The Health Protection (Coronavirus) (Requirements) (Scotland) Amendment Regulations 2022 and The Health Protection (Coronavirus) (Requirements) (Scotland) Amendment (No. 2) Regulations 2022: children's rights and wellbeing impact assessment
This children's rights and wellbeing impact assessment (CRWIA) analyses the potential impact, both positive and negative, of amending the definition of “fully vaccinated” to include the requirement for a booster vaccination if a person’s primary course of MHRA vaccine was more than 120 days ago and amend the definition of late night venue.
Children's Rights and Wellbeing Impact Assessment
CRWIA title:
The Health Protection (Coronavirus) (Requirements) (Scotland) Amendment Regulations 2022 and The Health Protection (Coronavirus) (Requirements) (Scotland) Amendment (No. 2) Regulations 2022
No 1 Regulations amend the Covid Status Certification definition of fully vaccinated to include the requirement for a booster vaccination if a person's primary course of MHRA vaccine was more than 120 days ago. No 2 Regulations amend the definition of late night venue.
Publication date: 24/1/2022
Summary of policy aims and desired outcomes
Legislative Background
The Health Protection (Coronavirus) (Requirements) (Scotland) Amendment Regulations 2022 and The Health Protection (Coronavirus) (Requirements) (Scotland) Amendment (No. 2) Regulations 2022 (the 'Regulations') are made under powers to make provision for the purpose of preventing, protecting against, controlling or providing a public health response to the incidence or spread of infection, conferred on the Scottish Ministers by schedule 19 of the Coronavirus Act 2020. These Regulations, which bring into force and amend The Health Protection (Coronavirus) (Requirements) (Scotland) Amendment Regulations 2021 ("the principal Regulations"), will come in to force on Monday 17th January and Monday 24th January 2022, respectively.Data from numerous studies pre-Omicron
Introduction
This Children's Rights and Wellbeing Impact Assessment (CRWIA) analyses the potential impact, both positive and negative, of amending the definition of "fully vaccinated" to include the requirement for a booster vaccination if a person's primary course of MHRA vaccine was more than 120 days ago and amend the definition of late night venue. The scheme will continue to accept a negative test (either LFD or PCR) as an alternative to proof of vaccination. The UN Convention on the Rights of the Child (UNCRC) defines a child as anyone under the age of 18. The child wellbeing indicators under the Children and Young People (Scotland) Act 2014 reflect the principles within the UNCRC and also apply to all children up to the age of 18 and so all children are within the scope of this CRWIA.
It is the view of the Scottish Government that Covid Status Certification is a proportionate means of helping to achieve the goals set out in the Policy Objectives section and, in view of this, any negative impacts are currently justified. However, we also recognise that these measures are only required to respond to the current set of circumstances, and only necessary as long as the potential public health benefits can justify any negative impacts caused.
International evidence suggests that crises responses often inadvertently discriminate. The Equality and Human Rights Commission, the Scottish Human Rights Commission and the Children's Commissioner for Scotland stated in April 2020 they had already found increasing evidence that some groups are experiencing disproportionately negative impacts from the virus and some of the responses to it.[1]
The Scottish Government are committed to ensuring that human rights, children's rights and equality are embedded in everything we do and are central to our response to the pandemic. The Framework for Decision Making recognises that harms caused by the pandemic do not impact everyone equally and that we must work to advance equality and protect human rights.
Background
Mandatory Covid Status Certification came into force on 1 October 2021. This required certain premises and settings to ensure that there is a reasonable system in operation for establishing that all people in the premises can demonstrate that they are fully vaccinated or can present a record of a negative test in the last 24 hours or that they are exempt, and to refuse access to or remove any one who is not fully vaccinated. To be considered fully vaccinated, you must have completed a course of an authorised vaccine with the final dose having been received at least 2 weeks previously. If 120 days have passed since the primary course was completed you must have had a booster dose plus 10 days (this is to ensure that the vaccine has taken effect). A negative test result means that a person has received a negative Lateral Flow Device test (LFD) or Polymerase Chain Reaction (PCR) test in the last 24 hours.
The settings covered in the original scheme on 1 October include:
- late night premises with music, which serve alcohol after midnight and have a dancefloor or space where dancing by customers take place
- indoor events (unseated) planned for 500 or more people at any one time
- outdoor events (unseated) planned for 4,000 or more people at any one time
- any event planned for 10,000 or more people at any one time
Based on evidence and a balance of the four harms[2] of the virus, the regulations were subsequently amended on 6th December to include a negative test result (either a lateral flow device (LFD) or polymerase chain reaction (PCR) from within the last 24 hours, as an alternative to proof of vaccination to gain entry to the settings in scope. Initially, the scheme – introduced on 30th September - did not include a negative test result as an alternative to proof of vaccination as we did not consider that it would be appropriate and believed it could undermine one of the policy aims of the scheme: to increase vaccine uptake. This new provision came into effect on 6 December.
This change makes it possible for more people to make use of the scheme, such as those who are not yet fully vaccinated. It also means that individuals who received a vaccine not recognised by the MHRA, or who have experienced difficulty accessing their vaccination record, will be able to attend venues covered by the scheme. We hope that the inclusion of testing will encourage the greater use of regular testing and will still support us to achieve our policy objective of reducing the risk of transmission of Coronavirus.
Ministers have been clear that the Covid Status Certification will not be a requirement for public services or other settings that many people have no option but to attend, such as public transport, health services and education.
The following people are exempt:
- under 18s
- people who for medical reasons cannot be fully vaccinated and cannot undertake a qualifying COVID-19 test
- people taking part (or who have taken part) in vaccine trials
- the person responsible for the premises
- workers and volunteers at the premises or event
- emergency services responders and regulators carrying out their work.
The regulations require the persons responsible for a setting to ensure there is a reasonable system in operation for checking that people seeking to enter the premises are either fully vaccinated or can provide record of a negative test result (either LFD or PCR), or are exempt, and to have in place a compliance plan for the system.
Legislative amendments
Since these regulations were amended in early December, the new Omicron variant of Covid-19 has emerged and is now dominant in Scotland. There is evidence to indicate Omicron is more transmissible than other variants and partially escapes immunity from vaccines as well as previous infections[3]. The modelling in Scotland up to 3 January 2022 estimates a doubling time of 3.88-3.95 days[4]. Omicron became the dominant variant in Scotland on 17 December 2021.[5]
Covid Status Certification has been amended so that the definition of "fully vaccinated" includes the requirement for a booster vaccination if a person's primary course of an MHRA vaccine was more than 120 days ago. These amendments come into force on 17 January 2022. The amendments to the definition of late night venue come into force on 24th January 2022.
Ministers must review The Health Protection (Coronavirus) (Requirements) (Scotland) Amendment Regulations 2021 (which makes provision for the Certification Scheme) at least every 3 weeks to assess whether any requirement in the regulations is still necessary to prevent, protect against or provide a public health response to the incidence or spread of infection in Scotland.
We will continue to assess whether any less intrusive measures could be introduced to achieve the same combination of policy objectives in respect of the higher risk sectors concerned; if so, the requirements will be immediately reviewed.
Sectoral Guidance is published on the Scottish Government website. Guidance for the wider public is published on the Scottish Government website.
Policy Objectives
In line with our strategic intent to 'suppress the virus to a level consistent with alleviating its harms while we recover and rebuild for a better future', the policy objectives of Certification remain to:
- Reduce the risk of transmission of Coronavirus, by ensuring that specified public spaces where transmission risks are higher are used only by those who are fully vaccinated including a booster when required, can provide a record of a negative test within the previous 24 hours, or are exempt. Vaccination or a negative test within the previous 24 hours reduces (but does not eliminate) the risk of being infected, the risk of serious illness and death if they are infected and the risk of infecting others;
- Reduce the risk of serious illness and death thereby alleviating current and future pressure on the National Health Service, by reducing transmission in specified settings where transmission risks are higher;
- Reduce the risk of settings specified in the scheme being required to operate under more restrictive protections, or to close, by ensuring that the risk of transmission in these settings is reduced; and
- Increase the protection enjoyed by those using settings covered by the scheme and their contacts, by incentivising those using the settings to get vaccinated and to test regularly and self-isolate if positive.
An evidence paper summarising the range of evidence available on certification schemes has been published. Consistent with our approach throughout the pandemic, the paper adopts a four harms approach covering the direct health harms of Covid-19, the indirect health harms, the social and the economic harms. Evidence is drawn from clinical and scientific literature, from public opinion and from international experience. A follow-up evidence paper which sets out the evidence on certification schemes since the original paper was published is available. An evidence paper on the Omicron variant was published on 10 December 2021. This impact assessment should also be considered alongside the latest State of the Epidemic report.
Public health rationale
The COVID-19 epidemic continues to pose considerable challenges. After decreasing in November 2021, new case rates rose sharply from the end of December and peaked in early January 2022. The 7 day positive PCR case rates per 100,000 are currently averaging around under a 1,000 per day (based on PCR tests only). However, it should be noted that on 5 January 2022, the Scottish Government announced that people who do not have symptoms of Covid-19 will no longer be asked to take a polymerase chain reaction (PCR) test to confirm a positive Lateral Flow Device (LFD) result. Instead, anyone with a positive LFD, who does not have symptoms, should report the result online as soon as the test is done. This means that those without symptoms who previously would have taken a confirmatory PCR test, will no longer do so. As a result, these positive cases are not directly comparable with previously reported number of cases.
Weekly hospital admissions with confirmed COVID-19 have started to decrease over the last week. Case rates and age standardised hospital admissions are considerably lower in vaccinated versus unvaccinated individuals. Modelling indicates uncertainty over hospital occupancy and intensive care in the next four weeks. Hospitals are currently at, or very close to, capacity and have been in this position for many weeks now with several Health Boards operating within an environment of unprecedented pressure and heightened risk, plus a requirement for military support. This is likely to be driven by Covid-19 cases and delayed discharges but also may reflect that patients with higher acuity are now requiring admission.
Omicron is now the dominant variant across the UK[6]. Risk assessments on Omicron (B.1.1.529) have been published by the UK Health Security Agency (UKHSA).[7] The growth advantage has been designated as red, with a high confidence, indicating that Omicron has a significant growth advantage over Delta, with greater household transmission risk and secondary attack rate being seen. [8] [9] There is high confidence that immune evasion is a substantial contributor to the growth advantage but it is also biologically plausible that increased transmissibility of the omicron variant is also contributing.
Therefore, the transmissibility of Omicron has been designated as amber with a low confidence by the UKHSA indicating that that Omicron is at least as transmissible as Delta but further analysis is required.[10] There is also evidence of widespread community transmission of Omicron.[11] [12]
Immune evasion to both natural and vaccine derived immunity has been designated as red with a high confidence by the UKHSA indicating that there is evidence of frequent infection in humans with known prior infection or vaccination[13]. Neutralisation data, real world vaccine effectiveness against symptomatic disease, and reinfection rate all confirm substantial immune evasion properties[14] [15].
Infection severity has been designated as green with high confidence by the UKHSA meaning there is evidence to support a moderate reduction in the relative risk of hospitalisation compared to Delta, ranging from 15 to 80%[16] [17]. The data published by UKHSA indicate that the risk of attending hospital or emergency care is around half that of Delta and the risk of being admitted from emergency care around is around one third of Delta[18]. SAGE 102 minutes identify a potential reduction of 35-65% for the risk of hospitalisation compared to Delta[19]. The reduction in infection severity is likely to be partly due to the nature of the variant and partly due to protection from prior infection; however, the relative contributions of the two factors has not been quantified[20]. Early data from COVID-19 Clinical Information Network (CO-CIN) considered by SAGE on 7 January 2022 indicate that the severity of disease being observed in hospital over the last three weeks is lower than observed in early phases of previous waves, with less need for oxygen, less admission to intensive care, better outcomes, and shorter stays[21]. From the SAGE 101 meeting on 23 December 2021, UKHSA data suggests a doubling time of 4 to 5 days for hospitalisations[22].
Infection severity in children has been designated as amber with a low confidence as, although there has been an increase in hospital admissions, further analysis is required to compare the risk of hospitalisation between Omicron and Delta, and to assess the clinical nature of the illness in children [23].
The Scientific Pandemic Influenza Group on Modelling, Operational sub-group (SPI-M-O) concluded that "If omicron in the UK combines increased transmissibility and immune escape, irrespective of severity, it is highly likely that very stringent measures would be required to control growth and keep R below 1"[24].
Our primary and secondary health and social care services are facing arguably the most significant and increasing pressures and demands in the history of the NHS. The winter period is also posing significant challenges of increased transmission and related pressure on the National Health Service. We remain of the view that action is therefore needed across all sectors to ensure adherence to baseline measures. Drawing on the evidence so far available, we consider that Covid Status Certification has an important role to play as one such measure including as a precautionary measure in light of the new Omicron variant.
Vaccination
While no vaccine is 100% effective at preventing infection, disease and transmission, and they do not completely break the link between a high volume of positive cases and serious pressure on healthcare services, they are our best route out of the pandemic. Vaccines help prevent transmission of the virus as vaccinated people are less likely to become infected and ill than unvaccinated people (and only infected people can transmit the virus). The UK Vaccine Effectiveness Expert Panel (VEEP) is a group of scientific and analytical specialists from academia and government in the UK who provide a consensus view on vaccine effectiveness, split by variant, vaccine and dose. They have published estimates for vaccine effectiveness based on an assessment of the evidence at the time of writing and as new evidence or data emerges, SAGE will update its advice. The most recent summary was published on 24th September 2021.
Vaccine effectiveness against symptomatic disease with the Omicron variant is lower compared to the Delta variant and wanes rapidly. However, boosting returns it to a comparable level[25]. Vaccine effectiveness 2 to 4 weeks after a booster dose ranged from around 65 to 75% for Omicron compared to >90% for Delta. Vaccine effectiveness against symptomatic disease drops to 55 to 70% at 5 to 9 weeks after a booster and a further drop to 40 to 50% from 10+ weeks after the booster for Omicron, whereas vaccine effectiveness for Delta remains over 80% at 10 weeks[26] [27].
Protection against hospitalisation from vaccination is much greater than that against symptomatic disease, in particular after a booster dose[28]. Vaccine effectiveness against hospitalisations 4 weeks after dose 1 is at 58%, between 2-24 weeks after dose 2 at 64% and for 25+ weeks after dose 2 at 44%. Data released by UKHSA suggest that 2 to 4 weeks after a booster, vaccine effectiveness increases to 92%, after 5-9 weeks drops to 88% and that at 10+ weeks after booster, vaccine effective against hospitalisation remains at 83%[29]
Early data considered by SAGE suggest that the probability of needing admission to ICU is very much higher in the unvaccinated population for the Omicron variant[30]. There is currently insufficient data to make an assessment of vaccine effectiveness against severe disease for Omicron compared to Delta[31]. However, though waning has been seen in vaccine effectiveness, it is thought that vaccine effectiveness against severe disease is more likely to be sustained, especially after a booster dose 32 . More analysis can be found in a number of large studies including EAVE-II (Early Pandemic Evaluation and Enhanced Surveillance of Covid-19) in Scotland[33], Real-time Assessment of Community Transmission (REACT-1) in England[34] and the Office for National Statistics (ONS) Covid-19 Infection Survey ONS study.[35] Therefore, we have strong evidence that vaccines are effective at preventing disease, hospitalisations and deaths.
As of 18 January 2022, 85.5% of the eligible population (12+) received two doses of the vaccine and 67.2% (12+) received a booster or third dose. In the week 1 to 7 January 14.2% of positive cases were in unvaccinated individuals. In the week 1 - 7 January in an age-standardised population, individuals were 4 times more likely to be in hospital with COVID-19 if they were unvaccinated compared to individuals that had received a booster or third dose of vaccine[36].
Vaccine uptake has progressed extremely well in the Scottish adult population with approximately 80.5% of 18 to 29 year olds and 81.8% of 16 to 17 year olds having received the first dose of the vaccine as of 18 January. At least 95% of people aged 50 and over have received two doses, but uptake of a second dose remains lower in people in their 30s (79.8%) and the 18-29 age group (72.2%) as of 18 January. Vaccine uptake has slightly increased since the scheme was announced, although it is not possible to directly attribute rises to the introduction of the Covid Status Certification. The proportion of those aged 12+ with a first dose rose to 91.8%, second dose rose to 85.5%, and a third dose or booster rose to 67.2% up to 18 January 2022[37].
Protection due to previous infection
There is limited evidence for Omicron on the duration of natural immunity due to the high levels of vaccination within the population. However, high levels of immune escape have been seen as well as a marked increase in overall reinfection rates[38] [39] [40].
Data published on 17 November, pre Omicron, showed that those who have had a COVID-19 infection previously continue to be less likely to test positive than those who had not, with estimated likelihood of testing positive similar to those who received three doses of COVID-19 vaccine more than 14 days ago and those who received two doses of Pfizer/BioNTech vaccine between 15 to 90 days ago. Those who had previous infection were 1/5th less likely to test positive for Covid compared to those who had not.[41]
Data from numerous studies pre-Omicron indicate that neutralising antibodies last from 5-7 months[42] for up to a year[43] after SARS-CoV-2 infection. Individuals with severe illness produce more antibodies[44] and vaccination of individuals who have already been infected induces higher levels of protection than following infection alone.[45] [46] Young people tend to have a stronger antibody based on immunity to SARS-CoV-2 that lasts longer. A UK based study focusing on prevalence of antibody positivity to SARS-CoV-2 after first peak of infections showed that the highest prevalence and smallest overall decline in positivity was in the youngest age group (18-24 years), and lowest prevalence and largest decline in the oldest group (>74 years).[47]
In summary it is difficult to say definitively how long natural (post-infection) immunity will last. A NERVTAG paper (New and Emerging Respiratory Virus Threats Advisory Group) presented to Scientific Advisory Group for Emergencies (SAGE) on 27 May discussed that protection from re-infection with SARS-CoV-2 can last at least 7 months and in some studies up to one year.[48]
Testing
Two main testing methods exist for detection of SARS-CoV-2: LFDs or PCR. PCR is the recommended testing method if you have COVID-19 symptoms while LFDs are recommended only for people who do not have symptoms.[49] PCR is a highly sensitive and specific technique to detect SARS-CoV-2 and is a recommended diagnostic testing method by the World Health Organisation (the WHO)[50]. Specificity and sensitivity levels of >95% have been reported by SAGE for PCR testing[51].
LFD testing is effective at identifying people with the virus when they are at their most infectious and have high viral loads.[52] A peer-reviewed study on sensitivity of the LFDs carried out by University College London found that LFDs are more than 80% effective at detecting any level of COVID-19 infection and, therefore, can be an effective tool in reducing transmission.[53] Another study showed that LFDs are 95% effective and 89.1% specific at detecting COVID-19 when used at the onset of symptoms.[54] A review on the diagnostic accuracy of point‐of‐care antigen and molecular‐based tests for diagnosis of SARS‐CoV‐2 infection concluded that LFDs which pass the criteria for use (e.g. WHO's priority target product profiles for COVID‐19 diagnostics) can be considered as a replacement for PCR.
Data from the Assessment of Transmission and Contagiousness of COVID-19 in Contacts (ATTACCC) study show that false negative LFD test results mostly occurred 1 to 2 days prior to peak viral load and became negative at approximately the same time as viral culture became negative[55]. This indicates that LFDs are effective at detecting infectious cases. All the LFDs in use in the National Testing System have been shown by the British Government's Science Park, Porton Down, and University of Oxford SARS-CoV-2 lateral flow antigen test validation cell to be effective in detecting the Omicron Variant of Concern[56].
SAGE endorsed the benefits that rapid antigen testing (such as LFD testing) could have on reducing transmission when discussing the UK Government Plan B options: "Other measures are available which, if introduced, could also make Plan B (or more stringent measures) less likely (and could potentially offer better efficiency or effectiveness) for example encouraging wider use of rapid antigen testing in workplaces and the community, and ensuring self-isolation of those who test positive by providing sufficient support".[57]
The Scottish Government recommends to take regular lateral flow tests - especially before mixing with other people or visiting a hospital or care home, regardless of vaccine status or recent periods of infection. This will almost always identify Covid during early stages of infection and thus significantly reduce disease transmission[58]. The optimal testing strategy in order to gain access to a high risk setting would be to take the test as close as practically possible to the time of entry. LFDs are less sensitive than PCR but have the advantage of providing rapid results, and SAGE has endorsed the benefits that rapid antigen testing (such as LFDs) could have on reducing transmission.
Customers can display an SMS (text), email or a paper printed copy showing they have registered a record of a negative test. There is no QR code within SMS or emails and so they do not need to be scanned by the NHS Scotland Covid Check App. Venues will instead perform a visual check and no data will be retained. Individuals can get an SMS or email by registering the result of their negative LFD test on the GOV.UK website, and opting in to receive notification of their result. If individuals undertake a PCR test they will automatically receive an SMS or email with the results.
The testing option requires people to have access to a standard mobile phone, mobile device or computer with an email address and access to a printer. This does not need to be a 'smart phone' and can be any mobile phone or tablet that can receive text messages or has access to email. Test results can be displayed on a mobile phone, tablet or other device, or a paper copy can be printed using a home printer or using a service which provides printing facilities, such as a public library.
For those unable to test themselves, self-test LFD kits can be administered by others (such as a family member, friend, or carer) who can also register the result on behalf of the person they tested if they are also unable to do so. For those unable to display their test results (such as people who do not have a mobile phone) when registering their result they could have it sent to another person's phone, who could then show the result on their behalf.
Settings
Higher-risk settings tend to have the following characteristics: close proximity with people from other households; settings where individuals stay for prolonged periods of time; high frequency of contacts; confined shared environments, and poor ventilation.[59] [60] These settings are considered higher risk due to the way COVID-19 spreads. COVID-19 spreads in small liquid particles when an infected individual coughs, sneezes, speaks, or breathes.[61] These droplets are able to remain suspended in the air. When people are close together or in a confined, unventilated space, it is more likely these droplets will enter another person, either through inhalation, the droplets coming into contact with their eyes, nose or mouth, or by touching an infected surface and then touching their eyes, nose or mouth. [62] When people meet who do not regularly see each other or have a high frequency of contacts, it is more likely one of the individuals is asymptomatically infected through their separate social groups as the total number of extended contacts is greater. Examples of settings identified by SPI-B as high risk include public transport; places of worship, shops, malls and markets; parties; cinemas; theatres; planes; large family gatherings; cultural, sporting and political events; crowds; pubs and clubs; restaurants and cafes; hotels, cruise ships, hospitals and care homes.[63]
The Virus Watch Community Cohort Study found that during a period of no restrictions (September – November 2021), hospitality was associated with an increased risk indoors but not outdoors. Participating in sports indoors or outdoors was also associated with increased risk (although it was noted that this may relate to associated social activities). It was found that there was no good evidence of increased risk from attending cinemas, theatres, concerts, indoor sports events or for beauty services[64]. Evidence from Germany has found that regular cinema ventilation is sufficient to minimise the risk of COVID-19 infection[65]. However, studies have shown that intoxication has the potential to increase the risk of transmission of COVID-19 due to a decrease in compliance with increasing levels of intoxication, notably a reduction in physical distancing, lack of face masks when not seated and mixing with groups at other tables[66]. In addition, modelled research by the Tony Blair Institute for Global Change reported that, if the NHS COVID pass had been made mandatory for crowded indoor and mass attendance settings (including sports matches, large outdoor events, indoor performances and nightclubs) in England after the lifting of restrictions on 19 July 2021, cases and deaths over the subsequent weeks could have been reduced by as much as 30%[67].
By restricting access to customers who are fully vaccinated and/or who can provide a record of a negative test, it is less likely that infection will take place in these settings, and it is less likely that infections within them will lead to illness. Additionally, vaccination, boosters and regular testing will continue to be incentivised.
Consequently, we can reduce the risk of transmission of the virus and help reduce pressure on health services, while also allowing settings to operate as an alternative to closure or more restrictive measures. As such, we consider the Covid Status Certification, as part of a package of measures such as improved ventilation, to be a necessary and proportionate public health measure.
NHS Scotland Covid App and Paper Certificate
On 30 September we launched the NHS Scotland Covid Status App (the "App") for international use. This contains two unique QR codes, one for each dose of the vaccine and since 13 January has included booster doses. This product has been designed for use for international travel and domestic use. To meet international travel requirements it is necessary to include full name, date of birth and details of vaccination to meet EU standards. This version of the App can be used to demonstrate vaccine status in the settings in scope.
On 20 October, the NHS Scotland Covid Check App, which is used by venues to check QR codes, was updated so that when an international QR code is scanned for domestic purposes only a green tick or 'Certificate not valid' is displayed, rather than a person's name, date of birth and vaccination details.
In order to further minimise data display, on 21 October, the Covid Status App was updated to include a domestic page. This option simply shows the person's name and a QR code. When the QR code is scanned by the NHS Scotland Covid Check App it shows either a green tick or 'Certificate not valid' representing someone's vaccination status. The domestic App has functionality to hide or display a person's name. The Privacy Notice can be found on NHS Inform: Personal information we process, How we use your data, Your Rights.
On 13 January the NHS Scotland Covid Status App was updated to reflect the Scottish Government's new definition of fully vaccinated. This means that anyone who has not received the booster dose within 120 days (four months) of completing their primary course will no longer be deemed to be fully vaccinated.
Many countries accept proof of a negative PCR test (valid for 72 hours in line with EU specifications) or recovery status (that you have tested positive for Covid within the past 180 days) as an alternative to vaccination and some countries request a third vaccine (booster) as proof of vaccination for international travel purposes. On 9 December the Covid Status App was updated to include recovery status, third dose of the vaccine and boosters.
The paper and PDF certificates were updated to include evidence of an individual's last 2 doses of the vaccine on 13th December. Boosters were added to the app for domestic use on 13th January, boosters will show on the domestic page 10 days after received. Further development work will be required to update further information such as LFD negative test status in a future release of the App. In the meantime, customers can display an SMS (text) or email which records they have received a negative test. There is no QR code within SMS or emails and so they do not need to be scanned by the NHS Scotland Covid Check App. Venues will instead perform a visual check and no data will be retained. Individuals can get an SMS or email by registering the result of their LFD test on the GOV.UK website.
The latest PHS report[68], published on Wednesday 19 January showed that, as of midnight 15 January 2022, the NHS Covid Status App has been downloaded 2,431,409 times. It is important to note a single user may choose to download the App on multiple devices, so this figure does not represent unique individuals. Between 03 September 2021 (introduction of QR codes) and midnight 15 January 2022, 715,974 paper copies of COVID-19 Status have been requested. This may not represent unique users if an individual requests a second copy (for example if they have lost their paper copy or needed to order a new one to refresh the QR codes after these have been updated). 1,736,949 PDF versions of COVID-19 Status have been downloaded. This provides a measure of the total number of times a new QR code has been generated via PDF. An individual can generate more than one successful QR code so the figure does not represent unique users. We continue to monitor user activity closely.
For those who do not have digital access or would prefer a paper copy, a record of vaccination can still be requested by phoning the Covid-19 Status Helpline on 0808 196 8565. The paper record of vaccination will then be posted to the address that is on the individual's GP records and held on the National Vaccination Service System (NVSS).
When registering an account on the App the user needs to verify their identity. This is for privacy protection as health data is special category data and protected by General Data Protection Regulations (GDPR) and human rights legislation (Article 8 right to respect for private and family life) and so additional safeguards and security measures are required to verify a person's identity before they are given access to their health records. This means users are asked to scan a photo of their passport or driving licence and then to take a live photo of themselves. The software then uses their live photo to compare likeness with the photo in their ID and confirm their identity. There is manual verification for the small number of cases which fail the automatic process. For the limited number of cases where a person's identity cannot be verified in the App, individuals can call the Covid-19 Status Helpline, or use NHS Inform to request a paper Certificate, which will be posted to them.
We continue to keep the ID Verification process under review. This includes consideration of alternative forms of ID that can be uploaded, such as PASS-accredited cards such as Young Scot and UK Government issued immigration and asylum cards as an accepted form of ID. Broader use of National Entitlement Cards have been ruled out due to lack of relevant security features on the cards themselves.
Identity verification (IDV) is an important safeguard for people using the App to ensure that only the person themselves is able to access their vaccination record, which is part of their medical record. We carried out an options appraisal which concluded that facial recognition was the option that provided the highest degree of security. IDV information is only used to identify the person and ensure the requester of the Certificate is actually the person holding the device/phone. This data is not retained. Due to the need to develop the NHS Scotland Covid Status App quickly for international travel purposes and against a backdrop of rising cases and pending winter pressures on the NHS in Scotland, which meant the introduction of domestic Covid Status Certification was likely, it was not possible to develop more than one IDV route for the App's introduction. Work is underway to put in place alternative IDV routes.
In addition the paper and PDF versions of the Certificate were already available for people to use, either if they are unable or unwilling to use the IDV route, so people are not excluded from accessing their medical data. The user pathway for these products is different for these routes, including using information in relation to the person's vaccination that it would not have been easily possible to replicate for the App. In addition paper Certificates are sent to the address the person is registered with at their GP.
Customers can display an SMS (text) or email showing they have registered a negative test. There is no QR code within SMS or emails and so they do not need to be scanned by the NHS Scotland Covid Check App. Venues will instead perform a visual check and no data will be retained. Individuals can get an SMS or email by registering the result of their negative LFD test on the GOV.UK website. If individuals undertake a PCR test they will automatically receive an SMS or email with the results.
The testing option requires people to have access to a standard mobile phone, mobile device or computer with an email address and access to a printer. This does not need to be a 'smart phone' and can be any mobile phone or tablet that can receive text messages or has access to email is sufficient. Test results can be displayed on a mobile phone, tablet or other device, or a paper copy can be printed using a home printer or using a service which provides printing facilities, such as a public library by the individual. In Scotland, it is estimated that 88% of households had internet access in 2019, however this varied by household net income and deprivation. The proportion of internet users reporting that they access the internet using a smartphone increased from 81 per cent in 2018 to 86 per cent in 2019 [69]
For those unable to test themselves, self-test LFD kits can be administered by others (such as a family member, friend, or carer) who can also register the result on behalf of the person they tested if they are also unable to do so. For those unable to display their test results (such as people who do not have a mobile phone) when registering their result they could have it sent to another person's phone, who could then show the result on their behalf.
Exemptions
There are medical exemptions for domestic Covid Status Certification for the very limited number of people who for medical reasons cannot be safely vaccinated or tested. In the vast majority of cases, a successful route to safe vaccination or testing can be found. Local vaccination centres can help to answer questions about the vaccine and can advise what arrangements may be put in place to enable safe vaccination.
In the rare cases where that support does not lead to vaccination, an exemption is offered to the individual which can be used for international use. If the individual cannot be tested, they will be advised to obtain proof of evidence from their primary or secondary care clinician in the form of a letter. This evidence will then be assessed by a Scottish Government clinician who will work with the Resolver Group to provide the necessary support on a case-by-case basis to determine whether the individual is exempt from testing. For more information on exemptions see the NHS Inform website, call the Covid-19 Status Helpline on 0808 196 8565 or visit your local vaccination centre.
Medically exempt individuals are provided with paper Certificates which have enhanced security features. Medical exemptions cannot be displayed on the international section of the App due to EU specifications. They are under consideration for a future release of the domestic section of the App. We continue to engage across the four nations to ensure that work around exemptions is taken forward collectively. All clinical trial participants have received a letter from their Principal Investigator which can be used for proof of their trial status. Clinical trials participants are encouraged to undertake testing and provide a record of a negative test, as they may have received a placebo dose.
While children are exempt from the requirement to provide Covid Status Certification for domestic purposes, 12-17 year olds who have been vaccinated may choose to download a PDF of their vaccine record via NHS Inform, or they may choose to request a paper Certificate by calling the Covid-19 Status Helpline. 12–17 year olds may also choose to provide a record of their negative test. This can be done using the same routes as adults for paper copies.
The paper vaccine Certificates are in English. Information about what information the Certificates contain can be requested in other languages and alternative formats including Easy Read, audio and Braille. Information can be found on NHS Inform, or when people request their Certificate. Information about PCR home testing is also available in a variety of languages and formats.
For more information on the Covid Status Certificate see the Scottish Government website.
Policy Objectives
In line with our strategic intent to 'suppress the virus to a level consistent with alleviating its harms while we recover and rebuild for a better future', the policy objectives of Covid Status Certification are to:
- Reduce the risk of transmission of Coronavirus, by ensuring that specified public spaces where transmission risks are higher are used only by those who are fully vaccinated, including a booster or have tested negative in the previous 24 hours
- Reduce the risk of serious illness and death thereby alleviating current and future pressure on the NHS, by reducing transmission in higher risk settings. Vaccination reduces (but does not entirely eliminate ) the risk of being infected, the risk of serious illness and death if infected, and the risk of infecting others
- Reduce the risk of settings specified in the scheme being required to operate under more restrictive protections, or to close, by ensuring that the risk of transmission in these settings is reduced, reducing overall cases of Covid
- Increase the protection enjoyed by those using settings covered by the scheme and their contacts, by incentivising those using the settings to get vaccinated and to test regularly and self-isolate if positive
Executive summary
The Scottish Government has introduced The Health Protection (Coronavirus) (Requirements) (Scotland) Amendment Regulations 2022 and The Health Protection (Coronavirus) (Requirements) (Scotland) Amendment (No. 2) Regulations 2022. in order to reduce the risk of transmission of Coronavirus; reduce the risk of serious illness and death; reduce the risk of settings specified in the scheme being required to operate under more restrictive protections, or to close; and to increase the protection enjoyed by those using settings covered by the scheme and their contacts.
The amendments to the scheme will come into force on January 17th and January 24th 2022. A record of a negative test (either LFD or PCR) as an alternative to proof of vaccination will continue to be accepted for the purposes of Certification.
This requirement applies to customers only and does not apply to staff, contractors, performers or volunteers involved in the delivery of the event or working in the settings in scope, as we do not want to compromise people's right to work (UNHRC Article 23; UNCRC Article 6) or employment prospects.
This document builds upon previous work undertaken to ensure that children's rights and wellbeing are at the centre of our response to the pandemic, and upon previously published CRWIAs. This document sets out the potential impact of Covid Status Certification, both positive and negative, on children's rights and wellbeing, and the mitigations put in place to negate the wider harms.
This is a global pandemic and these are highly uncertain times, which means our decision making process is continuous and multi-faceted. We will continue to make every effort to ensure that children's rights and wellbeing are central to our response to the pandemic and that CRWIAs are undertaken and published as necessary.
Background
On the 1 October the Scottish Government introduced Covid Status Certification. The requirement for persons responsible for late night premises or a relevant event to ensure a reasonable system is in operation for checking Covid Status Certification came into force on the 18 October 2021.
The Scheme was introduced in line with our strategic intent to 'suppress the virus to a level consistent with alleviating its harms while we recover and rebuild for a better future' and the policy objectives were to:
- reduce the risk of transmission of Coronavirus
- reduce the risk of serious illness and death thereby alleviating current and future pressure on the National Health Service
- allow higher risk settings to continue to operate as an alternative to closure or more restrictive measures
- increase vaccine uptake.
On the 6 December, based on the latest evidence and a balance of the four harms of the virus, the Scheme was amended to include a negative test result, either a lateral flow device (LFD) or polymerase chain reaction (PCR) in the previous 24 hours as an alternative to proof of vaccination to gain entry to the settings in scope. Initially, the scheme did not include a negative test result as an alternative to proof of vaccination as we believed it could undermine one of the policy aims of the scheme: to increase vaccine uptake. That aim was amended on 6 December to the following: Increase the protection enjoyed by those using settings covered by the scheme and their contacts, by incentivising those using the settings to get vaccinated and/or test regularly and self-isolate if positive.
On 7 December the First Minister gave an update to Parliament on the state of the pandemic and the emergence of the new Omicron variant. She stated that:
'given the situation we face it is important to remain open to any proportionate measures, for example the extension of COVID certification, that might help us reduce the risks should the situation deteriorate.'[70]
On 10 December an evidence paper summarising the known evidence on the Omicron variant was published on the Scottish Government website.
On 14 December Ministers decided not to extend the scope of the scheme and on 26 and 27 December omicron measures were introduced including capacity limits on indoor and outdoor events and the closure of late night venues. This meant settings within the scope of Covid Status Certification were largely closed. With the removal of capacity limits on large outdoor events on 17 January and on indoor events on 24 January as well as the reopening of Covid Status Certification in these settings has restarted. No 1 amendments update the definition of fully vaccinated to take account of the booster vaccination programme, in recognition of vaccine waning against Omicron. No 2 amendments make a technical amendment to the definition of late night venue for clarity. It does not expand the scope of the scheme.
Scope of the CRWIA, identifying the children and young people affected by the policy, and summarising the evidence base
Scope and summary of impacts
The UN Convention on the Rights of the Child (UNCRC) defines a child as anyone under the age of 18. The child wellbeing indicators under the Children and Young People (Scotland) Act 2014 reflect the principles within the UNCRC and also apply to all children up to the age of 18 and so all children are within the scope of this CRWIA. Consideration of the impacts on young people can be viewed as part of the Equality Impact Assessment.
All children would benefit from a reduction in transmission of Covid-19. Children will benefit from any increase in vaccination and boosters within the adult population, as this will increase overall community protection. Between the announcement of the scheme on 1 September and Children would also benefit from an increase in community testing, as more regular testing may increase the likelihood of identifying positive cases and preventing further transmission by people self-isolating, if they receive a positive test. As demonstrated in the summary of evidence below, disabled children and children from minority ethnic (ME) communities are most likely to positively benefit from a reduction in transmission, as evidence shows that these children have poorer health outcomes if they contract the virus. Children aged 12-16 may also benefit slightly more as some evidence shows that long Covid is more evident in this age group than the 2-11 age group 4-8 weeks after infection.
All children would positively benefit from allowing higher risk settings to continue to operate as an alternative to closure or more restrictive measures, as evidence shows that their mental health and wellbeing declined during lockdowns and gradually improved as restrictions eased. Evidence within the summary of evidence shows that the mental health and wellbeing of disabled children, ME children, young carers, LGBT youth and those from lower socio-economic backgrounds are most negatively impacted by restrictions and lockdowns. Therefore, it is likely that they would benefit most if Covid Status Certification allows higher risk settings to continue to operate as an alternative to closure or more restrictive measures.
There may be some unintended negative impacts on children and some groups of children may be impacted more than others. For example children under 18 who look 18 or older may be denied access to a space where Covid Status Certification is required if they cannot prove their age-based exemption.
It is possible that the policy could exceed the intention and children could be denied access to spaces, services, products, employment or education because they do not have Certification. In addition, if a parent, guardian or relevant adult does not have Certification, this could negatively impact on the child if adult supervision is required to enter a space or use a service where Covid Status Certification is required or in operation.
While children are exempt from the requirement to provide proof of vaccination or a record of a negative test for domestic purposes, 12-17 year olds who have been vaccinated may still choose to access their record of vaccination. At present, children cannot use the NHS Covid Status App. Scottish Government officials are working to understand how children could use the App, their understanding of the process, and fundamentally the ease of the user journey. Children's user experiences will support any future development of the App going forward.
12-17 year olds can however access their record of vaccination by requesting a paper copy on NHS Inform where they can also download a PDF, or they can call the Covid-19 Status Helpline on 0808 196 8565.
12–17 year olds may also choose to provide a record of their negative test. Individuals can get an SMS or email by registering the result of their negative LFD test on the GOV.UK website or by calling 119. People who undertake a PCR test will automatically receive an SMS or email with the results. The testing option requires people to have access to a standard mobile phone, mobile device or computer with an email address and access to a printer. This does not need to be a 'smart phone' and can be any mobile phone or tablet that can receive text messages or has access to email. Test results can be displayed on a mobile phone, tablet or other device, or a paper copy can be printed using a home printer or using a service which provides printing facilities, such as a public library.
More detail on each of the potential impacts can be found in the key findings section.
Summary of the evidence base
The summary of evidence below sets out the ways in which Covid-19 has both direct and indirect negative impacts on the children's health and wellbeing.
Direct harm from Covid
Evidence on the previous Covid-19 variants suggested that children are less susceptible and at a lower risk of severe illness compared to adults.[71] [72] Children of all ages are susceptible and able to transmit the Delta strain (B.1.617) of Covid-19[73]. It is suggested that younger children transmit Covid-19 at a lower rate. Data has also shown children aged between 1-18 years have lower rates of hospitalisation, severe disease requiring intensive hospital care, and death than all other age groups.[74] Most children do not develop symptoms when infected with the virus, or they develop a very mild form of the disease[75].
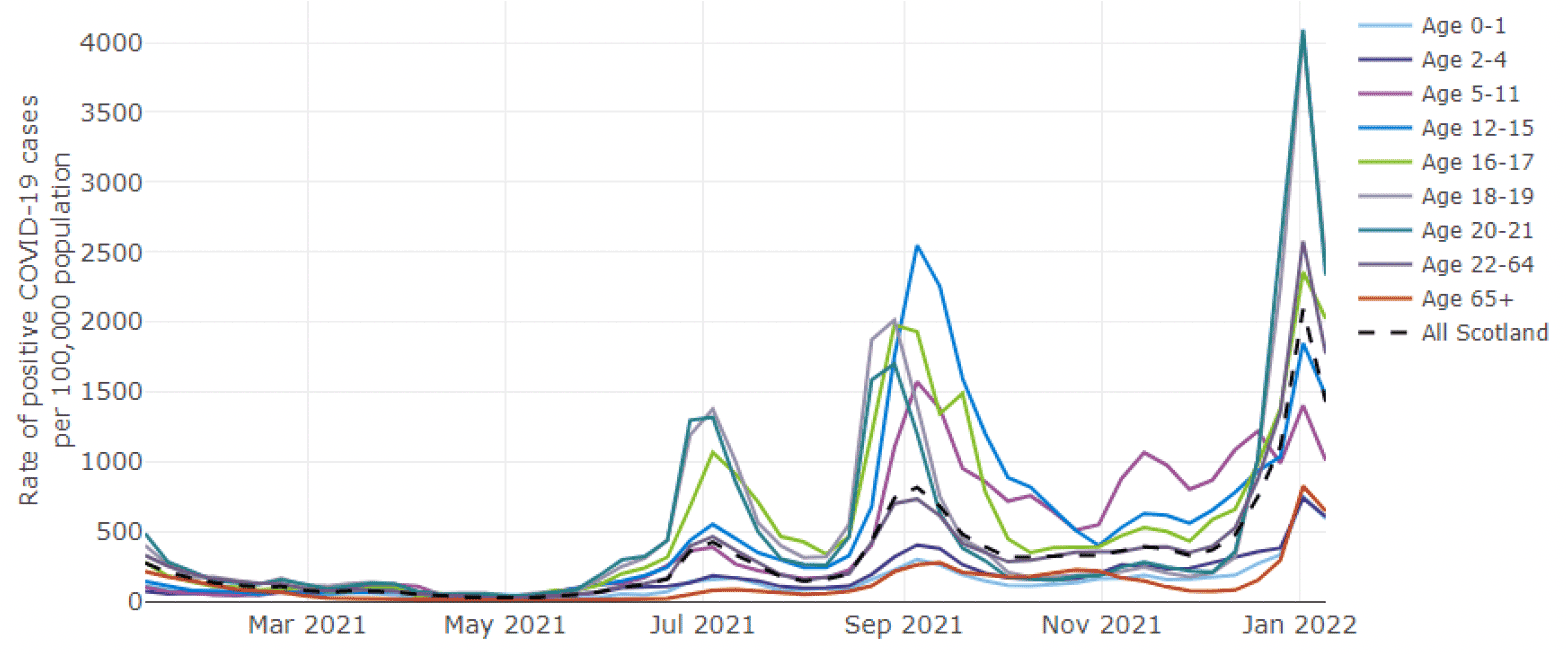
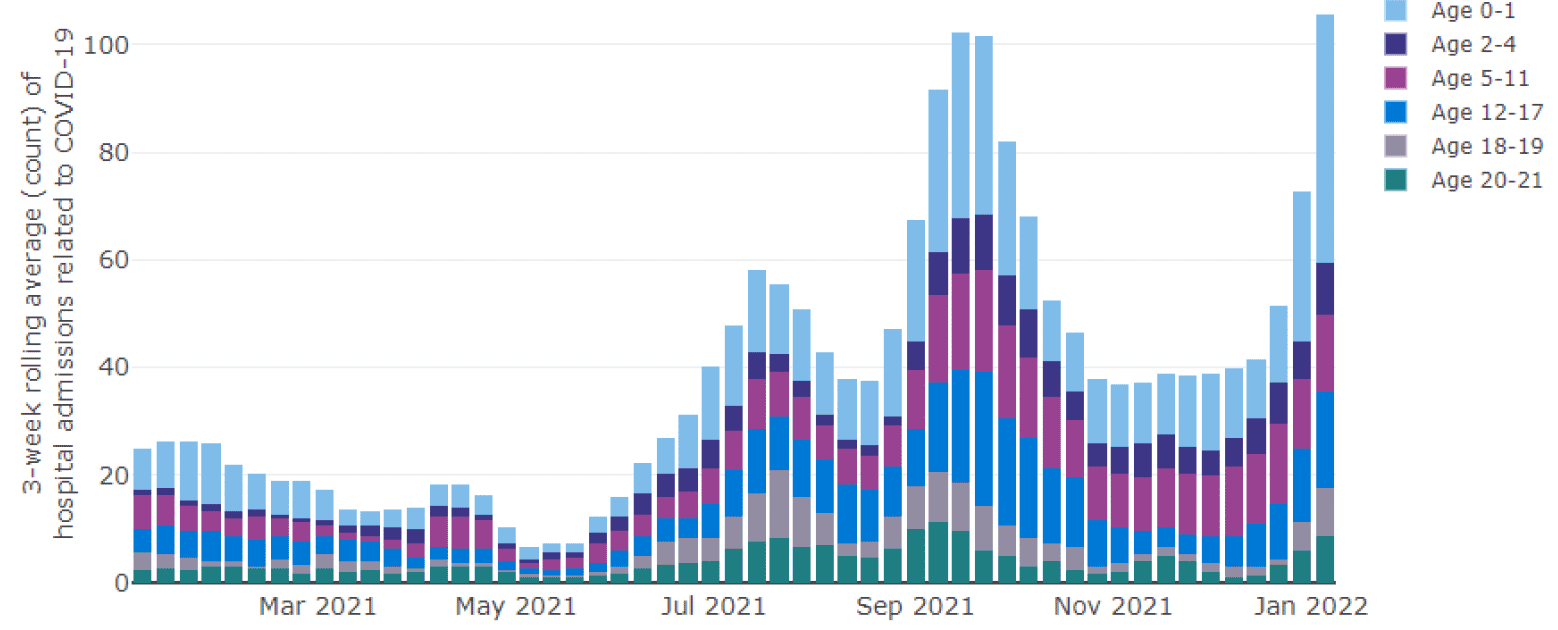
Since Omicron was detected in the UK, we have seen an increase in cases and hospital admissions, including in children (see Figure 1 and Figure 2). Cases increased sharply during late December and early January but showed a decline in the week ending 9 January 2022 (however, caution must be taken due to change in testing policy)[76]. Average hospital admissions (three-week rolling average) related to Covid-19 in children have continued to increase overall in the week leading up to 5 January 2022 compared to the previous three-week period leading up to 29 December 2021. The biggest increases in three-week rolling average were seen among those aged 0-1[77]. The number of paediatric admissions with COVID-19 infection began to rise from 26 December 2021, from an average of 40 admissions per day to 120 per day, a 3-fold rise in 2 weeks, with the most rapid change in children under 5, especially those under 1[78]. In the week to 3 January 2022, the largest increase in case rates in those under 22 occurred among those aged 0-1, with the case rate more than doubling in a week.[79]. In the week to 9 January 2022, those aged 12-15 and 16-17 continued to have a higher seven day case rate than the Scotland average[80].
Recent data considered by SAGE suggests that, compared to Delta, there does not appear to be a reduction in hospitalisation risk for Omicron in younger children (under 10 years old) though there is no indication of an increase in serious disease. In the very youngest (under 5, and particularly under 1-year olds), there appears to be an increase in the proportion of cases attending hospital compared to past waves. It is noted that this data is based on small numbers and is affect by epidemic phase bias, this was also noted in the early data from South Africa[81].
The UKHSA have designated infection severity in children as amber with low confidence in their risk assessment for Omicron, citing insufficient data to "compare the risk of hospitalisation between Omicron and Delta, and to assess the clinical nature of the illness in children"[82].
The South Africa government, the UKHSA and the Royal College of Paediatrics and Child Health (RCPCH) have made observations that the majority of children in hospital who have tested positive for Covid-19 are sick from a different illness or are not severely unwell[83] [84] [85]. SAGE noted with the recent data on Omicron in children that "For the small number of children who do attend hospital, the length of stay is typically short and where they stay overnight it is often to allow for screening for other infections" [86]
Source: PHS COVID-19 Education report (shinyapps.io).
Source: PHS COVID-19 Education report (shinyapps.io)
Evidence suggests that adults and children with learning disabilities have markedly increased risks of hospital admission and death from Covid-19, and that this is particularly high for those with Down's syndrome and cerebral palsy.[87] On 19 July 2021, the Joint Committee on Vaccination and Immunisation advised that children aged 12-15 with specific disabilities and health conditions should be offered the Covid-19 vaccination[88]. On 1 September, the advice was extended to include a 3rd dose (separate to the booster program) to those aged 12+ who are severely immunosuppressed[89]. On 3 September, vaccination was recommend to all children aged 12-15[90]. On 22 December 2022, the JCVI recommended primary vaccination of 5 to 11 year olds in a clinical risk group (as defined in the Green Book), or who are a household contact of someone who is immunosuppressed. JCVI also recommended a booster for those aged 16-17 and those aged 12-15 who are in a clinical risk group, who are a household contact of someone who is immunosuppressed children or who are severely immunosuppressed and have had a third primary dose[91].
People from minority ethnic groups in Scotland face significant societal and health inequalities and the pandemic has exacerbated existing health and wider inequalities. They are almost three times more likely than white groups to contract Covid-19 and five times more likely to experience serious outcomes. Evidence suggests this is largely due to social inequalities such as housing, occupational risk and access to healthcare.[92] Black, Asian or mixed-race children had a lower proportion of Covid-19 tests and higher proportion of positive results, Asian children were more likely to be admitted to hospital with confirmed Covid-19 and Black and mix-raced children were more likely to remain in hospital for 36 hours or longer, all relative to white children.[93]
Long Covid
On 22 July 2021 the Office of National Statistics (ONS) developed a short report on long Covid for SAGE. The report states that there is limited data for children, but the data available suggests that long illness duration after Covid-19 infection in school-aged children is uncommon, with around 2% experiencing symptoms at 8 weeks post infection.[94]
An ONS study investigating long Covid in children found there was no notable difference in children aged 2-11 who had any of the 12 most common symptoms 4-8 weeks and 12 to 16 weeks after infection. In 12-16 year olds, long Covid was more evident, though the percentage who still had symptoms decreased by 12-16 weeks after infection.[95] Similarly, data from the ZOE app showed that fewer than 1 in 20 children were symptomatic for longer than 4 weeks and only 1 in 50 after 8 weeks.[96]
A recent report from the Academy of Medical Science (AMS) highlights that, to date, Multisystem Inflammatory Syndrome in Children (MIS-C) is the primary Covid consequence studied in children.[97] The AMS report also shows the results from the ONS survey, dated April to December 2020, which revealed that 12.9% of UK children aged 2 to 11 and 14.5% of children aged 12 to 16 have symptoms five weeks after their first infection. Symptoms include fatigue, muscle and joint pain, headache, insomnia, respiratory problems and palpitations, severe enough to affect daily activities in a high proportion. Studies have also identified immunological differences between children that completely recovered from acute infection and those with long Covid. It is important to note that many of the symptoms of long Covid are also common in the adolescent population (e.g. fatigue, headache). The degree to which long Covid will have longer-term implications for children's health and wellbeing remains unclear.[98]
Data from another study conducted by University College London and Public Health England (PHE) in September 2021 found that 14% of children who caught Covid-19 had symptoms linked to the virus 15 weeks later (unusual tiredness, symptoms of ill health and headaches) while 7% had 5 or more symptoms.[99]
There is currently insufficient evidence to assess the impact of the Omicron variant on long Covid in children due to the time required to see the effects of long Covid.
Mental health and wellbeing
At a global level, Unicef have identified that the pandemic has raised huge concerns for the mental health of an entire generation including children and young people. Globally, 1 in 7 children have been directly affected by lockdowns and more than 1.6 billion children have lost some form of education. Mental health services for children have also been impacted with 2 out of 3 countries surveyed reporting disruption to services, increasing to 4 out 5 reporting disruption to mental health services in schools[100].
At the UK level, a PHE evidence report on mental health and wellbeing, drawing on data from the beginning of the pandemic up to January 2021, found that Covid-19 and associated interventions have likely had an adverse effect on the mental health and wellbeing of children and young people.[101] There is also increasing evidence that many children and young people are coping well overall and some have reported improvements in their mental health following the reopening of schools. Experiences vary by children and protected characteristics, with those from Black, Asian and Minority Ethnic backgrounds, those with existing mental health conditions, those with Special Educational Needs and Disabilities, and those from low-income families more likely to have been negatively affected.
A PHS study on the impact of Covid-19 on young people in April 2020 found that 39% of 11 to 12-year-olds were experiencing moderate to extreme concern about their mental health and that the impact on mental wellbeing appeared to increase with age (49% of 13 to 15-year-olds and 61% for 16 to 18-year-olds). In the follow-up survey conducted in September–October 2020 (after the schools had returned, but before the second Scottish lockdown), only 42% of respondents (aged between 11 and 25 years) strongly agreed or agreed that they felt good about their mental health and wellbeing, 23% disagreed and 15% strongly disagreed.[102]
In terms of differential impact by age, a survey of 11–25 year olds carried out between the end of March and beginning of June 2021 found that 40% of respondents agreed that they felt good about their mental health and wellbeing, while 35% disagreed.[103] In a later survey of the same age group carried out between September and November 2020 many young people discussed the mental wellbeing benefits of being able to meet up with their friends again and not being confined to their homes.[104]
Another survey and focus group with 14-20 year olds undertaken between August and September 2020 found that 9% of young people responding to the survey met clinical threshold levels for depression, 7% for anxiety, and 28% were categorised as having elevated avoidance and intrusive thoughts and behaviours in relation to the Covid-19 pandemic. The survey also found that while returning to school generally had a positive impact on wellbeing, this was also coupled with anxiety about Covid-19 related risks.[105]
The Scottish Children's Parliament survey of 8-14 year olds carried out in September 2020 found that respondents generally felt cheerful and in a good mood (64%); the largest increase in positive responses came from 12 to 14 year olds. There were significant improvements in children reporting that they often felt lonely (from 26% to 20%).[106] This was particularly so for the group of children who had reported highest levels of loneliness during lockdown 1, girls aged 12 to 14 (from 34% to 20%). Rates of worry across a range of topics including school work and 'the future' remained constant and worry about child and family health, money and exams increased post lockdown. Girls aged 12 to 14 were consistently most likely to agree that there were lots of things to worry about in their lives, whilst children aged 8 to 11 were more likely to report worrying about multiple areas than in previous surveys.
The second Covid-19 Early Years Resilience and Impact Survey of parents of 2–7 year olds carried out in November and December 2020 found that 39% of 2-3 year olds and almost a third (31%) of 4-7 year olds had a slightly raised, high, or very high Strength and Difficulty Score, indicating the presence of behavioural or emotional difficulties. Just under half (46%) of parents said that their child's mood was the same as during the initial lockdown, a third (33%) felt that it had improved, while a fifth (21%) felt that it had got worse. [107]
Children and young people's views and experiences
While no children and young people have been directly consulted on the use of Covid Status Certification domestically, we have engaged with organisations that represent their interests. The outputs of these engagements have fed into the development of the policy and mitigations and their input has been reflected in this CRWIA.
Throughout Spring 2021 we undertook initial scoping work with more than 35 equality, human rights and children's rights stakeholders on the potential impact of the domestic Covid Status Certification on children and equality groups. The Children and Young People's Commissioner Scotland, Young Scot, Youth Link, Children in Scotland and Intercultural Youth Scotland were involved in this engagement.
On 2 June 2021 the Cabinet Secretary for Health and Social Care chaired an Equality and Human Rights Roundtable on Covid Status Certification and children's interests were represented by the Children and Young People's Commissioner. A minute of the Roundtable is available on the Scottish Government website.
Throughout August we undertook further engagement and met with a number of equality, human rights and children's rights stakeholders to gain their insight on the potential impact of more detailed policy proposals.
In November we took forward three meetings with Equality and Human Rights stakeholders to understand the impact of the Covid Status Certification so far and to gain feedback on the extension of the Scheme to include testing.
We also took forward workshops in July to seek stakeholder feedback on the design and user journey of Covid Status Certification, and also to ensure that the paper alternative is as accessible as possible. The outcomes fed into the privacy notice which can be found on NHS Inform: Personal information we process, How we use your data, Your Rights. An Easy Read Version is also available. Further workshops are being set up to engage with children directly and will help in any future development of the App going forward.
A full list of stakeholders can be found at Annex A.
Evidence from a range of sources has been drawn upon to inform this CRWIA and references can be found throughout the document.
Key Findings, including an assessment of the impact on children's rights, and how the measure will contribute to children's wellbeing
A summary of the key findings is set out below. This is followed by an assessment of the potential impact of Covid Status Certification on children's rights.
- Protecting public health: this will positively impact all people, including children, and will particularly benefit disabled children, children from some minority ethnic groups and 12-16 year olds (Article 24).
- Protecting and promoting the wellbeing of children and young people in Scotland: during engagement, stakeholders recognised that Covid Status Certification could be beneficial in enabling entertainment settings, which are particularly attractive to younger people, to remain open if the state of the pandemic changes. As evidence shows, the restrictions and lockdowns had a negative impact on children's mental health, which gradually improved in line with the easing of restrictions.
- Exemption for under 18s: as the vaccine is not currently licensed in the UK for all under 12s (some 5-11 year olds) and not all 12-17 year olds have had the opportunity to receive both doses of the vaccine, this will allow them to continue to access spaces in scope. Stakeholders welcomed the continued exemption for this age group when the scheme was extended to include testing.
- Proof of age: while children are exempt from the requirement to provide proof of vaccination or record of a negative test, some may be asked to prove their age based exemption. Some children, particularly LGBT or migrant children, may not have proof of age or others may be challenged on the validity of their ID. Stakeholders felt this would most impact children who are under 18 but who look 18 or over and noted that the process of applying for a National Entitlement Card can be time consuming and inaccessible for some children and young people.
- Digital exclusion: all under-18s are exempt in the regulations from the domestic Covid Status Certification. However, some children may choose to access a record of their vaccination or register their test result. We know that digital exclusion affects some children, particularly care experienced, young carers, migrant, and children from low income backgrounds, as well as children from some minority ethnic groups. A paper Certificate can be requested by calling the COVID-19 Status Helpline on 0808 196 8565. This is free and open every day from 10:00-18:00. A test result can be registered by calling 119.
- Vaccine hesitancy: this could be exacerbated by Covid Status Certification in some communities and demographics. If so, this could impact negatively on vaccine uptake and our efforts to protect public health, which could in turn negatively impact upon children. However, the inclusion of testing as an alternative to vaccination may prevent against unintentionally embedding vaccine hesitancy.
- Exceeding the policy intention: even though children are exempt, there is the possibility that they could be refused entrance to a regulated setting if they cannot provide proof of vaccination or a record of a negative test. Additionally, even though the policy does not apply to employment, private business or third parties could make Covid Status Certification a requirement of employment. A negative test could be used as an alternative to proof of vaccination, however as an LFD test result is only valid for 24 hours testing every day could be burdensome.
- The Covid Status Certification status of parents, guardians or relevant adults: this could potentially impact on the enjoyment of a child's rights if a child is denied access to a regulated setting where adult supervision is required as their parent, guardian or carer does not have Covid Status Certification. Additionally, even though the policy does not apply to employment, private businesses or third parties could make Certification a requirement of employment. If a parent is unable to maintain or gain employment due to their Covid Status Certification status, this could impact upon the household finances and compromise their housing status or quality of life, which could in turn affect a child's enjoyment of their rights (Article 6).
- Potential for Certification to be used as a tool to exert control: as Covid Status Certification is required to access some settings, it could potentially be used as a method of coercive control, for example by taking a phone or paper Certificate from the victim. There is the potential that Covid Status Certification could be used to exert control over the relevant adult who cares for the child, which could in turn impact upon the child's wellbeing (Article 19).
The Scottish Government has found that a number of children's rights may be impacted by Covid Status Certification.
Right to non-discrimination (Article 2)
While children are exempt from the requirement to provide proof of vaccination or a record of a negative test to access the regulated spaces, stakeholders have highlighted that some children who are under 18 but who look 18 or older may be asked to provide proof of their age based exemption. While there are lots of pre-existing schemes which require proof of age for under-18s and there are schemes such as the Young Scot National Entitlement card which can act as proof of age, many children do not routinely possess or carry proof of identification (ID) and there is a risk that these children could be unfairly discriminated against.
The Children and Young People's Commissioner Scotland (CYPCS) have highlighted that the process to apply for a Young Scot National Entitlement Card can be quite difficult, burdensome and time consuming for children and young people. School administrations often support children and young people through the process and for those children and young people who are either at college or are not in school and do not have this support, the process can be even more challenging. Therefore there may be some children who look 18 and over and who are denied access to the regulated settings as they do not have ID or they are waiting long periods of time while they undertake the process to apply for and receive a Young Scot National Entitlement Card.
Stakeholders have highlighted that some groups are more unlikely to have ID than others. A joint survey of LGBTQ+ people run by Stonewall and LGBT Foundation found that nearly a quarter of trans people (24%) didn't have access to usable ID ('usable' = where the photo looks like them and the personal data matches their name and gender. Out of date ID is still 'usable' for the purposes of the survey), and 96% had experienced at least one barrier to obtaining ID. On types of ID specifically, the survey found that only 54% of trans respondents had a useable passport, and only 53% had a usable driving licence.[108] While this data does not distinguish between children and adults, there may be higher rates of LGBT children than non-LGBT children who do not have ID and as a result higher percentages of LGBT young people may be denied access to the regulated settings.
There are also other considerations in relation to proof of age. There is the potential that unconscious bias could cause enforcement of Covid Status Certification to be administered in a discriminatory manner. This is true for children as well as adults. While the possibility is low, a child could be refused access to a space where Covid Status Certification is required as the enforcer's unconscious bias could lead them to assume that the child is not using valid ID because of a protected characteristic, such as race, and deny them access to the space. There are also more subtle ways that unconscious bias could be enacted. For example while operating a system to check Covid Status Certification, employees may spot check children more frequently than others based on protected characteristics such as perceived race, gender, or disability. This is a concern that stakeholders have raised in relation to racial profiling and there is also anecdotal evidence that this has occurred and that ME adult attendees have been asked for proof of Covid Status Certification more frequently than white attendees. While children may ultimately gain access to the setting, the experience of feeling singled out could cause distress, a loss of time, distrust in Covid Status Certification, and anxiety about future use.[109] [110]
There is also the risk that Covid Status Certification exceeds the policy intention and while children are exempt, they could be denied access to the regulated spaces. There is also the possibility that businesses or third parties could use Certification voluntarily and deny access to children who do not have proof of vaccination or a record of a negative test. Stakeholders explained that accessing community spaces for young people remains an issue, Certification could create a new barrier to accessing spaces and services. A negative test could be used as an alternative to proof of vaccination, however as a LFD test result is only valid for 24 hours, testing every day could be burdensome. We also know that some groups of children are more digitally excluded than others and as a mobile phone, tablet or other device which receives texts or emails is required to receive a record of a test, there may be some children who are unable to provide proof of vaccination or a record of a negative test.
Therefore, unless mitigations are put in place, Covid Status Certification could potentially impact upon children's right to non-discrimination and exacerbate inequalities. Evidence suggests that those who face discrimination have poorer mental health and so if Covid Status Certification was used, even in a limited way, to enact discrimination, then this would be contrary to the promotion of children's wellbeing.
As a mitigation, sectoral guidance has been developed to support effective implementation consistent with our policy aims. This provides more information to the sectors where Covid Status Certification is mandated and the reasonable implementation, enforcement and handling of exemptions, including clarity on the exemption for all under 18s. The sectorial guidance can be found on the Scottish Government website. We have also produced public guidance to provide information on what Covid Status Certification is, the policy objectives, where it is regulated and why, the steps to attain Covid Status Certification and details of exemptions including in relation to all under 18s.
More information on mitigations to prevent the potential engagement of Article 2 can be found in the mitigations section of this document.
The best interests of the child (Article 3)
The best interests of children have been central in the policy development of Covid Status Certification. If the policy objective to reduce transmission and to increase the protection of people using specific settings are achieved, this would positively impact children, as any reduction in transmission of the virus would positively impact on the protection of public health, including the protection of children's health. As laid out in the summary of evidence, disabled children and children from minority ethnic groups are most likely to benefit from a reduction in transmission due to their poorer health outcomes if the contract the virus. Children aged 12-16 may also benefit slightly more as some evidence shows that long Covid is more evident in this age group than the 2-11 age group 4-8 weeks after infection.
We also know that social interactions, both with friends and wider family, play a key role in optimising children's development and their wider wellbeing. In answers to the Lockdown Lowdown 2 survey of 11–25 year olds (carried out in September to November 2020)[111] and in associated focus groups[112] carried out in October and November 2020, many young people discussed the benefits to their mental wellbeing of being able to meet up with their friends again and of not being confined to their homes. Therefore if the policy objective is achieved and the risk of transmission is reduced, allowing higher risk settings to continue to operate as an alternative to closure or more restrictive measures, Covid Status Certification could positively impact on children's wider development, promote their wellbeing and more generally be within their best interests.
Covid Status Certification may be particularly beneficial to promoting the wellbeing of some children. Evidence suggests that girls and young women had worse wellbeing outcomes than boys and young men throughout the pandemic. Gender differences were patterned by age and were generally more pronounced among the older age groups. The Lockdown Lowdown 2 survey cited above found that male respondents were substantially more likely to agree that they felt good about their mental health and wellbeing (59%) than female respondents (34%).[111] The Teen Covid Life 2 survey of 12–18 year olds found that a higher percentage of female participants (56% for those aged 12 - 14, 64% for those aged 15-18) reported low mood compared with male participants (33% for those aged 12–14, 46% for those aged 15-18).[113] Lastly, in the Children's Parliament survey of 8–14 year olds girls were less likely to feel resilient at both ages 8 to 11 (58%) and 12 to 14 (54%) than boys (76% 8 to 11; 69% 12 to 14%).[114]
A survey by Family Fund carried out during March and April 2020 found that 94% of families said the health and wellbeing of their disabled or seriously ill children had been negatively affected.[115] A qualitative study of the experiences of 16 families in Scotland with children that have additional support needs and disabilities found that most families mentioned the negative impact of the pandemic on the mental health and wellbeing of their children, while some mentioned challenges with maintaining their children's regular exercise.[116]
LGBT young people have been nearly twice as likely as their non-LGBT peers (52% vs 27%) to have felt lonely and separated from the people they are closest to on a daily basis during lockdown. 68% of LGBT+ young people surveyed also reported their mental health has worsened since the pandemic began, compared with 49% of non-LGBT+ young people.[117]
Findings from engagement with young care experienced people on the impacts of lockdown found that a large majority of participants said that their mental health had become worse during the pandemic, and that they often felt worried, anxious, depressed and lonely.[118]
Therefore, if the policy objective to allow indoor leisure and hospitality to continue to operate as an alternative to closure or more restrictive measures is achieved, this is likely to particularly positively impact girls, disabled children, LGBT children and young care experienced children, whose mental health and wellbeing has been negatively impacted by the pandemic.
Life, survival and development (Article 6)
The Scottish Government has been clear that Covid Status Certification will only be required for customers and not workers and volunteers at the venue or event. If Covid Status Certification were used beyond the policy intention as a condition of employment, children's right to life, survival and development could be engaged if they are unable to gain or maintain employment due to their Covid Status Certification status. Equally, if a child's parent, guardian, carer or relevant adult's employment or financial status is impacted by their Covid Status Certification status, then this too has the potential to impact upon a child's right to life, survival and development.
Sectoral guidance has been developed to support effective implementation consistent with our policy aims. This provides more information to the sectors where Covid Status Certification is mandated, and the reasonable implementation, enforcement and handling of exemptions including the exemption for all under 18s. We have also produced public guidance to provide information on what Covid Status Certification is, the policy objectives, where it is regulated and why, the steps to attain Covid Status Certification and details of exemptions including in relation to all under 18s.
More information on mitigations to prevent the potential engagement of Article 6 can be found in the mitigations section of this document.
Right to freedom of association (Article 15)
The Scottish Government recognises the right to freedom of association and the democratic right to protest as well as its integral role in society. Therefore, there is an exemption for events at which individuals gather to engage in a protest or demonstration.
If Covid Status Certification were used beyond the policy intention to deny children access to spaces, then there is the potential that their right to freedom of association could be engaged. If a parent, guardian or relevant adult does not have Certification, this could negatively impact on the child if adult supervision is required to enter a space or use a service where Covid Status Certification is required or in operation. For example, a child could be denied access to a concert if they are accompanied by an adult who does not have Certification. Public guidance which provides information on what Covid Status Certification is, the policy objectives, where it is regulated and why, and the steps to attain Covid Status Certification can be found on the Scottish Government website. More information on mitigations to prevent the potential engagement of Article 15 can be found in the mitigations section of this document.
Right to privacy (Article 16)
All under-18s are exempt from the domestic Covid Status Certification scheme. However, 12-17 year olds who have been vaccinated may choose to access their record of vaccination by downloading a PDF via NHS Inform or requesting a paper Certificate by calling the Covid-19 Status Helpline. If children do choose to use the paper or PDF Certificate their right to privacy could be engaged. A privacy notice is available on NHS Inform: Personal information we process, How we use your data, Your Rights. An Easy Read Version is also available. 12–17 year olds could also choose to register a test result and provide a record of a negative test by showing an SMS or email. A Data Protection Impact Assessment (DPIA) on the introduction of testing will be published.
Stakeholders have highlighted that data matching may be an issue for some users if they choose to request a hard copy or download a PDF Certificate. Some trans children may have different names on different documents and databases. While changing personal data with a GP is straightforward, stakeholders have highlighted potential issues with systems and data interoperability; data may be correct on one system but has not been updated on another and so could result in mismatches. This could create a more burdensome process for trans children and may mean they spend more time interacting with healthcare services and the helpline to ensure their data is consistent. Additionally, trans children may not want to call the helpline and explain their personal medical history to an unknown call handler.
Once a child has obtained a record of their vaccination, stakeholders have highlighted the risk of discrimination and distress if their name is displayed on the paper or PDF Certificate. For example, if someone's name on their medical records – and therefore on their paper or PDF Certificate – is different to the name that they use with their friends, family and others, this could lead to their transgender identity being unintentionally disclosed. LGBT young people are already fearful of disclosing their identity – 'coming out' – and 77% of young people believed their sexual/gender identity was a causal factor in their rejection from home.[119] The inclusion of testing as an alternative to vaccination reduces the risk that a person's transgender identity is unintentionally disclosed as any name can be registered with the testing portal and there is no verification of name or identity. A child can therefore use their chosen name if this is not the name listed at their GP or on their identity documents.
For some, there are real concerns regarding the right to privacy and the sharing of data. Stakeholders have informed us that migrants with secure, insecure and illegal immigration status have specific concerns that their data could be shared with the Home Office and impact their immigration status.[120] This is founded on historic experience of NHS data being shared with the Home Office.[121] Evidence shows that the majority of documented migrants that are recent entrants to the UK do not register with a GP, despite relatively easy access to primary healthcare.[122]
Protection from violence, abuse and neglect (Article 19)
As Covid Status Certification is required to access some settings, it could potentially be used as a method of coercive control. This could be done by taking a phone or paper Certificate from the victim. There is the potential that Covid Status Certification could be used to exert control over the relevant adult who cares for the child, which could in turn impact upon the child's wellbeing.
Throughout lockdown services received reports of children being exposed to increased levels of abuse and noted the impact of the perpetrator's psychological abuse and monitoring behaviours on the non-abusive parent.[123] The most consistent finding throughout the period of lockdown related to abuse perpetrated via child contact. Domestic abuse via child contact took a number of forms including perpetrators using telephone and video-call contact with children to monitor victims and perpetrators using the Covid-19 restrictions as a justification for increased contact.
Right of children with disabilities (Article 23)
As stated in the summary of evidence, disabled children are disproportionately impacted by Covid-19.
As of 13 September 2021 there are 1,431 under-16s on the clinically extremely vulnerable list (previously known as 'shielding'), although we do not have disaggregated data about the number of disabled children who are on it. While not all of those at highest risk are disabled, and not all disabled people are at highest risk, some disabled people are considered to be at high risk of health harms if they contract Covid-19, such as children with learning disabilities.[124] While not all disabled children were asked to shield, and shielding ended on 1 August 2020, anecdotal evidence from stakeholders suggests that concerns about contracting the virus have remained and many individuals and families have continued to behave as if they are still shielding, which has had an adverse impact on their quality of life.
A recent poll conducted by Disability Equality Scotland found that 82% of respondents had no concern about the Covid Status Certification scheme. Views on the scheme were mixed. However, some respondents perceived it as reassuring and a way to improve participation in society for those at risk.[125] Some respondents would like to see Covid Status Certification extended to more settings. Inclusion Scotland also noted anecdotal evidence that some carers would like to see Covid Status Certification extended to more settings as they felt the risk of attending settings where Covid Status Certification is not in place is too high and as a result the people they care for have been acting as if still shielding.
Public insights polling has found that 53% of those surveyed agreed that the high level of people with two doses of the vaccine in Scotland gives them more confidence to go out and about[126] and 29% of respondents agreed that, it they wanted to go to a venue or event, having Covid Status Certification in place would make them feel more comfortable doing this, with little difference between men and women (men 30% vs women 28%).[127] Caring is a highly gendered sector and women are disproportionately represented. Covid Status Certification could therefore provide reassurance for disabled children, their families and carers, and support them to feel safer and more confident participating in society. This could also positively impact on their mental health and wellbeing if they feel less anxious entering spaces where Covid Status Certification is in place.
Disabled children's mental health and wellbeing has been impacted by restrictions and lockdowns. Survey data from families with disabled or seriously ill children found that 94% of respondents said that the health and wellbeing of their child had been negatively affected by restrictions and lockdowns.[128] Other evidence found that respondents reported negative effects of lockdown restrictions, with 61% reporting a reduction in physical activity levels and over 90% reporting a negative impact on mental health (including poorer behaviour, mood, fitness and social and learning regression).[129] The pandemic has also had an impact on the parents and carers of disabled children: survey results found that 86% of respondents had higher stress levels than expected population norms; 82% of parents felt the Covid-19 pandemic had also affected their other children; 67% of parents reported their child's sibling to be having issues with their sleep; and 59% reported feelings of anxiety. It also found that 4 in 10 parents reported that their quality of life, and that of their disabled child, was worse in the last month, with 5 in 10 parents reporting the same for their other children.[130]
Lastly, if the policy objective is achieved and allows indoor leisure and hospitality settings to continue to operate as an alternative to closure or more restrictive measures, and disabled children are still able to attend the regulated settings with family, friends and support groups and services, this too could have positive impacts on disabled children as socialisation plays a key role in promoting wellbeing.
Right to health and health services (Article 24)
If the policy objectives to reduce the risk of transmission and reduce the risk of serious illness and death thereby alleviating current and future pressure on the National Health Service are achieved, this would result in a higher level of community protection and would positively impact upon children's right to health and health care services. Disabled children and children from some ME communities are most likely to positively benefit from a reduction in transmission, as evidence shows that these children have poorer health outcomes if they contract the virus. Children aged 12-16 may also benefit slightly more as some evidence shows that long Covid is more evident in this age group than the 2-11 age group 4-8 weeks after infection.
Covid Status Certification could provide reassurance to children, as those around them are vaccinated or have received a negative test result, and so they are less likely to contract and spread the virus to family and friends. This could support them to feel safer and more confident participating in society. Evidence has found that 45% of 11-25 year olds surveyed were concerned about catching coronavirus and 64% of respondents were concerned about transmitting coronavirus to others.[131] There is also evidence that young carers had higher levels of concern about catching and transmitting COVID-19.[132] Findings from Who Cares? Scotland[133] found similar results and focus groups[134] reported that young carers spoke about being particularly cautious going out and attending school in order to protect people they provide care to.
In terms of mental health and wellbeing during the pandemic, a PHE report found experiences vary by children and young people's characteristics, with those from Black, Asian and Minority Ethnic (BAME) backgrounds, those with existing mental health conditions, those with Special Educational Needs and Disabilities, and those living in low income families were more likely to have been negatively affected.[135] A different report found that LGBT+ respondents reported lower emotional wellbeing before and during lockdown compared with heterosexual respondents.[136] Who Cares? Scotland found that a large majority of participants said that their mental health had become worse during the pandemic, and that they often felt worried, anxious, depressed and lonely.[137] Lastly, consistent findings across a number of surveys and most questions found that girls and young women had worse wellbeing outcomes than boys and young men overall.[138]
Multiple surveys have found that children's mental health has gradually improved as restrictions eased. For example, in a survey of 11–25 year olds carried out between September and November 2020 many young people discussed the mental wellbeing benefits of being able to meet up with their friends again and not being confined to their homes[139], and in survey a parents of 2–7 year olds carried out in November and December 2020, 79% of parents said that their child's mood was the same or had improved since the initial lockdown.[140]
As such, if the policy objective of allowing indoor leisure and hospitality settings to continue to operate as an alternative to closure or more restrictive measures is achieved and children are still able to socialise and attend the regulated settings with family, friends and support groups and services, then this could positive promote their mental health and wellbeing. This could particularly positively impact girls, children from ME groups, LGBT, disabled and care experienced children whose mental health was more negatively impacted by lockdowns.
However, the policy may have unintended negative health impacts on some communities which are already less likely to come forward for vaccination. Survey data from UK-wide research suggests that, in comparison to White British and White Irish participants, Black African and Mixed Black African health and social care workers were less likely to have been offered a vaccine and much more likely to have declined vaccination if offered. Reasons for doing so among Black African participants included distrust in Covid-19 vaccination, healthcare providers and policymakers.[141] Uptake by the White Polish community is also comparatively much lower.[142]
Stakeholders raised concerns that the introduction of Covid Status Certification could exacerbate vaccine hesitancy in some communities, which could negatively impact on the objectives of the scheme[143]. Stakeholders also felt that as parents and guardians are influential figures in children's lives, children may hold the same sentiments as their parents and may also become less likely to take up the vaccine.
On 23 November, 51% of 12-17 year olds had their 1st dose[144]. There were large differences by ethnicity group with uptake ranging from 60.4% in Asian ethnic group, 57.7% in mixed/multiple and 57.2% in white, to 42.7% in African ethnic group and 39.6% in the Caribbean or Black group[145].
As stated throughout this document, even though they are exempt, children could be denied access to spaces and services as they are unable to provide proof of vaccination or a record of a negative test or if they are unable to provide proof of their age based exemption. The experience of being denied access to a space could negatively impact on a child's wellbeing. Additionally, if there is unconscious bias while enforcing Certification, as detailed under right to non-discrimination (Article 2), then this too could negatively impact on a child's mental health and wellbeing if it results in them feeling discriminated against and ostracised from friends, peers and society more widely.
Right to an adequate standard of living (Article 27)
The Scottish Government has been clear that Covid Status Certification will only be required for customers and not staff or volunteers at the premises or event. If Covid Status Certification were used beyond the policy intention as a condition of employment, children's right to an adequate standard living could be engaged if they are unable to gain or maintain employment due to their vaccine or testing status. Equally, if a child's parent, guardian, carer or relevant adult's employment or financial status is impacted by their Covid Status Certification status then this too has the potential to impact upon a child's right to life, survival and development.
Sectoral guidance has been developed to support effective implementation consistent with our policy aims. This provides more information to the sectors where Covid Status Certification is mandated, and the reasonable implementation, enforcement and handling of exemptions including for all under 18 year olds. We have also produced public guidance to provide information on what Covid Status Certification is, the policy objectives, where it is regulated and why, the steps to attain Covid Status Certification and details of exemptions including for all under 18s.
More information on mitigations to prevent the potential engagement of Article 27 can be found in the mitigations section of this document.
Right to education (Article 28)
The First Minister has been clear that the education and wellbeing of our children are paramount and should be prioritised above all else during the pandemic. As such, education is out of scope and Ministers have been clear that Covid Status Certification should not be used to access education.
However, we know that education occurs outside the classroom and other more formal teaching structures and can take place at societies and other social groups, such as those operated by or affiliated to students unions, colleges and universities. We have made clear that Covid Status Certification would not be a barrier for accessing public services and educational settings would be out of scope of the scheme, however we recognise that some organisations may choose to operate a voluntary scheme. Typically students from Scotland are slightly younger on average when they start university than students from the rest of the UK, due to differences in the school systems. Some students will be 17 when they begin university in September and might not turn 18 until February. A few students may be 16, as it's possible to attend university in Scotland without doing the final year of school (S6). While student unions across the UK, including Scotland,[146] have expressed their opposition to certification in educational spaces, individual students may choose to implement it at societies or social groups, for example, if certification is a condition of accessing a student run language café. If a student is unable to participate in societies or social activities as they do not have proof of vaccination or a record of a negative test then this could potentially impact upon their right to education and their right to development (Article 6).
More information on mitigations to prevent the potential engagement of Article 28 can be found in the mitigations section of this document.
Right to leisure, play and culture (Article 31)
There is a strong recognition that play and social interactions with friends and wider family plays a key role in optimising children's development and wider wellbeing. If the policy objective to allow indoor leisure and hospitality to continue to operate as an alternative to closure or more restrictive measures is achieved, this could positively impact on a child's right to leisure and to access cultural events if they are still able to attend the regulated settings with family, friends and support groups and services.
As previously explained, the Covid Status Certification status of a parent, guardian or relevant adult could impact upon the child's enjoyment of their rights in a number of ways. In terms of the right to leisure, play and culture, Covid Status Certification could cause negative impacts if a parent is denied access to a regulated setting where adult supervision is required and as a result the child is denied access too. A negative test could be used as an alternative to proof of vaccination. However, it is possible that that a relevant adult has neither proof of vaccination nor a record of a negative test, or that their test is no longer valid as it has exceeded the 24 hour limit.
As with many other rights assessed, even though they are exempt, there is the potential that private businesses and third parties could use Covid Status Certification beyond the policy intention and deny access to children. Children could therefore be denied access to leisure, play and cultural spaces if they do not have proof of vaccination or a record of a negative test, or they cannot provide proof of their age based exemption. This could negatively impact on their enjoyment of Article 31.
Sectoral guidance has been produced on the Scottish Government website to support effective implementation consistent with our policy objectives. Public guidance which provides information on what Covid Status Certification is, the policy objectives, where it is regulated and why, the steps to attain Covid Status Certification and details of exemptions including for all under 18s can be found on the Scottish Government website.
More information on mitigations to prevent the potential engagement of Article 31 can be found in the mitigations section of this document.
Mitigations
Mitigating actions
The Scottish Government considers that, subject to the below mitigations being implemented, where Covid Status Certification does engage rights, it does so in a proportionate way in order to protect public health.
Recognising that some people face barriers to taking up the offer of vaccination.
Embedding inclusion and equalities in vaccination programmes: our aim is to deliver our vaccinations in a way that ensures no-one is excluded, in particular those most at risk from COVID-19. The offer of COVID-19 vaccination will remain open to those newly eligible, or those who have not yet taken up the offer of a vaccine for the initial programme and the booster programme. The Inclusive Vaccine Programme includes targeted outreach and tailored communications e.g. Public Health Scotland and third sector partners have ensured the provision of a range of translated materials, British Sign Language (BSL) and other resources, such as the Covid-19 vaccine NHS Scotland explainer video, to ensure that everyone is able to access this information. Engagement with stakeholders is ongoing, including through individual meetings, to ensure opportunities to raise issues of concern. More information on the inclusive Vaccination Programme can be found in Scotland's autumn and winter vaccination strategy: progress report and accelerated delivery plans - December 2021 - gov.scot (www.gov.scot).
Inclusive testing programme: we know that some people cannot be vaccinated for legitimate reasons or have not yet taken up the vaccine. Initially, Covid Status Certification did not include a negative test result as an alternative to proof of vaccination as we considered that it would not be appropriate and could undermine one of the initial policy aims of the scheme: to increase vaccine uptake. Based on the latest evidence, and a balance of harms, Covid Status Certification now includes the option of providing a record of a negative test, with test results valid for 24 hours, as an alternative to proof of vaccination.
Exemptions: there are limited circumstances where a person may not yet have been vaccinated or may be unable to be both vaccinated and tested for legitimate reasons. For this reason, there are exemptions in the regulations for under 18s, those who cannot be both vaccinated and tested, and those participating in vaccine trials. Incorporating exemptions into the domestic App so that they appear as a green tick is under consideration for a future release.
Increasing accessibility
Paper Certification: in order to ensure Covid Status Certification is accessible to all and to mitigate against digital exclusion, which is higher among older people, disabled people and some minority ethnic groups. We have translated documents that explain what is shown on your Covid Status Certificate into different languages and formats, including Easy Read, audio and Braille.
The Covid-19 Status Helpline: to ensure that those who do not have digital access have a route to request their vaccination record. The helpline is also be available for people who cannot verify their identity on the App. The Covid-19 Status Helpline is free and open every day from 10:00-18:00 on 0808 196 8565.
A Resolver Group: has been established by NHS National Services Scotland to resolve any reported inaccuracies in vaccination records and wider issues relating to acquiring Covid Vaccine Certificate. Any requests for support can be escalated through the Covid-19 Status Helpline.
Communications and marketing: the implementation of Covid Status Certification is being supported by a range of communications and marketing resources and activity to help people understand where the scheme has been introduced, for what purpose and how to gain certification. This will provide information about identifying and avoiding scams and phishing attempts, and will take the opportunity to reinforce messaging that vaccination data will not be shared with the Home Office or impact on immigration status, unless shared by the data subject themselves (e.g. when they go on holiday) or in exceptional circumstances when required by law. It will also provide information on and raise awareness of schemes like the Proof of Age Standards Scheme (PASS) and the Young Scot National Entitlement card.
We are building on learning across other materials, such as the Covid-19 Vaccine Explainer animations, and are currently developing a Covid Status Certification Summary Information Sheet which will include key messages and guidance on how to access translated information about Covid Status Certification. This Summary Sheet takes into account conversations with minority ethnic and seldom heard audiences and will address their specific concerns, such as data collection, usage and privacy. The Summary Information Sheet will be created in multiple languages and accessible formats.
Data protection and privacy
Data Protection Impact Assessment (DPIA) and Privacy Notice (PN): these are created to ensure that all data is managed, handled, processed and destroyed in line with UK GDPR legislation, data protection laws and data ethics best practice as well as human rights legislation. The PN will support users to understand how their data is being used throughout these processes, emphasising protection of their data and ensuring government is being open and transparent. The Privacy Notice is already online and can be found on NHS Inform: Personal information we process, How we use your data, Your Rights. There is also an Easy Read Version.
Domestic App: within the NHS Scotland Covid Status App there is the function to access Covid Status Certification for domestic use. This only shows the QR code and the user's name can be hidden. When the QR code is read by the NHS Scotland Covid Check App it simply shows a green tick or 'Certificate not valid'. This mitigates against disproportionally engaging an individual's right to privacy (Article 8 ECHR: right to respect for private and family life). Individuals can create separate profiles for international and domestic use using different email addresses. If an individual wishes to use a different name domestically, and has photo ID in that name, they can create one account for international travel, which aligns with the details on their passport, and one account for domestic use, which aligns with their preferred name. The App can only host one account at a time, so if the user has two accounts under different names they will need to log in and log out to access the desired account.
Biometric identification software: Jumio, the company providing the software, state that their software has equal rates of success across all demographics with a matching rate of over 91%. For the other 9% there will be a manual check by Jumio staff to verify the user's identity. Work is underway to provide an alternative to biometric identification to register for the app. Work is also underway to add other forms of identity to the IDV scheme.
Supporting implementation in line with our policy aims
Sectoral guidance: to support effective implementation consistent with our policy aim, we have provided information to the sectors where Covid Status Certification is mandated on the policy and regulations, and the appropriate implementation, enforcement and handling of exemptions. Updated guidance can be found on the Scottish Government website.
Ministers have been clear that Covid Status Certification will not be a requirement for public services or other settings that many people have no option but to attend such as retail, public transport, health services and education. We recognise that some businesses, outside the regulated settings, are asking people for evidence they have been fully vaccinated as a condition of entry or as a condition of employment. We have emphasised in our guidance that businesses which are not covered by the Government's scheme would need to consider carefully their approach, in accordance with obligations under all relevant laws including data protection, the Equality Act 2010 and human rights. For more information see the Equality and Human Rights Commission Guidance for Employers.
Public guidance: we have also updated guidance for the wider public to provide information on what Covid Status Certification is, the policy objectives, where it is regulated and why, and the steps to attain Certification. Our Guidance is clear about the settings where the use of Covid Status Certification is appropriate as a public health mitigation. It explains that the scope of the Regulations has been carefully and deliberately limited to activities where the balance of public health risk clearly outweighs other rights considerations, and is designed to respect the rights of individuals. Specific protections, applicable within the limits of the statutory scheme, have been put in place to ensure the scheme operates in a lawful manner.
Ongoing stakeholder engagement: following the implementation of Covid Status Certification we have continued to engage with stakeholders to gather intelligence on the impact of Certification. We will continue to engage with stakeholders and we will create feedback loops, building this evidence into the policy.
Exceptions: There are exceptions for premises being used for certain purposes, including worship, un-ticketed events held at an outdoor public place with no fixed entry points and certain business events that individuals are required to attend for work purposes.
Monitoring and review
Monitoring and evaluation
Any policy that engages human rights needs to meet the test of necessity and proportionality at any given time, and should be immediately removed if it is found to no longer meet that test.
The Scottish Government is responsible for monitoring and evaluating the policy. As the regulations have been laid under the Coronavirus Act 2020 there is a requirement to review the regulations every 21 days. The extent to which the policy (Covid Status Certification) is achieving the policy objectives (reduce the risk of transmission of Coronavirus; reduce the risk of serious illness and death; reduce the risk of settings specified in the scheme being required to operate under more restrictive protections, or to close; and increase the protection enjoyed by those using settings covered by the scheme and their contacts) is being monitored and evaluated in line with this requirement. Monitoring and evaluation will also provide us with further information about other positive and negative effects of the introduction of the policy. We will also continue to assess whether any less intrusive measures could be introduced to achieve the same combination of policy objectives in respect of the higher risk sectors concerned; if so, the policy will be immediately reviewed.
An overview of the range of information being used to monitor Covid Status Certification is detailed at Annex B and C.
As the regulations have been laid under the Coronavirus Act 2020 there is a requirement to review the regulations every 21 days. The Covid Status Certification provisions will expire on 28 February 2022, as with all other Covid measures under the Health Protection (Coronavirus) (Requirements) (Scotland) Amendment Regulations 2022 and The Health Protection (Coronavirus) (Requirements) (Scotland) Amendment (No. 2) Regulations 2022. If Ministers wish to extend the measures further then additional regulations will be required.
To that end, we will continue to consider the impact of Covid Status Certification on protected characteristics and our obligations under the public sector equality duty. This will include engaging with relevant stakeholders and we will publish further equality impact assessments (EQIA) if needed.
Bill - Clause
The Health Protection (Coronavirus) (Requirement) (Scotland) Amendment (No. 5) Regulations 2021
Aims of measure
- Reduce the risk of transmission of Coronavirus
- Reduce the risk of serious illness and death thereby alleviating current and future pressure on the National Health Service
- Reduce the risk of settings specified in the scheme being required to operate under more restrictive protections, or to close; and
- Increase the protection enjoyed by those using settings covered by the scheme and their contacts.
Likely to impact on
All children, but particularly on:
- Care experienced children
- Disabled children
- LGBT children
- ME children
- Young carers
- Children from low-income families
- Children aged 12-16
Compliance with UNCRC requirements
We have detailed where the provisions engage UNCRC Articles and are of the view that the mitigations we have proposed minimise any negative impacts.
Article 3: the best interests of the child
Article 6: the right of every child to life and develop to their full potential.
Article 19: protection from violence, abuse and neglect.
Article 23: the right of a child with a disability to live a full and decent life with dignity and, as far as possible.
Article 24: the right to health and health services
Article 31: the right of every child to relax, play and take part in a wide range of cultural and artistic events.
Contribution to local duties to safeguard, support and promote child wellbeing
The following wellbeing indicator is relevant:
Healthy: Having the highest attainable standards of physical and mental health, access to suitable healthcare, and support in learning to make healthy, safe choices.
Achieving: Being supported and guided in learning and in the development of skills, confidence and self-esteem, at home, in school and in the community.
Active: Having opportunities to take part in activities such as play, recreation and sport, which contribute to healthy growth and development, at home, in school and in the community.
CRWIA Declaration
Authorisation
Policy lead
Danielle Logan
Team Leader
Covid Ready Society,
Covid-19 Public Health Directorate,
Scottish Government
Date: 24/01/2022
Deputy Director or equivalent
Elizabeth Sadler
Deputy Director
Covid Ready Society,
Covid Public Health Directorate,
Scottish Government
Date: 24/01/2022