Universal Health Visiting Pathway evaluation - phase 1: main report - primary research with health visitors and parents and case note review
The Universal Health Visiting Pathway was introduced in Scotland in 2015 to refocus the approach to health visiting. This is the first report of 4 that provides findings of the National Evaluation of Health Visiting. It focuses on primary research with health visitors and parents and case note review.
1. Core and additional pathway visits
In the survey, a third (34%) of health visitors reported they had been delivering the UHVP, either fully or in part, for more than three years, around half (47%) said they had been delivering it for between 1 and 3 years and 17% for under a year. Under 1% said they were not yet delivering the UHVP, and 2% were unsure how long they had been delivering it.
Figure 1.1 shows the distribution of UHVP visits amongst health visitors who reported that they delivered the UHVP to all or most families.
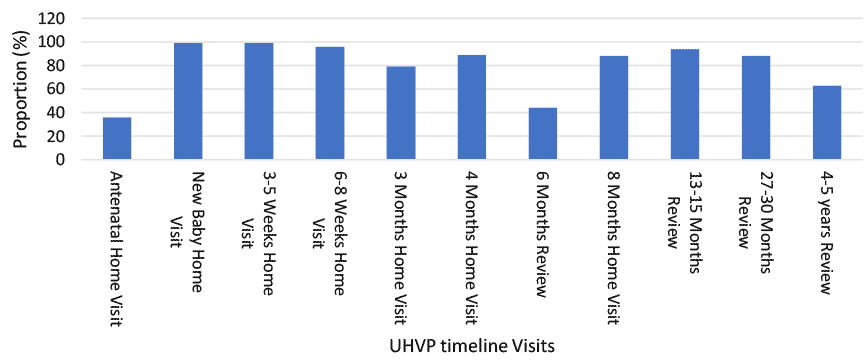
Overall, most visits were being delivered across health boards, however the antenatal home visit, 3 month visit, 6 month visit and 4-5 year review were the least likely to be rolled out at an earlier stage. However, by 1 January 2020 all Health Boards were delivering the pathway to new parents, and most were delivering all aspects of the pathway to their caseload. The pathway rollout across Scotland will be explored further in the routine data analysis implementation report.
In the qualitative research, almost all health visitors said that they had been delivering the core pathway fully or in part and that they felt that the pathway has enhanced the health visiting service. For many health visitors, the greatest value of the pathway lies in the structure and consistency it brings to the health visiting service with all families in Scotland receiving the same minimum number of visits. They believed this made the service equitable across Scotland and also made it possible to provide additional targeted support where required. This reflects the proportionate universalism concept of the pathway.
I think the timeline [or pathway] has been very good. I think it is, it has been more equitable. Do you know, people years ago, when I first started health visiting, people would sometimes see a health visitor, when the baby was born, you know at day ten, day eleven and then maybe again for a six-week check and then they would just be invited into a clinic and they might never be seen again by health visitors. So, how do you pick up concerns? So, I think it has been great from that point of view and everybody is getting the same thing. You know, so I think that is important. Some people are getting more than the timeline, because they need it but at least there is a minimum standard, so no, I think it is good. I am pro-timeline (Health visitor).
Through further exploration, it became apparent that health visitors particularly liked the frequent visits during the early weeks because they felt that parents mostly required their support during this period.
I think it’s quite nice to have the focus in the early weeks. Because that’s when most change is happening, and parents are most anxious (Health visitor).
However, a few health visitors were worried that the focus on providing support to all families meant it was sometimes challenging to support those who needed the service the most, such as children on an additional health plan indicator (HPI-A).
Core visits
There was national variation in the delivery of the various pathway visits. For instance, health visitors in the North (67%) and West (67%) Health Board Regions were more likely than those in the East (49%) to be delivering the 4-5 year review to all or most families. Those in the North were more likely to be delivering the 6 month review (53%, compared with 32% in the East). While those in the East (57%) and North (53%) regions more likely to be delivering the antenatal visit than those in the West (21%). Health visitors working full-time were more likely than those who were part-time to say they were delivering the 6-month review (52% vs 36%).
The survey further explored why some areas were not delivering some pathway visits. Personal caseload pressures (46%) and ‘My Health Board is not yet delivering all elements’ (41%) were the most common reasons provided by health visitors for not delivering all elements to all/most families. Staffing issues were reported by 12%, while 7% said they had insufficient training to deliver the pathway. It’s important to highlight that almost half of health visitors in areas not delivering some pathway visits cited workload pressures, and this could be an indication that health visitors workload may require review.
Those in the East (76%) and North (71%) Health Board Regions were much more likely to report personal caseload pressures as a reason than those in the West (29%), while those in the West were more likely to report that their Health Board was not yet delivering all elements of the pathway (58% versus 18% of those in the North and 10% of those in the East).
Antenatal visit
The antenatal visit can be regarded as a unique visit in the pathway as it is the only visit in the UHVP timeline that takes place before birth. In consideration of this, we explored the importance of this visit with health visitors and parents.
Health visitors delivering the antenatal visit considered it a crucial visit because it facilitates relationship building with families. This was consistently reported by health visitors across all Health Boards in the qualitative research. Health visitors explained that the antenatal visit provides an opportunity to establish trusting relationships with families by getting to know families within the prenatal context and being able to ease parental concerns about what will happen following the birth of a child. Health visitors also indicated that undertaking the antenatal visit helps to save time during the primary home visit, because a lot of information had already been provided to parents.
I think even with the antenatal visit, obviously the ladies are getting to meet us before the baby’s even born which I think is very beneficial because they know who’s going to be coming out when the baby is born. Then obviously the primary visit and then the weekly visits up until six weeks really gives us a chance to get to know the families, not just the mum, but the dad if there is a dad, other children, again which allows…it lets us get to know the [mother], you know, her presentation so if we go into a visit and we think, mmm, she doesn’t really seem herself today, allows us to quickly identify issues or potential mental health problems or anything (Health visitor).
Parents’ views were similar to those of health visitors. Parents reported that the antenatal visit is an important first meeting as it provides an opportunity to meet the health visitor and know who they are before the birth of the baby. They explained that this was helpful and made subsequent visits after the birth of the baby less stressful.
Because I got to meet [HV] before it and she gave me some information, she gave me leaflets to read. She just introduced herself and it was nice to meet her beforehand, so you knew who was coming to your house when you had your new-born. It was less stressful knowing who it was coming rather than meeting someone for the first time with a baby (Parent, first time).
Another important benefit that some parents noted was that the antenatal visit offered health visitors the opportunity to observe the physical and psychological state of the mother during pregnancy, therefore any deterioration in their health or wellbeing after birth could be identified and appropriate support provided.
I think just getting to meet her before [the birth], l think it did impact on…because she’d seen us before so she knew…she was able to see if there were changes in us, if that makes sense. Like mental health wise, because obviously that is quite a big and important thing after you’ve had the baby, so it was nice to see like what I was like before having a child and she knew that I was just the same (Parent, first time).
Despite the outlined benefits of the antenatal visit, health visitors mentioned that in some areas it was often the visit to be removed from the pathway timeline if they needed to prioritise workloads (Figure 1.1 reflects this). Some health visitors also mentioned that parents do not often take up the offer of antenatal visit. This seemed to mainly be the case for health visitors working in one particular Health Board and it was noted that that the opt-in approach of the letter for this visit could be responsible. However, lack of uptake was also reported as being common amongst parents where this was not their first child, some of whom felt the antenatal visit would not be necessary. Health visitors believed there was a benefit here for maintaining engagement with families identified as requiring additional support. In some cases, health visitors coupled antenatal visit with scheduled visits to older siblings in families who were already in receipt of the pathway at this point.
When I contact people to say, “hi my name is…I’m your health visitor and we have our universal pathway and part of that is an antenatal contact, so would you want me to come to visit you?”. Some people think it’s a waste of time, quite a few people have declined that contact. I think it’s beneficial if people engage with you but obviously if they don’t want to, they think they’re seeing the midwife and that’s sufficient at this point in time. It can [also] be because they’ve had two or three children previously, so they know what it’s all about or the other side of that is it could be someone in their professional role who feels they can’t afford the time to allocate to see somebody else, they already make appointments with the midwife. So because of work commitments, they feel they don’t want to see somebody else, because it’s going to be another appointment that they have to attend (Health visitor).
It appeared from both individual interviews and focus groups with health visitors that in some areas within a Health Board, the uptake of antenatal visit was initially low, and this was attributed to the nature of the opt-in letter sent out to families. However, uptake seemed to have improved when an opt-out approach was adopted.
In a very deprived caseload…what we found is, when we were offering, sending out the letter: would you like us to offer an antenatal visit? There was probably ten per cent uptake. When we changed to using the letter saying, I will be your health visitor, I will visit you at home at ten o’clock on that day, should you not want this, and we are now up to probably about 89, 90 per cent of uptake (Health visitor, Focus Group).
In the case note review, it was evident in most Health Boards that the antenatal home visits were not being achieved as anticipated. This supports the qualitative findings above that it is one of the pathway visits most likely to be removed when Health Boards are struggling with capacity. Amongst the records reviewed, it was found that in HB1, five antenatal home visits (out of a possible fifteen) to five separate families were achieved and in addition there was one attempted home visit, but the pregnant woman was not at home. The two home visits achieved in HB2 (out of a possible thirteen) were both related to referrals from another service. In HB4, three visits were recorded (out of a possible fifteen), one following a referral at 17 weeks gestation. In addition, one letter was recorded as being sent. In HB5, where three home visits were achieved (out of a possible fifteen), another visit was arranged but cancelled by the pregnant woman, although another contact was achieved through a telephone call.
In the survey of health visitors, those who had been delivering the UHVP for four years or more were also more likely than those that had been delivering the pathway for a shorter time period to be delivering the antenatal visit (55%, compared with 36% overall).
Additional visits
The UHVP presents a core home visiting programme to be offered to all families by health visitors as a minimum standard. However, additional visits from a health visitor may also be deemed beneficial following a ‘Getting it right for every child assessment’ which is undertaken as routine part of the UHVP. When asked to think about families in their personal caseload identified as requiring additional visits, 43% of health visitors said that those families received all of the required additional visits, 40% said most of them, 13% said some of them and 2% said none of them. Health visitors who had been practicing for under a year were the least likely to say that all/most of the families in their caseload received the required additional visits (71% versus 83% overall).
Analysis of the case note data revealed that aside from the core visits, some families received a large proportion of additional visits, and a closer observation of the data indicates that they seem to cluster at certain points between some pathway visits. Examination of Table 1.1 using the case note review data seemed to highlight an increased number of additional visits between 3/4 month and 8 months pathway visits. Table 1.1 also shows increased additional visits from some families between the 13-15 month and 27–30-month pathway visits, and between 27-30 month and 4-5 year visits.
Additional visits appear to have taken place for a wide range of reasons, including feeding support, maternal depression and domestic abuse as can be seen in Appendix 7. It was evident that additional visits taking place up to the age of 15 months were provided to children assigned to both HPI Core and Additional indicators, whereas beyond 15 months of age, additional visits were more often provided to those assigned HPI Additional. Table 1.1 identifies the distribution of extra home visits and includes the timeframe between Pathway visits.
| Health Board | Extra visits between 6-8 week and 3-month visit | Between 3/4 month and 8-month visits | Between 8 month and 13–15-month visits | Between 13-15 month and 27–30-month visits | Between 27-30 month and 4–5-year visits |
|---|---|---|---|---|---|
| HB1 | 4/15 total cases (27%) | 3/15 total cases (20%) | 4/15 total cases (27%) | 5/10 total cases (50%) | 5/9 total cases (55%) |
| (2 Core; 2 Additional) | (2 Core; 1 Additional) | (2 Core; 2 Additional) | (3 Core; 2 Additional) | (2 Core; 3 Additional) | |
| HB2 | 5/13 total cases (38%) | 4/13 total cases (31%) | 4/13 total cases (31%) | 4/10 total cases (40%) | 1/2 total cases (50%) |
| (2 Core; 3 Additional) | (1 Core; 3 Additional) | (1 Core; 3 Additional) | (1 Core; 3 Additional) | (1 Core; 0 Additional) | |
| HB3 | 2/15 total cases (13%) | 3/15 total cases (20%) | 7/15 total cases (47%) | 7/9 total cases (78%) | No case records reviewed |
| (2 Core; 0 Additional) | (2 Core; 1 Additional) | (2 Core; 5 Additional*) | (2 Core; 5 Additional*) | ||
| HB4 | 2/15 total cases (13%) | 3/15 total cases (20%) | 4/15 total cases (27%) | No case records reviewed | No case records reviewed |
| (1 Core; 1 Additional) | (2 Core; 1 Additional) | (2 Core; 2 Additional) | |||
| HB5 | 6/15 total cases (40%) | 9/15 total cases (60%) | 5/13 total cases (38%) | 4/9 total cases (44%) | 1/5 total cases (20%) |
| (3 Core; 3 Additional) | (4 Core; 5 Additional) | (2 Core; 3 Additional) | (1 Core; 3 Additional) | (0 Core; 1 Additional) |
* due to the large number of extra visits undertaken every visit date was not collected
Pathway schedule
During the interviews and survey, it emerged that parents and health visitors both had concerns about some of the gaps in the pathway schedule. Health visitors universally highlighted two main gaps: the gap between the four to eight-month visits; and the gap between 13-15 month and 27-30 month visits.
After the pathway visit at four months, there is a six-month review, which is not conducted as a home visit but as a record update only, according to the pathway.
Both parents and health visitors felt that the gap between four and eight months was particularly important because it is during this period that weaning (introduction of complimentary foods) typically begins. The WHO, UNICEF and the UK Scientific Advisory Committee on Nutrition recommend that introduction of nutritionally-adequate complementary foods should begin after six months.
Weaning was noted to be one of the greatest sources of parental anxiety, especially for first time parents. There are challenges associated with introduction of solid foods and inappropriate foods can lead to longer term health implications, including malnutrition, unhealthy weight, obesity and tooth decay. Health visitors said they are expected to educate parents about weaning at the four-month visits, yet they are keen to avoid promoting weaning at this stage. Health visitors felt that providing weaning information to parents at four months and encouraging them to begin weaning at six months is challenging and creates confusion for some parents. This is discussed further below in the Infant Weaning section under Impact on parental understanding, choices and behaviour [theme 3].
Health visitors also described a perceived gap between the 13-15 month and the 27–30 month visits. Both of these visits are when child health developmental reviews take place. They felt it was possible they were missing opportunities to identify important developmental concerns within the intervening time period.
At one year if they don't speak it doesn't mean anything, but if they are not speaking by 18 months it means a lot. And you don't see them at that time, you don't see them until they are 27 months, therefore yes, you are late, you are very late in making a referral (Health visitor).
Yeah, I definitely think rather than maybe like the thirteen to fifteen month [visit], I think a visit around eighteen months would be more appropriate because they likely would be walking and they would be reaching a lot more of their milestones like their kind of language development would be kind of you know, a lot better as well. But as I say we don’t see them until they are twenty-seven months unless they are an additional family (Health visitor).
Health visitors explained that a child unable to meet a developmental target at 13-15 months could be a source of worry for parents. While it is possible that the child could attain that particular developmental goal within a few months, the next scheduled visit is not until the 27-30 months. However, parents can contact their health visitor at any time.
I think perhaps the 13-15-month [visit] could be delayed slightly to 18-months. Just I think a lot of the children when you visit at 13 months, on the ASQ forms, are not walking, are not getting from a sitting to a standing position. That puts a lot of parental anxiety into the interaction between us and the parents. So, I feel that if we waited to perhaps, even instead of 13-15 months, if we incorporate it at 15-18 months, that would be a better age group to deal with, rather than the earlier and putting that anxiety onto the client (Health visitor).
Data from the case note review (Table 1.1) supports the concept that there is gap in contact with health visitors around 6 months which is when health visitors advise children should be weaned onto solid foods. It is apparent in this data that there is an increased number of additional visits when children are around 6 months and this may be due to requests by parents for additional help or advice at this time. Similarly, Table 1.1 shows increased number of additional visits between the 13-15 month and 27–30-month visits, which may also reflect parents request for help or advice around during this time. It appears these identified gaps in the pathway are problematic and might require attention to enhance parents’ experience of the UHVP. Addressing the issue of the gaps might also help address the increased additional visits health visitors provide out with the pathway schedule.
Contact
Email: Justine.menzies@gov.scot