The Scottish Health Survey 2021 - volume 1: main report
Presents results for the Scottish Health Survey 2021, providing information on the health and factors relating to health of people living in Scotland.
Chapter 1 General Health, Cardiovascular Conditions and CPR Training
Chapter Summary
Among all adults in 2021:
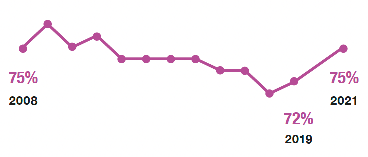
- 75% described their general health as 'very good' or 'good'
- 8% described their general health as 'very bad or bad'
Self-assessed 'very good' or 'good' general health has increased since 2019, although it has remained at around 75% for most of the period 2008 to 2021.
A higher proportion of men self-assessed their general health as 'very good' or 'good' in 2021.
- 77% men
- 73% women
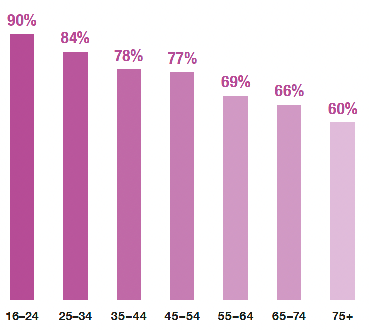
The proportion of adults who self-assessed their general health as 'very good' or 'good' decreased with age in 2021.
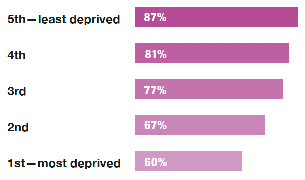
The proportion of adults who self-assessed their general health as 'very good' or 'good' decreased with increasing levels of deprivation in 2021.
- 96% of children described their general health as 'good' or 'very good'
- 1% of children described their general health as 'bad' or 'very bad'
Almost half of all adults reported living with a long-term condition in 2021.
- 47% living with a long-term condition
A third said they had a long-term condition which limited their day-to-day activities.
- 34% limited day-today activities
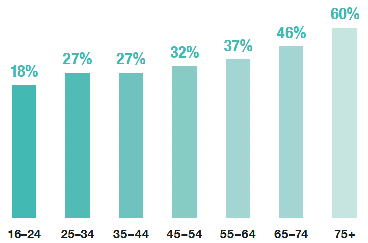
The proportion of adults living with a limiting long-term condition increased with age.
Following the same pattern as for all survey years since 2003, prevalence of cardiovascular disease (CVD) and diabetes was much higher in the most deprived areas compared with the least deprived in 2021.
Higher proportions of men than women had:
In 2021, nearly two thirds of adults reported ever attending cardiopulmonary resuscitation (CPR) training.
- 61% CPR training
Of those who had ever attended training:
- 46% had attended refresher training
- 26% had received some form of training in the last two years
General Health, Cardiovascular Conditions and CPR Training
Sophie Birtwistle
1.1 Introduction
Population measures of self-reported health are evidenced to be good predictors of mortality, morbidity or use of health care.[1] These measures can reflect subjective experiences of diagnosed and undiagnosed (both physical and mental) illnesses which can be overlooked by more objective measurements.
The prevalence of long-term conditions has placed considerable and unsustainable strain on healthcare provision.[2] Further challenges are presented by ongoing inequalities in health outcomes and the ageing population.[3]
Cardiovascular disease (CVD) is a general term for conditions that affect the heart and blood vessels, whereby blood flow to the heart, brain, or body is restricted. Its main components are ischaemic heart disease (IHD) and stroke, both of which are well-established clinical priorities for the NHS in Scotland.[4],[5] Since 2009, there has been a steady downward trend in incidence and deaths from IHD and stroke in Scotland.[6] However, IHD continues to be one of the leading causes of death in Scotland, with stroke also remaining as one of the biggest killers as well as the leading cause of disability in Scotland.[5]
Diabetes, the most prevalent metabolic disorder, is a growing health challenge for Scotland. The prevalence of people registered with Type 1 diabetes has increased since 2013, and this reflects better survival and the rising prevalence in children. The majority of registered people have Type 2 diabetes. The number of people registered with Type 2 diabetes has increased since 2013 which could relate to several factors, including: demographic change - diabetes is more prevalent in older people, so the increasing number of older people each year increases the prevalence of diabetes - better survival, and possibly better detection.[7]
Cardiac arrest is when the heart suddenly stops pumping blood round the body. When someone has a cardiac arrest cardiopulmonary resuscitation (CPR) will keep blood circulating until attempts are made to restart the heart. Every year over 3,000 people around Scotland are treated by the Ambulance Service after having an Out of Hospital Cardiac Arrest (OHCA) with around 1 in 10 surviving to hospital discharge. Key factors in determining survival from OHCA are early, high quality hands-only CPR and counter-shock therapy (defibrillation).
1.1.1 Policy background
The Scottish Government's strategic policies focus on promoting and improving general health and wellbeing, as well as supporting those living with long-term illnesses/conditions. The six Public Health Priorities for Scotland[8] are aimed at improving the health of people in Scotland and are supported by a number of strategies covering specific conditions such as heart disease,[9] stroke[10] and diabetes.[11]
The Heart Disease Action Plan (2021) sets out the priorities and actions Scottish Government will take to minimise preventable heart disease and ensure equitable and timely access to diagnosis, treatment, and care for people with suspected heart disease in Scotland.
Increasing survival following a cardiac arrest is supported by Scotland's OHCA Strategy.[12] Through the delivery of the initial OHCA Strategy (2015-2020), OHCA survival rates rose from 1 in 20 to 1 in 10, and bystander CPR rates rose from 43% before the strategy to 64% in 2020. In addition, over 640,000 people were equipped with the skills to perform CPR during the lifetime of the strategy. The strategy was refreshed in 2021.[13] Key aims of the refreshed strategy are to equip a total of 1 million people in Scotland with CPR skills by 2026 and to increase the number of OHCAs which have a defibrillator applied before the ambulance service arrive from 8% to 20%.
The Stroke Improvement Plan (2014) provides the overarching policy framework for improving stroke services in Scotland. A Progressive Stroke Pathway[14] was published on 22 March 2022 and met with public endorsement from the Stroke Association. The Progressive Stroke Pathway was produced by the National Advisory Committee on Stroke and sets out a vision for each stage of the stroke pathway, from diagnosis and acute care to the provision of person-centred rehabilitation.
The recommendations in the Progressive Stroke Pathway will inform the publication of Scottish Government's refreshed Stroke Improvement Plan, to be published by the end of 2022. Work is also continuing to progress the rollout of a National Thrombectomy Service in Scotland, with 'hub' centres providing mechanical thrombectomy in NHS Tayside, NHS Lothian, and NHS Greater Glasgow & Clyde.
In 2014, the Scottish Government published its first Diabetes Improvement Plan, which set out aims and priorities to deliver safe, effective, and person-centred healthcare, treatment, and support to those living with diabetes. The Plan has been refreshed and was subsequently published on 25th February 2021, outlining commitments from 2021 to 2026.
The Framework for the Prevention, Early Detection and Early Intervention of Type 2 Diabetes was published in July 2018. It targets early identification of those at risk of type 2 diabetes and identification of those with pre-diabetes through diagnostics.
1.1.2 Reporting on general health, CVD, diabetes and CPR training in the Scottish Health Survey
In this chapter trends in self-assessed general health for adults and children are presented. Prevalence of self-reported long-term conditions in adults is reported for 2021. Trends for self-reported CVD conditions and diabetes prevalence in adults are presented as well as for 2021. Blood pressure level trends and detection and treatment of hypertension are not presented in 2021 as physical measurements were not taken during fieldwork as a result of COVID-19 restrictions. Prevalence of CPR training (including refresher training) and the length of time since CPR training was last attended are also reported for 2021.
The area deprivation data are presented in Scottish Index of Multiple Deprivation (SIMD) quintiles. To ensure that the comparisons presented are not confounded by the different age profiles of the quintiles, the data have been age-standardised. For a detailed description of both SIMD and age-standardisation as well as definitions of other terminology used in this chapter and for further details on the data collection methods for general health, CVD and CPR training, please refer to Chapter 2 of the Scottish Health Survey 2021- volume 2: technical report.
Supplementary tables on general health and CVD are also published on the Scottish Government website: Scottish Health Survey.
1.2 General Health, CVD and CPR Training
1.2.1 Self-assessed general health, adults and children, 2008 to 2021, by sex
The proportion of adults who reported their general health as 'good' or 'very good' has shown only small fluctuations between 2008 and 2021. Since 2019 this proportion has increased from 72% to 75% in 2021. A similar pattern was observed for both men and women, with the proportion of men self-reporting as being in 'good' or 'very good' health the same as or higher than the proportion of women between 2008 and 2021 (77% of men and 73% of women in 2021). Self-assessed 'bad' or 'very bad' general health for all adults has remained in the range of 7%-9% since 2008 (8% in 2021). This trend was also observed for both men and women (8% for both men and women in 2021).
For children, the large majority continue to be reported as having 'good' or 'very good' general health (96% in 2021). No more than 1% of children have been reported as being in 'bad' or 'very bad' general health in any year since 2008. Table 1.1
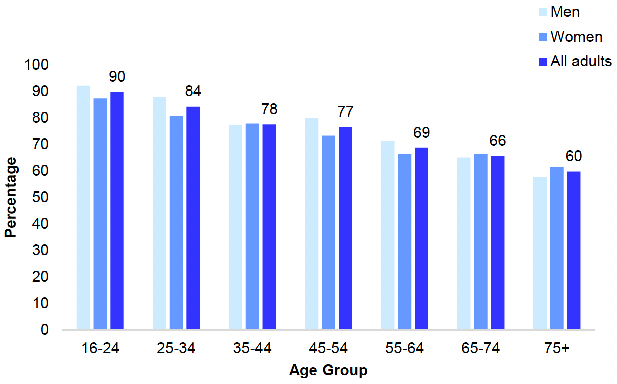
1.2.2 Adult self-assessed general health, 2021, by age and sex
The proportion of adults self-assessing their general health as 'good' or 'very good' decreased with age. In 2021, 90% of those aged 16-24 described their health as 'good' or 'very good' with this proportion falling to 60% of those aged 75 and above. A similar pattern was observed for both men and women.
The proportion of adults who self-assessed their general health as 'bad' or 'very bad' generally increased with age, from 3% for those aged 16-24 to 13% for those aged 75 and above. Figure 1A, Table 1.2
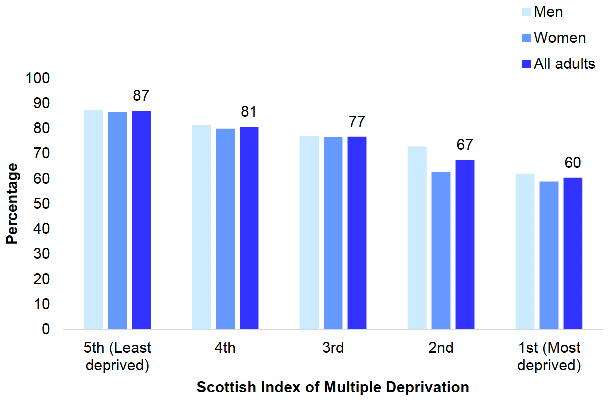
1.2.3 Adult self-assessed general health (age-standardised), 2021, by area deprivation and sex
In 2021, the age-standardised proportion of adults that self-assessed their general health as 'good' or 'very good' decreased as area deprivation increased. This proportion declined from 87% in the least deprived quintile to 60% in the most deprived quintile.
This pattern was reversed for adults (age-standardised) who self-assessed their general health as 'bad' or 'very bad'. This proportion increased from 3% in the least deprived quintile to 15% in the most deprived quintile. The patterns were similar for both men and women. Figure 1B, Table 1.3
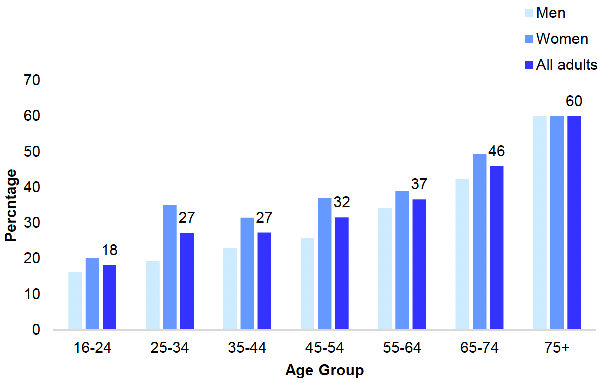
1.2.4 Prevalence of long-term conditions in adults, 2021, by age and sex
In 2021, almost half (47%) of the adult population reported living with a long-term health condition. Women were more likely than men to report having such a condition (52%, compared with 43%). This proportion increased with age for both men and women. Just over a quarter (26%) of all adults aged 16-24 reported living with a long-term condition, rising to almost three-quarters (74%) of those aged 75+.
In 2021, a third (34%) of adults reported living with a limiting long-term condition, more than two-thirds of those with any long-term condition. The proportion of adults living with a limiting long-term condition increased with age. Less than one-in-five (18%) of those aged 16-24 reported living with a limiting long-term condition compared with three-in-five (60%) of those aged 75 and above. Again, women were more likely than men to report having a limiting condition (39% compared with 30%). Figure 1C, Table 1.4
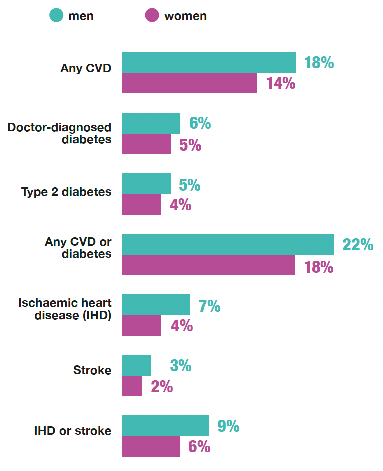
1.2.5 CVD and diabetes, 2021, by age and sex
Any CVD
In 2021, 16% of adults reported having ever had any Cardiovascular Disease (CVD), with this proportion increasing with age. Prevalence of CVD was 5% for those aged 16-24 compared with 41% for those aged 75 and above. Men reported a higher prevalence of CVD than women (18%, compared with 14%), although the difference was only significant for those aged 65 to 74 (33% of men compared with 20% of women).
Doctor-diagnosed diabetes
In 2021, 6% of adults reported having doctor-diagnosed diabetes, and the prevalence of this increased with age. Of those aged 16-24 fewer than 0.5% reported having doctor-diagnosed diabetes compared with 13% of those aged 75 and above. Prevalence of diabetes was slightly higher for men than for women (6% compared with 5%).
Diabetes Type 1
In 2021, 1% of adults had Type 1 diabetes. This proportion did not vary between men and women and did not vary significantly by age.
Diabetes Type 2
In 2021, Type 2 diabetes was more common than Type 1, with 5% of adults reporting this condition. Prevalence increased with age, from less than 0.5% of those aged 16-24 to 12% for those aged 75 and above. This pattern was similar for both men and women.
Any CVD or diabetes
In 2021, 20% of adults reported having any CVD or diabetes. The prevalence of CVD or diabetes increased with age from 5% of those aged 16-24 to 47% of those aged 75 and above. Men reported a higher prevalence of having any CVD or diabetes than women (22% compared with 18%). Differences in this proportion between men and women were significant in the 55-64 age group (29% of men compared with 22% of women of this age) and the 65-74 age group (41% of men compared with 26% of women).
Ischaemic Heart Disease (IHD)
In 2021, 5% of adults reported ever having had IHD, and the prevalence of this increased with age. No one aged 16-24 participating in the survey had ever had IHD, compared with 20% of those aged 75 and above. This pattern was similar for both men and women, albeit with men reporting a higher prevalence of IHD than women (7% compared with 4% of women).
Stroke
In 2021, 3% of adults reported ever having had a stroke. This proportion increased with age. None of the participants in the survey aged 16-24 reported ever having had a stroke compared with 10% of those aged 75 and above. This pattern was similar for both men and women. Men reported a higher overall prevalence of stroke compared with women. In 2021, 3% of men reported having ever had a stroke compared with 2% of women.
IHD or Stroke
The proportion of adults in 2021 that reported ever having had IHD or a stroke was 7%. This proportion increased with age, from no one participating in the survey aged 16-24 to 26% of those aged 75 and above. Prevalence of IHD or stroke was higher for men than women (9% compared with 6%). Table 1.5
1.2.6 CVD and diabetes prevalence (age-standardised), 2003 to 2021, by area deprivation and sex
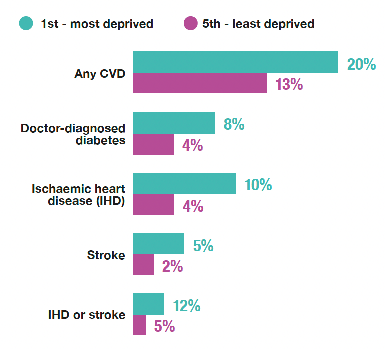
Any CVD
Prevalence of age-standardised CVD by area deprivation has varied a little since 2003, but CVD has remained more prevalent in the most deprived quintile compared with the least deprived. In 2021, 20% of adults in the most deprived quintile reported having any CVD compared with 13% in the least deprived quintile. Patterns were similar for both men and women.
Doctor-diagnosed diabetes
As in previous years, age-standardised doctor-diagnosed diabetes was more prevalent in the most deprived quintiles compared with the least deprived quintiles. In 2021, 8% of adults in the most deprived quintile reported doctor-diagnosed diabetes compared with 4% in each of the two least deprived quintiles. Patterns were similar for both men and women.
Ischaemic Heart Disease (IHD)
In 2021, the prevalence of IHD varied by area deprivation, in a similar way to that seen in previous years. IHD was more prevalent in the most deprived quintile (10%) than in the three least deprived quintiles (4%). Similar patterns were observed for both men and women.
Stroke
In 2021, as in every year since 2003, the prevalence of stroke varied by area deprivation and was more prevalent in more deprived quintiles compared with less deprived quintiles. In 2021, 5% of adults in the two most deprived quintiles reported ever having had a stroke compared with 1% - 2% in the three least deprived quintiles.
IHD or stroke
The pattern of prevalence of IHD or stroke across the SIMD quintiles has not changed since 2003. In 2021, prevalence was higher in more deprived quintiles compared to less deprived quintiles. In 2021, there was a 12% prevalence in IHD or stroke in the most deprived quintile compared with 5% in the three least deprived quintiles. This pattern was similar for both men and women with men having a higher prevalence of IHD or stroke compared to women. In the most deprived quintile, there was a 15% prevalence in IHD or stroke for men and 10% for women. In the least deprived quintile, there was 7% prevalence for men and 3% prevalence for women. Table 1.6
1.2.7 Adult prevalence of CPR training, length of time since original training and whether attended refresher, 2021, by age and sex
In 2021, 61% of adults reported ever having attended CPR training, with variation in this proportion by age. The proportion was highest for those aged between 25 and 54 (67 - 68%). Above this age it fell to 35% of those aged 75+. Women were slightly more likely than men to ever have attended training (63% of women compared with 59% of men).
Of those who reported having ever attended CPR training, 81% reported that their original training was four years ago or more. Only in the youngest age group was this proportion significantly lower (46%). There was no significant difference between men and women. Only 3% of adults reported having attended their original CPR training in the last 12 months and a further 3% reported having received their training between one and two years ago, while 12% reported receiving their original training between two and four years ago.
Of those who ever attended CPR training, just less than half (46%) reported attending refresher training. The proportion of those who attended refresher training was highest for those aged 45-54 (54%).
Of all adults in 2021, 16% reported attending any CPR training in the last two years, equating to 26% of those who had ever attended training. The proportion of adults who attended training in the last two years was just under a quarter (20% - 23%) for the younger age groups (16-54), and then decreased with age, to 1% of those aged 75 and above. Figure 1D, Table 1.7
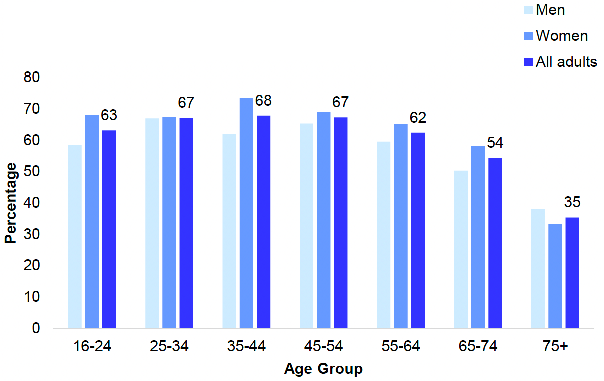
Table list
Table 1.1 Self-assessed general health, adults and children, 2008 to 2021, by sex
Table 1.2 Adult self-assessed general health, 2021, by age and sex
Table 1.3 Adult self-assessed general health (age-standardised), 2021, by area deprivation and sex
Table 1.4 Prevalence of long-term conditions in adults, 2021, by age and sex
Table 1.5 CVD and diabetes, 2021, by age and sex
Table 1.6 CVD and diabetes prevalence (age-standardised), 2003 to 2021, by area deprivation and sex
Table 1.7 Adult prevalence of CPR training, length of time since original training and whether attended refresher, 2021, by age and sex
The tables can be found on the main report page under supporting files.
References and notes
1. Vaillant, N and Wolff, FC (2012). On the reliability of self-reported health: Evidence from Albanian Data. Journal of Epidemiology and Global Health; 2(2): 83-98.
2. The Scottish Government (2018). Public Health Priorities for Scotland. [Online]
3. ScotPHO. (2019). Older people: key points. [Online]
4. Heart Disease Action Plan. Edinburgh: Scottish Government, (2021). Available from: Heart disease: action plan - gov.scot (www.gov.scot)
5. Stroke Improvement Plan, Edinburgh: Scottish Government, 2014.
6. National Records of Scotland (2021). Vital Events Reference Tables 2020. [Online]
7. Scottish Diabetes Data Group, NHS Scotland (2018). Scottish Diabetes Survey 2020. [Online]
8. Public Health Priorities for Scotland, Edinburgh: Scottish Government/COSLA, 2018.
9. Heart Disease Action Plan (2021). Edinburgh: Scottish Government, 2021. Available at: Heart disease: action plan - gov.scot (www.gov.scot)
10. Diabetes Improvement Plan (2014). Edinburgh: Scottish Government, 2014.
11. Stroke Improvement Plan (2014). Edinburgh: Scottish Government, 2014.
12. Out of hospital cardiac arrest: strategy 2021 to 2026. Edinburgh: Scottish Government, 2021.
13. The Scottish Government (2021), Scottish Out of Hospital Cardiac Arrest Strategy 2021 – 2026, available at: Out of hospital cardiac arrest: strategy 2021 to 2026 - gov.scot (www.gov.scot)
14. Strokes: progressive stroke pathway (2022). Edinburgh: Scottish Government, 2022.