Distress Brief Intervention pilot programme: evaluation
This report presents a realist evaluation of the Distress Brief Intervention (DBI) programme. DBI has been successful in offering support to those in distress, and has contributed to peoples’ ability to manage and reduce their distress in the short term, and for some in the longer term.
4 Overview of DBI activity in the evaluation period
In this section, we provide an overview of DBI delivery during the evaluation data collection period, which ran from 1st January 2019 until 30th May 2020. We draw on routine DBI data as well as financial information provided by DBI Central.
DBI Central went through various stages of development from the beginning of the DBI programme until today. It started in a Development and Start-Up phase between 2016 and 2018 and then entered a Delivery and Growth stage between 2018 and 2021. Total spending per year at DBI Central has changed accordingly over the years rising from approximately £60,000 per year in 2016-2017 to over £300,000 per year in 2019.
In terms of personnel, DBI Central consisted of a programme manager, programme administrator, clinical leads, a communications officer and two data analysts from Public Health Scotland. For more details on when each role became active and respective grades see Appendix C.
4.1 Referral demographics
During the evaluation data collection period (1st January 2019 to 30th April 2020), 5316 referrals were made to DBI.
Almost half of all referrals came from Lanarkshire (48%), with 19% coming from Aberdeen City, 18% from Scottish Borders and 15% from Inverness City. This reflects the relative population sizes from each of these areas, with the combined populations of North and South Lanarkshire accounting for 63% of the entire population covered by the four pilot sites. However, Inverness City had the highest number of referrals relative to its population size (16.8 referrals per 1000 population), followed by Scottish Borders (8.3 referrals per 1000 population). Referral rates were lower in Aberdeen City (5.0 referrals per 1000 population) and Lanarkshire (4.1 referrals per 1000 population).[2]
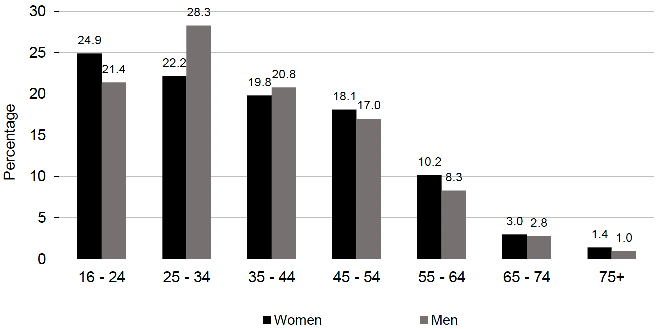
Women accounted for 58% of total referrals and men accounted for 42% of total referrals. Four of those referred were recorded as 'other' gender. These individuals are not included in further sub-analysis analyses due to their small number. Individuals referred were most commonly aged between 16[3] and 44 (68%). Among women, the highest proportion of referrals were from the 16-24 age group (25%) while, among men, the highest portion of referrals was from the 25-34 age group (28%) (Figure 4.1).
Almost 60% of individuals referred lived in the two most deprived quintiles, as measured by the Scottish Index of Multiple Deprivation (SIMD). Only half of the individuals referred to DBI gave their ethnicity. Of those, over 98% were white (including white Scottish, white other British, white Irish and white Polish). Further data is available in Appendix 3, Table 4.1.
1 Excluding individuals who selected "other gender" and age. These are not recorded as the numbers are too small (n=24).
4.2 Referral sources
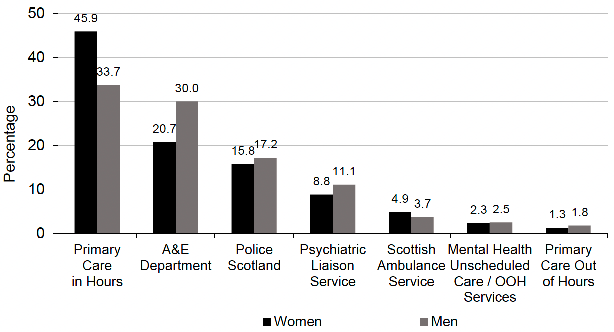
The greatest proportion of referrals to DBI came from Primary Care in Hours (41%) followed by the A&E department (25%), Police Scotland (16%) and psychiatric liaison service (10%). The smallest proportion of referrals came from Scottish Ambulance Service (4%), mental health unscheduled care and out of hours services (2%) and primary care out of hours (2%).
Men were more likely than women to be referred by A&E and women were more likely to be referred by Primary Care in Hours (Figure 4. 2). There was little difference in the age profile of those referred by different Level 1 referrers. Further data is available in Appendix 3, Tables A4.2 and A4.3.
1 Excluding Level 1 referrer not recorded (n=2). Social work referrals are not presented in the chart (n=9).
4.3 Presenting problems and contributory factors
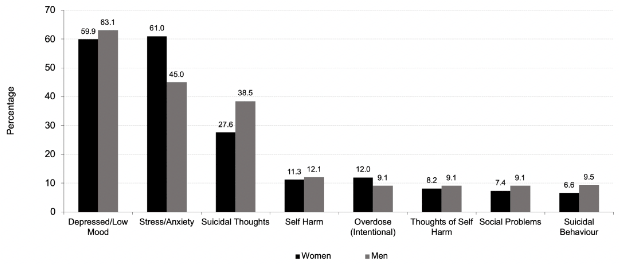
Individuals referred to DBI presented to Level 1 and Level 2 practitioners with a wide range of presenting problems (Figure 4.3) and factors which contributed to their distress. Multiple presenting problems and contributory factors could be identified and recorded for each individual. Feeling depressed/having low mood was the most commonly recorded presenting problem, recorded in 61% of all referrals (60% of women; 63% of men). Presenting problem differed by gender, with women more likely than men to present with stress/anxiety (61% of women; 45% of men), and men more likely than women to present with suicidal thoughts (28% of women; 39% of men) and suicidal behaviour (7% of women; 10% of men).
Relationship issues were the most commonly recorded contributory factor for both men and women, recorded in 48% of all referrals. Other common contributing factors included alcohol use (22%), life coping issues (21%) and money worries and unemployment (18% each). Alcohol use was recorded as a contributory factor in a higher proportion of men (29%) than women (16%). Substance misuse was also a contributory factor in a higher proportion of men (19%) than women (7%).
Alcohol use was most common among those referred by A&E (35%) and Scottish Ambulance Service (32%), less common among those referred by mental health unscheduled care/out of hours services (22%), primary care out of hours (16%). Recorded use of alcohol was lowest among those referred by primary care in hours (10%). Substance use was most common among those referred by A&E (23%) and Psychiatric Liaison Service (20%), less common among those referred by Police Scotland (9%) and Primary Care Out of ours (8%) Recorded substance use was again lowest among those referred by primary care in hours (5%).
Further data is available in Appendix 3, Tables A4.4, A4.5a, and A4.5b.
1 Presenting problems which were recorded in 5% or fewer of all referrals (Physical Health; Sleeping Issues; Panic Attacks; Crisis Call; Behaving Strangely) are not shown.
4.4 Contact within 24 hours
A key component of the DBI approach was that contact was made between DBI Level 2 and the individual within 24 hours of referral from Level 1. A contact attempt was made within 24 hours for all referrals made to DBI. Successful contact was made with individuals within 24 hours in 65% of cases. A further 21% were successfully contacted beyond 24 hours of their referral. The remaining 14% could not be contacted by DBI practitioners. In cases where no contact could be made, Level 2 practitioners sent a letter to the individual and their GP explaining that contact attempts had been unsuccessful.
There was no difference in successful contact within 24 hours by gender. However, older age groups were successfully contacted within 24 hours slightly more often than younger age groups.
Successful contact within 24 hours varied by pilot site. The proportion of referrals successfully contacted within 24 hours was highest in Inverness (72%) and Scottish Borders (70%), average in Aberdeen City (65%) and lowest in Lanarkshire (60%).
Further data are available in Appendix 3, Table A4.6.
4.5 DBI Level 2 outcomes and throughput
During the initial contact between a referred individual and a DBI practitioner, the individual was offered up to 14 days of compassionate, community-based, problem-solving support, with wellness and distress management planning. As shown in Figure 4.4 (overleaf), 3464 (66%) of those referred to DBI by Level 1 took up this support from DBI Level 2. A further 14% of referrals received one supportive phone call from a DBI practitioner but declined further support and 6% did not receive support from DBI due to escalating level of risk, inappropriate referral or ongoing inpatient care. The remaining 14% of all referrals could not be contacted by DBI practitioners.
Of those individuals who took up support from DBI, 84% were supported to a planned exit from the service, while the remaining 16% of those who took up support from DBI exited the service in an unplanned way (e.g. stopped attending appointments or responding to contact from DBI).
More women than men took up Level 2 support through to planned exit (women 59%; men 51%) and more men than women did not respond to contact attempts from DBI (women 12%; men 16%).
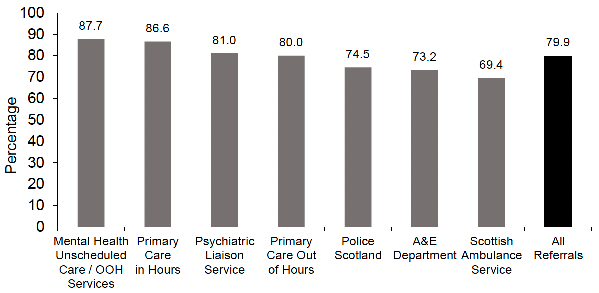
The proportion of referrals taking up any Level 2 support (that could range from one supportive phone call, to ongoing support over and above one supportive phone call, and Level 2 support with a planned exit) varied by pilot site. The highest proportion of referrals was taken up in the Scottish Borders (any support 86%; any Level 2 80%; support to planned exit 70%) and the lowest in Lanarkshire (any support 76%; any Level 2 62%; support to planned exit 49%).
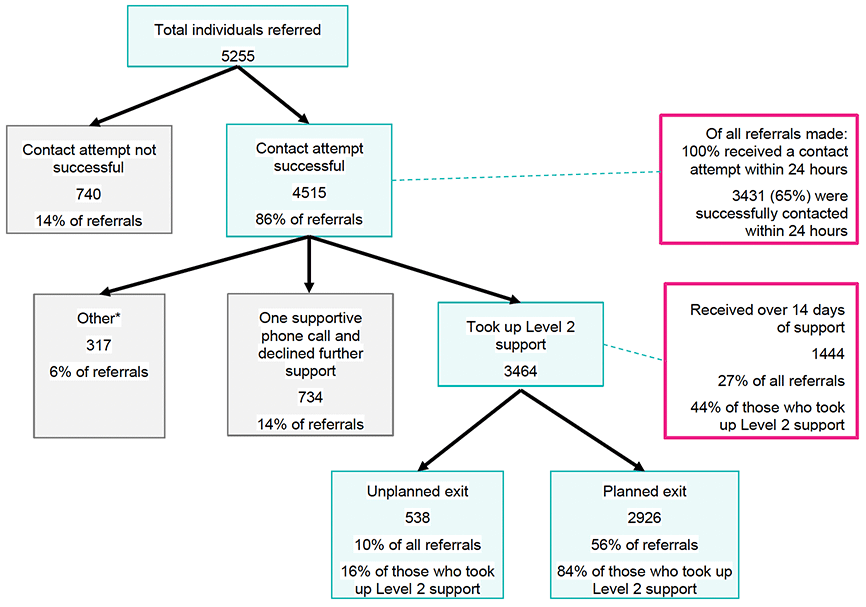
Source: Public Health Scotland. * Includes DBI stopped due to escalating level of risk, inappropriate referral or Level 2 cannot proceed due to ongoing inpatient care.
Those referred by Primary Care in hours and mental health unscheduled care/out of hours services were most likely to take up any support, while those referred by A&E, Police Scotland and Scottish Ambulance Service were less likely to engage.
Further data is available in Appendix 3, Tables A4.7 and A4.8.
1 Missing values (n=61, outcome not recorded).
4.5.1 Length and intensity of support
DBI level 2 offers individuals up to 14 days of support as a guideline. However, from the outset of the DBI programme, all Level 2 providers were enabled to provide support beyond the 14 days, dependent on individual need. During this time, individuals are offered a series of support sessions. A support session includes any contact with an individual accessing Level 2 where the individual received support (i.e. not administrative contact). This includes in-person sessions, phone calls and conversations by text message.
Of all referrals to Level 2 (n=5255): 27% received over 14 days of support, 38% received up to 14 days of support; 14% received one supportive phone call and did not take up further support from DBI, and 14% could not be contacted. The remaining 6% did not receive support from DBI due to escalating levels of risk, inappropriate referral or ongoing inpatient care (see Figure 4.4). So, of the 3464 individuals who took up more support than just one supportive call, 58% (2020) received 14 or fewer days of support. Of all individuals who took up support from DBI Level 2 to planned or unplanned closure, 42% received over 14 days of support.
There was variation by pilot site in the proportion of individuals who took up support from Level 2 and received over 14 days of support. The proportion was highest in Aberdeen City where 71% of individuals who took up Level 2 support received over 14 days of support. The proportion of individuals receiving over 14 days of support was lower in Lanarkshire (44%) and Inverness City (36%) but lowest in Scottish Borders at only 14%.
On average, individuals who took up support from DBI Level 2 received 4.1 support sessions. There was also variation across pilot sites in the average number of support sessions delivered per individual. Aberdeen City and Inverness City delivered, on average, the lowest number of support sessions (3.1 sessions and 3.2 sessions per individual, respectively). Lanarkshire delivered an average of 4.4 sessions per individual and Scottish Borders delivered the highest number of support sessions (6.8 sessions). Some of this variation may be accounted for by the different ways in which sites recorded the number of sessions. Some pilot sites may have recorded a brief phone call or text messaging exchange as a session while others may not.
Individuals who received up to 14 days of support received, on average, 3.1 sessions, while those who received more than 14 days of support received an average of just over 5 sessions. There was no difference in the average number of sessions received per person as the length of support increased. Those who received between 15 and 21 days of support received an average of 5.1 sessions, those who received between 22 and 28 days of support received an average of 5.1 sessions and those who received more than 29 days of support received an average of 5.2 sessions.
There was no clear difference in the number of support sessions by age or gender, although older adults (aged 45 and over) did seem to have more support sessions on average than younger adults (4.6 to 5.0 mean sessions compared with 4.2-4.3 mean sessions respectively).
Further data is available in Appendix 3, Tables A4.9 and A4.10.
Contact
Email: socialresearch@gov.scot