Scottish COVID-19 Mental Health Tracker Study Wave 5 Report
This is the final report of the Scottish COVID-19 (SCOVID) Mental Health Tracker Study, covering findings for a range of mental health outcomes across all the five waves of the Study.
1. Background
1.1 Study overview and aims
The Scottish COVID-19 (SCOVID) Mental Health Tracker Study helps us to understand the impacts of the coronavirus pandemic on people's mental health and wellbeing in Scotland[2], particularly the differential impacts on sub-groups of the population. The study surveyed adults (18 and over) in Scotland at five points in time (waves) over a roughly year-long period, starting in May 2020. This report presents findings from Wave 5, the final wave of the study, which took place in June and July 2021.
This final report presents data from each wave of the study, and the report findings will aid with the tracking of mental health outcomes in the population through the different levels of restrictions.
At each wave of the study, respondents were asked to complete questions about various aspects of mental health and wellbeing. The final report presents findings about suicidal thoughts, depressive symptoms, anxiety symptoms and mental wellbeing, while the previous SCOVID reports[3] included findings concerning additional aspects of mental health and wellbeing. A narrower focus on the most common aspects of mental health and wellbeing was adopted for this report to allow more detailed examination of intersectional subgroups (e.g., young women, young men, young adults and women with mental or physical health problems).
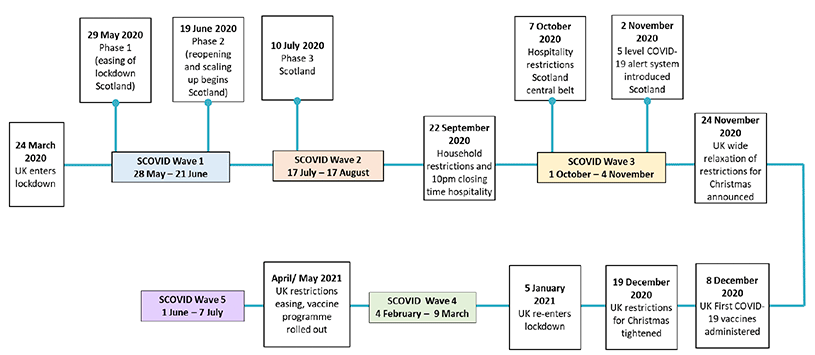
Figure 1.1 below provides an overview of key events/policy decisions for Scotland in relation to the waves of the SCOVID mental health tracker study. For details of the route map out of lockdown phases see: Coronavirus (COVID-19): Scotland's route map - gov.scot (www.gov.scot). SCOVID Waves in relation to Scotland restrictions were as follows:
- Wave 1:
- Spring 2020 (28th May to 21st June 2020).
- Coincided with the Phase 1 easing of lockdown measures in Scotland.
- Wave 2:
- Summer 2020 (17th July to 17th August 2020).
- Coincided with the Scottish Government's introduction of Phase 3 of the easing out of lockdown. Phase 3 included an increase in the number of households that could meet indoors and outdoors, and the opening of indoor hospitality.
- Wave 3:
- Autumn 2020 (1st October 2020 to 4th November 2020).
- Coincided with the increasing of COVID-19 restrictions in Scotland. Specifically, on 1st October people could no longer meet inside people's homes unless they were part of a bubble, and on 7th October restrictions on hospitality were announced.
- Wave 4:
- Winter 2021 (4th February to 9th March 2021).
- Coincided with a UK-wide lockdown that had been announced on 4th January 2021. At this point lockdown restrictions included a strict stay at home message, with all non-essential retail and services closing, including hospitality, and stringent restrictions on meeting friends and family indoors and outdoors.
- Wave 5:
- Summer 2021 (1 June 2021 to 9 July 2021).
- Coincided with the easing of lockdown restrictions across the UK. Specifically, as of 26th April 2021 shops and sports facilities opened, and some hospitality restrictions eased, and further easing was seen throughout May and June. Additionally, the COVID-19 vaccination programme was underway across Scotland. Therefore, Wave 5 represents a period of returning to normality and a decreasing of uncertainty. Wave 5 is the final wave of the SCOVID study.
Key research aims for Wave 5 of the SCOVID study:
1. To track cross-sectional changes in people's mental health and wellbeing in Scotland during the COVID-19 pandemic and changing of government restrictions. Specifically, changes in mental health and wellbeing from the initial easing of restrictions in Spring 2020 (Wave 1), and further easing in Summer 2020 (Wave 2), to the increasing of restrictions in Autumn 2020 (Wave 3), to the introduction of a UK-wide lockdown in Winter 2021 (Wave 4), to the easing of lockdown restrictions in Summer 2021 (Wave 5).
2. To investigate the mental health and wellbeing of subgroups found to report poorer mental health and wellbeing in Waves 1 to 5; specifically, young women and men, and young adults and women. Additional findings are reported for those with a pre-existing mental health condition, a pre-existing physical health condition, caring responsibilities, young dependents, or vaccine hesitancy. The aim was to identify whether these subgroups were at higher risk of poor mental health and wellbeing.
1.2 Sampling and methodology
At Wave 1, 2594 members of an existing online UK panel (Panelbase.net) participated in the first SCOVID MH tracker online survey. Recruitment quotas were set for specified population sub-groups (see Tables A-C in Annex 2 for details). All the Wave 1 participants were invited to take part in the subsequent waves, and, due to attrition, additional recruitment was conducted at Wave 3 and Wave 5[5].
The loss to follow-up over the study reduced the size of the sample of those who have completed every wave. As a result, it was not possible to conduct a robust longitudinal analysis, and so cross-sectional trends across the waves are reported instead. Therefore, the changes over the waves included within this report do not represent statistical differences. The cross-sectional samples were slightly different across the five waves of the study (including the recruiting of booster samples at Wave 3 and Wave 5): Wave 1 (n=2594), Wave 2 (n= 1703), Wave 3 (n=1625), Wave 4 (n=1288), and Wave 5 (n=1213).
The Wave 1 to Wave 5 reports[6] provide detail about each wave's cross-sectional sample, and Table D in Annex 3 provides an overview of the demographics and subgroups for each wave.
As several demographic groups were under- or over-represented in the samples at each wave, data were statistically weighted to reflect the Scottish population. This allowed for the shortfall or surplus in particular groups to be adjusted, so that the findings are more representative of the original quota sample. The weighting was based upon age, sex, and socioeconomic group (SEG) (see Annex 2, Tables A-C for details of the original quotas). A breakdown of the Wave 5 weighted sample can be found in Annex 3 (Table E1), as well as tables indicating how this reflects the Scottish population (Tables E2 and E3). The weighting methodology is identical to that employed in the previous waves for consistency. The weighted sample is used in all figures in this report, although non-weighted data is reported in the annex for comparability.
Although weighting is widely used there is still a risk of bias, as the weights may inflate or suppress the data from subgroups in the sample. The extent of the bias is dependent on the representativeness of the data collected. As the unweighted samples and their representativeness varied across the waves, this potential bias is therefore a caveat that should be kept in mind when making comparisons across the waves.
Subgroup findings
To explore the impact upon certain subgroups of the COVID-19 pandemic and subsequent restrictions, an intersectional approach was taken to understand whether an individual's age and sex increased or decreased risk of poor mental health. Review of the data shows that the following subgroups that were deemed to be at high risk for poor mental health:
- Young women,
- Young men,
- Young adults, and
- Women
Additional intersectional findings are reported for young adults and women, specifically those with a pre-existing mental health condition, a pre-existing physical health condition, unpaid caring responsibilities, young dependents (under 5 years), or vaccine hesitancy. These at-risk subgroups were investigated as they had been identified as being more vulnerable to worse mental health at the start and throughout the pandemic, as reflected within previous Wave 1 to Wave 4 reports. Further intersectional reporting for young men or young women (e.g., young women with a mental health condition) was not possible due to small numbers in these subgroups.
For each subgroup at Wave 5, additional characteristics are reported, such as socio-economic group (SEG), change in working status, key worker status, caring responsibilities, young dependents, and mental and physical health conditions. While these factors were not specifically included in mental health outcome analyses, intersections between all of these characteristics potentially influence an individual's mental health and wellbeing.
Mental Health and Wellbeing Measures
This report focuses on four mental health and wellbeing indicators: suicidal thoughts, depressive symptoms, anxiety symptoms, and mental wellbeing.
To measure suicidal thoughts, respondents were asked: 'how often have you thought about taking your life in the last week?', and were provided with options that ranged from "Never", "One day", "Several days", "More than half the days", "Nearly every day", and "I would rather not answer". For the purposes of this report, respondents who experienced any suicidal thoughts in the week prior to the Wave 4 questionnaire (i.e., one day or more) were included in the suicidal thoughts findings.
Depressive symptoms were assessed through participants' responses to the Patient Health Questionnaire (PHQ-9; Kroenke et al., 2001), which assesses frequency of depressive symptoms over the previous two weeks. For the purposes of this report, scores above the cut-off for moderate to severe depression (score 10) are reported as this suggests that treatment (psychotherapy or medication) may be recommended.
Anxiety symptoms were assessed using the Generalised Anxiety Disorder (GAD-7; Spitzer et al., 2006) scale, which asks about frequency of anxiety symptoms in the last 2 weeks. For the purposes of this report, the clinical cut-off for moderate to severe anxiety (score ≥10) was reported, indicating anxiety symptoms that may require further treatment.
Respondents' mental wellbeing was measured using the Short Warwick-Edinburgh Mental Well-being Scale (SWEMWBS)[7]. This scale measures the frequency of various thoughts and feelings over the past two weeks, such as feelings of optimism, being useful, and thinking clearly. A SWEMWBS score is created for each individual by adding together their responses to each question. The scores range from 7 (indicating very low wellbeing) to 35 (indicating very high wellbeing), therefore a higher score suggests better mental wellbeing. Throughout this report average mean scores are reported for each of the subgroups.
Layout of report
In the final report, the mental health outcomes are reported first for the overall sample, then by the subgroups that are deemed to be most at risk: young women, young men, women, and young adults. For women and young adults, a summary of the intersectional findings (pre-existing mental and physical health condition, young dependents, unpaid carer, and vaccine hesitancy) is included. Further detail for these subgroups can be found in Annex 4 and 5.
Each section will include:
- An overview of the background and health of that subgroup at Wave 5,
- Their mental health outcomes at Wave 5,
- How their mental health compares to their subgroup counterparts, and
- An overview of trends in changes in their mental health over the waves.
Terminology
This report uses particular terms to describe the mental health outcomes reported by subgroups in the overall sample. The term 'rate' refers to the proportion of respondents within a subgroup who have reported a particular outcome; it does not describe the degree of a particular outcome. For example, an increased rate of men reporting moderate to severe depressive symptoms means that a higher proportion of men have reported these symptoms; it does not mean that men as a subgroup are experiencing more severe depressive symptoms. The term 'level' refers to the degree to which a particular mental health or wellbeing measure is being experienced. For example, stating that older adults reported higher levels of mental wellbeing than younger age groups means that the average mental wellbeing score for older adults was higher than the average score for younger groups.
Contact
Email: socialresearch@gov.scot