Coronavirus (COVID-19): Scotland's Strategic Framework update - November 2021
We expect a challenging winter ahead and know that the effect of the COVID-19 vaccine reduces over time. It is within the context of these pressures, and the risk of increasing COVID-19 cases, that this update of the Strategic Framework sets out our latest approach to managing the pandemic.
Overview
This update to our COVID-19: Strategic Framework (last updated in June 2021) sets out progress against the range of strategies being deployed across government and the broader public sector in Scotland in response to the coronavirus pandemic and explains our approach to the future management of the pandemic.
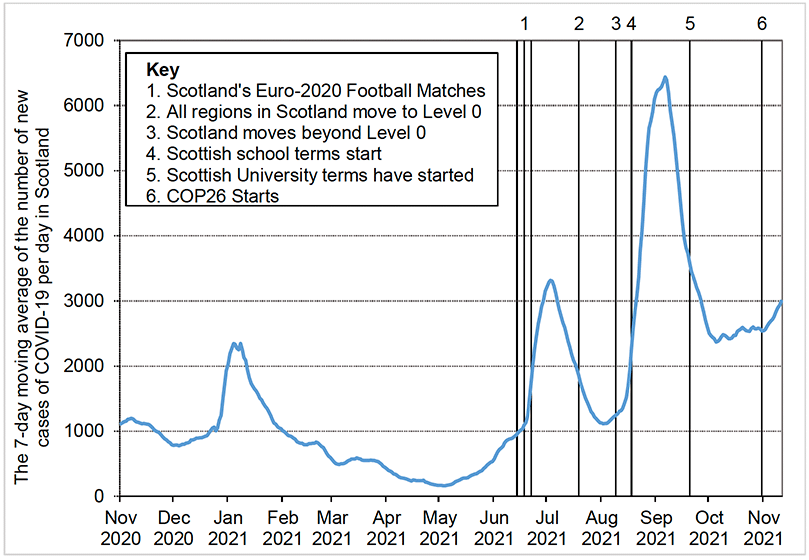
The June publication followed a period of declining incidence of the coronavirus in Scotland as shown in Figure 2. This decline reflected our managed exit from lockdown during the first half of 2021, as increasing vaccination coverage permitted a greater easing of restrictions while keeping the virus suppressed.
By June 2021, it was clear that the Delta variant was going to dominate other variants of the coronavirus, with its increased transmissibility contributing to rising case rates. However, it was also clear that the positive effect of the vaccine had fundamentally changed the balance of harms associated with the pandemic: the relationship between infections and serious health harms had weakened significantly compared to earlier stages of the pandemic. Serious health harm continued but at much lower levels for a given number of cases than in the past. Meanwhile, broader harm to the economy and wider society also continued, and though these harms had been considerably alleviated by fewer restrictions, certain sectors continued to be severely affected, including those unable to operate at all. This fundamental adjustment in the balance of harm, brought about through vaccination, underpinned our shift in strategic intent from one of suppressing the virus to the lowest possible level to one of suppressing the virus to a level that was consistent with alleviating the broader harms of the virus.
In late June and early July, cases in Scotland spiked, peaking at just over 3,900 new positive cases per day. A key factor likely associated with this spike was increased socialising across Scotland around the time of Scotland's participation in the (delayed) Euro 2020 football championships (with three matches on 14, 18 and 22 June 2021). At this time, most of Scotland remained in Levels 1 or 2 in terms of restrictions.
Following Scotland's exit from Euro 2020, the combination of protective measures in place, fairly high population immunity (from both vaccine coverage and prior infection) and the scheduled closure of educational settings for the summer holidays (alongside other factors such as warmer temperatures, the Test and Protect programme and the degree of adherence to protective measures) was sufficient to reduce case numbers again without an increase in restrictions. This was significant as it was the first time that there had been a sustained reduction in cases without an escalation of non-pharmaceutical interventions (restrictions). Daily cases had fallen to 1,865 (7-day average) by 19 July, at which point Scotland generally moved to Level 0 restrictions (some island communities already having been in Level 0). This was the lowest level within the levels system of protective measures but still maintained certain restrictions including in high transmission-risk settings. In addition, physical distancing requirements were also reduced (to 1 metre in all indoor public settings and outdoors).
New positive cases continued to fall, to around 1,132 (7-day average) by the end of July. However, it is likely that the move to Level 0, alongside wider factors present at the time (including the dominance of Delta, the reduction in physical distancing requirements and potentially some relaxing in adherence to the remaining rules), had tilted the balance in favour of renewed growth of the virus, although case numbers and wider harms at the time remained manageable.
Consistent with our revised strategic intent, and recognising the broader harms of restrictions both economically and socially, the Level 0 restrictions and remaining physical distancing requirements were lifted, as planned, on 9 August. At this time, the number of cases (7 day average) was 1,245 (and the 7 day rate of positive cases per 100,000 population, by specimen date, was 159). Several important baseline measures were retained in law to control and prevent future growth of the virus including:
- mandatory face coverings in indoor public settings and on public transport (with some exemptions);
- attendance limits on large events (with exceptions, where approved);
- collection of contact-tracing details in some settings; and
- having regard to guidance to reduce transmission risk.
The combination of the lifting of Level 0 restrictions, which enabled the re-opening of venues such as nightclubs and the general return of full stadia and large events, together with the return of schools (11-19 August) and with potential reductions in adherence, likely contributed to the rapid escalation in case numbers observed during August. Cases reached a record high of 7,525 on 2 September (and the 7-day moving average peaked at 6,439 on 6 September). Due to the effect of the vaccine in weakening the link between cases and serious health harm, the impact on hospitalisation and mortality from this peak was correspondingly lower, but still significant. The growing number of therapeutics to treat COVID-19, mainly in hospitalised patients, were also helping to manage the severity of symptoms.
Although some increase in case numbers had been considered plausible following the easing of Level 0 restrictions, it was expected that increasing immunity and adherence to the baseline measures in place would curb any increase. This expected reduction in cases – without the need for further restrictions – subsequently took place, with 7-day average cases falling back below 2,400 at the start of October.
The decision not to re-impose restrictions to curb the August surge in cases was an example of one of the very difficult balancing acts that many governments have faced during the pandemic, given the various harms involved. Following this decision, cases reduced significantly (more than halving from their peak) without the re-imposition of restrictions and their associated harm for business, educational and other settings.
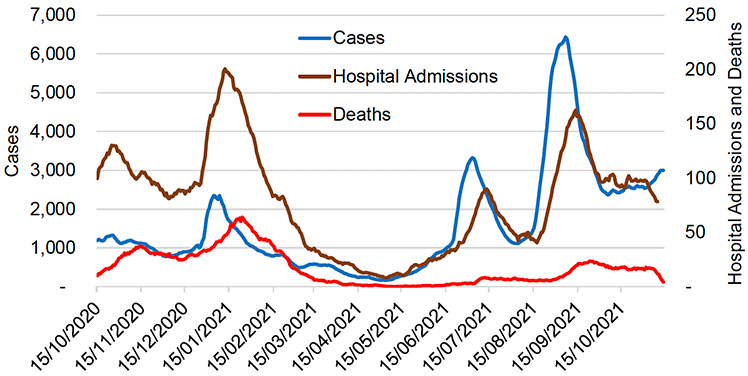
However, the surge in cases translated into a high level of COVID-19 hospital admissions (peaking at over 150 per day) and COVID-19 bed occupancy at a time when hospital pressures were already significant. Figure 3 shows that, even with the increased protection from vaccination, higher case numbers translated into higher admissions and to an increase in COVID-19 deaths, though neither reached the levels seen in early stages of the pandemic in Jan 2021 and April 2020.
Reflecting these conflicting harms, the June 2021 Strategic Framework Update described how a 'gateway condition' for lifting Level 0 restrictions had been set of double vaccinating the over 40s age groups. This was specifically done to address the balance of harms as we knew that most (but certainly not all) COVID-19 deaths occur in the over 40s and we judged that waiting to fully vaccinate the entire (adult) population before lifting Level 0 restrictions would likely have imposed disproportionate economic and social harm. By the end of July 2021, all over 40s were offered a second dose, and 94.2% had taken up that offer ahead of the lifting of Level 0 restrictions on 9 August.
From recent experience it is clear that increasing immunity, or reducing susceptibility, to the virus is able to exert pressure on COVID-19 case numbers as – even where that immunity is only partial - it becomes more difficult for the virus to spread. In essence, immunity from COVID-19, whether full or partial, comes in two ways – from vaccination or from infection (or from both, where vaccinated individuals have also been infected, or vice versa).
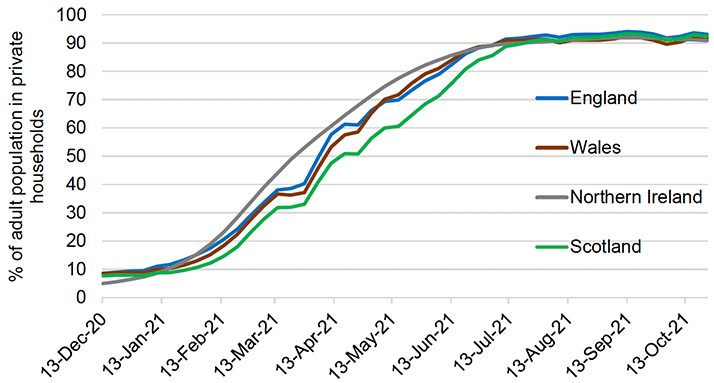
Antibody data indicate that Scotland's population now has a very high level of COVID-19 antibodies, particularly among adults. (See Figure 4 below). This is in large part because of the success of the vaccination programme, with over 82% of the total eligible (12+) population (and 88% of the adult population), now double vaccinated as of 15 November. However, it is important to increase still further the proportion of adults and young people who have been vaccinated, to ensure that as many are protected as possible – and we will continue to strive to do this.
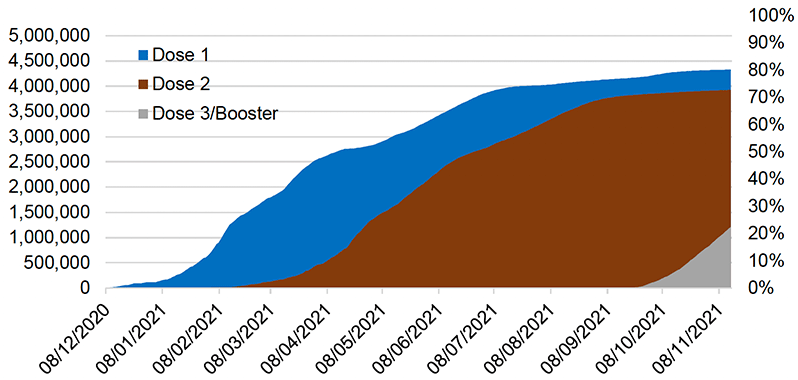
Eligibility for vaccination has been expanded since the last Strategic Framework Update. On 4 August 2021 the JCVI issued advice recommending vaccination for all 16 to 17 year olds and on 13 September 2021 the four UK Chief Medical Officers provided advice on a 'one dose' offer of vaccination for all 12 to 15 year olds. Good progress has been made in providing first doses to these groups (certain individuals within these groups are eligible for two doses). On 15 November 2021 the JCVI advised broadening the offer of a COVID-19 booster to 40 to 49 year olds, and offering all 16 to 17 year olds who are not in an at-risk group a second dose of the Pfizer vaccine. Further take-up of the vaccine across the eligible population will help to increase downward pressure on the virus. Figure 5 shows vaccine coverage by day.
The level of antibodies in the population will not naturally remain fixed at some high level. There is growing evidence that the antibodies from vaccination may reduce over time. This is important because there may be a positive correlation between the level of antibodies and the degree of protection a person has from the virus. A reduction in antibodies may reflect waning immunity, particularly as the protective effect of vaccinations appears to reduce to some degree over time. We are continuing to learn about this effect with Scottish research groups contributing significantly to global understanding here.
To address waning immunity, it is important to provide booster vaccinations for eligible people. These 'boosters' are being offered to: people living in residential care homes for older adults; frontline health and social care workers; all adults aged 50 years or over; adults aged 16 to 49 years with underlying health conditions that put them at higher risk of severe coronavirus; adult carers (aged 16 or over); household contacts (aged 16 or over) of immunosuppressed individuals. So far take-up has been strong. As of 15 November, 1,208,387 people had received a booster vaccination or their third primary vaccination. Following JCVI advice on 15 November, people aged 40 to 49 will also be offered a booster vaccination and will be able to book their appointments soon.
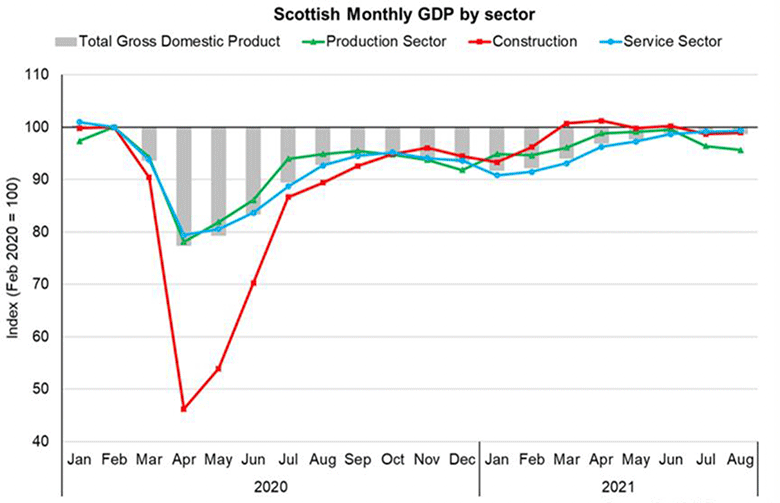
The careful, staged lifting of restrictions in Scotland has enabled the gradual re-opening of the economy and broader society. There are no longer any restrictions requiring the closure of particular business or other premises, which is important, not least given the end of the UK Government's furlough scheme. Whilst overall economic output in Scotland, as measured by Gross Domestic Product (GDP), has returned almost to its pre-pandemic level, as shown in Figure 6, consumer facing services sectors, such as hospitality, remain notably below pre-pandemic levels. Labour-market indicators, including the unemployment rate, are similarly near their pre-pandemic levels but the re-opening of the economy has led or contributed to specific challenges in the labour market, such as staff shortages in some sectors.
We will continue to engage with the Convention of Scottish Local Authorities (COSLA), local authorities, trades unions, other regulators and business organisations to ensure that compliance with COVID-19 regulations and guidance is maintained in business and event settings and we will continue to promote, across sectors, tools to increase understanding and to promote good practice.
Source: Scottish Government
All of our schools, further and higher educational establishments and early learning and childcare settings are able to open, though all continue to operate with some protective measures in place. Depending upon the setting, such measures might include a focus on hygiene, ventilation, vaccination, the use of face coverings, and asymptomatic testing.
Despite facing significant challenges, we are continuing to build on the approach to recovery and renewal set out in our NHS Recovery Plan. Our health and social care services are under more pressure than at any point in the pandemic and the situation is likely to get worse as we move into the winter months. This is why the NHS will remain on an emergency footing until at least 31 March 2022. Our immediate priority is to continue to prepare the NHS for and support staff through the pressures they will face in the coming months, including normal winter illnesses, weather issues, and any further resurgence of COVID-19. We recently announced a package of measures,[6] [7] backed by additional recurring funding of more than £300 million, which demonstrates our commitment to having a well-staffed, well-supported and resilient health and social care system. This is in addition to more than £1 billion of targeted investment to help the NHS recover.
With the lifting of restrictions and the broad-based recovery that we are now witnessing even in the face of evident challenges, the economic and social harms caused by COVID-19 today are much reduced compared to earlier stages of the pandemic. However, a range of harms that accumulated during earlier stages continues to be acutely felt. These include bereavement; those suffering from the long-term mental and physical health effects of the pandemic, including 'long COVID'; the backlog of non-COVID-19 health treatments; disrupted education; higher levels of debt; and lost jobs, livelihoods and businesses.
Our COVID Recovery Strategy has set out how we intend to alleviate many of these harms. It will be a long-term challenge but we are fully committed to a better, fairer and greener Scotland emerging as a legacy of the pandemic.
Work is underway to establish a COVID-19 public inquiry for Scotland by the end of this year. Once set up, the Inquiry will operate independently of the Scottish Government. We are committed to supporting a full and transparent review of handling of the epidemic in Scotland and learning lessons for the management of future crises.
Like many other countries, we believe that retaining a limited number of baseline measures (such as wearing face coverings in public indoor spaces and on public transport) is essential for controlling the virus, particularly over the coming winter. We keep such measures under ongoing review as we know that they continue to affect education and business and wider activity.
On balance, we currently judge that any inconvenience and drawbacks these measures cause is outweighed by their benefit in reducing transmission of the virus and the health, social and economic harms that follow from that. These measures include the vaccine certification scheme for certain higher transmission-risk settings in Scotland. We see this as an important measure to help to reduce direct health harm from COVID-19 while enabling affected businesses to continue operating. We view this as a temporary measure and, as with other legal measures, we will keep it under review to ensure its coverage is appropriate and to remove it when it is no longer necessary.
Continued strong adherence to these measures is required to maximise their effectiveness in helping to control the virus and thereby reducie the likelihood of needing further restrictions, though they remain a contingency.
We fully intend for some measures put in place to tackle COVID-19, such as improved ventilation and testing, to become part of the 'new normal' – as they will be of economic and social as well as public-health benefit in the long term and will support the better, fairer Scotland that we all want to see. They will also help to manage COVID-19 as it moves from the acute phase of the pandemic in Scotland to becoming endemic.
Contact
Email: CEU@gov.scot