Citizens' Jury on QCovid: Report on the jury's conclusions and key findings
Ipsos Scotland was commissioned to conduct a Citizens' Jury exploring views on QCovid®. QCovid® is a risk model developed to identify people at the highest risk of death or a poor outcome should they catch Covid-19. This report documents the Citizens' Jury process and findings.
5. Public-facing tool
Summary and key principles
The public-facing tool is an online tool which could be used by the general public. With this tool, an individual would enter their data into an online form to view their own risk score, which would be generated using the QCovid® model. A public-facing tool had not been deployed anywhere in the UK at the time of research.
In session two of the Citizens' Jury, members heard from an expert speaker (Professor Alison McCallum from the University of Edinburgh) who introduced the public-facing tool, explaining how it would work and what the key considerations would be for its use. Following exploration, Q&A, and discussions in session two, participants deliberated on the public-facing tool, discussing the key risks, benefits, and ethical considerations in relation to it before drawing their conclusions on what would make use of the tool acceptable or unacceptable. Over the course of deliberation, views on the public-facing tool remained mixed. This was the tool that met the most criticism from participants, with some saying that the risks (particularly the lack of accessibility, susceptibility to misuse and perceived lack of support that would be available) outweighed the benefits.
"The only people that would use it are people who are following the rules and are interested, and are more engaged to begin with, or people trying to game the system, to get a low score, and use that as a justification. I don't think it would help the people it's intended to help. How I perceive risk, and the actual risk, are different things."
(Participant in session 2)
The jury concluded that the use of such a tool in Scotland, as part of the QCovid® model or a similar risk model, would only be acceptable if:
- There is sufficient support in place to help people understand their risk score.
- It is accessible (e.g. alternative formats – language translations, large print, braille or text to speech, and simple language).
- There are alternative ways of accessing the score for those who are not online or who require additional support.
- There is clear, simple guidance for using the tool to reduce the risk of misuse, and there are consequences for misuse along with a way to report suspected misuse.
- The tool is kept up to date in case of people moving from low risk to high risk (and vice versa) based on new evidence or changing circumstances (including in relation to the virus e.g. a new variant).
Reflecting the generally negative sentiment towards this tool, there were more issues identified to render the tool unacceptable than was the case for the others.
The jury concluded that the use of the public-facing tool in Scotland would be unacceptable if:
- There is not adequate support in place to help people understand their score.
- It is introduced on its own (without the clinical tool being available).
- There is no alternative for people excluded from using an online tool.
- The information an individual inputs can be accessed and/or used by anyone else.
- Identifiable information is requested and/or stored.
- It doesn't reach everyone who needs it i.e. exacerbates inequalities.
- There is any obligation for people to pass on information about their risk score.
- It cannot be guaranteed that the data put in is accurate.
- Note that the group who deliberated this final "red line" recognised this would not be plausible without a medical professional present, at which point it becomes the clinical tool. They therefore suggested changing the intended use of the public-facing tool to maintain intentions of empowerment but reduce the risk e.g. using the score from a clinician, provided using the clinical tool, to input onto a public-facing tool that provides information about actions that should be taken and how to access support.
Risks and benefits
As part of their deliberation on the public-facing tool, participants considered the risks and benefits of it, as well as any key ethical concerns.
The key risks identified were that:
- There is a potential lack of immediate emotional support for people finding out their score. This was deemed to pose a significant risk to peoples' mental wellbeing, particularly when presented with a high risk score.
- It could be difficult for people to interpret their score and understand what it means for them. There was a sense that this could lead to problematic behaviours when receiving a low or high risk score.
- People may input incorrect information about themselves and get an incorrect score. It was felt among participants that this could be done deliberately or by accident, which would undermine the usefulness of the tool.
- It could be misused to get a score for someone else. For instance, there was one view that an employer could enter information on behalf of an employee which could result in the employee being treated differently.
- The online tool is not accessible for all groups in society and might not be used by those who need it. Not having accessible formats was considered to be 'discriminatory' and it was felt that those most likely to benefit from the tool would be least likely to use it, thus widening existing inequalities.
- The information put into the tool could be hacked. Although over the course of the jury participants were reassured that the QCovid® public-facing tool would not store any data, this remained a concern for some.
The key benefits of the public-facing tool were that:
- It enables those with access to the internet to find out their score in private. One view was that most people have access to the internet nowadays and so it provides a useful alternative to the GP.
- It is publicly available. The availability of such a tool was considered to be a benefit because, if well-designed, it could help encourage action. Conversely, there was a sense that not having a tool publicly available could deny someone life-saving information.
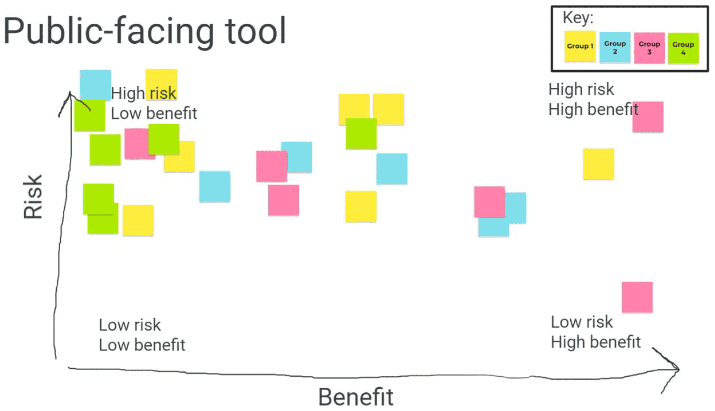
On balance, the jury concluded that the public-facing tool presents a number of significant risks and there remained mixed views on the benefits. This is depicted in figure 4 overleaf, where participants each placed a digital post-it according to their own assessment of the risk-benefit of the public-facing tool.
Key ethical considerations
Having learned more about the public-facing tool, the jury discussed the ethical considerations for QCovid® being deployed in this way. These concerns remained prevalent throughout the jury's deliberation and formed the key principles underpinning the possible use of a public-facing tool in Scotland.
Availability of support
The availability of support to help people understand and deal with their risk score was the most prominent issue for participants when considering the ethical issues with the public-facing tool. The type of support participants discussed were:
- Emotional support, particularly when receiving a high risk score.
- Interpretative support to help people understand what their score means.
- Practical support to help people take appropriate action based on their risk score.
It was generally felt that receiving a risk score online would have potentially harmful impacts on peoples' mental wellbeing, particularly if being informed that they are at high risk from Covid-19. There was consensus that the risk score would also be subjective and that people would interpret their score in different ways.
"If it's a good result.. it might make people too confident. 'Oh, I am fine even if I get it' attitude. Even it's not affecting you personally, you can still spread it and I feel like, if they get a good result, it doesn't matter if I get it when you can really affect other people. But if you get a bad result, it can badly affect your mental health and if you do talk to friends and family, it could worry them. It could cause panic or worry in general."
(Participant in session 2)
Therefore, they felt that a public-facing tool would need to have immediate support available to help people interpret their score and consider their options. For some, this led to the conclusion that the clinical tool would be the most effective way to ensure that people received their score in a supportive environment.
"There is too much uncertainty and risk. Risk of putting people under stress when they don't need to be. It's a GP's job, not everyone's job."
(Participant in session 2)
For one participant, however, the perceived lack of adequate support with the public-facing tool was considered an insurmountable challenge which rendered this tool unworkable.
Accessibility and equalities
Another prominent concern was the lack of accessibility, which participants understood to be a current limitation of the public-facing tool. Without accessible options, such as language translations, large print, text to speech, or alternative formats for those who are not online, it was felt that this tool would be 'discriminatory' and would prevent some groups in society from accessing their risk score, such as disabled people, those with learning difficulties and those who are digitally excluded.
"I would assume by default it would be developed and made more user-friendly already […] Everybody should have access to it in some way. Either everybody has access or it doesn't work."
(Participant in session 2)
Participants also learned about the concept of the inverse care law, which states that those who most need medical care can be least likely to receive it.[9] This raised some concerns among members that a public-facing tool, if used on its own, would not reach the people it needed to and would therefore widen inequalities.
Deployment of the public-facing tool was considered acceptable only if accessible and alternative versions were made available.
Protecting against misuse
The susceptibility of the public-facing tool to misuse was also an ongoing concern for the jury. A common example was the potential for employers to use the tool to find out their employees' risk scores. For some, this concern was rooted in their own experiences and views of their employers' handing of the pandemic. Another concern was that people might 'game the system' for their own benefit.
Over the course of deliberation, while some questions over this were addressed by the expert speakers through the Question & Answer sessions, reassuring participants to some extent, there remained some concern about the scope for misuse, particularly among employers.
It became important to the jury that there were mechanisms to report suspected misuse and clear consequences for those misusing the tool. The jury also concluded that there should be no obligation for people to pass on information about their score to mitigate against any discriminatory treatment (for example with insurance providers).
Accuracy and security
Early in the deliberations, participants raised concerns about the accuracy of the data being input to the public-facing tool. For instance, someone could generate their risk score without full knowledge of their health status, resulting in them either taking or not taking action based on inaccurate information. This underscored the importance of ensuring that the data input is accurate, although it was acknowledged that this is difficult to control for.
It was suggested by one group that, to mitigate the risk of inaccuracy, the public-facing tool should be designed to support the clinical tool; an individual would find out their risk score via their GP and then could input their score to the public-facing tool for resources and guidance on interpreting and acting on the score.
A related issue was raised around data security. In the early stages of learning about the tools, this concern was largely based on the perception that the public-facing QCovid® tool would store data. Over the course of deliberation, with clarifications provided by speakers to reassure participants that the QCovid® tool would not store data, there was a greater sense of reassurance over data security. However this remained a risk for some participants.
"If you have a website, there is always a risk - anything that is a website open to the public is open to being closed and copied and information being taken that way."
(Participant in session 5)
Contact
Email: shielding@gov.scot