The Scottish Health Survey 2021 - volume 1: main report
Presents results for the Scottish Health Survey 2021, providing information on the health and factors relating to health of people living in Scotland.
Chapter 2 Mental Health and Wellbeing
Chapter Summary
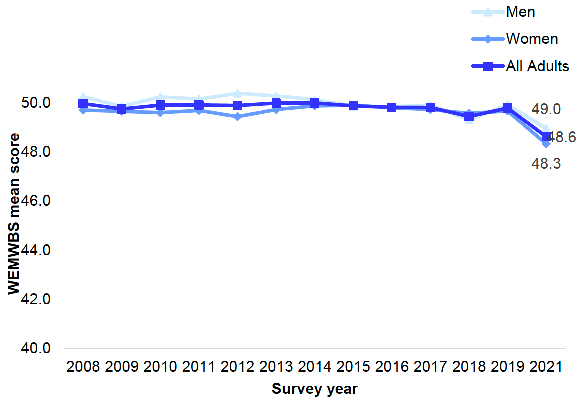
Average levels of mental wellbeing (measured by mean WEMWBS1 scores) were lower in 2021 than in 2019, following a decade in which levels had remained fairly constant.
- 49.8 in 2019
- 48.6 in 2021
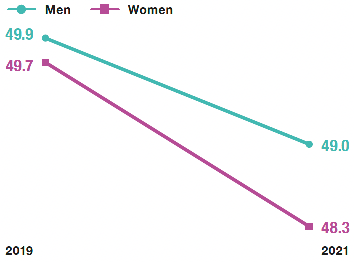
Women's average mental wellbeing scores fell by more than those for men.
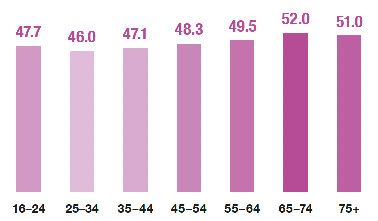
In 2021, adult mean WEMWBS scores varied by age; highest for those aged 65 and above, and lowest for those aged 25 to 34.
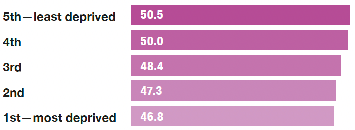
In 2021, adult mean WEMWBS scores were lower in the most deprived areas.
In 2017/2018/2019/2021 combined, boys aged 13-15 had higher mean WEMWBS scores than girls of the same age.
- 50.8 All children aged 13-15
- 51.9 Boys aged 13-15
- 49.6 Girls aged 13-15
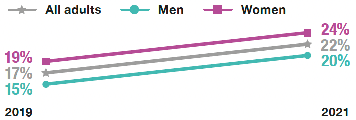
In 2021, 22% of adults had a GHQ-122 score of four or more (indicating a possible psychiatric disorder), an increase from 2019 for both men and women.
The proportion of adults with a GHQ-12 score of four or more tended to decrease with age.
1 WEMWBS scores range from 14 to 70. Higher scores indicate greater wellbeing.
2 GHQ-12 scores range from 0 to 12. Scores of 4 or more are indicative of a possible psychiatric disorder.
In 2021, prevalence of depression, anxiety and ever attempted suicide were at similar levels to 2018/2019 combined. Prevalence of ever having self-harmed increased over this period.
Depression, anxiety, ever attempted suicide and ever self-harmed were more common among younger than older age groups.
Depression, anxiety, ever attempted suicide and ever self-harmed were also more common in the most deprived areas.
In 2021, prevalence of anxiety was higher for women than for men.
- 10% men
- 18% women
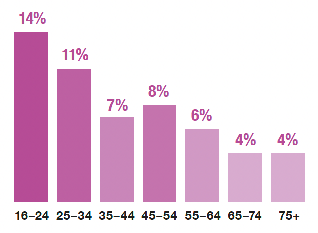
In 2021, 8% of adults reported feeling lonely 'most' or 'all of the time' in the last week. This was higher for younger people.
- 8% All adults
- 7% Men
- 8% Women
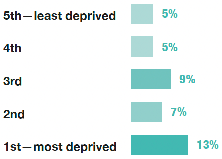
Prevalence of feeling lonely 'most' or 'almost all of the time' in the past week was highest in the most deprived areas in 2021.
Mental Health and Wellbeing
Erin Deakin
2.1 Introduction
Mental health is defined by the World Health Organization as a state of well-being in which every individual realises their own potential, can cope with the stresses of life, can work productively, and is able to make a contribution to their community.[1] Positive mental health encourages better quality of life overall, healthier lifestyles, better physical health, improved recovery from illness, better social relationships, and higher educational attainment.[2] Mental disorders often co-exist with physical illnesses[3] and those with severe mental disorders have a life expectancy 15-20 years shorter than the general population.[4]
Around one in four[5] people are estimated to be affected by mental health problems in Scotland in any one year.[6] It is also evidenced that mental ill health in adolescence increases the risk of subsequent mental ill health later in life.[7] Globally, around 5% of adults are estimated to experience depression and along with anxiety it is more prevalent among women than men.[8] Around 700,000 people die due to suicide every year globally[9] and rates remain consistently higher for men than for women.[10]
Poor mental health, including mental disorder, has a considerable impact on individuals, their families and the wider community[11] and is clearly associated with both poverty and social exclusion.[12] Loneliness is a significant public health problem[13] which can contribute to the onset and continuation of poor mental health.[14] Some population groups at increased risk include those with poor mental and/or physical health, those living in poverty, those with disabilities, those from LGBTI or minority ethnic communities and carers.[15] The risk of loneliness is also greater for those with mental health problems than for those with physical health problems and particularly high for those who experience anxiety, depression or stress.[16],[17]
2.1.1 Policy background
The impact of the COVID-19 pandemic has been felt widely at both societal and individual levels, impacting on mental health. In response to this, the Mental Health – Scotland's Transition and Recovery Plan[18] sets out the mental health needs resulting from the pandemic and lockdown and how the Scottish Government is addressing these.
The plan's commitments focus on areas or groups of people where COVID-19 is likely to have particularly impacted on mental health. Each area of focus includes responses that span multiple types of need including:
1. Promoting and supporting conditions for good mental health and wellbeing at a population level
2. Providing accessible signposting to help, advice and support
3. Providing rapid and easily accessible responses for those in distress, and
4. Ensuring safe, effective treatment and care for those living with a mental illness.[3]
The plan acknowledges a range of pandemic-related pressures that may have impacted on mental wellbeing. These include inequalities, employment, impacts on particular groups such as children, young people, families, older people, and those with long-term conditions or disabilities.[3]
Additionally, the plan lays out government action to provide the right help and support for mental illness. In particular, it illustrates the government's vision for the renewal of mental health services, including CAMHS and psychological therapies.[3]
The Scottish Government is due to publish a new Mental Health and Wellbeing Strategy in 2022 which will build on the Transition and Recovery Plan and set out priorities for the coming years.
2.1.2 Reporting on mental wellbeing in the Scottish Health Survey
This chapter updates trends in mental wellbeing for adults and children using the Warwick-Edinburgh Mental Wellbeing Scale (WEMWBS). Trends in mental health are also updated for adults including the General Health Questionnaire 12(GHQ-12) and CIS-R anxiety and depression scores, as well as data on attempted suicide, self-harm and loneliness. Figures are also reported by age, sex and area deprivation. To increase the sample size available, the analysis of child mental wellbeing used data from the 2017, 2018, 2019 and 2021 surveys combined.
The area deprivation data are presented in Scottish Index of Multiple Deprivation (SIMD) quintiles. To ensure that the comparisons presented are not confounded by the different age profiles of the quintiles, the data have been age-standardised. For a detailed description of both SIMD and age-standardisation as well as definitions of other terminology used in this chapter and for further details on the data collection methods for mental health and wellbeing and loneliness, please refer to Chapter 2, of the Scottish Health Survey 2021- volume 2: technical report.
Supplementary tables on mental wellbeing are also published on the Scottish Government website: Scottish Health Survey.
2.2. Mental Health and Wellbeing
2.2.1 Adult WEMWBS mean score, 2008 to 2021, by sex
In 2021, the mean WEMWBS score for adults was 48.6, the lowest recorded and outside of the range observed over the rest of the time series (49.4 – 50.0).
Throughout the survey years, mean WEMWBS scores have varied by sex with men generally recording higher mean scores, although the differences have not always been significant. There was no signification variation between the scores recorded in 2021 for men (49.0) compared with women (48.3). Figure 2A, Table 2.1
2.2.2 Adult WEMWBS mean score, 2021, by age and sex
As reported in previous survey years,[19] older adults generally reported higher mental wellbeing with a mean WEMWBS score of 52.0 recorded among those aged 65-74 and 51.0 among those aged 75 and over in 2021. In comparison, a mean score of 47.7 was recorded among those aged 16-24. In 2021, scores ranged between 46.0 - 49.5 for those aged 25-64, which is in line with previous years.
There were no significant variations by sex in 2021. Table 2.2
2.2.3 Adult WEMWBS mean score (age standardised), 2021, by area deprivation and sex
In 2021, area deprivation has continued to have a significant impact on the age-standardised adult WEMWBS mean scores. A decrease was recorded from a mean score of 50.5 in the least deprived areas to 46.8 in the most deprived.
No significant differences were recorded by SIMD between men and women in 2021.
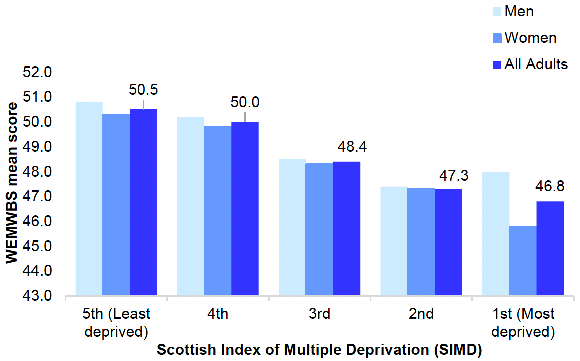
Figure 2B, Table 2.3
2.2.4 Child (aged 13-15) WEMWBS mean score, 2017/2018/2019/2021 combined, by sex
In 2017/2018/2019/2021 combined, the WEMWBS mean score for children aged 13-15 was similar to that recorded in previous years (50.8 compared to 51.0 in 2012-2015 combined).
As previously observed,[19] there were significant differences by sex in 2017/2018/2019/2021 combined. A mean WEMWBS score of 51.9 was recorded among boys aged 13-15, while the score among girls aged 13-15 was significantly lower at 49.6. The scores for boys and girls remain similar to those recorded in previous survey years. Table 2.4
2.2.5 Child WEMWBS mean score, 2017/2018/2019/2021 combined, by area deprivation and sex
In 2021, no clear pattern was evident for the mean WEMWBS scores for children aged 13-15 by deprivation. Those living in the least deprived areas recorded a mean score of 51.4 with a similar score recorded among those living in the most deprived areas (51.2). The mean WEMWBS score for those living in the other three quintiles ranged between 50.0 – 50.9. Table 2.5
2.2.6 GHQ-12 score, 2003 to 2021, by sex
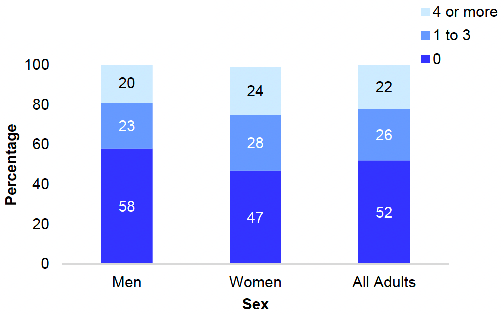
A GHQ-12 score of four or more is indicative of a possible psychiatric disorder. In 2021, the proportion of adults with a GHQ-12 score of 4 or more was 22%, a significant increase on the proportion recorded in 2019 (17%), as well as the scores recorded in previous years which ranged from 14%-19%.
In 2021, the proportion of adults with a GHQ-12 score of zero (52%) is the lowest in the time series (with a similar score of 53% recorded in 2018), while the proportion with a score of between one and three (26%) in 2021 remains in the range 21% - 28% recorded between 2003 and 2019.
Similar patterns were observed by sex. Table 2.6
2.2.7 GHQ-12 score, 2021, by age and sex
In 2021, a higher proportion of women recorded a GHQ-12 score of four or more compared to men (24% and 20% respectively), a pattern also recorded in previous survey years. Meanwhile, the reverse was recorded for the proportions recording a score of zero (47% of women compared with 58% of men). There was a difference of five percentage points when comparing scores between one and three by sex (28% for women and 23% for men).
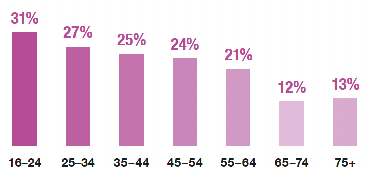
In 2021, a decrease with age was observed in the proportion of adults recording a GHQ-12 score of four or more. Younger adults had higher scores with 31% of those aged 16-24 scoring four or more compared to 12% of those aged 65-74 and 13% of those aged 75 and over. For those with a score of zero, the opposite was observed as the proportion increased from 40% among those aged 16-24 to 66% among those aged 65-74 and 62% among those aged 75 and over. Similar patterns were observed for both men and women.
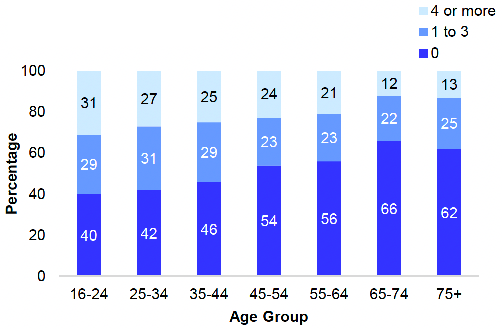
Figures 2C and 2D, Table 2.7
2.2.8 CIS-R anxiety and depression scores, attempted suicide and self-harm, 2008/2009 combined to 2021, by sex
To increase the sample size available, the analysis of anxiety and depression scores, attempted suicide and self-harm, by sex used sets of two-years of combined data from 2008/2009 to 2018/2019, while the data is presented for a single year for 2021 due to the lack of comparable data for 2020.
Depression
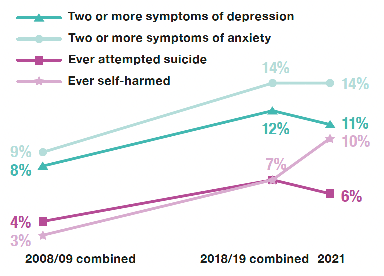
In 2021, the proportion of adults displaying two or more symptoms of depression (11%) remained in the range 10% - 12% recorded since 2014/2015 combined. No significant differences were found when comparing the proportion of men and women displaying two or more symptoms of depression (12% and 10% respectively).
The proportion of men that reported having two or more symptoms of depression increased overall from 7% in 2010/2011 combined to 12% in 2018/2019 combined and 2021. Scores for men in recent years are significantly higher than those in both 2010/2011 and 2012/2013 combined (7% and 9% respectively) indicating a real change regardless of the data collection mode (i.e. nurse interview or self-report).
The prevalence of two or more symptoms of depression has varied among women over the time series, with the highest level reported in 2016/2017 and 2018/2019 combined (both 11%). The proportion recorded in 2021 (10%) remains in the range 8% - 11% recorded since 2008/2009 combined.
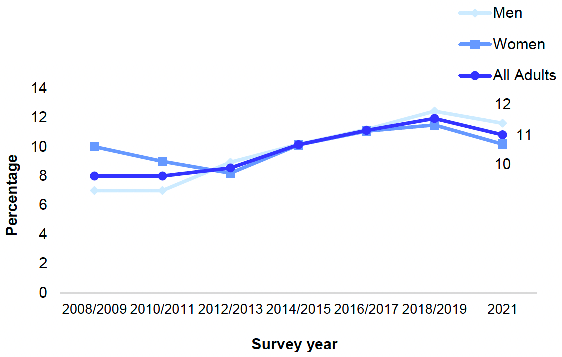
Figure 2E, Table 2.8
Anxiety
In 2021, the proportion of adults reporting having two or more anxiety symptoms was 14%, equal to that recorded for 2018/2019 combined and the highest proportion in the time series. By comparison, 9% recorded two or more symptoms of anxiety between 2008/2009 and 2012/2013 combined.
The prevalence of men reporting two or more symptoms of anxiety decreased to 10% in 2021 from 13% in 2018/2019 combined, returning to a similar level as recorded between 2008/2009 and 2016/2017 combined (in the range 7% - 9%).
There has been an overall increase over time in the prevalence of two or more symptoms of anxiety among women, which has risen from 10% - 11% in 2008/2009 and 2010/2011 combined to its highest score across the time series of 18% in 2021.
Over the time series (2008/2009 combined to 2021), women have been consistently more likely than men to record two or more symptoms of anxiety, although the difference has varied from 2 to 8 percentage points higher. The difference by sex in 2021 is the highest across the time series (eight percentage points).
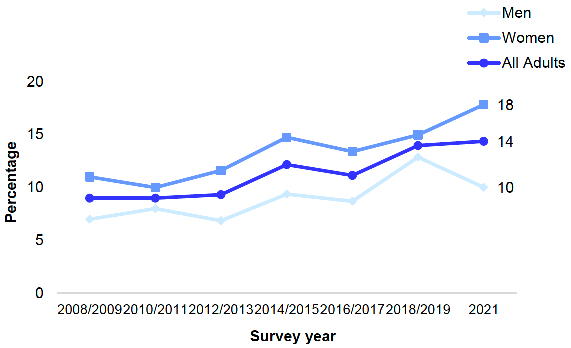
Figure 2F, Table 2.8
Attempted suicide
The proportion of adults reporting that they had ever attempted suicide was 6% in 2021. The 2019 SHeS report[19] highlighted potential evidence of an increasing trend in the attempted suicide rate, which had risen from 4% in 2008/2009 to 7% in 2018/2019 combined. However, further data is required to evaluate whether the slight decrease recorded in 2021 is evidence of a change in this potential trend or not.
The prevalence of ever attempting suicide has consistently been higher for women compared with men over the time series (two to three percentage points difference), with a non-significant difference in 2018/2019 combined. In 2021, the gap between men and women reduced to one percentage point, meaning that the difference in prevalence was not significant (6% for men and 7% for women).
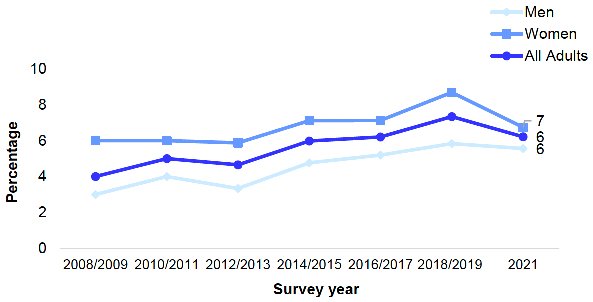
Figure 2G, Table 2.8
Self-harm
In 2021, one in ten adults reported ever having self-harmed (10%), the highest proportion recorded in the time series, with an overall increase from 2% - 3% in 2008/2009 combined and 2010/2011 combined. It should be noted that in 2012/2013 combined the mode of data collection changed from nurse administered to self-completion questionnaire.
In 2021, the prevalence of self-harm for both men and women was the highest in the time series at 8% and 11% respectively. Although women have consistently been more likely than men to report ever having self-harmed over the time series, the difference recorded in 2021 was not statistically significant.
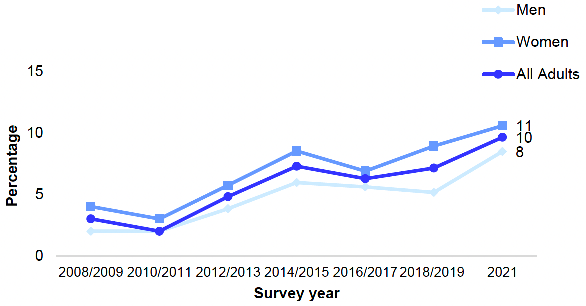
Figure 2H, Table 2.8
2.2.9 CIS-R anxiety and depression scores, attempted suicide and self-harm, 2021, by age and sex
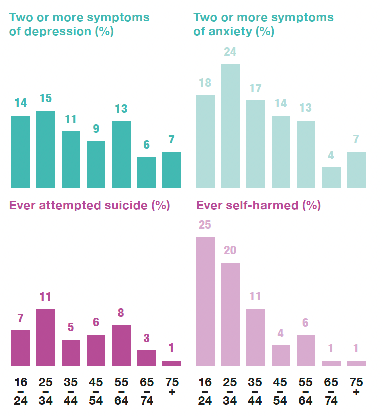
In 2021, a general decrease in prevalence of two or more symptoms of depression was recorded with age, with the highest proportion recorded among those aged 25-34 (15%) and the lowest among those aged 65-74 (6%).
In 2021, a general decrease in prevalence of two or more symptoms of anxiety was recorded with age, with the highest proportion recorded among those aged 25-34 (24%) and the lowest among those aged 65-74 (4%). Younger women were significantly more likely to report two or more symptoms of anxiety compared to men of the same age, with proportions of 12% for men aged 25-34 and 33% for women in this age group.
Age was a significant factor in whether someone had ever attempted suicide, with those aged 25-34 most likely to report having ever tried to take their own life (11%) and those aged 75 and over the least likely to report having done so (1%). A similar pattern by age was observed for both men and women.
Age was also a significant factor in relation to the prevalence of self-harm, with younger people being more likely than older people to have ever self-harmed (25% of those aged 16-24 and 20% of those aged 25-34 compared with 1% of those aged 65 and over). Table 2.9
2.2.10 CIS-R anxiety and depression scores, attempted suicide and self-harm (age standardised), 2021, by area deprivation and sex
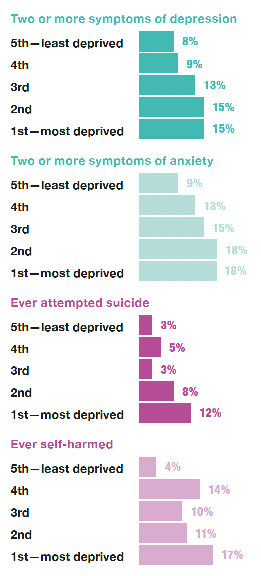
Neither the prevalence of two or more symptoms of depression nor anxiety were significant in 2021 when analysed by area deprivation.
However, significant variation was recorded in relation to whether suicide had ever been attempted, with adults from the most deprived areas being much more likely to ever have made an attempt to take their own life (12% compared to 3% among those in the least deprived areas).
Area deprivation also had a significant impact in relation to the prevalence of self-harm, however, there was not a linear pattern. The highest prevalence was among those in the most deprived areas (17%) and the lowest among those living in the least deprived areas (4%), with a range of 10% - 14% among those living in the three remaining areas.
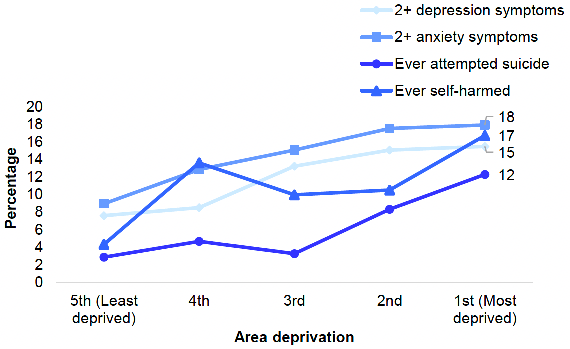
Similar patterns were reported for both men and women for depression, anxiety, suicide and self-harm when analysed by area deprivation in 2021, although prevalence was generally higher for women than men in the most deprived areas. Figure 2I, Table 2.10
2.2.11 Adult loneliness, 2021, by age and sex
In 2021, 8% of adults reported having felt lonely 'most' or 'all of the time' in the week prior to being interviewed. Meanwhile, 28% of adults reported having felt lonely 'some of the time' and 64% reported feeling lonely 'almost none of the time' or 'not at all'. Patterns were similar for men and women, with no significant variations by sex.
Overall, younger adults were more likely to report feeling lonely 'most' or 'all of the time' (14% of those aged 16-24) compared to older adults (4% of those aged 65 and over).
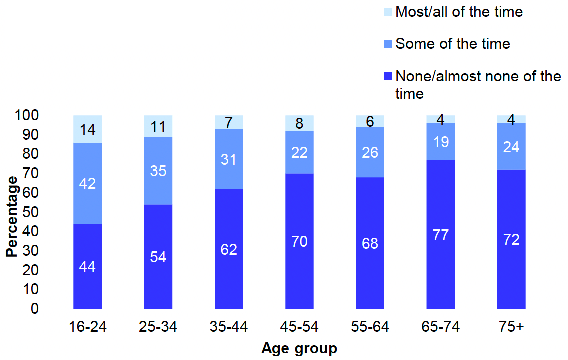
Figure 2J, Table 2.11
2.2.12 Adult loneliness (age-standardised), 2021, by area deprivation and sex
In 2021, loneliness was most prevalent among those in the most deprived areas, with 13% reporting having felt lonely 'most' or 'all of the time' compared with 5% among those in the least deprived areas.
Disparity by area deprivation was also evident for the proportions that reported feeling lonely 'none' or 'almost none of the time', which ranged from 72% among those living in the two least deprived areas to 52% among those living in the most deprived areas. No significant differences were observed between men and women. Table 2.12
2.2.13 Adult loneliness, 2021, by long-term illness and sex
In 2021, those with a limiting long-term condition were more likely to report being lonely 'most' or 'all of the time' (13%) compared to those with non-limiting long-term conditions (4%) and those who did not report having any long-term condition (5%).
Similar patterns were found for both men and women. Table 2.13
Table list
Table 2.1 Adult WEMWBS mean score, 2008 to 2021, by sex
Table 2.2 Adult WEMWBS mean score, 2021, by age and sex
Table 2.3 Adult WEMWBS mean score, (age-standardised), 2021, by area deprivation and sex
Table 2.4 Child WEMWBS mean score, 2017/2018/2019/2021 combined, by sex
Table 2.5 Child WEMWBS mean score, 2017/2018/2019/2021 combined, by area deprivation and sex
Table 2.6 GHQ-12 score, 2003 to 2021, by sex
Table 2.7 GHQ-12 score, 2021, by age and sex
Table 2.8 CIS-R anxiety and depression scores, attempted suicide and self- harm, 2008/2009 combined to 2021, by sex
Table 2.9 CIS-R anxiety and depression scores, attempted suicide and self- harm, 2021, by age and sex
Table 2.10 CIS-R anxiety and depression scores, attempted suicide and self- harm (age-standardised), 2021, by area deprivation and sex
Table 2.11 Adult loneliness, 2021, by age and sex
Table 2.12 Adult loneliness (age-standardised), 2021, by area deprivation and sex
Table 2.13 Adult loneliness, 2021, by long-term illness and sex
The tables can be found on the main report page under supporting files.
References and notes
1. World Health Organization (2018). Mental Health: strengthening our response. [Online]
2. World Health Organization (2009). Mental health, resilience and inequalities. [Online]
3. World Health Organisation (2018). WHO Guidelines: Management of Physical Health Conditions in Adults with Severe Mental Disorders. [online]
4. Mental Health Strategy: 2017-2027, Edinburgh: Scottish Government, (2017).
5. Bebbington, P. E. and McManus, S. ORCID: 0000-0003-2711-0819 (2020). Revisiting the one in four: the prevalence of psychiatric disorder in the population of England 2000-2014. The British Journal of Psychiatry: 216(1): 55-57.
6. See Mental health.
7. Johnson D, Dupuis G, Piche J, Claybourne Z and Coleman I (2018). Adult Mental Health Outcomes of Adolescent Depression: A Systematic Review. Public Medicine: 35(8): 700-716.
8. World Health Organization (2021). Depression Fact Sheet.
9. World Health Organization (2021). Suicide Fact Sheet.
10. World Health Organization (2017). Depression and Other Common Mental Disorders.
11. World Health Organization (2013). Investing in Mental Health.
12. NHS Health Scotland (2017). Mental Health: Inequality Briefing. [online]
13. A Connected Scotland: our strategy for tackling social isolation and loneliness and building stronger social connections. Edinburgh: Scottish Government (2018).
14. Health Scotland (2018). Social Isolation and Loneliness in Scotland: a review of prevalence and trends. [online]
15. Health Scotland (2018). Social Isolation and Loneliness in Scotland: a review of prevalence and trends. [online]
16. Melzer H, Bebbington P, Dennis M et al. Feelings of loneliness among adults with mental disorders. Social Psychiatry and Psychiatric Epidemiology 2013; 48: 5–13.
17. Victor CR and Yang K. The prevalence of loneliness among adults: A Case Study of the United Kingdom. The Journal of Psychology 2012; 146(1–2): 85–104.
18. Mental Health – Scotland's Transition and Recovery. Edinburgh: Scottish Government (2020).
19. Christie, S & Wilson, V. (2019) Chapter 2: Mental Wellbeing. McLean, J & Wilson, V (eds). The Scottish Health Survey 2019 – volume 1: main report Edinburgh: Scottish Government.