Peer support in perinatal mental health: evidence review
This internship project report reviews the evidence base for peer support in perinatal mental health, considering evidence of effectiveness, models of support currently in place and potential ways of further developing peer support in Scotland.
4. Key findings
4.1 What evidence is there on the effectiveness of peer support in the perinatal period?
Evidence from the literature and responses from stakeholders demonstrate the benefits of a range of peer support models.
- Quantitative evidence shows that peer support can significantly reduce depressive symptoms for women experiencing postnatal depression.
- Qualitative evidence makes it clear that women experience improved self-efficacy, self-esteem and parenting confidence through peer support.
- Peer support directly reduces social isolation and can increase social activities outside the home for women experiencing perinatal mental health difficulties.
- There is also evidence that peer support can act as a bridge to build trust with clinical services.
A leading scholar in the field, Cindy-Lee Dennis (2009) summarises three ways peer support can be effective:
a) Direct effect, where the peer support fulfils basic social needs or links clients with services that can meet those needs
b) Buffering effect, where peer support helps protect clients from direct stress by bolstering coping mechanisms through additional resource
c) Mediating effect, where peer support helps improve areas which have a protective effect for clients against direct stress.
To give an example of the mediating effect of perinatal peer support, Dennis suggests that support from peer volunteers may improve self-efficacy and social integration for women, enhancing their resilience to perinatal mental health difficulties (Dennis et al., 2009). Reviewing the evidence base on psychosocial interventions to treat perinatal depression, Dennis argues that there is the potential for peer support interventions to have beneficial effects for women with mild to moderate postnatal depression (Dennis, 2014). This is in the context of extensive research showing that 'a lack of social support is a significant predictor of postpartum depression.' (Dennis 2014).
What are the most effective forms of peer support?
It is clear that peer support in the form of peer workers, peer befrienders, peer groups or informal and online support, can be highly effective in supporting parents with perinatal mental health difficulties. Research evidence suggests that peer support:
- Builds parenting confidence and improves parenting self-efficacy for mothers/carers
- Reduces social isolation for mothers/carers and encourages them to form further social bonds
- Builds links between parent and other services, helping to develop trusting relationships
- Can reduce depressive symptoms as measured by the Edinburgh Postnatal Depression Scale
- Can be highly rewarding for both peer supporter and mother/carer when safe and appropriate
Research suggests that rather than one model of peer support being the most effective, different models of peer support serve different functions:
- Individualised peer support can be especially helpful for women who feel unable to take part in activities outside the home or who experience stigma or self-stigma, as they are not required to share with a group. It also seems to be helpful for women from disadvantaged backgrounds who are less likely to attend groups regularly.
- Group support is helpful in reducing isolation and forming more social bonds, for women who feel able to attend. Group support seems to help normalise the experience of mental health difficulties in the perinatal period and reduce stigma. Some studies suggest that women who are from less disadvantaged backgrounds are more likely to regularly attend peer support groups.
- Telephone-based or online support seems to be especially useful for women who may find it hard to access other forms of peer support, due to geographical isolation, lack of other peer support options or other restrictions. The benefits of this kind of support seem to be flexibility, accessibility and autonomy for women with how they engage with support.
What does the evidence tell us about potential challenges and barriers?
The evidence indicates a number of potential challenges in the provision of perinatal peer support, which are summarised below.
Appropriate referrals
Peer support is suitable for women with mild to moderate mental health difficulties and can help prevent the worsening of their symptoms. Inappropriate referrals may occur due to a lack of other perinatal mental health support, leading to women being referred or self-referring into peer support services who require more intensive support.
Peer support is not a substitute for appropriate clinical treatment for severe perinatal mental illness, although it can provide complementary support. Severe perinatal mental illness requires more intensive, professional support or referral to formal counselling or psychological supports. Ensuring clarity in service provision and sharing referral criteria for peer support widely could help to ensure referrals are appropriate and safe (Heywood et al., 2016).
Preparation and supervision
Training and supervision for peer workers (whether paid or voluntary) is important. Insufficient training can mean that practice is variable in quality and may be ineffective or unhelpful. In rare cases this may lead to practice being harmful rather than helpful, for example, mothers feeling that their problems were being 'minimised' when the peer workers were simply trying to normalise the experiences the women were going through. Insufficient supervision can lead to similar issues with quality and reliability of support, and also may leave peer workers vulnerable to burnout or re-traumatisation.
Ensuring that the wider staff team are ready to work alongside peer support workers is also important. Conflict between the expectations of peer staff and non-peer staff can make it difficult for peer workers to integrate into the team. If existing staff do not have a recovery focus, or have not been trained and supported to embrace peer working, it is possible that peer workers might not be welcomed.
Clear role boundaries
Role conflicts and confusion about who is doing what and why can make it difficult for clinical staff and peers to work together. Clear job descriptions and proactive steps to integrate peers into the wider staff team can help to mitigate this difficulty.
Evidence suggests that women prefer to receive advice or training from professional clinical staff, and that when peers are asked to provide training to mothers this can be less effective. Letourneau et al (2011) found that when peer volunteers delivered a maternal–infant interaction intervention, this was not well received by the mothers and would have been better delivered by clinical staff. This is reflected in the Perinatal Peer Support Principles, suggesting that peer work is highly valued as distinct from the work of clinical staff.
Accessibility of services
In the course of researching this report, several barriers to accessing peer support were identified which may prevent parents from getting the help they need:
- Minority ethnic groups experience additional difficulties in accessing peer support, including language difficulties, and cultural and religious beliefs which may stigmatise seeking support for mental health difficulties. A Home-Start evaluation in north Glasgow identified language and cultural barriers as a key difficulty in supporting mothers (Heywood et al., 2016).
- Rural isolation, transport difficulties and a lack of local infrastructure can make it difficult for some women to access peer support, especially outside of the central belt of Scotland.
- Disabilities or health problems may make accessing peer support difficult, either through lack of accessible peer support or through stigma or discrimination.
- Fathers or partners are likely to experience the absence of peer support, with many perinatal peer support services only available for mothers. It is also likely that fathers and partners may experience additional stigmatisation in relation to perinatal mental health difficulties and this may mean they are less likely to seek support.
- Socioeconomic disadvantage is likely to prevent families from accessing peer support services which require any additional cost, such as the cost of transport to attend support groups, or paying for childcare to attend a group.
4.2 What models of perinatal peer support can be identified in Scotland?
This report identified 53 organisations in Scotland who provide peer support for parents in the perinatal period. These included paid peer workers (the smallest number), volunteer befrienders, peer support groups, and online and email peer support. These organisations are overwhelmingly based in the central belt of Scotland, suggesting less provision for women living in rural or remote areas.
4.3 What evaluation evidence exists on the effectiveness of current models of peer support in Scotland?
Very limited evidence exists to evaluate the efficacy of perinatal peer support models in Scotland. Nurture the Borders use pre and post measures to evaluate their service, which includes paid peer work, however current numbers are still quite low (Nurture the Borders 2019). Aberlour, Home-Start and Nurture the Borders have conducted their own evaluations of their volunteer perinatal peer support. These evaluations have returned positive feedback on the services, however the sample sizes are too low in these studies to offer robust evidence on the efficacy of the support services. Quarriers evaluated their perinatal peer-support groups, however experienced very low response rates. Several of these evaluations were conducted with external academic partners, and show strong commitment to robust evaluation by the services involved. However, limited numbers, limited resources and low response rates among clients are currently curtailing the extent of evaluation activity in perinatal peer support in Scotland.
Cost effectiveness
Overall, there is a lack of data to evaluate if peer support offers a cost saving overall by supporting women and families and diverting them from requiring more intensive support later. This review found two examples from Scotland of economic evaluations of perinatal peer support. An evaluation of a Home-Start trial, providing specialist perinatal support in North East Glasgow found that: "The peer support model is a cost effective way of supporting vulnerable and marginalised mothers and their families in the perinatal period" (Heywood et al., 2016). A realist evaluation of Aberlour's Perinatal Befriending Service in Forth Valley and East Lothian suggested that the service could have economic benefits by preventing the need for more intensive support at a later point, but that the data gathered was not sufficient to provide evidence of potential cost-savings.
4.4 Potential resources for developing perinatal peer support in Scotland.
This review has identified a number of resources that could be useful when developing perinatal mental health peer support in Scotland.
Case study examples
- The Greater Glasgow and Clyde Perinatal Mental Health Network (PMHN) is an informal network of NHS, Local Authority and Third-Sector organisations supporting parents' and infants' mental health in the perinatal period. It is an innovative approach to promoting awareness and access to perinatal mental health services, and an example of facilitating good relationships between clinical services and the third sector. Further information is given in Annex 2.
- The Mother and Baby Unit at Devon Partnership NHS Trust is another innovative approach that could act as a model for promoting peer support in perinatal mental health in Scotland. Further information is available at Annex 3.
- The case studies were developed through interviews with staff and reviewing key documents (e.g. job descriptions). It should be noted the case studies are descriptive but not evaluative, so they do not provide any indication of the quality of the service.
Job roles and descriptions
- Exemplars from peer support services in the rest of the UK – for instance, the perinatal peer support worker job description from the Mother and Baby Unit at Devon Partnership NHS Trust – could be a helpful resource for developing job descriptions for NHS Scotland.
- ImROC Guides to Peer Recruitment and working with/supporting peer workers (Repper et al., 2013) have already been used with success in introducing peer work in adult acute mental health wards in the West of Scotland. Job descriptions for these peer workers in a general acute mental health setting are helpful in defining the peer worker role.
Evaluation
- The validated Peer Support Evaluation Inventory (Dennis, 2003) is a custom tool to evaluate participants' experience of peer support. Evidence suggests this could be a useful data collection tool in evaluation of peer support, alongside pre and post measures such as the Edinburgh Postnatal Depression Scale.
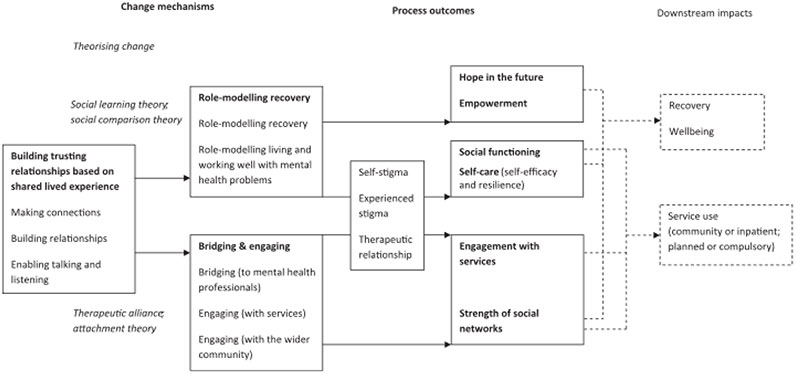
Change model
- The change model developed by Gillard (2014) offers an excellent overview of the processes and outcomes when incorporating peer work into existing NHS or third sector services. Figure 1 below illustrates the resources, mechanisms of change and process outcomes making up peer work interventions. The model reflects the evidence base detailed in the literature review and is a useful distillation of a complex intervention.
Contact
Email: socialresearch@gov.scot