Citizens' Jury on QCovid: Report on the jury's conclusions and key findings
Ipsos Scotland was commissioned to conduct a Citizens' Jury exploring views on QCovid®. QCovid® is a risk model developed to identify people at the highest risk of death or a poor outcome should they catch Covid-19. This report documents the Citizens' Jury process and findings.
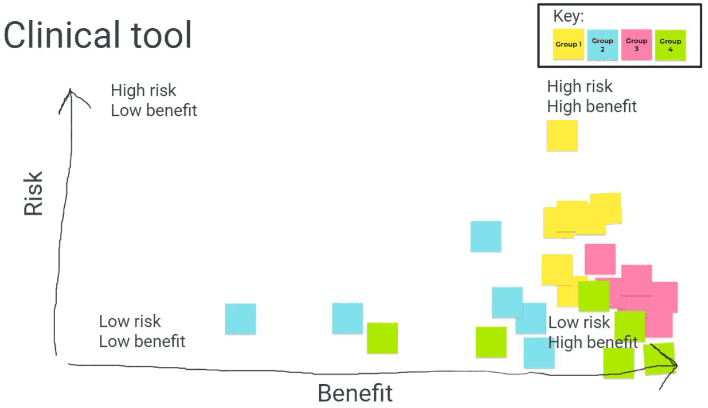
4. Clinical tool
The clinical tool is a tool which could be used by GPs (or other healthcare professionals) who would enter a patient's data into an online form to view their risk score, which would be generated using the QCovid® model. In 2021, the UK Government had developed and given GPs access to a clinical tool based on QCovid®. Participants viewed a demonstration of the tool as an example of how it would work in practice in session two, following a presentation by an expert speaker (Professor Aziz Sheikh from the University of Edinburgh) who introduced the clinical tool.
Following exploration, Q&A, and discussions in session two, participants deliberated on the clinical tool, discussing the key risks, benefits, and ethical considerations in relation to it before drawing their conclusions on what would make use of the tool acceptable or unacceptable.
Initially, participants were surprised by how much personal information was needed to get the score. They were generally positive, but also surprised that the public is not more aware of this tool already being used in England. As participants deliberated, there was some (occasional but noteworthy) confusion expressed over whether the data inputted would provide information for the QCovid® model, and some interest in whether this tool could be used in combination with the non-anonymised population tool to identify people who need support.
Nevertheless, the jury concluded that the use of such a tool in Scotland, as part of the QCovid® model or a similar risk model, would be acceptable if:
- Information is provided to explain to patients what the tool is and how it will be used.
- It is communicated why this tool is available, including via GPs (or healthcare professionals) to flag that it is available when with a patient.
- Practical and emotional support is provided to help patients according to their risk score.
- GPs (or other healthcare professionals) can help patients understand their risk score.
- GP resources are not placed under too much burden (which may involve outsourcing to relevantly trained health professionals rather than GPs).
- GPs (or other healthcare professionals) are trained to use the tool and interpret and communicate the results effectively.
- Patients have the option to ask for their score (and to refuse the option to discover their score).
- Results are confidential.
- The tool is kept up to date in case of people moving from low risk to high risk (and vice versa) based on new evidence or changing circumstances (including in relation to the virus e.g. a new variant).
The use of a clinical tool was deemed to be unacceptable if:
- It collects personal information which is not needed for the tool to work.
- The data is kept after you've received your score (although it was acknowledged that the QCovid® clinical tool does not retain data).
- If it detracts from GPs' ability to address other, more critical, health needs.
- If your score is shared with other parties (i.e., anyone other than your GP) without your consent.
Risks and benefits
Through in-depth deliberation, the key risks identified for use of this tool were:
- GP resource – participants were concerned about the burden this tool could put on GP time, and that this could take away from other priorities and ultimately not provide enough in terms of a cost-benefit assessment for public health.
- Availability of support – while participants considered a benefit to be the offer of support, they also felt there is a significant risk that the availability of support would not be able to meet demand.
- Accessibility – participants were mindful that trust in GPs varies and so this may not be an accessible tool for all. They also expressed concerns about the risks associated with visiting a GP during a pandemic (if face-to-face).
The key benefits identified for use of this tool were:
- Support – particularly in comparison with the public-facing tool, a key benefit was seen to be the availability of support and guidance on receiving the score as a GP, with a duty of care, would be present when the patient received their score (this was seen to be particularly important if the patient received a high-risk score). In comparison to the public-facing tool, participants valued the input of a medical professional who could accurately interpret the score and guide patients on what actions they should take.
- Confidentiality – participants were confident (more so than for the public-facing tool) that the information provided, if it was to be held for a risk prediction model to run, would be kept safely confidential.
- Accuracy – participants felt that GPs would have the information collected by the tool already (such as age, postcode and existing health conditions), or could ensure its accuracy while gathering it from the patient if needed, therefore making it lower risk compared to the public-facing tool (which participants largely felt could produce incorrect results). However, there was some perceived risk that not all GPs would know how to interpret the result.
- Immediacy – participants liked that the results could be produced with an immediate professional interpretation, which patients could act on.
On balance, the jury concluded that the clinical tool could be highly beneficial and that the risks are relatively low, given the presence of a medical professional. This is depicted in figure 3, where participants each placed a digital post-it according to their own assessment of the risk-benefit of the clinical tool.
Key ethical considerations
Accuracy
Participants expressed concerns about accuracy in terms of the QCovid® risk model used, given missing audiences (e.g. pregnant women and younger people) and concerns about how up-to-date the information is. They also expressed concern about the difficulty of keeping data up-to-date and accounting for the complexities of prevalence in a community when giving someone a risk score. Specifically for the clinical tool, they also raised questions and concerns about the accuracy of the information a GP currently holds on a patient, a lack of access to relevant health records (such as cancer treatments) and the implications of peoples changing health status for the accuracy of their score. Overall, it was of high importance to participants that a risk model like QCovid®, which provides a risk score, is kept up to date in order to justify using this tool, particularly in the case of Covid-19 and new variants arising.
"I could see a GP tomorrow and have a low risk, but then a new variant could come across and then I might be really high. If that data isn't getting saved anywhere, [would I] have to make an appointment to get another risk factor? Is it just wiped again?"
(Participant in session 2)
Confidentiality
It was important to participants that not only should the risk score be held confidentially in terms of data storage, but also in terms of any pressure or incentive for this information to be passed on to, or used by, other actors such as insurance companies. However, the choice should be given to patients if they want proof of risk level e.g. for their employer.
Support
Participants felt strongly that support should be in place for those informed of being high risk, and that the GP should be able to offer or direct them towards this. It was acknowledged that different levels of support would be needed; immediate emotional support for those receiving a high risk score, and also signposting to practical support for making necessary lifestyle adjustments (such as help with groceries or financial assistance). However, they were concerned this support may not be available to the extent that it would be needed by the high-risk population. Participants highlighted the potential impacts on mental health and behaviour, which underscored the importance of adequate support being in place for patients who are provided with their risk score, particularly if they are high risk.
The GP was viewed as an essential communicator in terms of helping people understand their score, and an essential provider of emotional support and practical guidance. However, there was concern over the burden that this could place on GPs and whether they would receive training on how to use the tool effectively.
"Everybody has a different perception of risk, [it] is better to have somebody with knowledge there to discuss that at the time."
(Participant in session 2)
Accessibility
Participants were mindful that trust in GPs varies and so this may not be an accessible tool for all. They also expressed concerns about the risks associated with visiting a GP during a pandemic (if face-to-face) along with broader concerns about those who would not be invited or able to make use of this tool e.g. pregnant women and younger people. They wanted a revision of this, so that access to the benefits of the tool is more open to all. They also reflected on the importance of having telephone options available rather than face-to-face in the scenarios of a new variant, high prevalence or a lockdown, in order for patients to safely utilise this tool.
Resourcing
Participants felt it important that support to correctly interpret the score, and any actions needed, be provided in order for this tool to provide its benefits, though had significant concerns about resourcing i.e. the impact on GP time and whether this would be worthwhile compared to other uses of GP time. Participants suggested widening the scope to other medical professionals (such as pharmacists), while still providing the benefits of offering support and guidance. They felt that GPs, and by proxy of the previous statement potentially other medical professionals, should be provided with training to ensure they know how to interpret the score and what support to offer.
"With the time pressure on GPs and the fact people need to make time to go to the GP to talk about it, takes the benefit down. I think there could be more benefit if you could go other places like the pharmacy. That would increase the benefit as there is more access to the clinical tool."
(Participant in session 5)
Choice
The importance of personal choice and the use of the tool being driven by a patient (as opposed to a patient simply being given their score, particularly if this could then be used to negatively discriminate against them in some way) was another ethical consideration raised by the jury. This also linked to an interest in focusing on high-risk patients in order to ease resourcing which was met with reservations as conditions and health status is not always known by the GP or could be out-of-date.
Contact
Email: shielding@gov.scot