways of interest here, as well as the uncertainties around the appropriateness of using fish as a proxy for human beings. The RfDs for benzothiazole, triclocarban and the cyclomethicones were all values that are currently used in regulatory situations.
The analysis also suggests that metformin, sertraline and tamoxifen might also pose a risk, however given the 'realistic worst case' assumptions it is likely that this risk is minimal. The main exposure route for sertraline and tamoxifen is via consumption of root vegetables, while consumption of cereals drives the risk from metformin (Figure 3‑13). Therefore, again the restriction of sewage sludge application to forage crops would minimise this risk if necessary.
These estimates of HQ are based on realistic worst case assumptions, thus the exposure scenarios will only apply to a very small proportion of the population (if at all). The majority of individuals living close to sewage sludge application activities are not going to be exposed via drinking water, and it is unlikely that they will be consuming 10% of their food intake from locally-grown produce.
The use of 'realistic worst case' scenarios is a conservative approach aimed at protecting the most vulnerable in society and hence the approach tends to drive up risk estimates. This is helpful as it gives a level of confidence where we identify compounds that despite the worst case assumptions pose little risk to inhabitants. The recommendations made here have been made on the assumption that the potential exposures highlighted are found to be real and reasonably widespread.
Contact
Email: gary.gray@gov.scot