Tuberculosis - RNOH/GIRFT review: national report
The GIRFT Tuberculosis (TB) report is a comprehensive, data-driven national review of TB services across Scotland.
8 Workforce Issues in the Management of Tuberculosis
The efficient and safe running of TB services is dependent upon its staff and infrastructure. To deliver against the requirements of a variable, but increasing workload, acute providers and Health Boards need to ensure there are sufficient staff to not only deliver the service, but also to ensure policies are up to date and provide education. These responsibilities are covered in the ‘workforce’ sections for medical, nursing and administrative and clerical resources. Pharmacist input is also essential and covered in the ‘medicines management’ section.
TB colleagues should be encouraged to participate in academic activities related to TB and this should be recognised in job plans. This activity should include an audit of the service provided, with presentations at either local or national meetings. Where possible, more formal research should be undertaken which may be either commercial, multi-centre trials or ‘in house’. Supporting staff, from all disciplines to apply for grants in TB research is to be encouraged. Other academic activities beyond teaching such as contributing to and authoring guidelines should also be recognised and supported.
Recommendation: Workforce Issues in the Management of Tuberculosis
2. TB clinicians and teams should be encouraged and supported to participate in research and other academic activities which include teaching (as in workforce specific sections) production of guidelines etc.
P, HB
8.1 Medical Workforce
From the survey returns, and data validated during the deep dives, there was marked variation in the medical support for TB services. Only two services had any ‘supporting professional activity’ (SPA) time for ‘running the service’ and for these two it was 1x ‘programmed activity’ (PA) or less (see graph 15 in the data pack in Annex E).
It is essential that the clinical lead has sufficient time for developing policies and protocols that are up to date and compliant with national advice. Meeting with the Health Board Directorate management team and infection prevention teams is an essential way of raising and maintaining the profile of TB management. As noted in Table 3, in the Delays in Management section 10.3, education is a consistent theme and the clinical lead should have responsibility for developing education programs across the Health Board in conjunction with colleagues from Public Health and Health Protection. This is especially important in low incidence Health Boards to maintain the knowledge and profile of tuberculosis with the positive benefit of reducing delays to diagnosis.
The overall service lead responsibility was split between infectious disease and respiratory doctors but in some services there was no recognised ‘lead’, which is a serious concern if there is no named clinician to take responsibility.
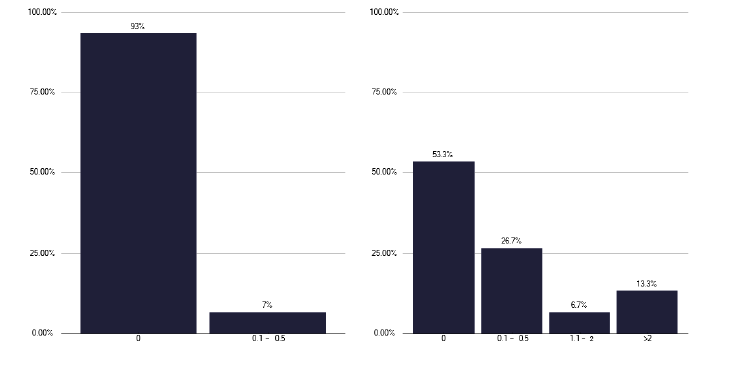
With regards to respiratory medicine, shown in Figure 1, the absence of general SPA time was marked. Direct clinical care (DCC) varied with the size of the service but there was generally insufficient DCC time and it appeared to be counted only as clinic time.
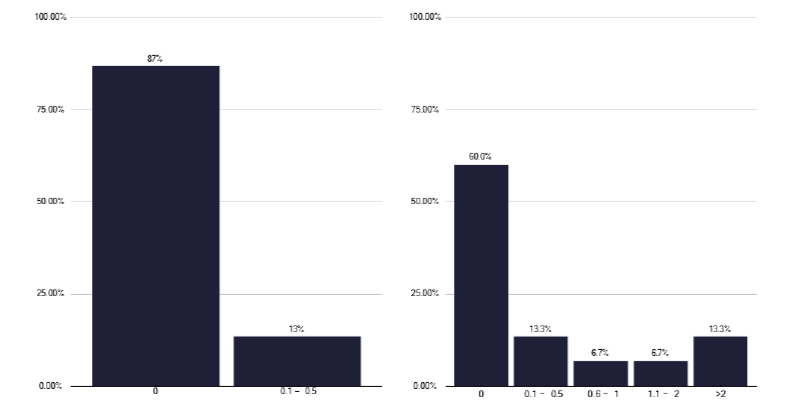
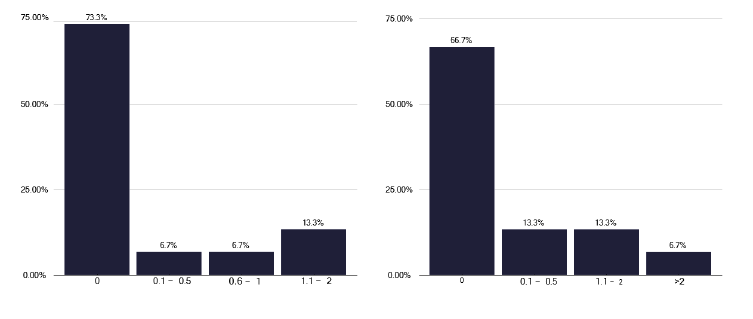
For both infectious diseases, Figure 2 and paediatricians, Figure 3, there were similar findings as for respiratory medicine, with no general SPA time and limited DCC time. These are issues that need to be addressed for all three speciality teams dealing with TB.
We also noted during some of the deep dives, where patients with TB were managed by non-dedicated respiratory or ID physicians. In one provider, the random distribution of patients meant that some clinicians could potentially go several years without managing a patient with TB, a practice that is unacceptable.
Furthermore, this lack of co-horting patients led to patients with TB being managed in general clinics, with the potential for cross infection. We also noted some services where the bulk of care was delivered by a named respiratory physician, but where some patients were randomly managed by one of several ID physicians. The recommended practice should ideally be for care to be shared, with a named ID and named respiratory physician for adult care where the clinicians’ skillsets complement each other, especially around the management of Human Immunodeficiency Virus (HIV) and TB co-infected patients.
Delivering care to patients with TB doesn’t only include the face-to-face activity of clinics but also general TB administration. This is a poorly-recognised issue, and missed results can lead to delays in management. Communicating with colleagues together with attending regular service meetings is essential for managing TB patients (depending on the size of the service).
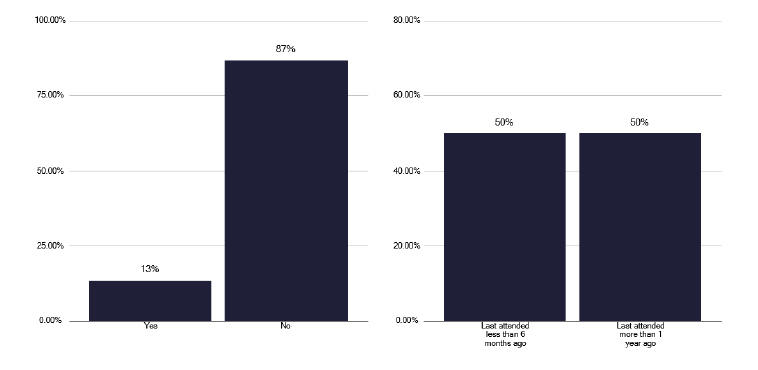
Embedded within this DCC activity is time for undertaking cohort reviews. These are an important aspect of improving services with independent external scrutiny, so time is required for both attending and preparing for cohort reviews, together with TB leads acting as ‘external service reviewers’. Regrettably we found very few services that were undertaking cohort reviews, one of which had only done so on the basis of a recent surge in notifications Figure 4.
For lower volume services, such as those for children and young people (CYP), it is difficult to maintain a skill set within all Health Boards and so more national support needs to be established. This is discussed in the CYP section.
Recommendations: Medical Workforce
3. Each TB service should have a recognised lead who is named, with responsibility for maintaining policies and overseeing Health Board education. This is dedicated lead SPA time and is generally the same for most services as even those with few notifications still need to deliver these general aspects of the TB service.
P, HB
4.The clinical lead should deliver all, or the bulk of TB medical care and should have sufficient DCC time in their job plan for this to take place.
P, HB
5. Depending on the size of the service, time for a clinical deputy and/or support needs to be included. There are advantages of this being from a different speciality, especially in managing co-infection with HIV.
P, HB
6. In all job plans, appropriate SPA time for providing education and self-continuing professional development (CPD) should be included together with DCC time for service delivery. This should include, not only clinic activity, but time for regular local and Health Board or National MDTs and clinical administration.
P, HB
7. Cohort reviews should be re-established with time in job plans to attend, with the lead clinician acting as a reviewer for other Health Boards. To support data collection for such reviews, there needs to be administrative time, and such reviews should be a feature of job plans for all individuals i.e. medical, nursing, pharmacist. A formal report with actions should be generated, hence the need for administrative time.
P, HB
8. For some services such as CYP, non-tuberculous mycobacteria, where there may be a Health Board or National lead role, time needs to be allocated in the individual Lead’s job plan for this work. Such networks need to be agreed and funded at Health Board or at National level.
P, HB
8.2 Nursing Workforce
The nursing workforce has a variable model, with some services having embedded TB nurses, others having a combination of a dedicated TB nurse with support from Health Protection, whilst others have a Health Protection service that ‘in reaches’ into the acute provider, and finally where Health Protection run the TB service.
This variability in TB nurse service provision does not fully relate to the number of notifications, contacts traced or use of preventative therapies. CYP TB services are often small and have no dedicated workforce. In some services, the TB nurses also administer Bacillus Calmette-Guérin (BCG) as part of a neonatal programme, while other services had a well-established process for neonatal BCG vaccination, as described the BCG section of prevention 11.2.
Most nurses were graded at Band 7 and we found fewer lower banded or unqualified nurses (Healthcare Assistants), meaning that the higher qualified staff were often doing routine tasks that could be delegated. This is in sharp contrast to England where Band 3 and 4 staff play a major role in TB services. Staffing of services in general needs to be considered in light of The Health and Care (Staffing) (Scotland) Act 2019.
We did hear different views about the benefits of unqualified staff. In several deep dives we heard that these staff played a useful role, while in other visits we heard the view that Band 3 and 4 nurses would have a minimal role. This was based upon the changing epidemiology, such that most notifications were born outside of the UK and were adherent to therapy and so there was little need for enhanced case management (ECM), where Directly Observed Therapy (DOTs) and Video Observed Therapy (VOTs) would be needed. This was in sharp contrast to other areas in Scotland where both geography and ECM generated a significant workload and DOTs and VOTs were important aspects of therapy that could be fulfilled by lower banded nursing staff. Depending upon the service and local need, the indicative workforce developed in the England report could form the basis for staffing discussions.
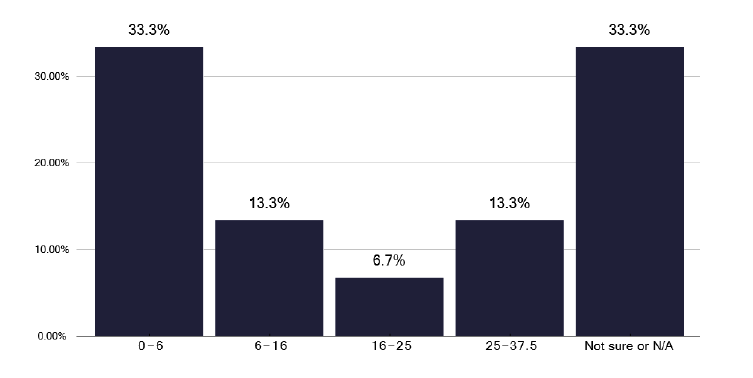
Whatever the model, senior nursing management to support the service is important, but limited, as shown in Figure 5.
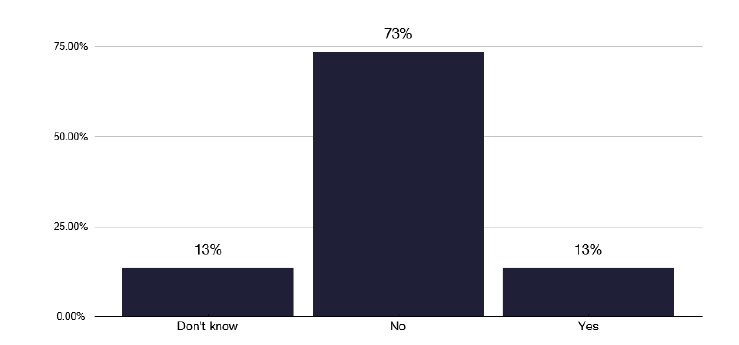
Data from the survey did show several pressure areas, with insufficient staff to deliver a TB service during times of short-term sickness or annual leave. Figure 6 highlights the capacity issues within the nursing workforce. We did note the inherent flexibility of the larger team to fill any gaps, with nurses in Glasgow working as a team and when Health Protection teams were involved in the TB services.
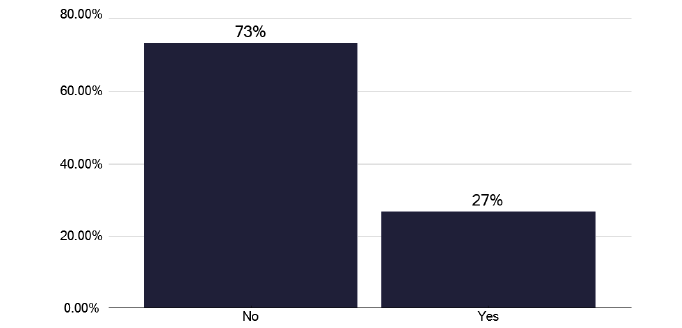
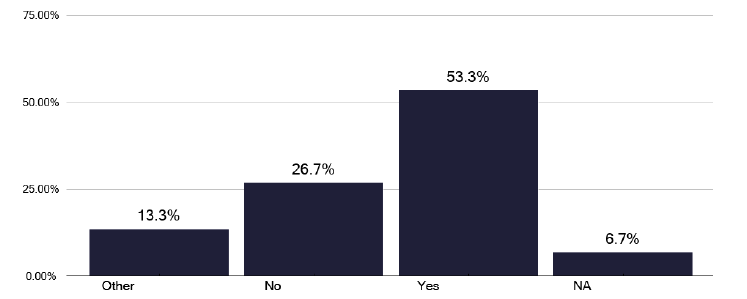
Surprisingly only 27% of services ran ‘nurse-led’ clinics, as in Figure 7, though we found excellent examples during the deep dives of nurse-led clinics, where they would order radiographs and prescribe medications. The good practice via the link in Annex E has examples of these services with their standard operating procedures and protocols. We noted from the survey, in Figure 8, that over half of nurses could order X-rays and many could prescribe medication, though we did hear that some nurses did not think this was needed. The role of TB nursing staff during inpatient management is commented on in section 10.2.
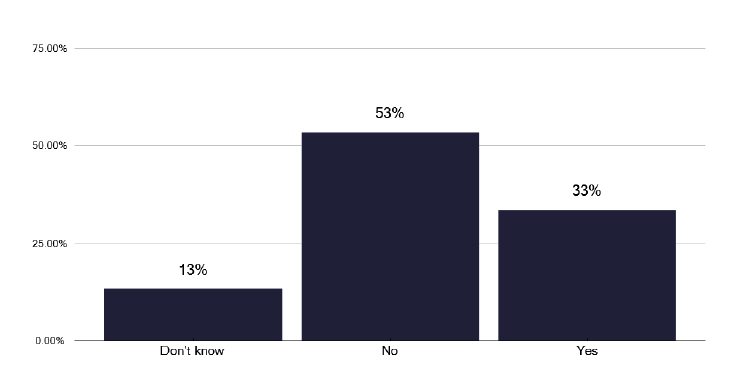
Education and training are important and we noted that only one third of services had access to training budgets for nursing staff, as shown in Figure 9. Education is a key aspect of continuing professional development and given how the management of TB is continuing to change, time for education, both internal and on recognised external courses, is essential in ‘nursing job plans’ with access to appropriate funds to support this.
A specific issue in the low volume services was having sufficient CYP infrastructure, not only for managing the relatively few notifications, but also for the large number of contacts that may occur.
Often the volume of work is insufficient for dedicated CYP TB nursing teams and so a flexible approach, with Health Protection and liaising with other services is important unless there is specific children’s’ nurse training within the team.
Recommendations: Nursing Workforce
9. Services should review their nursing workforce to ensure they are not doing tasks which could be done by lower banded staff i.e. ensuring senior qualified staff are working at ‘top of licence’.
P, HB
10. There are excellent examples of nurses where they run their own clinics and prescribe and request radiographs. These nursing options should be explored in each TB service.
P, HB
11. There should be sufficient senior nursing time to manage the TB service.
P, HB
12. All nurses, as part of their re-validation process, should ensure they are up to date with current TB practices and where training is required should have access to funds for such education, at whatever level is appropriate.
P, HB
8.3 Administration & Clerical Support
Throughout the deep dives, we found a scarcity of formal administrative staff dedicated to the TB services. This is listed in Table 2 and leads to senior nursing staff undertaking inappropriate tasks, such as routine chasing, and calls with patients and carers, which are very time consuming.
While booking clerks can help free up clinic management time, they are often unaware of some of the important issues of infection prevention for patients who may have active TB, with the risk of transmission to other potentially immunocompromised patients in an open clinic waiting area.
While medical secretaries have taken on some activity for consultants, nurses are often unsupported and need to do clinic letters, chase results etc., which are duties that can be undertaken by administrative and clerical staff, freeing up qualified nurse time to work at top of licence.
Additionally, there is a considerable burden of work in updating data sets such as ESMI that also sits with nursing staff, a duty that can readily be performed by admin and clerical staff, freeing up clinical time. A further duty that will be required with the establishment of cohort reviews is the need to organise the notes and collate results, a very time consuming activity that with training can be delegated.
| TB Service | Specific Admin/Nursing Support | Notifications by service |
|---|---|---|
| Service A | Supporting staff (Band 3): 0.8 WTE Admin (Band 4): 0.4 WTE | <20 |
| Service B | Supporting staff (Band 4): 0.1 WTE Admin (Band 3): 0.1 WTE | <10 |
| Service D | Admin (Band 3): 0.22 WTE | >20 |
| Service E | Admin (Band 4): 2 WTE | <10 |
| Service F | Admin (Band 4): 0.13 WTE | >20 |
| Service I | Admin (Band 4): 0.1 WTE | >20 |
| Service J | Admin (Band 4): 0.25 WTE | <10 |
| Service K | Admin (Band 4): 0.14 WTE | <10 |
| Service L | Admin (Band 3): 0.1 WTE | <10 |
Recommendations: Admin and clerical workforce
13. On a pro rata basis, Admin & Clerical support at Band 3 or Band 4 should be available in a dedicated role to support the TB service, acting as the focus for the service. This role would develop reports, collate information for MDTs and cohort reviews and facilitate data entry and general communication, informing all parties involved in TB care of decisions and outcomes.
P, HB
Contact
Email: healthprotection@gov.scot