Tuberculosis - RNOH/GIRFT review: national report
The GIRFT Tuberculosis (TB) report is a comprehensive, data-driven national review of TB services across Scotland.
11 Preventative Strategies
Preventative strategies for managing tuberculosis cover a range of different populations, and interventions are based on the knowledge that individuals exposed to tuberculosis can develop active disease later. This principle of identifying individuals who have been exposed to TB and have ‘dormant’ or ‘latent’ disease, with the potential risk of developing the disease, is especially relevant to different populations.
The population at risk, beyond those found during contact tracing, may be migrant workers, asylum seekers, those identified through occupational health screening and individuals whose immunity is potentially going to be reduced by using disease-modifying agents. Additionally, identification of individuals through exploring the contacts of a patients with active notified disease, contact tracing, is an important aspect of preventing the spread of active disease.
The preventative strategies employed may be a ‘wait and see’ administration of BCG or a short course of anti-tuberculosis drugs.
These areas will be considered as: BCG; contact tracing, occupational health screening, disease modifying agents (biological therapies) and migrant/asylum seeker/refugee populations, with recommendations made for each.
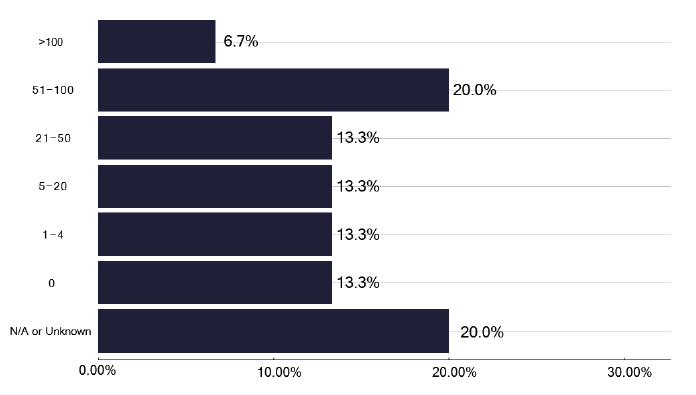
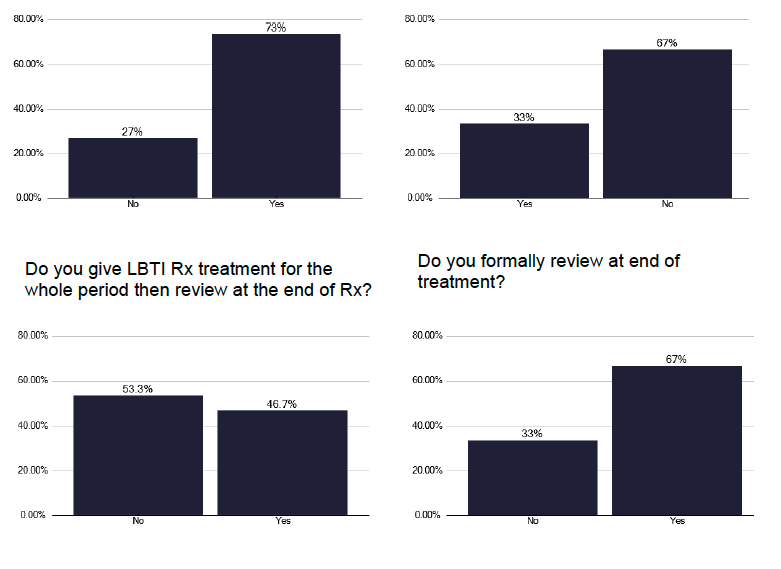
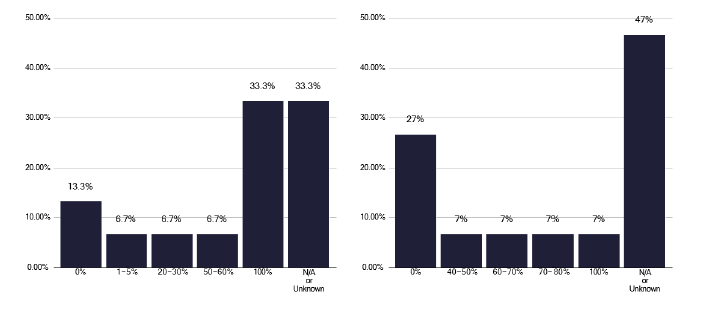
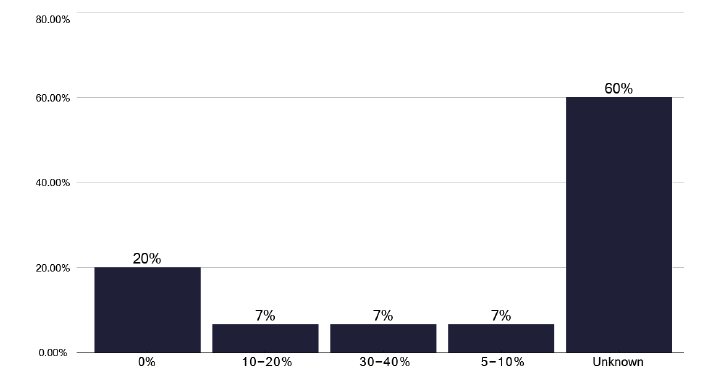
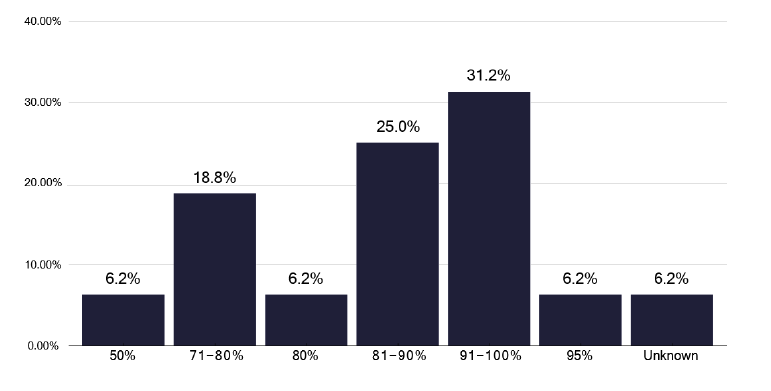
An analysis of these different preventative management plans, recognising that they may vary in different populations, shows a significant variation in the number of patients receiving treatment for latent TB, as shown in Figure 68. However, this is self-reported, so we are unsure of the populations included. The process of care for these Individuals on commencing treatment varied, see Figure 69a & 69b, with some being reviewed within 2-4 weeks of initiating treatment, some after 1 month, and 46% of services gave all the treatment at initial attendance and reviewed at the end of treatment. However, one third of services did not review after the end of treatment, suggesting there is no standard process that is followed. The checking liver function tests (LFTs) was also variable, with 53% checking after 2 weeks, but 20 % stated they never checked LFTs, some reviewing based on age criteria.
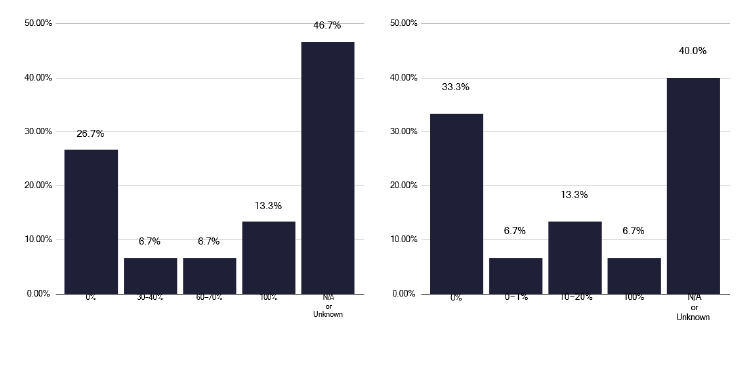
The support of these individuals on treatment also varies. Figure 70 suggests most patients were followed up by a phone call, though this was unknown in one third of responses. For a home visit, a large number were unknown, with four services bringing a variable percentage back to clinic. A similar figure for a face-to-face appointments was noted, as in Figure 71, and a significant number did not know about the use of virtual appointments.
While recognising there is some overlap in these questions, and variation in the population needing these interventions, there is considerable inconsistency. This may be of more importance when we consider Figure 72, which asks about the number of these LTBI individuals who need enhanced case management (ECM), as over 60% were unknown.
Note: This includes those from national and/or local LTBI testing and treatment programmes and/or contact tracing
Recommendations: Preventative strategies
54. A formal preventative strategy needs to be developed for Scotland, encompassing all groups who may be eligible, but also recognising that some populations may have more numbers identified from a screening exercise and some may have a greater benefit from preventative therapy.
N
55. There is wide variation in the practice of initiating and reviewing treatment for latent TB, including checking liver function and the nature of any follow up. TB services should develop a more uniform practice based on best evidence.
N
11.1 Contact Tracing
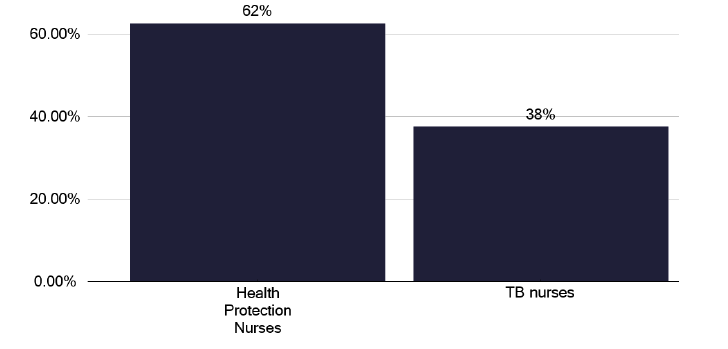
Contact tracing describes the process of identifying individuals who have been in contact with an individual who has notified tuberculosis. Usually, a nurse from the TB team or, more commonly in Scotland, as seen in Figure 73, the Health Protection team, will meet the patient (called the “index case”), and find out who their contacts are, recognising the longer an individual is exposed to the index case, if infectious, the greater the risk of contracting tuberculosis.
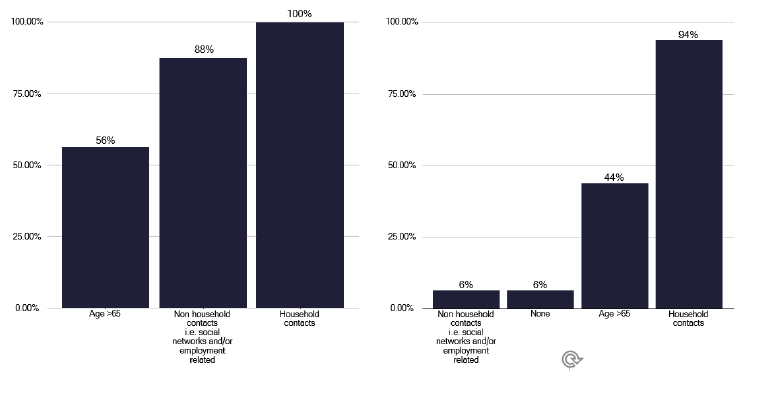
We noted variation in several aspects of contact tracing. In Figure 74, we see the practice of who is screened if the index case has pulmonary or non-pulmonary, and in Figures 75 and 76, the number of contacts identified depending upon the disease site. The practice of follow up arrangements if the contact (adult, child or young person) does not attend, are shown in graphs 306 and 307 in the data pack in Annex E.
Note: Time period includes notified cases between January 2022 and December 2022. The data source is the Enhanced Surveillance of Mycobacterial Infections (ESMI) system
Note: Time period includes notified cases between January 2022 and December 2022. The data source is the Enhanced Surveillance of Mycobacterial Infections (ESMI) system.
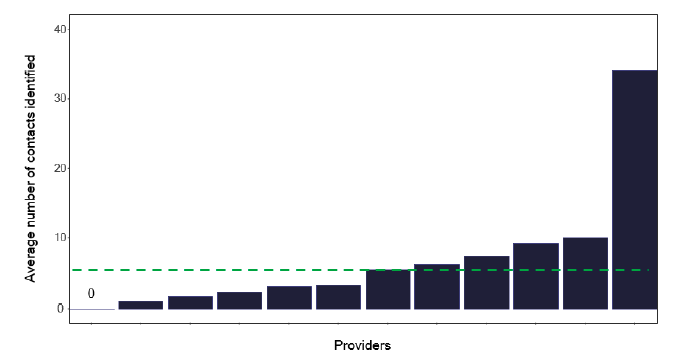
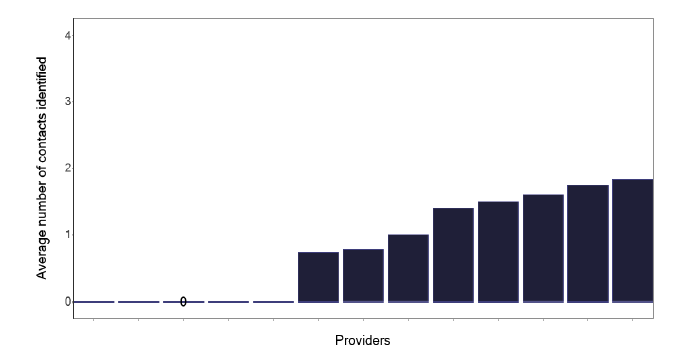
The average number of contacts per notification is shown in Figure 77, which shows that those services with more than 20 notifications have fewer contacts. The reasons for this are unclear, as the case-mix appears similar to those services with fewer notifications. The practice of the larger services, perhaps merits a review to investigate why there is a lower number of contacts. Of course, the services with 6-20 notifications may be undertaking too many contacts, as detailed below.
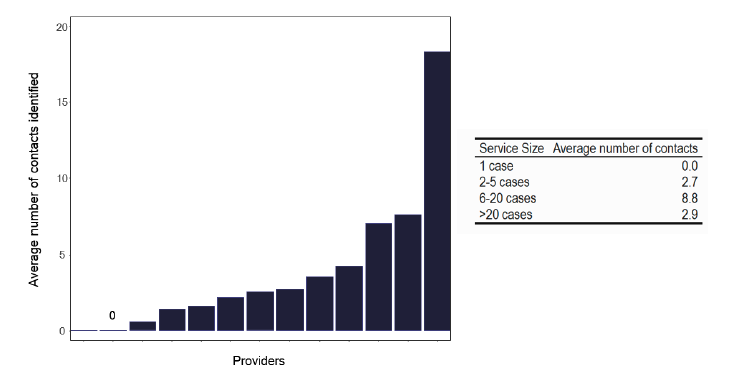
Note: Time period includes notified cases between January 2022 and December 2022. The data source is the Enhanced Surveillance of Mycobacterial Infections (ESMI) system.
Five or more contacts per notification.
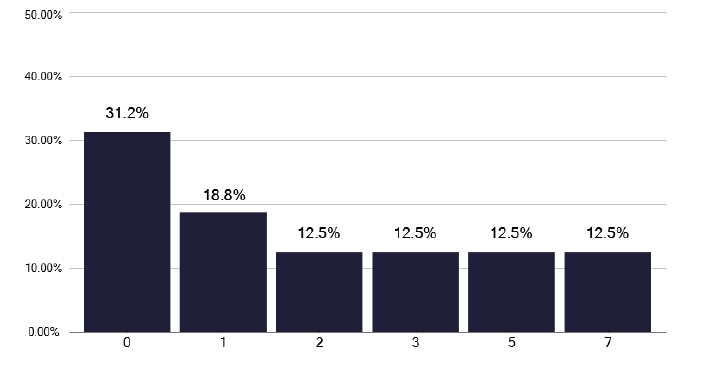
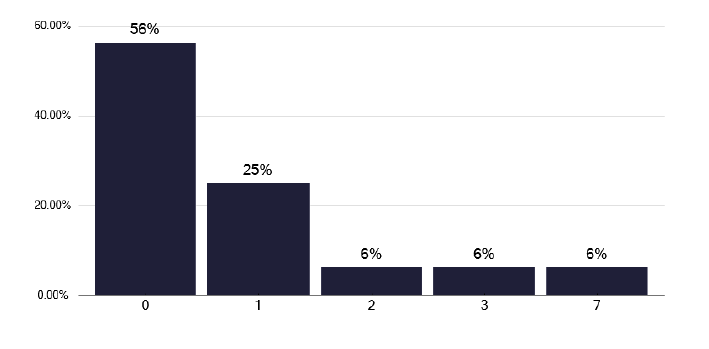
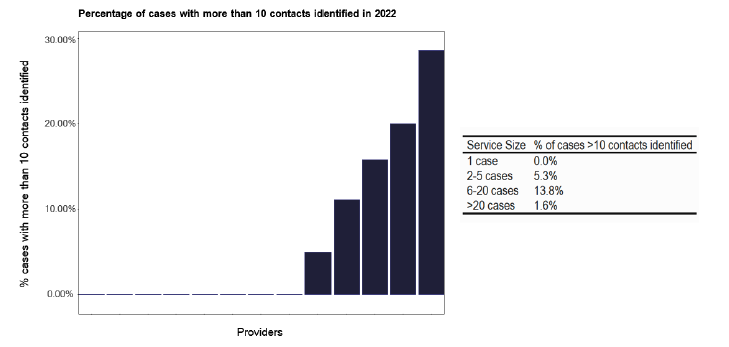
A key recommendation is that more than 5 contacts should be identified for each ‘infective’ index case. The self-reported activity for this, shown in Figure 78, and the ESMI data displayed as a proportion, in Figure 79, shows considerable variation based on the number of notifications. Similar data is displayed for more than 10 contacts per case, as in Figures 80 and 81, and shows smaller numbers, as expected. We explored this data further by looking at greater than 5 contacts per index case for overall notifications, pulmonary notifications and for those with identified smear positive disease (44 out of 201 notifications, 22%). These numbers and the ratios i.e. contacts per case for different services, are shown in Table 3. There is marked variation between services in their contacts for different index cases, but the findings appeared consistent in that those who had high screening ratios for smear positive disease had high screening ratios for ‘all’ notifications. This variation relates to the service, as it is unlikely to be explained by any outbreaks in different settings, as shown in Figures 82 and 83, and therefore merits internal review.
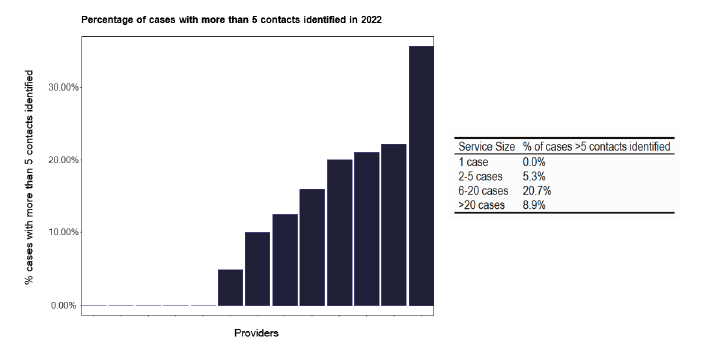
Note: Time period includes notified cases between January 2022 and December 2022. The data source is the Enhanced Surveillance of Mycobacterial Infections (ESMI) system
Note: Time period includes notified cases between January 2022 and December 2022. The data source is the Enhanced Surveillance of Mycobacterial Infections (ESMI) system
| TB services | Notifications (ESMI) | Total Contacts Identified | Total Contacts Screened | Average contacts per notification | Average number of contacts per case (self-reported from survey) | Number of pulmonary notifications (ESMI) | Average contacts per pulmonary notification | Total number of cases with sputum smear positive | Average contacts per smear positive notification | Total number of cases without a sputum test | Number of LTBI cases (self- reported from survey) | Total Number of LTBI Patients Screened (from Survey Submissions) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Grampian | 19 | 348 | 251 | 18.3 | 13.0 | 10 | 34.8 | 7 | 49.7 | 9 | 169 | 2170 |
| Ayrshire & Arran | 5 | 7 | 6 | 1.4 | 1.8 | 3 | 2.3 | 3 | 2.3 | 2 | 2 | 98 |
| Dumfries | 2 | 0 | 0 | 0.0 | 4.0 | 2 | 0.0 | 1 | 0.0 | 0 | 4 | 503 |
| Lothian | 40 | 170 | 149 | 4.3 | 2.4 | 21 | 8.1 | 8 | 21.3 | 17 | 2 | 5596 |
| Forth Valley | 8 | 22 | 11 | 2.8 | 2.0 | 4 | 5.5 | 2 | 11.0 | 5 | 2 | 193 |
| GGC North | 25 | 64 | 61 | 2.6 | 2.0 | 13 | 4.9 | 5 | 12.8 | 13 | 2 | 48 |
| GGC Clyde | 8 | 13 | 13 | 1.6 | 1.9 | 6 | 2.2 | 2 | 6.5 | 3 | 2 | 34 |
| GGC South | 60 | 132 | 97 | 2.2 | 4.0 | 21 | 6.3 | 8 | 16.5 | 39 | 4 | 132 |
| Lanarkshire | 14 | 98 | 87 | 7.0 | 2.5 | 9 | 10.9 | 5 | 19.6 | 3 | 3 | 59 |
| Tayside | 9 | 32 | 27 | 3.6 | 3.0 | 4 | 8.0 | 3 | 10.7 | 6 | 3 | 285 |
| Highlands | 5 | 38 | 26 | 7.6 | 8.0 | 4 | 9.5 | 1 | 38.0 | 2 | 8 | 21 |
| Fife | 6 | 3 | 3 | 0.6 | 6.0 | 3 | 1.0 | 0 | 0.0 | 5 | 6 | 0 |
| Borders | * | * | * | * | 50 | * | * | * | * | * | NA | NA |
| Orkney | * | * | * | * | 0 | * | * | * | * | * | 0 | 0 |
| Western Isles | * | * | * | * | 0 | * | * | * | * | * | 0 | 0 |
| Shetland | * | * | * | * | 0 | * | * | * | * | * | 0 | 3 |
| * No 2022 ESMI data | ||||||||||||
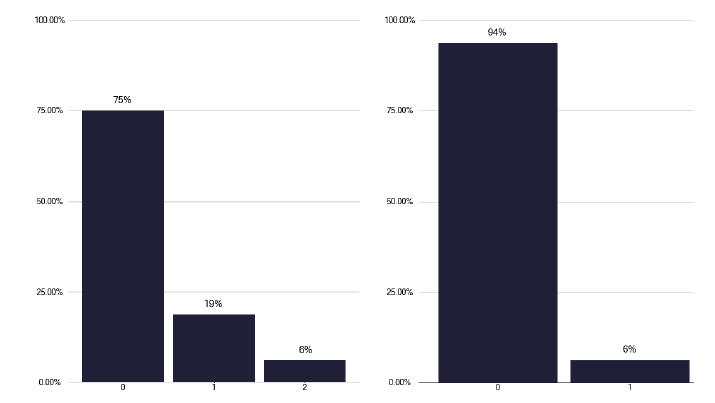
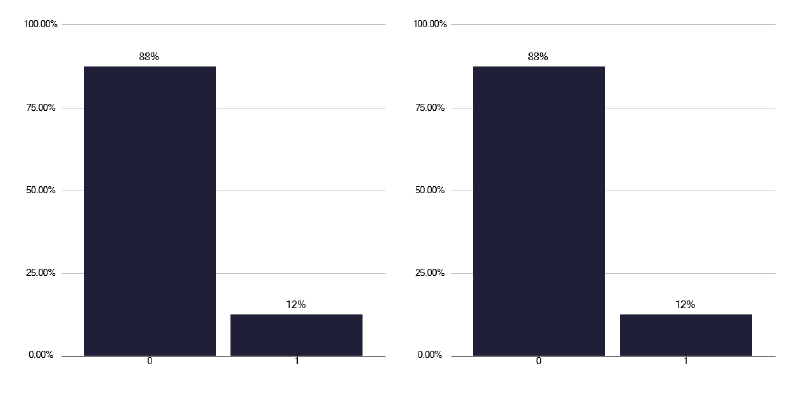
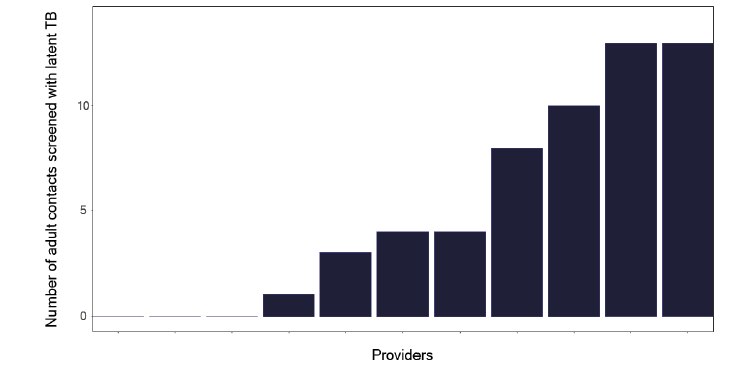
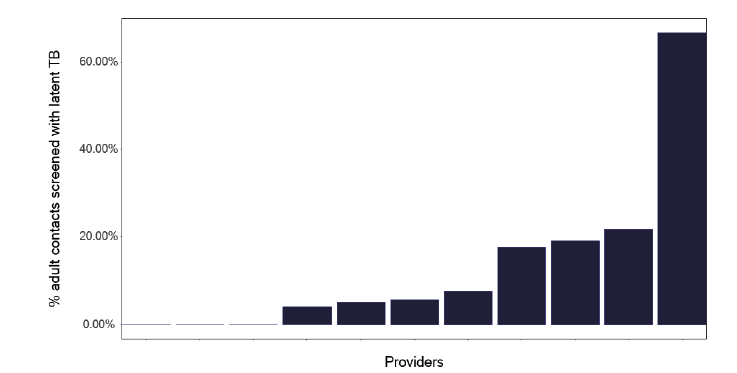
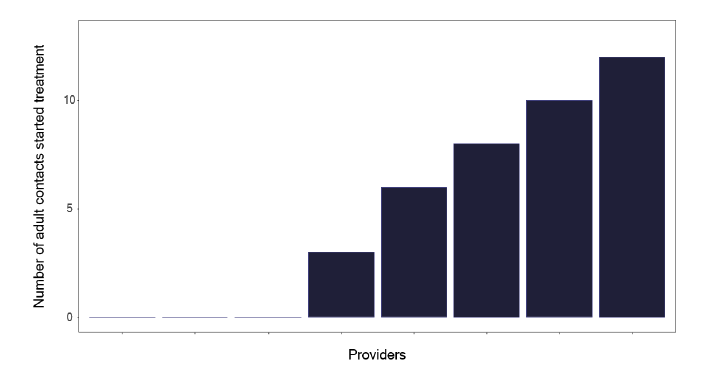
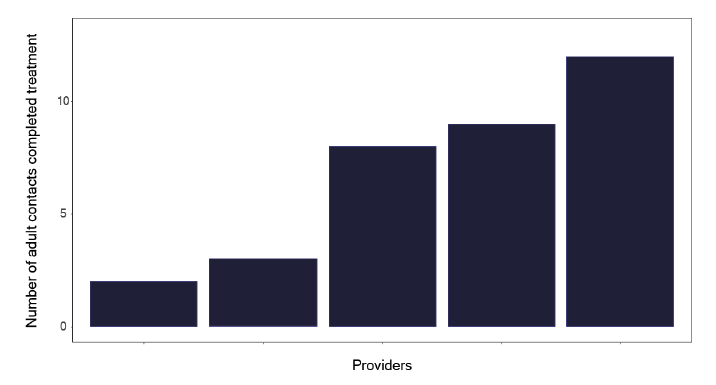
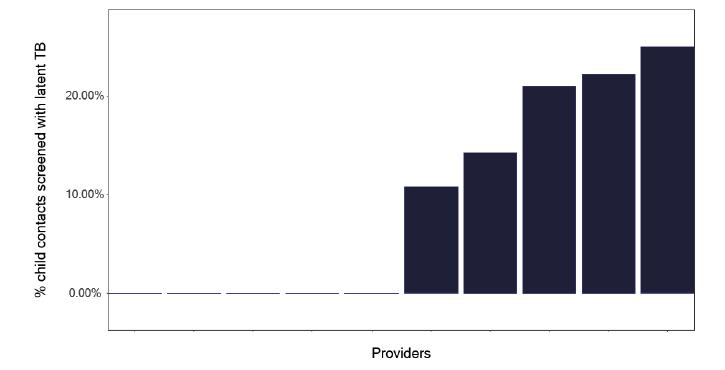
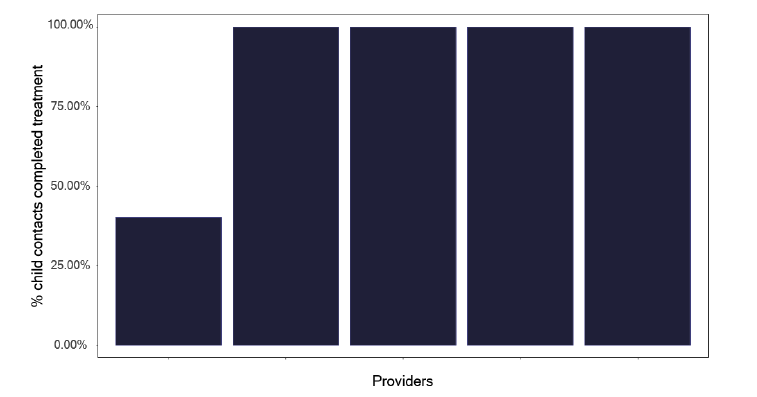
If we explore the results of contact tracing, we find that the number of individuals who are eligible for screening and who attend, as shown in Figure 84, is very variable, with one service having only half of those identified who merit screening, attending. This should be explored within each service to see what is needed to improve attendance rates. Figure 85 shows the number and Figure 86, the proportion of contacts screened who had latent TB, yet a smaller number started treatment as in Figure 87 and even fewer completed treatment as per Figure 88. Services should know this variation and explore why individuals who had latent TB did not start or complete treatment. The initiation and completion of treatment in children appears better than the adult population, as shown in Figures 89 and 90. Discussions at cohort reviews should occur in each service to identify if there is systematic variation in practice.
Note: Time period includes notified cases between January 2022 and December 2022. The data source is the Enhanced Surveillance of Mycobacterial Infections (ESMI) system.
Note: Time period includes notified cases between January 2022 and December 2022. The data source is the Enhanced Surveillance of Mycobacterial Infections (ESMI) system.
Note: Time period includes notified cases between January 2022 and December 2022. The data source is the Enhanced Surveillance of Mycobacterial Infections (ESMI) system.
Note: Time period includes notified cases between January 2022 and December 2022. The data source is the Enhanced Surveillance of Mycobacterial Infections (ESMI) system.
Note: Time period includes notified cases between January 2022 and December 2022. The data source is the Enhanced Surveillance of Mycobacterial Infections (ESMI) system.
Note: Time period includes notified cases between January 2022 and December 2022. The data source is the Enhanced Surveillance of Mycobacterial Infections (ESMI) system.
Recommendations: Contact Tracing
56. There is an element of inconsistency regarding who is screened in pulmonary and extra-pulmonary disease, which reflects a lack of current guidance. A standardised approach, based on best practice, may be helpful in maximising the use of resources.
P, N
57. Services should look to identify 5 or more contacts per index case with active disease, which most services appear to be doing already. However, there is wide variation in the number of individuals screened, which merits a review by the service and a discussion during cohort reviews.
P, HB
58. The reasons for variation in self-reported attendance of individuals for screening needs to be explored by each service. To address low attendance rates. Services should seek to learn from colleagues who have better attendances.
P, HB
59. Services should explore why there is variation between the identification of individuals who should start preventative treatment, and those who appear not to do so, or fail to complete treatment. Some of this may relate to contact tracing procedures and support during therapy, as noted previously. Cohort reviews have a role here.
P, HB
11.2 Bacillus Calmette-Guerin (BCG)
Administration of Bacillus Calmette-Guerin (BCG) is effective at reducing the risk of developing tuberculosis in individuals who are exposed to mycobacteria tuberculosis. BCG is deployed in three broad areas: to prevent tuberculosis in high-risk groups after birth (the neonatal BCG programme), as part of a management strategy in contact tracing and to give protection for individuals travelling to high prevalent areas of tuberculosis.
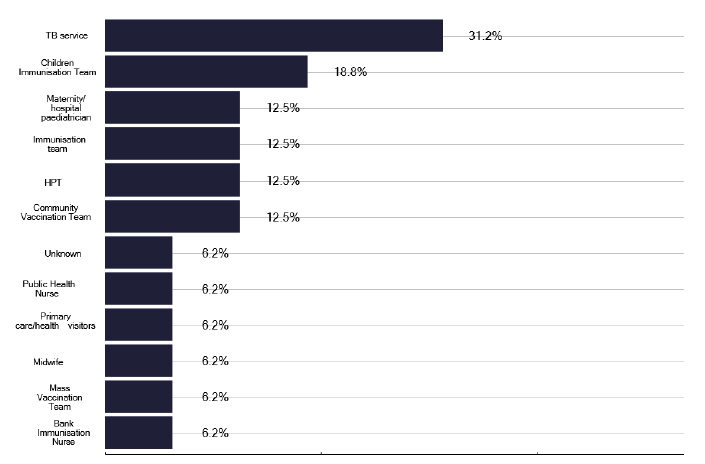
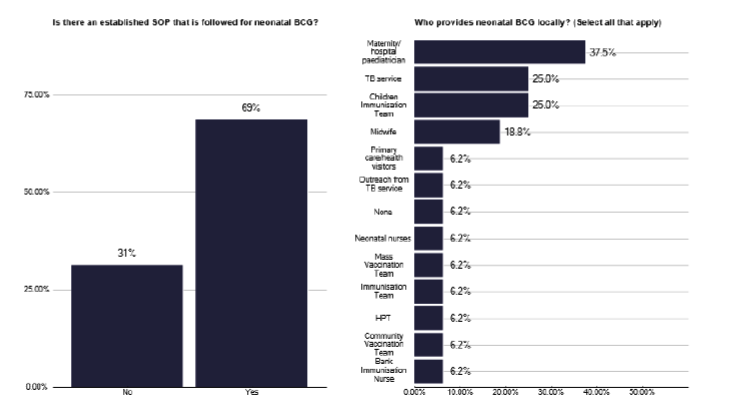
We explored who was administering BCG to the general eligible population (non neonates) and found several providers, as shown in Figure 91, with services having multiple options, creating a significant workload for TB nursing staff. In the neonatal program where BCG is given to individuals who are at risk of being exposed to TB (e.g. parents and grandparents from high prevalence countries), we found marked variability in service provision, with 69% of services having a well-established standard operating procedure, as shown in Figure 92. For each TB service there were often multiple answers to who administers BCG, so a site-specific review is needed, but again their seemed a significant burden on TB nursing staff.
Whatever model is used, and it does need to vary given the geography of Scotland, the deep dives confirmed it was generally an efficient process. In urban areas we noted that TB nurses would recall children into a clinic for BCG and this had good attendance, and a similar model occurred in a very rural area which served a predominately UK born population. However, we also found excellent administration of BCG on maternity units, which seems valid in busy maternity units where staff are trained and in sufficient number to ensure a high vaccination rate. See the example of a good protocol in the good practice via the link in Annex E.
Note: total percentage of responses can be over 100% as multiple options can be selected for this question.
Note: total percentage of responses can be over 100% as multiple options can be selected for this question
Recommendations: BCG
60. BCG vaccination for neonates is an effective way of reducing the risk of developing TB, so a model that works for each service provider and Health Board is essential. With the potential for more babies to receive BCG, due to the evolving population, sufficient infrastructure needs to be in place. Health Boards need to keep the workload and delivery model under review.
P, HB
11.3 Occupational Health Screening
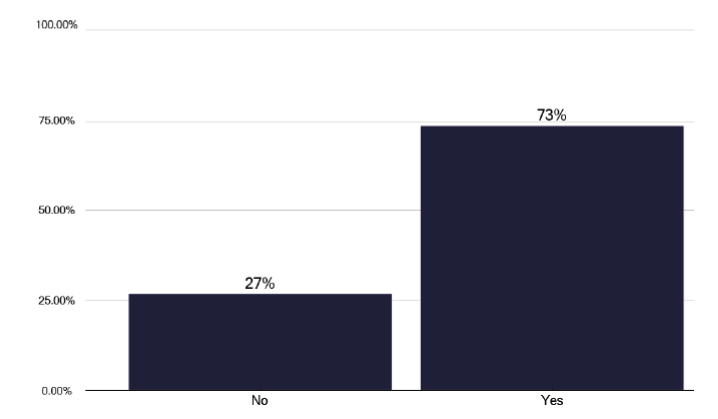
We asked about screening for newly recruited staff for TB. As shown in Figure 93, we found that 73% of providers have a policy for international healthcare workers and of the 27% who do not, the deep dives suggested the policy sat with occupational health. We asked about the volume of work and all colleagues stated that this is significant and increasing. However, when we asked for specific figures on the amount of occupational health screening, we obtained quite marked variation in the activity as shown in graph 100 in the data pack in Annex E).
Some of this may relate to data capture, i.e. the number of individuals with positive IGRAs that the service treated, the size of the organisation and the uncertainty of how many IGRAs had been requested by the occupational health service and were negative.
We were fortunate, during one of the deep dives, to be joined by an occupational health physician who had accurate data outlining the activity. For the year of 2024, 157 IGRAS were performed as part of the screening, of which 41 were positive (29%) and required preventative treatment. This workload related to increased numbers of staff being recruited not from the EU, as previously, but from high prevalence areas of the world, specifically Nigeria, Uganda and Kenya. Individuals on preventative therapy were risk assessed for both their infectivity and for the population they would be caring for, to ensure they were in gainful employment while on preventative therapy. Given these continued recruitment patterns, it seems there will be a continued significant volume of work for both occupational health and TB services.
Concern was expressed during several deep dives that the processes for healthcare workers were robust but not for those employed in social care environments. Figure 94 shows what other populations were screened for TB and that only 13% of staff working in care homes were screened, despite the potential vulnerable population they are looking after. This was highlighted during one of our deep dives when an individual who had been recruited from abroad to work in a care home and had not undergone any occupational health screening was found to have active TB.
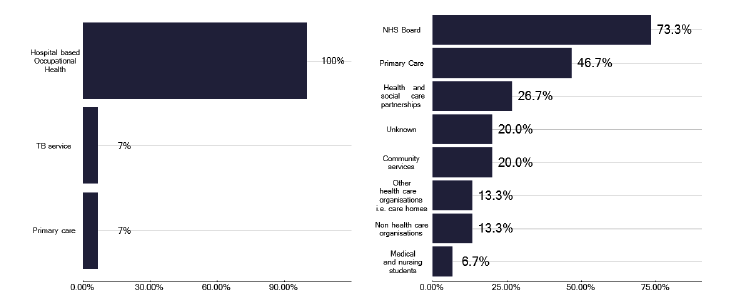
Note: total percentage of responses can be over 100% as multiple options can be selected for both questions.
Recommendations: Occupational health screening
61. A robust screening process needs to be in place due to staff from high prevalence areas being recruited into delivering health care.
P, HB
62. There appears to be an increasing volume of work for occupational health services, for pathology services who perform the IGRA, and for TB services involved in delivering preventative therapies. This activity should be reviewed by Health Boards to ensure there is sufficient capacity to deliver a prompt service.
P, HB
63. Consideration needs to be given to screening for TB in other workers involved in health care beyond acute providers’ e.g. social care.
P, HB
11.4 Screening for biological therapies
With the marked increase in the availability and variety of biological therapies for a wide range of diseases, most specialist societies have produced documentation about processes for screening for TB before commencing treatment. Most of these protocols involve an IGRA test, though skin testing and chest X-ray are still considered. This reflects a significant increasing workload for TB services, and for pathology departments, who are undertaking the IGRA test which does not appear, from our deep dives, to be paid for by the specialist service.
Positive IGRAs are normally referred into the service but we heard excellent examples, as documented in the good practice via the link in Annex E, where all results or results for positive IGRAs were referred from pathology to the lead clinician as a failsafe practice that should be more widely adopted.
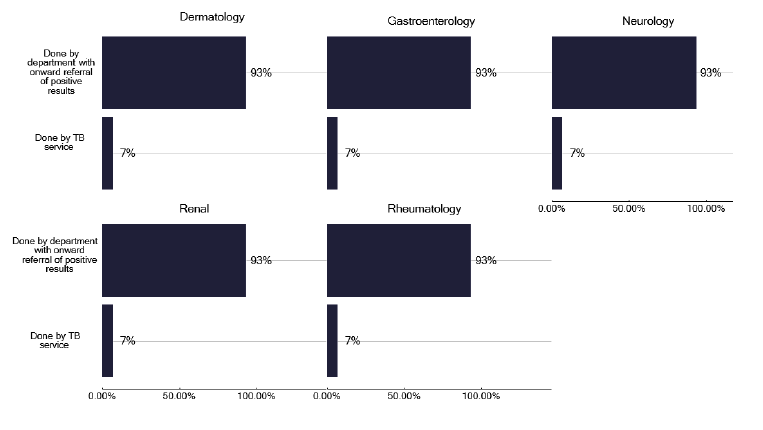
As shown in Figure 95, the majority of TB services are only seeing those with a positive IGRA. We did, however, identify one specialist service in a provider that was referring all patients for consideration of a biological therapy into the TB service. This produced a considerable workload for the TB service which was not funded and had limited capacity to undertake other TB activities. Where such specialist services are requesting a formal evaluation by the TB service there should be clear cross charging.
Additionally, the pathology department needs some reimbursement for the IGRA testing, which is a considerable burden. Although we asked for information on the number of IGRA tests done, this was often not possible to determine generally, and certainly not specific biological therapies. While we did tabulate the activity in both IGRAs and individuals for receiving preventative therapy, this is inaccurate, because in many instances the number of IGRAs performed and the reason was unclear. One service was able to produce clear documentation which confirmed the huge workload, with over 4000 IGRAs performed, many of which were for biological therapies see graph 100 in the data pack in Annex E).
Recommendations: Screening for biological therapies
64. There should be discussion between pathology departments and specialist services regarding the increasing cost burden of IGRA tests (As in the diagnostics section 8.3,) so this is managed appropriately within the Board/service.
P
65. TB services and pathology departments should be aware of the volume of requests for IGRA before biological therapies and to ensure current guidelines are followed, for example, that there are not unnecessary repeat tests requested.
P
11.5 Preventative therapies: Migrants and asylum seekers
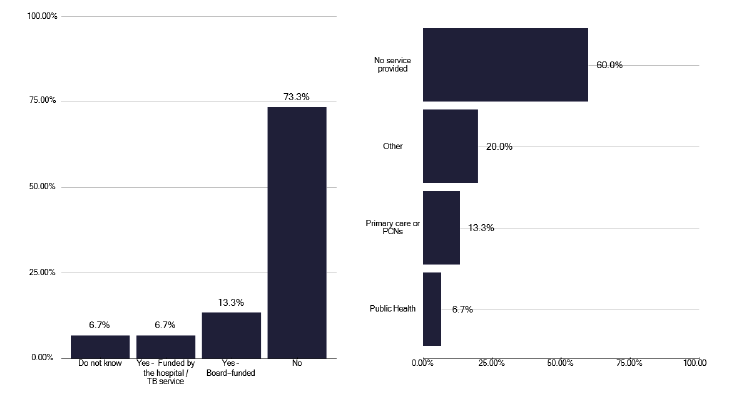
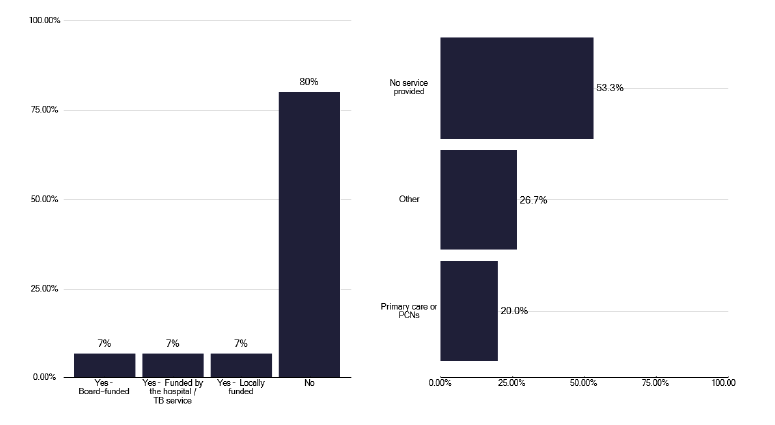
There is no national Scottish commissioned service for preventative therapy for asylum seekers and migrants, as shown in Figures 96 and 97 respectively. However, we did hear during deep dives of several services attempting to address this issue in the absence of any central funding.
These populations are very different and include unaccompanied children, relocated individuals and asylum seekers. Services had developed different unfunded models to support such individuals, which were affected by service geography and the location of the populations. We identified several smaller services that had taken a holistic approach, as detailed in good practice in Annex E. This included screening for TB and blood born viruses together and addressing mental health issues etc. with asylum seekers in their hostel. Another service had a similar model but also included a ‘safety net’ to ensure these individuals were not lost in the system.
An area of some concern from two of the deep dives was unaccompanied children. These services had attempted to review these children, who are often over 18 years old when formally assessed. Whilst the numbers are small, in one service we found approximately 18% of these unaccompanied children required preventative therapy while in the other service, which has a much smaller number, it was approximately 15%. This is a concern for the potential breakdown and development of tuberculosis in a young and mobile group which risks infecting others. It would seem appropriate for this population to be specifically targeted in any preventative therapy strategy.
Contact
Email: healthprotection@gov.scot