Our Path Ahead: Chief Medical Officer for Scotland Annual Report 2025–2026
This report frames our path ahead for Scotland’s health and care: supporting careful and kind care, responding to disruption and creating the conditions for health. By designing systems around people, we can achieve a more humane, sustainable and fair system focused on the outcomes that matter.
Chapter 3: Creating the Conditions
Health is shaped beyond the walls of clinics and hospitals. The circumstances in which we grow, learn, work and age remain the strongest determinants of wellbeing. To improve population health, reduce inequalities in health outcomes and ensure long-term sustainability of our universal system of healthcare, we must shift focus from reacting to illness toward building the social, economic and environmental foundations that keep people well. Put simply, we must move from a repair shop mentality to one of pro-active, preventative societal interventions.
Creating a sustainable approach to healthcare requires us to balance biology with biography- delivering careful and kind care grounded in evidence, while recognising how people’s life circumstances shape health, risk and resilience. Connection with those we care for must remain at the heart of reform, alongside sustained action on the upstream conditions that determine health.
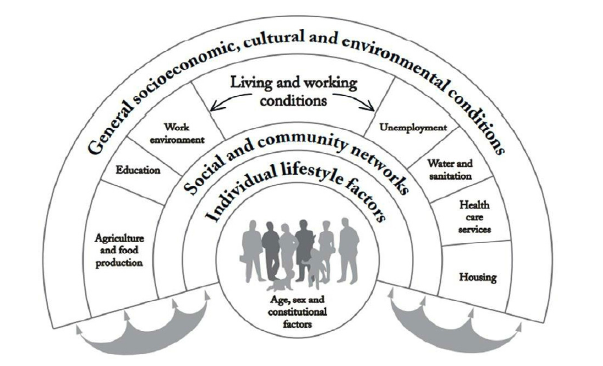
Source: Dahlgren, Whitehead 1993
Improving health means addressing its social, economic and commercial determinants. Professionally, this calls for the practice of Realistic Medicine: understanding what matters to people, sharing decision-making and ensuring our care respects the time, energy and attention of those we support. Our duty does not stop at treatment. We must understand the upstream drivers of poor health and do what we can, individually and collectively, to address them.
This chapter sets out how we can strengthen these foundations: by prioritising prevention; building a wellbeing economy; supporting children and young people; reducing financial insecurity; and creating healthier places to live, learn and work. It reflects a clear reality: the conditions we have created are not working equally well for everyone, as seen in the persistent inequalities across Scotland today. Responding to this requires looking beyond health and care alone and working with partners such as workplaces, schools and cultural organisations as active contributors to health creation. Improving population health and reducing inequalities will depend on acting earlier, working across boundaries and sustained collective effort.
Shifting to Prevention
Globally, health spending is outpacing both GDP growth and general inflation, increasing the share of national income devoted to healthcare. The rising burden of disease and demographic changes including population ageing mean demand and costs will continue to rise unless we shift course. Health and care spending is projected to rise from around 40 per cent of devolved public spending in 2029-30 to almost 55 per cent in 2074-75. When health and care spending expands, it impacts our ability to invest in other public services- early years, education, housing, employment support- that keep people healthy in the first place. Sustainability requires strengthening these wider determinants. Addressing rising pressures and complexity requires a deliberate shift towards targeted prevention, acting earlier to reduce avoidable illness.
Scotland has taken important steps toward public service reform with the Health and Social Care Renewal Framework (SRF) and the Population Health Framework (PHF) which provides an evidence-based focus on improving health and reducing inequality by strengthening the building blocks of health. The PHF reinforces a life course approach and the importance of prevention at every stage.
Prevention is central to a sustainable system. It remains one of the most cost-effective ways to improve population health and reduce inequalities. Primary prevention is 3-4 times more cost-effective than investing in treatment. The median return on investment (ROI) for £1 invested was £34 for health protection (e.g. vaccines and immunisation) and £46 for legislative interventions. Maintaining focus on primary, secondary and tertiary prevention is essential for long-term sustainability.
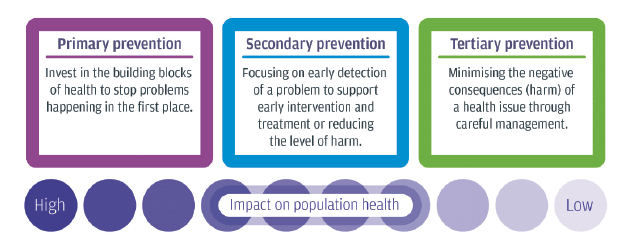
Primary prevention
Invest in the building blocks of health to stop problems happening in the first place.
Secondary prevention
Focusing on early detection of a problem to support early intervention and treatment or reducing the level of harm.
Tertiary prevention
Minimising the negative consequences (harm) of a health issue through careful management.
The call for focus on prevention is not new. The 2011 Christie Commission highlighted, ‘A cycle of deprivation and low aspiration has been allowed to persist because preventative measures have not been prioritised… as much as 40 per cent of all spending on public services is accounted for by interventions that could have been avoided by prioritising a preventative approach.’ Scotland has shown what is possible through successful preventative approaches from vaccination programmes to smoke-free legislation. We must continue to close the implementation gap.

A powerful example of preventative intervention is the school-based HPV vaccination programme. This was introduced for girls in 2008 and, from 2019, extended to include boys, helping to further protect against high-risk HPV types which may develop into cancer later in life. This has been highly successful in Scotland; a recent study found no cases of invasive cancer recorded in women immunised at 12 or 13 years of age. Yet we also see stark inequalities: women in more deprived communities are more likely to be diagnosed with cervical cancer at a later stage, and elimination will happen later, too. Building on the success of the programme must include ensuring equitable access and uptake.
Despite strong evidence, prevention can be difficult to fund because its benefits are often invisible; they show up as the absence of illness, while the pressures and costs of unmet need in acute care are felt immediately. Budget tagging work now underway in Scotland may help by allowing preventative spend to be tracked across accountable organisations and its impact more clearly understood.
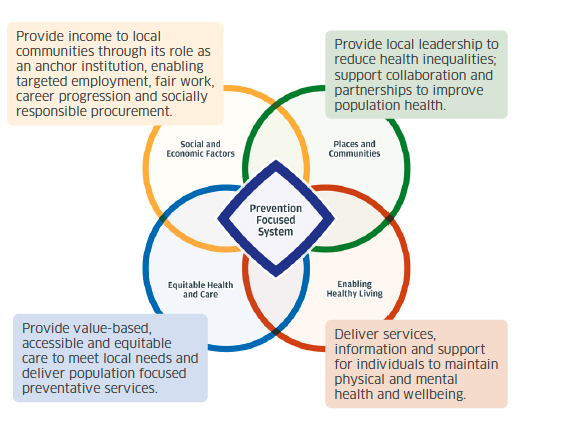
Prevention Focused System
Social and Economic Factors
Provide income to local communities through its rolse as an anchor institution, enabling targeted employment, fair work, career progression and socially responsible procurement.
Places and Communities
Provide local leadership to reduce health inequalities; support collaboration and partnerships to improve population health.
Equitable Health and Care
Provide value-based,accessible and equitable care to meet local needs and deliver population focused preventative services.
Enabling Healthy Living
Delivering services, information and support for individuals to maintain physical and mental health and wellbeing.
Case study: Collaboration for Health Equity in Scotland (CHES)
CHES brings together PHS, NHS Boards and local authorities in Aberdeen City, North Ayrshire and South Lanarkshire, and University College London’s Institute of Health Equity to accelerate action on Scotland’s persistent health inequalities.
The programme embeds health equity into planning and decision-making across councils, NHS boards and community partners, building leadership, supporting proportionate universalism and ensuring policies reflect lived experience.
Place-based work includes strengthening action on wider determinants of health in Aberdeen City through the NIHR funded Health Determinants Research Collaboration; applying health equity principles to play services to better align resources with need; using data in North Ayrshire to inform budgets and policy; and securing £5 million in South Lanarkshire to improve family support through whole system partnership.
Alongside this, CHES has established a national learning system to share insight and support health equity action across Scotland.
To simultaneously deliver effective services for those who need them now while also investing to improve future health is not straightforward. But who better to solve the problems we face than those familiar with them? As health and care professionals, we know the people we serve, we know their challenges and we know our systems. I am continually humbled by the compassion, creativity and dedication of colleagues across health and care. This gives me confidence that, together, we will continue to rise to meet the challenges we face.
Addressing Inequalities
Health inequalities in Scotland remain deep and persistent. While progress has been made in some areas, wide and enduring gaps in health outcomes continue to reflect socioeconomic disadvantage, gender and other social and structural factors. These patterns are not inevitable.
Reducing inequality is central to prevention, population wellbeing and the long-term sustainability of our health and care system. Understanding and responding to these inequalities demands an explicit and sustained equality lens across policies, programmes and services—shaping priorities, resource allocation and delivery from the outset. This includes collecting and using the right data; understanding how decisions affect different groups; recognising how social, economic and environmental conditions influence health at every stage of life; and acting on this insight consistently and with clear accountability.
Deaths from drugs, alcohol and suicide
People in Scotland are generally more likely to die from drugs, alcohol and suicide than in any other country in the UK. Drug deaths rose markedly in recent years with a peak of 1339 deaths in 2020. Although drug mortality rates have reduced slightly since, they remain high, while alcohol and suicide related mortality rates have shown little meaningful improvement.
These deaths are preventable. They are typically shaped by a constellation of pressures including trauma, poverty, educational disadvantage, unemployment, relationship breakdown, homelessness and interactions with the criminal justice system. These harms illustrate how social and economic conditions translate into physical and mental health outcomes over time. Interventions that reduce these pressures earlier and across systems can improve life chances and help prevent premature death.
Age standardised alcohol-specific, drug misuse and probable suicide mortality rates (per 100,000 population)
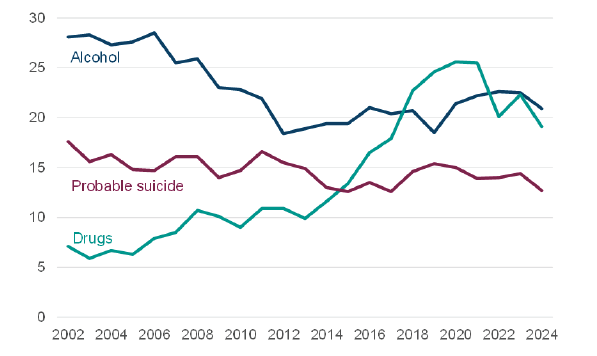
Source: National Records of Scotland, Drug related deaths, Alcohol-specific deaths and Probable suicides in Scotland, 2025
The burden of harm is not evenly distributed. In 2024, 37% of all deaths from drugs, alcohol or suicide occurred among people living in the most deprived 20% of communities. There are also regional differences: drug and alcohol related death rates are higher in urban areas, while suicide rates have been highest in remote small towns for most of the last decade (though in 2024, differences between more urban and more rural areas were not statistically significant).
The issue is most acute for men. In 2024, 69% of those who died from drugs, alcohol and suicide were male, with the highest rates generally seen in men in their forties and fifties. For many, risk accumulates long before contact with health services. Employability services, social security and other touchpoints offer opportunities for earlier identification and support, well before health crisis points are reached.
Preventing Harm, Promoting Recovery sets out a long-term, public health and evidence informed approach to reducing alcohol and drug harms, with renewed emphasis on prevention and early intervention alongside continued support for harm reduction and stronger treatment and care pathways. A parallel commitment is set out in Creating Hope Together, Scotland’s long-term suicide prevention strategy, which focuses on tackling the inequalities associated with suicide. This includes addressing the social circumstances that increase risk. Across this work, including delivery by Suicide Prevention Scotland, principles of time, space and compassion are being embedded across supports in clinical services and communities. Together, these approaches reflect a shared commitment to dignity, respect, compassion and sustained action to prevent avoidable harm.
Racialised health inequalities
Racialised health inequalities persist in Scotland, though they are not consistently reflected in routine health data. Evidence from across the UK shows that racism, discrimination and socioeconomic disadvantage intersect to shape outcomes such as maternal and infant mortality, alongside factors including barriers to timely access to care, experiences of trauma, racism and/or discrimination and language barriers.
Case Study: Amma Birth Companions
In the UK, Black and racially minoritised women and their babies face significantly increased risks during pregnancy and birth. Black women are nearly three times more likely to die during or after pregnancy than white women, with Asian women and women living in the most deprived areas also at elevated risk. These inequalities reflect the impacts of structural racism, socio-economic disadvantage, structural and language barriers.
Amma Birth Companions works with women from asylum-seeking, refugee and migrant communities through pregnancy, birth and early parenthood in Glasgow. To help improve experiences and outcomes, Amma provides trauma-informed, culturally sensitive care through companionship, advocacy and peer support. Amma’s practice is built on safety, trust and each woman’s right to make decisions about her own care.
‘She always waited for me to understand and make my own decision... she didn’t make me feel like she knew it all. I felt like I had power and belonging.’ – Client supported by Amma, speaking about her birth companion.
That proximity to women’s experiences gives Amma a distinctive evidence-base for system-level change. Amma’s 2024 Birth Outcomes and Experiences Report documents the scale of inequity facing the women it supports: with 74% facing communication barriers related to interpreting and over a third experiencing discrimination or poor practice in their maternity care. That evidence is shaping how services are designed and delivered. Amma is co-producing training for midwives and is contributing to national policy on racialised health inequalities.
Scotland’s Maternity care standards place reducing inequalities at their core. National strategies, including the Anti-racism delivery plan 2026-2030 and the Women’s Health Plan, set important direction. However, strategy alone is not sufficient. Progress depends on sustained leadership, consistent implementation and accountability for change at local and national levels. In addressing racialised health inequalities in health and care services, progress is strongest where there is visible, sustained senior and clinical leadership and ownership, supported by robust data and a clear focus on lived experience.
Improving outcomes requires services to be designed and delivered in ways that reflect lived experience, address structural barriers and actively mitigate bias. This includes ensuring relational continuity of care for those at greatest risk, supporting a culturally competent and inclusive workforce and targeting resources in line with need.
Mind the gap: data, insight and action
Differences in health and mortality are consistently associated with exposure to structural racism as well as related socioeconomic factors including education. Yet in Scotland, our understanding of how outcomes vary across these characteristics remains incomplete. Data on social and protected characteristics are not always consistently collected or linked to health records, limiting our ability to fully understand how patterns of illness and death differ between groups and across the life course.
Data linkage offers one important way to strengthen insight by connecting information from different sources, particularly where data are missing or where people may not feel comfortable sharing sensitive information directly. The value of this approach became especially clear during the COVID-19 pandemic, when analysis revealed significant differences in outcomes by ethnic group, including hospitalisation, mortality and vaccine uptake.
PHS is working collaboratively with a range of stakeholders, including anti-racism experts, to address these gaps. While this work progresses, PHS has developed a Race and Ethnicity Index which allows, under strict governance, ethnicity information to be linked to health records where it is not otherwise available. Data produced using the Index was published in Scottish bowel screening uptake statistics by race and ethnicity.
How data are used matters as much as how tools are developed. Anti-racism principles are embedded in both the design and application of the PHS Index to avoid reinforcing bias, stigma or discrimination. While data linkage is not a substitute for improving routine data collection, used responsibly it can support better informed decisions to reduce inequalities and improve outcomes.
The Scottish Government also conducted an audit of ethnicity data, highlighting areas for improvement and actions taken in its Equality Data Improvement Programme (EDIP), as part of Scotland’s Equalities Evidence Strategy (2023-25). A new EDIP audit for 2026 is underway.
From insight to implementation
Persisting health inequalities reflect both what we already know and what we still need to understand better. While gaps remain in data and insight, there is sufficient evidence to act. Progress now depends on sustained, collective action not only across government and public services, but also with partners in sectors such as industry, education and the wider community, with health treated as a shared outcome and a shared responsibility. This means prioritising prevention, targeting resources according to need and accepting that narrowing the gap will require deliberate choices and different ways of working.
The Wellbeing Economy
Health and the economy are inseparable. Our economy shapes the building blocks of health and wellbeing. It influences the availability and affordability of quality housing, education, leisure and social care services, as well as the price and availability of goods and the availability of fair and healthy work across our communities. In Scotland, austerity policies during the 2010s have been identified as one of the principal drivers of changes in mortality rates.
Health determines our ability to learn, work, care and contribute to our communities. When health declines, so too does economic participation, productivity and opportunity. This relationship is bidirectional: financial insecurity and unemployment worsen mental and physical health outcomes.
Good work is good for health. It provides income and can contribute to connection, identity and purpose. But access to good work is not equal. Some have less fairly paid, flexible and good quality work available, and for some people the work available is not accessible because of their health, disabilities or caring responsibilities. This can create a harmful cycle in which ill-health limits access to work, increasing the risk of financial insecurity, which in turn impacts negatively on wellbeing with harmful consequences for people, communities and the wider economy.
This cycle is not inevitable. In Scotland, we are taking preventative action to ensure our economy supports everyone to access the building blocks of health. Current initiatives that promote wellbeing in Scotland via the economy include Fair Work, the Real Living Wage and Community Wealth Building. This approach is reinforced through the Population Health Framework, which includes a commitment to developing a Health and Work Action Plan.
Fair Work offers effective voice, fulfilment, opportunity, respect and security. These foundations create positive practice which benefit both organisations and workers. The Keep Britain Working report reinforces this, highlighting the importance of employer leadership and shared responsibility for health and good work.
Fair Work First encourages employers receiving public funding to adopt these practices, including paying at least the Real Living Wage and ensuring workers have channels to be heard.
The Real Living Wage, based on the cost of living, is paid voluntarily by employers and helps prevent in-work poverty. This matters because over the past 20 years, the proportion of those in relative poverty who belong to working households has increased. Three quarters of children in poverty live in a household where someone works.

Anchor institutions
- Supporting local and regional economies
- Reducing poverty and inequality
- Working collaboratively with local partners
Community wealth building
- Workforce
- Land and assets
- Inclusive ownership
- Spending
- Finance
Wellbeing economy
- An economy that protects the planet and works for people, including future generations, by improving living standards, creating good jobs and purposeful businesses, and building economic resilience
NHS Scotland has major economic influence, employing staff across almost every community and with major spending on goods, services and infrastructure. As an Anchor institution, decisions shape local economies- from recruitment and procurement to how land and buildings are used. By applying community wealth building approaches that ensure wealth is generated, circulated and retained locally and that support sustainable development, we can help strengthen local economies and improve community wellbeing.
NHS Scotland is already embedding these principles. The Community Wealth Building (Scotland) Act 2026 further positions organisations to meet these duties and increase their positive impact on communities and our planet.
Case study: Scran Academy - NHS Lothian as an Anchor Institution
As an Anchor Institution, NHS Lothian wanted to explore catering provision options that could enhance community connections, establish effective local partnerships and offer opportunities for local organisations to utilise space on its sites while generating community wealth. NHS Lothian is working with Scran Academy, a youth-led local social enterprise, to provide a café at the Royal Hospital for Children and Young People, as well as Space @ The Broomhouse Hub at the Princess Alexandra Eye Pavilion and Lauriston Building. The Scran Café opened in July 2025 and averages 200 customers each weekday. In seven months, they have served 10,000 cups of coffee and 5,500 sandwiches. They employ seven young people on the Real Living Wage and are supporting three young people to achieve cooking and food safety qualifications. Scran Academy and Space @ The Broomhouse Hub illustrate how clear strategic Anchors intent can galvanise a complex system to improve services for patients and staff while benefitting our wider community.
Health and care’s role extends beyond our economic impact as Anchor Institutions. Every day, we see the ways financial pressures and insecure work manifest in ill health. Our ability to support people and provide careful and kind care depends on recognising these drivers and responding to them. We do this through compassionate conversations, effective signposting, partnership with local services and practices that protect peoples’ time, energy and resources.
Young People, Health and Economic Participation
In pursuit of a healthier Scotland, we must also reduce the barriers that keep people out of work. Rising economic inactivity due to long-term ill health, particularly among younger people, signals both a public health challenge and a missed economic opportunity.
Since the COVID-19 pandemic, economic inactivity rates (age 16-64) have been increasing across the UK. Much of this upturn appears to be driven by long-term ill health and disability.
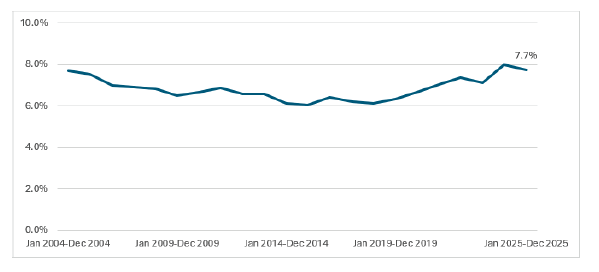
Source: Annual Population Survey, ONS
Across the UK, people in their early twenties are now more likely to be out of work due to ill health than those in their early forties. Between 2020 and 2023, two in five (42%) young people who were out of work because of ill health cited a mental health condition as their main issue. This proportion is rising. Even when not the primary reason, mental health problems frequently co-exist; among young people who are economically inactive due to ill health, 65% had a mental health condition compared with 23% of those in employment and 38% of those unemployed. UK young people who are not university graduates and have a mental health problem are particularly disadvantaged with higher rates of unemployment and low pay than their graduate peers. This highlights the intrinsic links between health, education and work.
Addressing Financial Stress in Practice
We cannot separate people from their context. Money matters- for stability, for opportunity, for health. Poverty, unemployment and financial stress show up every day, shaping symptoms, decisions and outcomes. To care effectively, we must understand the economic pressures faced by the people we serve and work across sectors to ensure people can access support that keeps them well.
Talking about money can be difficult. Health and care professionals are often trusted in moments of vulnerability, which gives us an important opportunity to respond with sensitivity. Early, compassionate conversations can help identify issues sooner, with a positive impact on wellbeing. While health and care professionals are not responsible for delivering welfare or debt advice, we must be aware of the impact of financial stress on health, understand who is at greatest risk and know where to signpost for help.
Case Study: Working Health Services Scotland
Working Health Services Scotland (WHSS) is an NHS service supporting small and medium-sized businesses and self-employed people to address health issues impacting ability to work. The service provides support for physical, mental and social health concerns without requiring a formal diagnosis. NHS case managers coordinate personalised interventions such as physiotherapy, counselling and specialist advice, liaising with GPs and employers where appropriate.
In 2025/26, WHSS received 1641 referrals with 90% engagement. Participants reported average improvements of 41% in anxiety, 46% in depression and 33% in overall health and wellbeing. Nearly 89% reported a positive impact on their health, 95% remained in work following service input and all respondents said they would recommend the service. WHSS is available nationwide with referrals accepted via self-referral, employers, health professionals and partner organisations.
Case Study: Tackling Poverty: Everyone’s Business, NHS Lanarkshire
In 2024/25, the NHS Lanarkshire Health Improvement Tackling Poverty Team delivered 42 ‘Tackling Poverty: Everyone’s Business’ training sessions to 448 NHS Lanarkshire staff, building confidence and skills to discuss financial hardship and refer for financial support. Following the training, referrals to North and South Lanarkshire financial support increased.
Through partnership with South Lanarkshire Council’s Money Matters Advice Service, the team have access to a dedicated Welfare Rights Officer who contributes to training and provides direct support to patients and staff. Over the last year, the service engaged in a range of events and ward visits, leading to 150 interactions offering help including income maximisation, benefit applications, signposting to carers’ organisations and emergency food and fuel support.
Poverty has a profound impact on the health and wellbeing of children and parents, affecting families in every part of Scotland. Strengthening the links between health services and welfare advice, known as income maximisation, is an important action in the PHF and the Child Poverty Delivery Plan. Many services already ask about money matters and connect families with support in their communities. There is scope to strengthen the reach and impact of these approaches further.
Partners in Creating Health
Health is shaped not only in homes and communities, but also through the design, culture and expectations of the institutions that structure everyday life. These settings offer powerful opportunities to embed health promotion.
Health promoting workplaces
Employers have long played a role in shaping population health. Anchor institutions, including NHS Scotland, contribute to local wellbeing through employment, procurement and investment. But there is a broader responsibility. Employers have much to gain from investing in the health of their workers, from improved employee wellbeing and job satisfaction, to a supportive and thriving workplace culture, to strengthened reputation and staff retention.
This is not a new idea. Over two centuries ago, Robert Owen at New Lanark attracted international attention by demonstrating how employer decisions could transform health and opportunity: reducing working hours and providing childcare, education, a doctor and access to allotments.
Today, Scotland’s employers continue to show leadership. Many employers are recognising the value of investing in their workforce, from benefits to workers and families, to productivity, communities and the economy. PHS’ Healthy Working Lives, alongside resources such as the Mentally Flourishing Workplaces Framework, offer practical steps for organisations seeking to improve staff wellbeing.
In health and care, our actions also matter: timely assessment, treatment and support can help people stay in work or return to it, particularly where health affects education, employability or social stability. Beyond healthcare, wider policies that support fair, secure employment have clear health, economic and equity benefits.
Health promoting schools
Education is one of the strongest determinants of future health, employment and wellbeing. Healthy children and young people are better able to engage and achieve in school, while education in turn shapes lifelong health and opportunity. Scotland has long recognised this reciprocal relationship: schools are key partners in creating health, just as health underpins educational attainment. Strengthening health promotion and improving health literacy in schools is therefore vital for long-term sustainability and the shared shift towards prevention.
Since 2007, schools have had a statutory duty to make health promotion a central purpose of education. Health and wellbeing are also core components of the Curriculum for Excellence, providing a solid foundation on which schools build. Maintaining and strengthening health literacy is central to equipping young people with the skills needed to navigate increasingly complex health information and make informed choices as they grow. Alongside these, schools adopt a whole-school approach, recognising health is shaped not only through teaching, but the wider school experience.
Health promoting schools are shaped not by curriculum alone, but by culture, relationships and environment. Young people should feel safe, respected and included, supported by positive relationships, opportunities for physical activity, creativity and play, access to nutritious food and a strong sense of connection and belonging. In this way, schools operate not only as places of learning but as everyday settings that actively support health and wellbeing—much as workplaces can for adults.
Like health services, schools are expected to deliver better outcomes while stewarding finite resources. The challenges facing health and education are interconnected, and so too are the solutions. One example is the statutory duty for local authorities to provide balanced, nutritious and sustainable school meals, supporting children’s health directly and wider sustainability goals. How this duty is realised varies across Scotland, with programmes such as Food for Life demonstrating how some schools are building on this.
Case Study: Food for LIfe Scotland
The Food for Life Scotland programme, delivered by Soil Association Scotland, supports system change in public-sector food by working with caterers to achieve Food for Life Served Here (FFLSH) certification. The standards promote scratch-cooking, reduced reliance on ultra-processed products, seasonality, increased use of vegetables and pulses and connecting diners with where their food comes from.
In 2025, over 100,000 FFLSH certified meals were served daily across Scotland, with 16 local authorities holding Bronze, Silver or Gold certification for their school meals services, alongside 9 other public sector settings, including care homes. The programme supports innovative supply chain approaches, including Argyll and Bute Council’s introduction of locally sourced wild venison onto school menus in Islay and Jura, developed with pupils and local suppliers.
By recognising schools as long-term partners in health promotion, we can keep the focus on practical, place-based solutions that support young people and help build the foundations for their future health, wellbeing and opportunity.
Creativity and Health
Creativity is core to our humanity. For many, art and culture help make life ‘worth living.’ Arts and cultural activities can support the management and prevention of mental and physical health conditions, as well as increase health-promoting behaviours. Emerging research is clarifying how these activities help. One study looking at cultural engagement and depression noted:
‘Cultural engagement…combines a number of protective factors including social interaction, cognitive stimulation and gentle physical activity.’
Much attention and research have rightly been devoted to establishing the case for six pillars of lifestyle health; healthy eating, physical activity, sleep, mental wellbeing, healthy social relationships and the minimisation of harmful substances. These interconnected behaviours are recognised to support illness prevention and overall health. A growing evidence base suggests that engagement with the arts does not merely sit alongside these pillars but actively interacts with them.
Art promotes dignity, identity and humanity. Part of its power lies in the stance artists take toward people and their potential:
‘Participants value the gaze of the artist which, unlike that of the therapist, regards them as people with potential – potential to create, to inspire, to develop – rather than a problem to solve.’
This perspective can help counter the unintended narrowing of the clinical gaze to symptoms, risks or tasks. For health and care professionals striving to deliver careful and kind care, engaging with artists and creative practice offers a valuable shift: it encourages us to look beyond the immediate problem and reconnect with the person in front of us.
Attending and participating in arts activities can also benefit wider society. Recent economic analyses reinforce how these activities can reduce demand on traditional healthcare services and support productivity. Investment by the Arts Council of Wales in funded arts organisations is estimated to generate around £11 in health, wellbeing and productivity benefits for every £1 invested. This economic impact strengthens the case for viewing arts organisations as public health assets.
Access matters. Creativity should be for everyone. Yet some face barriers to engaging in the arts. Health conditions, confidence, transport, cost and education all shape participation. Designing for equity means recognising different patterns of engagement and facilitating access.
Case Study: Art in Renal Care, Art in Hospital
People undergoing long-term haemodialysis often experience emotional and psychological challenges. In partnership with NHS staff, Art in Hospital developed Art in Renal Care, a programme delivered across three NHS Greater Glasgow & Clyde renal units to provide meaningful, person centred creative activity during treatment.
Artists worked alongside people during dialysis through weekly sessions focused on creative expression, agency and human connection, with all materials provided. Participants were encouraged to share their work, and three public exhibitions celebrated creativity, challenged perceptions of illness and recognised participants as artists. The programme has grown from a pilot into an internationally recognised model of good practice.
Independent evaluation identified four major areas of impact: increased self efficacy, strengthened human relationships, reduced psychological intrusion of dialysis and renewed connection with life beyond illness. Participants described feeling calmer, more positive and more in control, with half reporting that they actively looked forward to dialysis sessions during the programme. Staff noted improved mood, greater engagement and more meaningful interactions. Art in Renal Care demonstrates a powerful and sustained contribution of creative practice to quality of life for people receiving dialysis.
Case study: ReConnect
The Scottish Chamber Orchestra’s ReConnect programme uses co-creative music making to support wellbeing, communication and social connection for people living with dementia. Developed in partnership with the University of Edinburgh and delivered with health and care organisations across the Lothians, the programme offers weekly sessions in hospital wards, care homes and community settings. These sessions have been shown to improve mood, increase engagement, reduce anxiety and create meaningful opportunities for creative expression, with families and staff reporting stronger relationships, reduced stress and deeper connection.
Central to ReConnect is a commitment to dignity and humanity. By engaging with people as creative individuals rather than as patients or residents, the programme supports agency, identity and personhood. Musicians and facilitators respond to verbal, musical and gestural contributions, creating inclusive shared experiences that shift interactions away from clinical routines and towards moments of joy, connection and self-expression. This approach enhances wellbeing while helping staff and families relate with renewed empathy and recognition of enduring strengths.
ReConnect also demonstrates how an orchestra can act as a public health asset. Through sustained collaboration, the SCO contributes to preventative health, social cohesion and improved mental wellbeing, complementing care services and strengthening community resilience.
Case study: Playlist for Life
More than 90,000 people in Scotland live with dementia. Playlist for Life promotes the use of personally meaningful music as a simple, person centred approach to improving quality of life. They provide practical resources and training to help families, communities and professionals integrate music into support.
NHS Fife has adopted Playlist for Life across wards and community services. In an A&E study involving 28 people with dementia, 96% became markedly less stressed during procedures after using personal music. In NHS West Fife, use of playlists at home supported symptom management, with 80% of individuals experiencing a reduction in PRN medication.
As one person living with dementia reflected, ‘Music has a way of connecting to you and that really can make you better. I think we should be prescribing it… taking it more seriously.’ Staff report similar benefits, with personalised music now used strategically to provide comfort and reduce anxiety during care.
Playlist for Life is working across NHS Lanarkshire, NHS Greater Glasgow and Clyde and NHS Fife to further evaluate impact and develop an implementation pathway for wider adoption. Free resources are available.
Health and care professionals have an important role in supporting creative engagement as part of holistic care. We can ask about creative interests and signpost people to local opportunities, using social prescribing pathways to connect people with activities. Initiatives such as artist-in-residence programmes or creative groups in care settings enhance the environment, benefitting people who use services and staff. Crucially, arts organisations should be viewed as public health assets: they foster connection, meaning, identity and joy and support mental and physical wellbeing. Making creative experiences accessible at scale requires cross sector collaboration to embed art and culture into everyday life and Scotland’s wider public health approach.
Conclusion
The wellbeing of the people of Scotland is central to the success of our nation. Health is shaped not only by health and care services, but by the conditions of everyday life—in the places where people grow, learn, work, create and belong. These conditions shape wellbeing long before people reach our clinics and underpin persistent inequalities.
To build a healthier population and sustainable system, we must move decisively from reacting to illness to creating health. Prevention must become core business—embedded systemwide. This means acting earlier, investing in the building blocks of health and working differently: across sectors, across systems and alongside the people and communities we serve. Place-based approaches show what is possible when services, resources and local insight align to address root causes.
The inequalities we see today reflect a constellation of social, economic and environmental pressures. Addressing them requires coordinated action beyond healthcare. It also requires strengthening understanding: improving protected characteristics and socio-demographic data, including on ethnicity, education and broader determinants so that action is targeted, effective and accountable.
Health and financial security are deeply interdependent. Supporting wellbeing through fair work, secure income and inclusive opportunity goes hand in hand with improving health. Employers, education settings and cultural institutions are therefore central partners shaping the environments in which people live, work and thrive.
As health and care professionals, we have a distinctive role within this wider system. As trusted voices at moments of vulnerability, we see how these conditions affect health. That trust brings responsibility: to understand those influences, support access to help and use our influence—through our organisations as anchor institutions and in our day-to-day interactions—to help create healthier, fairer conditions.
By building on progress already underway- deepening collaboration, embedding prevention and tackling inequalities with purpose and persistence- we can create a Scotland where health is not determined by circumstance but supported by design and where people are healthier, more secure and better able to live lives they value.
Contact
Email: RealisticMedicine@gov.scot