Distress Brief Intervention pilot programme: evaluation
This report presents a realist evaluation of the Distress Brief Intervention (DBI) programme. DBI has been successful in offering support to those in distress, and has contributed to peoples’ ability to manage and reduce their distress in the short term, and for some in the longer term.
7 Impact of DBI on Individuals Experiencing Distress
7.1 Impact of DBI Level 1 on individuals
Findings on the impact of the DBI Level 1 on individuals, including perceptions of a compassionate response, impact on their ability to cope, their distress levels and the factors that could be identified as influencing these are presented below.
7.1.1 Perceptions and impact of the compassionate response
Overall, individuals felt that they were treated with compassion by DBI Level 1 practitioners. Those who completed the first session evaluation survey at the start of their Level 2 intervention were asked to select the number (from 0: 'not at all to 10: 'completely') that best described how much they felt that the Level 1 provider who referred them to the DBI Level 2 service treated them with compassion. Most indicated they felt treated with a fairly high level of compassion (a mean of 8.6). Younger adults tended to provide slightly lower ratings, although still high (a mean of 8.2 for those aged 16-24 and 8.3 for those aged 25-34, compared with 8.7 to 9.1 for older age groups) (Appendix 3, Table A7.1).
Those who showed the lowest levels of psychological distress at the start of Level 2 (that is, those with a low score on the CORE-OM 5) were more likely to rate the compassion of the Level 1 provider very highly. Those with a CORE-OM 5 score of 0-10 at the start of Level 2 (indicating low levels of distress) gave a very high mean rating of 9.9 but this fell to 8.4 for those with a CORE-OM 5 score of 32-40 (indicating severe levels of distress).
Mean ratings of being treated with compassion at Level 1 were highest for those who presented to the police (9.3) and lowest for those who presented at an A&E department (7.7). Those presenting to A&E did not present with higher levels of distress than those presenting to the other Level 1 providers (see Appendix 3, Table A7.2) and the reduction in distress levels between contact with the Level 1 referrer and the Level 2 DBI service was lowest for those coming through A&E or the psychiatric liaison service (Appendix 3, Table A7.3). This may explain the relatively lower compassion scores for Level 1 in Lanarkshire (8.2) compared with other pilot areas. In Lanarkshire higher proportions of evaluation respondents (more than 50%) presented at an A&E department than in other pilot sites (between 0% and 2%).
Some individuals interviewed noted that the compassionate response they received from frontline practitioners in services participating in DBI differed from their previous experiences of those services.
"Usually they just get you in the ambulance and don't bother but they really were awful nice." Individual
On occasion, a referral to DBI was enough to alleviate their distress without further support from clinical or other services. For some of those interviewed, DBI served a highly useful purpose in providing an alternative or complement to medication or being placed on waiting lists for clinical intervention as a response to their distress.
"I was too accustomed in the past to seeing GPs about mental health problems and then just being given drugs and told to go away basically. So, I was actually pleasantly surprised…very pleasantly surprised that it wasn't just a case of, okay, here's some medication. For once there was, you know, something else that was actually…some other form of help that was actually being offered to me straightaway for free." Individual
Level 2 practitioners commented that DBI Level 1 formed the base for individuals' further engagement with services, attributing this effect to Level 1 practitioners having broken down barriers to seeking/accepting help and perhaps reducing the self-stigma associated with distress by offering a compassionate response. DBI Level 1 practitioners felt that their provision of a compassionate response validated the individuals' distress and this may have helped the individuals not to become more distressed.
"I don't know if it's the level one response has already opened the kind of floodgates because quite often, I'll walk into the room and say 'right, so tell me a wee bit about what's happening?' and they just breakdown ... I was quite astounded by it… so I think there's a connection there that they've already started to break down the barriers…" Level 2 practitioner
7.1.2 Impact of Level 1 on individual distress levels
Those who completed the first session evaluation survey were also asked to rate (from 0: 'not at all to 10: 'completely') how much they thought that the Level 1 provider helped them to cope with the immediate distress they were feeling. Most indicated a fairly positive score (a mean of 7.8), although there were a range of scores, with one-in-five respondents (19%) providing a score of five or less (Appendix 3, Table A7.4).
The mean 'helped to cope' score was lower for younger adults (7.2 for those aged 16-24 and 7.6 for those aged 25-34, compared with 8.0 to 8.4 for older age groups). It was lowest for women aged 16-24 (6.9), although the difference between men and women of this age was not significant.
Mean 'helped to cope' scores were highest for those presenting to the police (8.6) and lowest for those presenting at an A&E department (7.1), the same pattern noted above for ratings of the compassion of Level 1 providers. This was also reflected in the lower scores in Lanarkshire, where respondents were much more likely to have presented at A&E.
There were similar results for the two measures, CORE-OM 5 and the Distress Thermometer (Appendix B) when they were used at the same time points. However, because they measure slightly different things and they were administered differently (the CORE-OM 5 was completed by individuals themselves in the surveys and the Distress Thermometer was completed with or by the DBI staff member), there were some differences in results. For example, a few individuals scored high distress on one of the measures and lower distress on the other.
The CORE-OM 5 scores suggest that the support Level 1 practitioners give is important in helping individuals to cope with their immediate distress, and the more they can do this, the less distressed individuals will be when they arrive at Level 2. Those in less distress at the start of their Level 2 intervention were more likely to rate the Level 1 provider highly in terms of helping them to cope (9.2 for a CORE-OM 5 score of 0-10, falling to 7.5 for those with a CORE-OM 5 score of 32-40).
Eight out of ten (80%) Level 1 practitioner survey respondents agreed that as a result of the Level 1 training they believed they were contributing to better outcomes for the individuals who present to them in distress (see Appendix 4, Figure D). Level 1 provider interviewees felt that they could now give individuals a tangible offer of help which could prevent them from going on to express their distress in more harmful ways.
"People have expectations when they come to see you. And nine times out of ten, it would be admission to hospital, because they have a problem. And then, when you turn around and say, well in actual fact, your problem is a social one, you need to deal with it, they feel kind of, oh, I'm not getting admitted then, and you're giving me a blooming phone number, what good is that you know. But if you can say, right, you've got this problem, somebody can sit down and work it out with you, there you go, there's a referral, and they're a lot happier. Whereas before, they would have just said, well I'll show you the problem I've got, and I'll go and take a few paracetamols, and it would escalate." Level 1 practitioner, Mental Health Crisis Service
Respondents to the first session evaluation survey were asked whether they were left with a clear understanding from the person who had provided the Level 1 intervention of what would happen over the next 24 hours. Five in six (83%) said that they were left with a clear understanding of what would happen, with no clear differences between subgroups (Appendix 3, Table A7.5).
Level 1 service interviewees reported that individuals seemed to respond well to being offered such a prompt source of support. Some individual interviewees who took up the referral to Level 2 services suggested they were not entirely clear as to what support would be given and suggested this may need to be explained more consistently in the future.
Some practitioner interviewees from the police felt that DBI may be less beneficial for individuals with more enduring problems who made repeated contact with them and more beneficial for those presenting to them for the first time.
"It seems to work best for people who are only in contact with the police maybe once or in a short period of time and the repeat callers that I've offered it to and even if they've accepted, it's not really seemed to make that much difference cause they just keep phoning the police or whoever they're phoning is then contacting the police again, but there are obviously people who are just having an incidence of distress and it's got to the point where they've come in contact with the police and they seem to get a bit more benefit of it, or certainly we don't really hear from them again so we hope that they get benefit from it." Level 1 practitioner, Police Scotland
7.2 Impact of DBI Level 2 on individuals
Findings on the impact of DBI Level 2 on a range of individual outcomes including distress levels, ability to self-manage, self-stigma and help-seeking and general wellbeing, and the factors that could be identified as influencing these are presented below.
7.2.1 Impact of Level 2 on individual distress levels
Across both distress measures, for most individuals, distress decreased during the course of the entire DBI intervention (from Level 1 to end of Level 2). This suggests that DBI is working well for most individuals, including those presenting with lower and higher levels of distress but around one in ten had increased distress levels by the end of Level 2.
As measured by the Distress Thermometer, distress decreased during the course of the entire DBI intervention (from Level 1 to end of Level 2) for most individuals (93%), with just 7% showing an increase in distress. On presentation at Level 1, the majority of individuals (82%) reported being in high distress (a score of 7-10), with a mean score of 7.8. At the start of Level 2, generally within 24 hours of referral, this proportion had fallen to 53%, and the mean score was 6.5. By the end of Level 2, the proportion in high distress had fallen further to 15%, and the mean score was 3.9. While there may be a certain degree of regression to the mean within these figures – with random variation, a high distress score is more likely to fall further towards the average score than a lower distress score – these figures go well beyond what would be expected, showing a continued decrease over the period of the intervention (Appendix 3, Tables A7.2, A7.6, A7.7 and A7.8).
The CORE-OM 5 provided similar findings. It measured a decrease from 29% in high distress (a score of 32 to 40), and a mean score of 25.9 at the start of the Level 2 intervention to 7% in high distress and a mean of 16.8 at the end of the Level 2 intervention. Of those who showed a decrease in distress on the CORE-OM 5, 64% had a decrease in their score of 5 or greater (indicating the reliable change that exceeds what might be expected by chance alone or measurement error) and 20% saw a decrease in their score taking them to a CORE-OM 5 score of less than 10 indicating a distress level lower than that of a typical 'clinical' population after therapy (Appendix 3, Tables A7.9, A7.10 and A7.11).
Of those completing the first and final Level 2 session evaluation forms, however, 11% of respondents showed an increase in psychological distress, highlighting that the intervention had not been successful for everyone in terms of reducing distress. There were no clear patterns in the characteristics or nature of the intervention received to distinguish this group and so the reasons for worsening distress remain unclear. In Section 7.2.2 below we discuss factors that were found to have influenced changes in individual distress levels.
7.2.2 Factors influencing change in individual distress levels
This section sets out the factors that our analysis suggests are associated with changes in distress levels of individuals between the start and end of their DBI intervention. Factors considered include individual characteristics, presenting problem and level of distress, provider and individual perceptions of how they were treated and the impact of the intervention on how they perceived their distress.
Neither the length nor the intensity of the intervention was associated with changes in the level of distress as measured by either the distress thermometer or CORE-OM. Also, individuals who felt they had improved during the course of the intervention were more likely to say that two weeks was about the right duration for the intervention.
We conducted a regression analysis to determine the factors independently associated with distress levels, when controlling other factors, or more simply, those most strongly associated with levels of distress at the end of the level two intervention. In this analysis, while the length of the Level 2 intervention seems to be linked to the distress level at the end of Level 2 (Appendix 3, Table A7.12) this is off-set in the statistical model by the fact that LAMH had the second highest proportion of Level 2 interventions of over 14 days and the highest proportion of interventions of a total of more than seven hours of support. Interpretation of this type of analysis is more complicated when the factors entered into the model are not independent of each other. This is exemplified by the length of the intervention and the level two provider. While the model appears to show that length of intervention is significantly associated with distress levels, this needs to be considered along with the reverse finding for those for whom DBI was provided by LAMH. Taken together, there is no real association between length of intervention and level of distress, nor between the provision of DBI by LAMH and level of distress.
Figures 7a and 7b below illustrate that the decrease in distress scores are universal across all providers using both measures, although there is some variation in the size of the decrease.
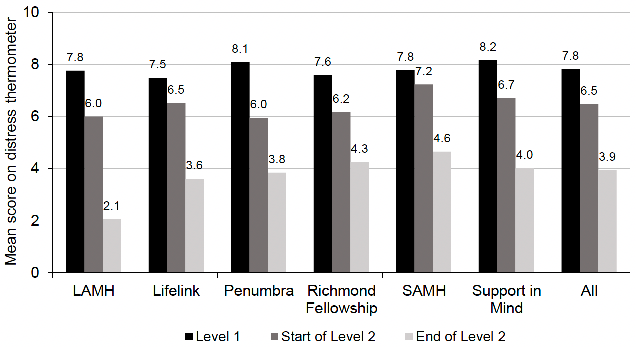
Sources: DBI routine data for Level 1, individual evaluation participant surveys for start and end of Level 2.
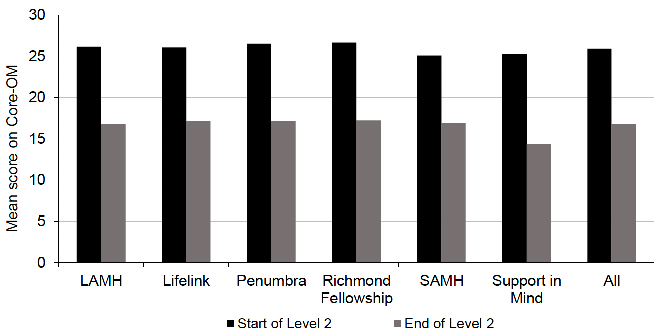
Sources: Individual evaluation participant surveys for start and end of Level 2.
Those who completed the final session evaluation survey at the end of their Level 2 intervention were asked to select the number (from 0: 'not at all' to 10: 'completely') that best described how much they felt that the Level 2 provider treated them with compassion. Most indicated they felt treated with a very high level of compassion (a mean of 9.7) (Appendix 3, Table A7.13).
Although the level of change in distress within individuals was not associated with age, gender, area deprivation or the main presenting problem, differences were seen in how individuals rated Level 2 practitioners in terms of compassion and on the Consultation and Relational Empathy (CARE) Measure (Mercer et al. 2004). Those who rated the Level 2 providers more highly tended to achieve greater decreases in their distress on both the distress thermometer and the CORE-OM 5 scales. This does not necessarily indicate that more compassionate providers achieved better results, as the direction of causality between change in distress and the individual's rating of their practitioner is not clear (Appendix 3, Tables A7.8 to A7.11). It is important to note here that compassion ratings were fairly high overall and most of the individuals who experienced worsening distress over the course of the intervention felt that they had been treated with a fairly high level of compassion.
Individuals' level of distress at the start of Level 2 was associated with their level of distress at the end of Level 2 (on both the Distress Thermometer and CORE-OM 5), but distress at Level 1 was not significantly associated with the final outcome. This demonstrates that if an individual was still in high distress at the start of Level 2, they were more likely to have high distress at the end of Level 2. This emphasises the importance of the Level 1 practitioners helping the individual cope with their distress at the referral point. Varying levels of distress at the start of Level 2 could also be related to the underlying cause of an individual's distress, which could influence the extent to which their distress would be likely to decrease by the commencement of Level 2 (Appendix 3, Tables A7.12, A7.14 and A7.15).
When controlling for distress levels at the start of Level 2, women were likely to have a higher distress level at the end of Level 2 than men (+0.5 on the Distress Thermometer). This suggests that for some reason DBI Level 2 may be working less well for women than for men; it is not clear why, but the difference is significant and merits further consideration (Appendix 3, Table A7.14).
Also, when controlling for distress levels at the start of Level 2, younger adults, particularly those aged under 35, were likely to have lower distress by the end of Level 2 than older adults (by 2.5 - 3 points on the CORE-OM 5), suggesting that DBI Level 2 is may be working better for younger adults at least in the short term, and merits further investigation (Appendix 3, Table A7.12). This is despite the finding that the mean 'helped to cope' score was lower for younger adults (see 6.1.2 above) at Level 1. It is not clear what this means. It could be that i) Level 2 practitioners are better prepared or trained to work with young adults or; ii) that the Level 1 setting is less conducive to supporting young adults to cope or, iii) that younger adults have less well-developed coping skills than older adults. This merits further exploration.
There is clear evidence that when DBI practitioners helped individuals to improve their understanding of why they feel distressed, this had an important influence on reducing distress levels. Individuals who agreed that DBI had improved their understanding of why they feel distressed were likely to have a lower distress rating at the end of Level 2 (by 1 point on the Distress Thermometer and by 5 points on the CORE-OM 5) (Appendix 3, Tables A7.12 and A7.14).
The above findings on practitioner care are also reflected in the responses of some individual interviewees whose distress was reduced at the end of Level 2. According to them, the combination of practical support to address issues that were causing their distress, and emotional support to validate their feelings and expression of distress, were central to reducing their distress.
"Everything that happened to me was all positive. There was nothing I came away with and said 'd'you know what, that was an absolute waste of time', cause I went into the whole thing going, you know, pretty much I can't be bothered with anything, I just don't want to deal with anything, you know, and it was affecting everything, no presence about myself, I didn't have any fun, … so for that kick start that it took me to actually turn round and say this is what I need or think that I need and go through with things, you know, so everything that happened to me from that point of going to the doctor, receiving the first phone call, receiving the visits, the action plan, you know, everything was all positive for me." Individual
"I just wanted to feel like, like you're worth something, like, life is worth living. And that you had, that you have meaning, and that it's okay to feel the way that you feel. I think, especially as a man, there's a lot of stigmatising in media, and in just the way our society is run, that men are just supposed to feel like, you're supposed to just man up and get on with it. But I feel like that's a very wrong approach to be taking, and that's probably why men, sadly in this country, have such a high rate of suicide. I think we need more services like this that tell you that it's okay to feel how you feel." Individual
Others recognised the benefit of immediate support.
"I think it made a difference to me in the short term because I was very, very ill and it was really…it was…even though maybe the meetings didn't go exactly how I expected them to go, it was still reassuring to me in the state that I was in, which was a very anxious state. And it was just, like, the state of abject terror, that I…you know, somebody was texting me and saying, okay, you're coming to meet me on whatever day, and that was something to hold on to." Individual
7.2.3 Inappropriate referral and individual outcomes
For those with more severe and enduring mental health problems, such as recurring depression or Post-Traumatic Stress Disorder, DBI may be less appropriate, although, for some of those interviewees, their distress levels were still reduced. Some individual interviewees with such problems suggested that they were 'bombarded' with information by DBI Level 2 at a point where they were too vulnerable to take much in. Those individuals recognised that there were limits to the support that could be offered by DBI within the guideline 14 days and expressed a preference for counselling or more clinical support.
"A problem I did have with it was that I was almost bombarded with information and I know that it's better than no information but I…my criticism of the experience would be that the particular individual I saw didn't take in to account that I was in a very vulnerable state and…in terms of my anxiety level was through the roof, you know, it was really high. And I couldn't process all the information that was thrown at me. I just couldn't. I was too anxious." Individual
Some referred to an awareness that DBI could not provide a 'miracle' but expressed some disappointment that it hadn't lived up to expectation, nonetheless.
"The only complaint I would've had, I kinda thought that I was… it's not even a complaint, but I kinda thought it'd be more like a therapist type thing, but I kinda realised fairly quickly that it wasn't really like that." Individual
Some Level 2 practitioners echoed this concern. Although nearly four in five (77%) Level 2 practitioners who completed the practitioners' survey agreed that they were contributing to better outcomes for individuals as a result of their DBI training, around one in seven (15%) disagreed, one of them commenting:
"I feel we are still receiving referrals which are not for people in distress but rather due to drug and alcohol misuse, and ongoing mental health issues. I also think a lot of the people being referred on are being misled about what support they will receive at DBI Level 2, e.g. counselling, medical interventions." Level 2 practitioner
These findings merit further exploration and may highlight a tension between the option of providing a referral to DBI on the one hand where a quick response is guaranteed, and in referring to more appropriate supports such as counselling or other talking therapies who are not able to respond quickly due to widespread long waiting times. However, the finding may highlight a weakness in the Level 1 referral assessment practices leading to inappropriate referrals. Section 5 highlighted that additional training updates would improve clarity on the appropriate distress level for DBI referrals to help reduce the number of inappropriate referrals to DBI.
Not being able to see the same DBI practitioner consistently or as much as expected in cases where holidays or sick leave impacted on the contact had a negative impact on satisfaction with the Level 2 service. In some cases, individuals had missed early contacts or confused timings and felt no allowance was made for this.
"She obviously knew my story, like, the woman that was dealing with me was talking about me, but I felt like she didn't know my story if that makes sense, she wasn't there the whole time, like, she just came in and was, I don't know, giving me things that I thought 'that's not what I talked about, that's not what happened'. I would've preferred it if I waited." Individual
7.2.4 Impact of Level 2 on self-management, help-seeking and self-stigma
Individuals completing the final Level 2 session evaluation survey (n=499) tended to report very positive impacts of the Level 2 intervention on their ability to self-manage their distress:
- 90% agreed that DBI had given them the tools and skills to manage their distress.
- 97% agreed that DBI has helped them to find out where they can access support if they feel distressed.
- 86% agreed that DBI has improved their understanding of why they feel distressed.
- 87% agreed DBI has helped them to recognise when they start to become distressed.
- 94% agreed DBI has helped them make plans to improve the situations in their lives which are causing distress.
Subgroup analysis showed the same pattern for all five questions, with no significant differences by age, gender, SIMD, main presenting problem or pilot site. Large differences were noted in response to all the above questions when broken down by the rating of the Level 2 practitioner in terms of compassion and an individual's scores on the adapted Consultation and Relational Empathy (CARE) Measure (Mercer et al. 2004). Individuals rating compassion and practitioner care more highly were more likely to agree with the above statements. The differences were more pronounced for DBI improving understanding of why they feel distressed and for DBI helping them to recognise when they start to become distressed. This reinforces what was discussed above in terms of the importance of individuals' perceptions of practitioner care and compassion and the changes in their level of distress. The findings suggest that the more the practitioner shows compassion, interest, understanding, makes the person feel at ease, is positive, clear and enabling, the better the outcome for the individual (Appendix 3, Table A7.16)
Many individual interviewees reported that they found that DBI enhanced their ability to cope with their distress and many found that it developed their confidence to connect or reconnect with services they were signposted to. This seemed to be partially due to being listened to in a non-judgemental and relaxed environment, where Level 2 practitioners had not judged individuals' previous failures to maintain contact with community services. Interviewees reported that this led to reducing self-stigma around seeking support and for some individuals, those services went on to provide sustained support which helped reduce future episodes of distress.
7.2.5 Perceived outcomes if DBI had not been offered
In their Level 2 final session, survey respondents were asked an open question "If DBI had not been offered to you, what would you have done instead?" One in ten (10%) revealed that they may have attempted suicide or continued with their suicidal thoughts. This represents a considerable number of people whose lives, in the short term at least, could have been very different in the absence of DBI.
One in seven (14%) answered that they would have returned to their GP or other frontline medical services, while a slightly smaller proportion (12%) said that they would have tried to access counselling or other formal support. Others thought that their distress would have become worse, that they would have self-harmed, or used potentially harmful coping strategies such as alcohol or isolating themselves, with many saying they did not know what they would have done (Appendix 3, Table A7.7).
7.2.6 Longer-term impact of DBI on individual outcomes
Respondents to the three-month follow-up survey (n=102) were asked an open question on what they had hoped to achieve from DBI when they were referred to it. The most common answers were that they had hoped to get skills and techniques to manage their distress (28%); they wanted to talk about their problems / be listened to without judgement (26%); they wanted to feel better / feel more positive / feel less distressed (16%); they wanted to get help (15%); and they wanted insight / greater understanding of their distress (11%) (Appendix 3, Table A7.18).
Half of the respondents (51%) felt that the intervention had helped them fully achieve their aims, with a further 40% saying that they had partially achieved their aims. Small base sizes in the follow-up survey make it difficult to drill down further into these findings (see Table A7.19).
Views on the longer-term impact of DBI were mixed among the individual interviewees. Some described how DBI had helped them to feel valued and rediscover a focus, with positive outcomes. The follow-up survey findings suggest that many of those going through DBI may have been using what they learned during the intervention to help them manage their distress, with four in five (79%) stating that they had used the plans or strategies from their D-MaP to manage their distress (Appendix 3, Table A7.20). This is a good outcome but it is possible that individuals with a more negative experience were less likely to return their follow-up questionnaire and that the survey findings were biased. Among interviewees, individuals described how even in difficult situations, coping techniques offered through DBI were recalled and used. Among interviewees, there was often little recall of completing the D-MaP without prompting by the interviewer, although this could have been to do with how the document was referred to.
For some, particularly where individuals had an existing mental health diagnosis, DBI may have had a less positive longer-term impact. Some individuals were left feeling quite low as they had appreciated the contact for the 14 days of DBI and then felt isolated while awaiting further support.
"They did listen and I was able to tell my story and at the end of the meeting, they said 'right, that's you finished with us now, go away and phone these numbers up' and of course I never phoned the numbers up, I just went back into my house and I had other people come round and I just sort of… I reclused for about four/five weeks inside my house, didn't eat or nothing and then, I can't even remember what happened then, oh someone from AA come round, one of my friends from AA come round and they brought me back out into the world again." Individual
"It might have not changed how I felt at that point in time, but it felt nice to say something about it to somebody rather than just not saying anything to anybody. So because I didn't have that anymore it resulted in me having more episodes because I legit had absolutely nobody cause I was waiting on referrals and stuff like that, and that didn't come until months, so by that time I was in hospital for about four, three times in that time gap that I had absolutely nobody to speak to." Individual
For many, however, referral to appropriate community support or service appears to have led to more positive longer-term outcomes with over half of the 3-month follow-up survey respondents reporting that they were referred to other services by their DBI provider and four out of five of those reporting they had taken up the service. Among the individual interviewees, there were examples of DBI successfully bringing individuals into contact with both statutory and non-statutory services and this had, on occasion, led to re-engagement with work or previous activities, in addition to offering a longer-term support mechanism.
"It gave me the stepping stone to go to [service X][11] and then from [service X], through another friend, to [service Y] and out of everything, I will have to say that, and I've said it to [name of leader] on a few occasions of which he's told me to shut up, you were embarrassing him, but if it wasn't for [3rd sector organisation], I don't think I'd be here today." Individual
"They gave me the number and that was one of the biggest things as well because I was sitting arguing with them that I didn't want to go to [3rd sector organisation], I didn't want to be that woman who's abused and I didn't want to tar my husband with that brush, I kinda argued that quite a lot and then I ended up just doing it and it was probably the best thing I did, to be honest." Individual
There was also evidence from interviewees of the effectiveness of being signposted to other services in helping to cope with further episodes of distress.
"I can manage better in myself than I, better by myself, than I could before. But I feel like I also know where to go if I feel like I do need support. Whereas, before, I wasn't very sure if you should, like, phone Samaritans, or if you should go and arrange counselling, and stuff. It feels like you know better what to do if you need that help" Individual
Overall, DBI has proved to be successful in offering support to those in distress, with most receiving a compassionate and practical response that has contributed to their ability to manage and reduce their distress in the short and longer-term. However, DBI has worked less well for some and referrals were not always appropriate. As indicated in Section 7.2.1 for individuals whose distress increased, we are not able to offer definitive conclusions as to what factors may be associated with this. It is clearly of some concern and should be addressed as a priority in future research.
Contact
Email: socialresearch@gov.scot