Scottish COVID-19 Mental Health Tracker Study Wave 5 Report
This is the final report of the Scottish COVID-19 (SCOVID) Mental Health Tracker Study, covering findings for a range of mental health outcomes across all the five waves of the Study.
Annex 5: Mental health and wellbeing of each subgroup
Summary of subgroup findings
- Pre-existing mental health condition
- Across Waves 1 to 5 of the SCOVID study, people with a pre-existing mental health condition consistently reported higher rates of suicidal thoughts, depressive symptoms, anxiety symptoms, and lower levels of mental wellbeing, than people with no pre-existing mental health condition.
- At Wave 5, 27.8% of respondents with a pre-existing mental health condition reported suicidal thoughts, 59.6% reported depressive symptoms, and 54.4% reported anxiety symptoms. The average mental wellbeing score for those with a pre-existing mental health condition was 16.92, lower than the average of 22.08.
- Pre-existing physical health condition
- Across Waves 1 to 5 of the SCOVID study, people with a pre-existing a physical health condition consistently reported higher rates of suicidal thoughts, depressive symptoms, anxiety symptoms, and lower levels of mental wellbeing, than people with no pre-existing physical health condition.
- At Wave 5, 12.6% of respondents with a pre-existing physical health condition reported suicidal thoughts, 36.4% reported depressive symptoms, and 27.7% reported anxiety symptoms. The average mental wellbeing score for those with a physical health condition was 20.83, lower than the average of 22.08.
- Unpaid caring responsibilities
- Across Waves 1 to 5 of the SCOVID study, people who had unpaid caring responsibilities reported higher rates of suicidal thoughts, depressive symptoms, anxiety symptoms, and lower levels of mental wellbeing, than people with no caring responsibilities.
- At Wave 5, 17.1% of those with unpaid caring responsibilities reported suicidal thoughts, 33.9% reported depressive symptoms, and 25.5% reported anxiety symptoms. The average mental wellbeing score for those with unpaid caring responsibilities was 20.60, lower than the average of 22.08.
- Dependents under 5 years
- Across Waves 1 to 5 of the SCOVID study, people who had dependents under 5 years tended to report higher rates of suicidal thoughts, depressive symptoms, anxiety symptoms, and lower levels of mental wellbeing, than people with no dependents under 5 years.
- At Wave 5, 11.9% of those with young dependents (under 5 years) reported suicidal thoughts, 27.4% reported depressive symptoms, and 18.8% reported anxiety symptoms. The average mental wellbeing score for those with young dependents was 22.19, similar to the average of 22.08.
- Vaccine hesitancy
- Vaccine hesitancy is described as behavioural delay in acceptance or refusal of vaccines despite availability of vaccine services (SAGE, 2014). Questions about vaccine hesitancy were asked at Wave 4 and Wave 5, therefore trends are limited to these waves.
- At both waves, people who had hesitancy in taking the COVID-19 vaccine reported higher rates of suicidal thoughts, depressive symptoms, anxiety symptoms, and lower levels of mental wellbeing, than people who had taken, or planned to take, the vaccine.
- At Wave 5, 30.7% of those with vaccine hesitancy reported suicidal thoughts, 33.2% reported depressive symptoms, and 30.4% reported anxiety symptoms. The average mental wellbeing score for those with vaccine hesitancy was 19.54, lower than the average of 22.08.
- At Wave 5, those with vaccine hesitancy were more likely to have unpaid caring responsibilities, have dependents under 5, and a mental health condition; these factors place them at higher risk of poor mental health.
- Young adults were more likely to report vaccine hesitancy (12.3% of young adults, compared with 8.8% of 30-59 year olds, and 1.7% of 60+ year olds).
- Young adults with vaccine hesitancy tended to report higher rates of depressive symptoms and anxiety symptoms than vaccine hesitant 30-59 years and 60+ year olds. The exception is at Wave 5, where 60+ year olds reported higher rates of both depressive and anxiety symptoms.
- The mental health of men and women with vaccine hesitancy differed, and both reported worse mental health than men and women with no vaccine hesitancy. Women tended to report higher rates of anxiety symptoms and lower mental wellbeing than men, and men with vaccine hesitancy reported higher rates of suicidal thoughts and depressive symptoms compared with women who also had vaccine hesitancy.
A1. Mental health of people with a pre-existing mental health condition
People with a pre-existing mental health condition may be particularly vulnerable to poor mental health and wellbeing during the COVID-19 pandemic, as the pandemic may exacerbate existing issues. Worldwide evidence from the early stages of the pandemic suggests that people with a mental health condition may experience a worsening in symptoms and an impact of loneliness and social isolation on their wellbeing (Rains et al., 2021). Further, people with a pre-existing mental health condition may be more adversely affected by the pandemic than the general population, with evidence from a meta-analysis of studies from around the world demonstrating an increased risk of severe or fatal COVID-19 among patients with a pre-existing mental disorder and of lack of access to services and resources (Toubasi et al., 2021).
Across Waves 1 to 5 of the SCOVID study, people with a pre-existing mental health condition consistently reported higher rates of suicidal thoughts, depressive symptoms, anxiety symptoms, and lower levels of mental wellbeing, than people with no pre-existing mental health condition.
Looking at Wave 5 data for those with a pre-existing mental health condition:
- 27.8% of reported suicidal thoughts,
- 59.6% reported moderate to severe depressive symptoms, and
- 54.4% reported moderate to severe anxiety symptoms.
Findings from the UK COVID-MH Study (Wetherall et al. under review) suggest that respondents who reported having a pre-existing mental health condition had consistently higher rates of suicidal thoughts, depressive symptoms, anxiety symptoms, defeat, entrapment and loneliness compared with those with no pre-existing mental health condition, and similarly wellbeing scores were lower for this group.
Overall trends in the SCOVID study suggest that young adults and women with a pre-existing mental health condition may be at increased risk of poorer mental health than their age and sex counterparts.
A1.1 Young adults with a pre-existing mental health condition
Findings from the SCOVID study suggest young adults are at a higher risk for mental health problems and lower mental wellbeing during the COVID-19 pandemic compared with other age groups (30-59 years, 60+ years). In a Young Minds survey conducted with young people with mental health needs in the UK (June 2020), 80% of respondents felt that the COVID-19 pandemic had made their mental health worse (Young Minds, 2020).
Looking at the background and health of young adults with a pre-existing mental health condition, 52.2% were in the lower SEG, 25.0% reported that their working status had changed (i.e., furloughed, lost job), and 26.1% were key workers. 12.0% had dependents under 5 years and 31.5% reported having unpaid caring responsibilities. 29.3% also had a pre-existing physical health condition. Compared with young adults with no mental health condition, young adults with a mental health condition were more likely to be in the lower SEG, to have unpaid caring responsibilities, have young dependents (under 5 years), and have a physical health condition; these factors may place them at higher risk of poor mental health.
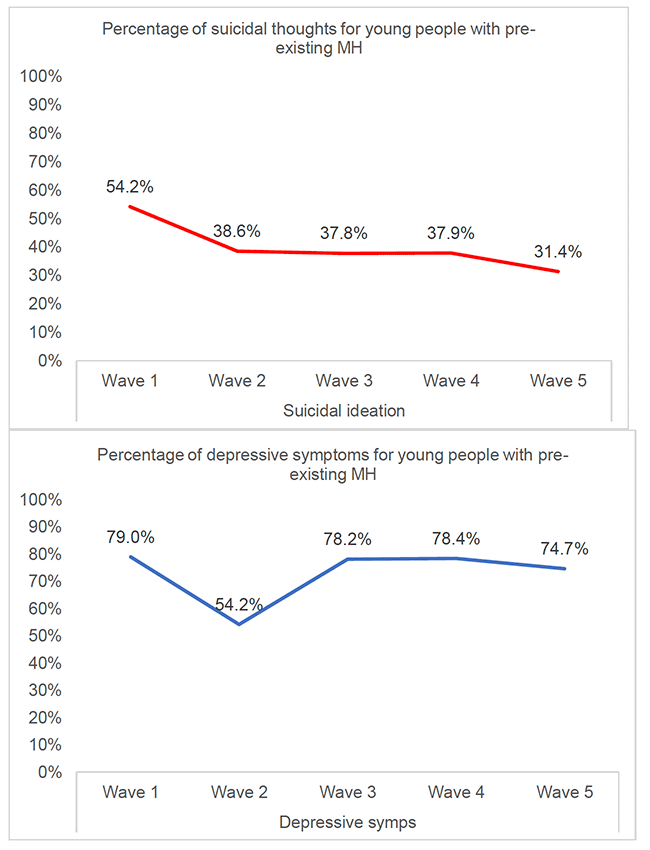
Findings from Wave 1 to Wave 5 of the SCOVID study suggest that young adults (18-29 years) with pre-existing mental health conditions are at higher risk of poorer mental health than young adults with no pre-existing mental health condition. Additionally, at most waves, young adults with a pre-existing mental health condition reported higher rates of suicidal thoughts, depressive symptoms, anxiety symptoms and lower mental wellbeing than the other age groups (30-59 years and aged 60+ years) who also had a pre-existing mental health condition.
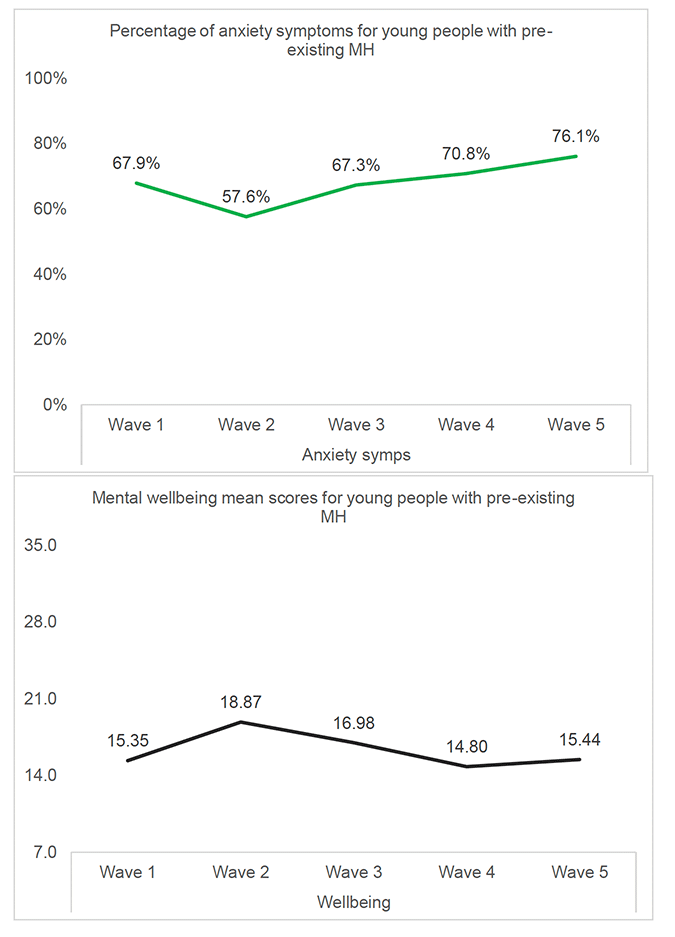
Figure A1.1 illustrates mental health outcome trends (suicidal thoughts, depressive symptoms, anxiety symptoms, and the SWEMWBS wellbeing scores) for young adults with a pre-existing mental health condition across the SCOVID study. Looking at these trends across the waves in context of changes in pandemic restrictions, young adults with a mental health condition reported the highest rates of suicidal thoughts and depressive symptoms, and lowest levels of mental wellbeing, at Wave 1 (May – June 2020), which was closer to the start of pandemic and coincided with Phase 1 of the easing of lockdown restrictions in Scotland. By Wave 2 (July – August 2020), at which point restrictions had eased during the summer, rates of suicidal thoughts, depressive symptoms and anxiety symptoms were at their lowest, and mental wellbeing was at its highest. By Wave 5 (June – July 2021), suicidal thoughts, depressive symptoms and mental wellbeing appeared to improve, which coincided with a period of easing of restrictions. In contrast, anxiety symptoms were at their highest at Wave 5. This suggests that although young adults with a pre-existing mental health condition reported overall better mental health and wellbeing when restrictions were eased, symptoms of anxiety appeared to remain high. As a booster sample was added at Wave 5, this finding should be interpreted with caution.
A1.2 Women with a pre-existing mental health condition
Data shows that women are more likely than men to report and be diagnosed with a mental health condition. For example, the Adult Psychiatric Morbidity Survey (APMS, 2016) reported that one in five women (20.7%) had a common mental disorder (e.g., depression, anxiety) compared with one in eight men (13.2%). Similarly, in the Scottish Health Survey (SHeS, 2019), 19% of women reported having psychiatric symptoms, compared with 15% of men. Therefore, women were more likely to have a pre-existing mental health condition at the start of the COVID-19 pandemic, and this may add to their vulnerability.
A Wave 5 of the SCOVID study, 53.8% women with a pre-existing mental health condition were in the lower SEG, 63.7% reported their working status had changed (e.g., furloughed, lost job), and 31.8% were key workers. 10.1% had dependents aged under 5 years, and 38.2% had caring responsibilities. 51.9% also had a physical health condition. Compared with women with no mental health condition, women with a mental health condition were more likely to be in the lower SEG, have caring responsibilities, have young dependents and have a physical health condition; these factors may make this group at higher risk of poorer mental health.
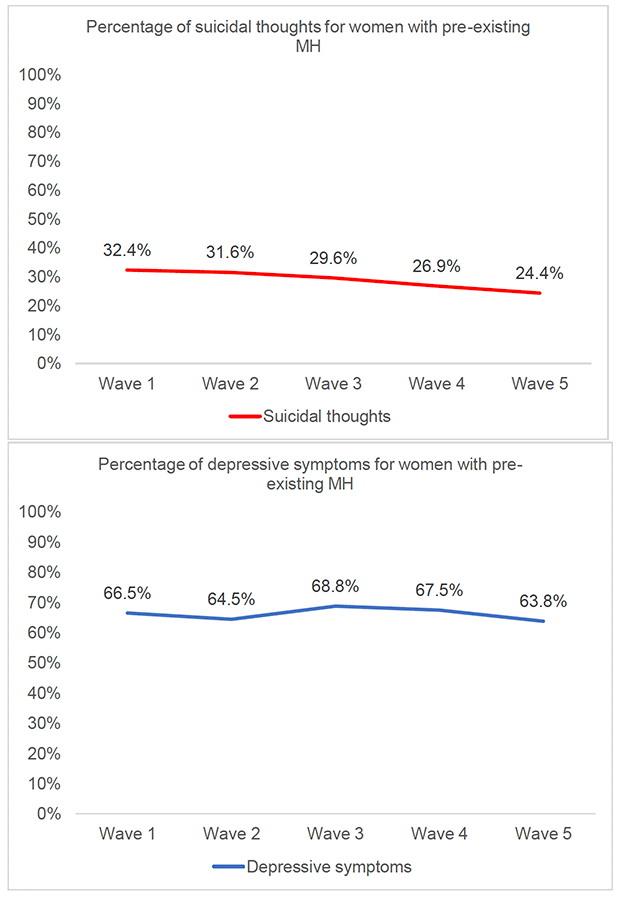
Wave 1 to Wave 5 of the SCOVID study suggests that mental health for women with a pre-existing mental health condition was consistently much worse than for women without a pre-existing mental health condition. For example, at Wave 5, 15.6% of women with no pre-existing mental health condition reported depressive symptoms, compared with 63.8% of women with a mental health condition, and this trend is seen for each outcome across the waves (see Annex 4 Table F). Compared with men with a pre-existing mental health condition, women in this group consistently reported higher rates of depressive symptoms and anxiety symptoms across the waves, although rates of suicidal thoughts and levels of mental wellbeing appeared to fluctuate more.
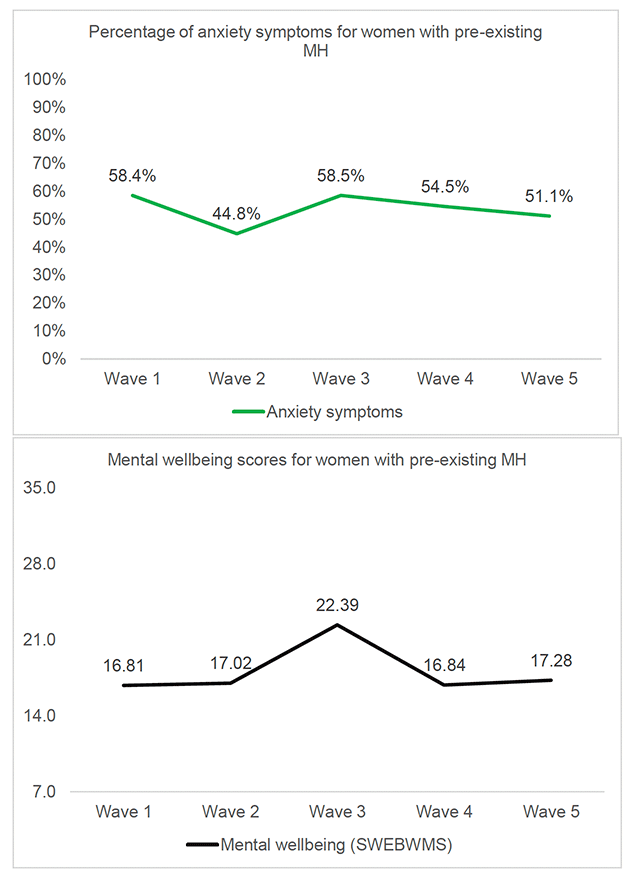
Figure A1.2 displays mental health outcome trends (suicidal thoughts, depressive symptoms, anxiety symptoms, and the SWEMWBS wellbeing scores) for women with a pre-existing mental health condition across the SCOVID study. Overall, there were no standout trends for women with a pre-existing mental health condition in the mental health outcomes in relation to the COVID-19 restrictions in place. Women did appear to report lower rates of suicidal thoughts, depressive symptoms and anxiety symptoms at Wave 5 (June - July 2021), when restrictions had been eased. The lowest anxiety symptoms were reported at Wave 2 (July – August 2020), which also coincided with the easing of restrictions. In contrast, the highest levels of wellbeing were reported at Wave 3 (October 2020), which coincided with the increasing of restrictions across Scotland.
A1.3 Men with a pre-existing mental health condition
Although women consistently report higher rates of common mental health disorders than men (APMS, 2016), there is some evidence that men's mental health has been worsening in recent years. For example, the SHeS (2019) found that the proportion of men reporting symptoms of depression and anxiety has increased over surveys, with 9% of men reporting anxiety symptoms in 2016, increasing to 13% in 2019, and 7% reporting depressive symptoms in 2011, rising to 12% in 2019. Further, the monitoring of men's mental health is made more pertinent by the fact that men are approximately three times more likely to die by suicide than women (ScotPHO, 2020).
Looking at background factors at Wave 5 of the SCOVID study, 58.9% of men with a pre-existing mental health condition were in the lower SEG, 54.4% reported their working status had changed (e.g., furloughed, lost job), and 26.6% were key workers. 5.1% had dependents aged under 5 years, and 33.5% had caring responsibilities. 51.9% also had a physical health condition. Compared with men with no mental health condition, women with a mental health condition were more likely to be in the lower SEG, have caring responsibilities, and have a physical health condition; these factors may make this group at higher risk of poorer mental health.
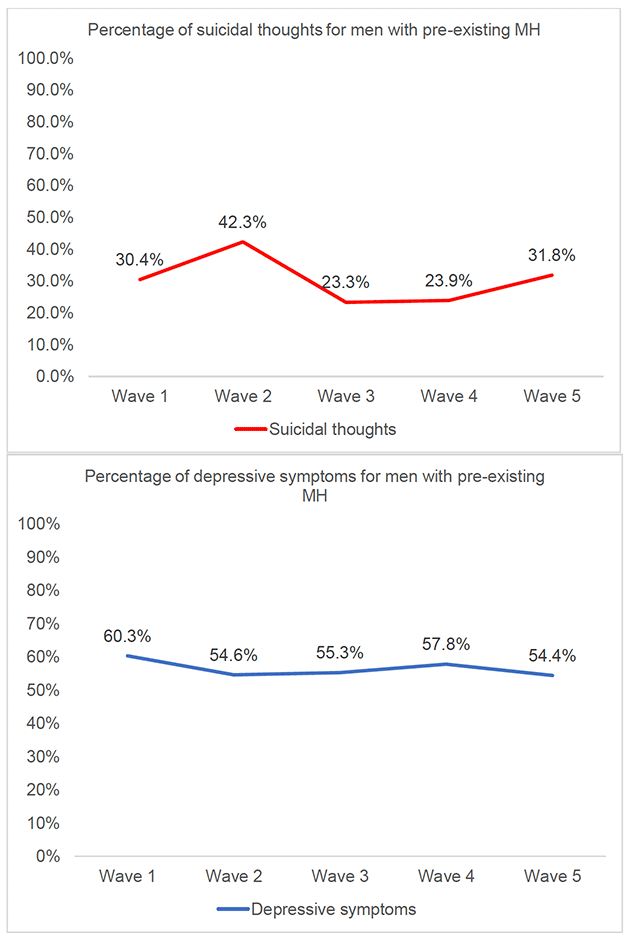
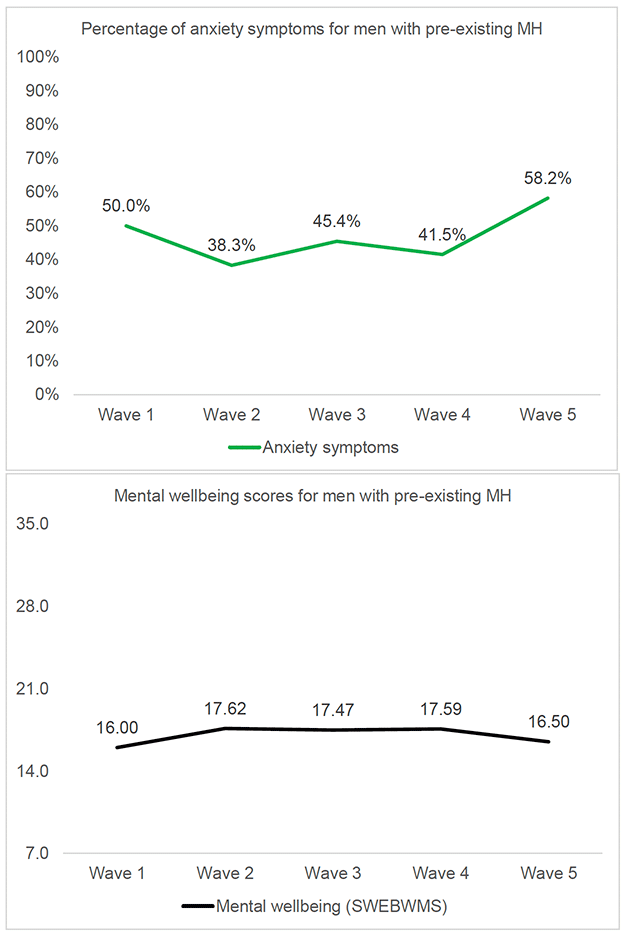
Wave 1 to Wave 5 of the SCOVID study suggests that mental health for men with a pre-existing mental health condition was consistently much worse than for men without a pre-existing mental health condition. For example, at Wave 5, 9.4% of men with no pre-existing mental health condition reported suicidal thoughts, compared with 31.8% of men with a pre-existing mental health condition, and this trend is seen for each outcome across the waves (see Annex 4, Table F). Although women with a pre-existing mental health condition appeared to consistently report higher rates of depressive symptoms and anxiety symptoms across the waves, rates of suicidal thoughts and levels of mental wellbeing fluctuated more. For example, at Wave 2, 42.3% of men with a pre-existing mental health condition reported suicidal thoughts, compared with 31.6% of women in this group, and this trend is found at Wave 5 as well.
Figure A1.3 displays mental health outcome trends (suicidal thoughts, depressive symptoms, anxiety symptoms, and the SWEMWBS wellbeing scores) for men with a pre-existing mental health condition across the SCOVID study. Similar to women with a pre-existing mental health condition, there were no standout trends in the data in relation to the restrictions in place at each wave. Looking at suicidal thoughts, the highest rates were reported at Wave 2 (July – August 2020) and Wave 5 (June - July 2021), which both coincided with a period of eased restrictions in Scotland. For this group, the highest rate of anxiety symptoms was reported at Wave 5, where levels of wellbeing were also lower than at previous waves. In contrast, the highest rates of depressive symptoms were reported at Wave 1 (May – June 2020) and Wave 4 (February 2021), which were periods of higher restrictions. Therefore, there is some evidence that men with a pre-existing mental health condition reported worse mental wellbeing at times of loosened restrictions, although this is not consistent. As a booster sample was added at Wave 5, these findings should be interpreted with caution as this is a sample is made up of different participants than at the previous waves.
A2. Mental health of people with a pre-existing physical health condition
People with a pre-existing physical health condition may be vulnerable to poor mental health and wellbeing during the COVID-19 pandemic, as the pandemic may exacerbate existing health and mental health issues in a population that may be more susceptible to the effects of the COVID-19 virus. Looking at levels of access to health services in the UK, evidence suggests that primary care contacts for almost all conditions dropped considerably after the introduction of population-wide restrictions, and by July 2020 they had not returned to pre-lockdown levels (Mansfield et al., 2021). Further, an international study found the prevalence of anxiety symptoms, depressive symptoms, and stress to be higher in individuals with certain pre-existing chronic health conditions, such as asthma, diabetes, and cardiovascular disease (Sayeed et al., 2020). Therefore, individuals with a pre-existing physical health condition appear to be at high risk for poor mental health and wellbeing.
Across Waves 1 to 5 of the SCOVID study, people with a pre-existing a physical health condition consistently reported higher rates of suicidal thoughts, depressive symptoms, anxiety symptoms, and lower levels of mental wellbeing, than people with no pre-existing physical health condition.
Wave 5 data for those with a pre-existing mental health condition indicates that:
- 12.6% reported suicidal thoughts,
- 36.4% reported moderate to severe depressive symptoms, and
- 27.7% reported moderate to severe anxiety symptoms.
Overall trends suggest specific subgroups may be at higher risk of poorer mental health:
- young adults with pre-existing physical health condition
- women with pre-existing physical health condition
- men with a pre-existing health condition
A2.1 Young adults with a pre-existing physical health condition
As noted in previous sections, young adults appear to be at higher risk of poor mental health and wellbeing during the pandemic, and this may be exacerbated by pre-existing mental and physical health conditions. For example, in a UK study two thirds of young people with a physical or intellectual disability reported a reduction in their physical activity, and the majority said this had an impact on their mental health (Theis et al., 2021).
Looking at the background and health of young adults with a pre-existing physical health condition, 39.4% were in the lower SEG, 12.1% reported that their working status had changed (i.e., furloughed, lost job), and 6.1% were key workers. None had dependents under 5 years and 39.4% reported having unpaid caring responsibilities. 79.4% also had a pre-existing mental health condition. Compared with young adults with no physical health condition, young adults with a physical health condition were more likely to report a change in their working status and have unpaid caring responsibilities; these factors may make them at higher risk of poor mental health.
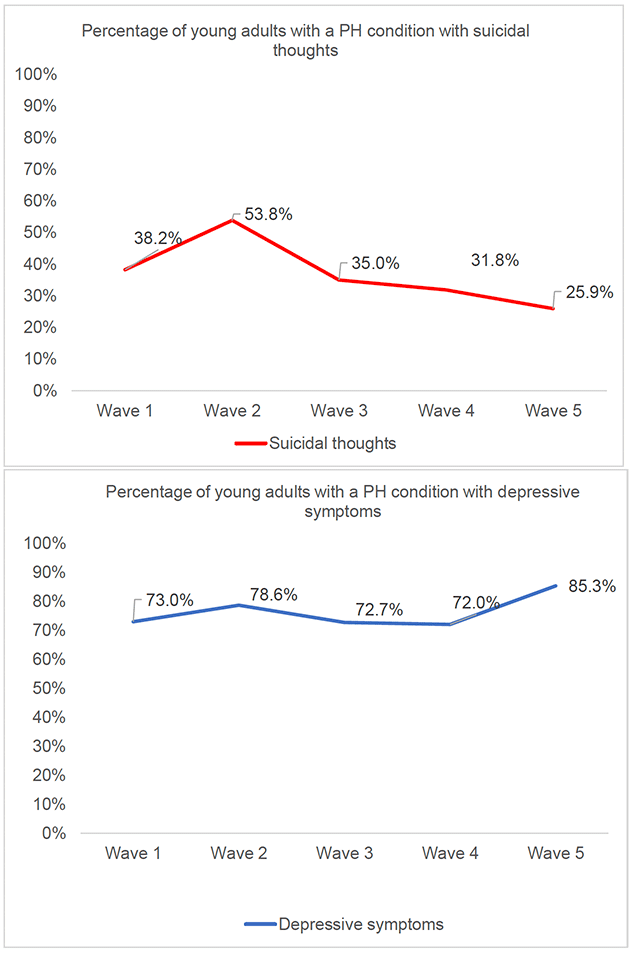
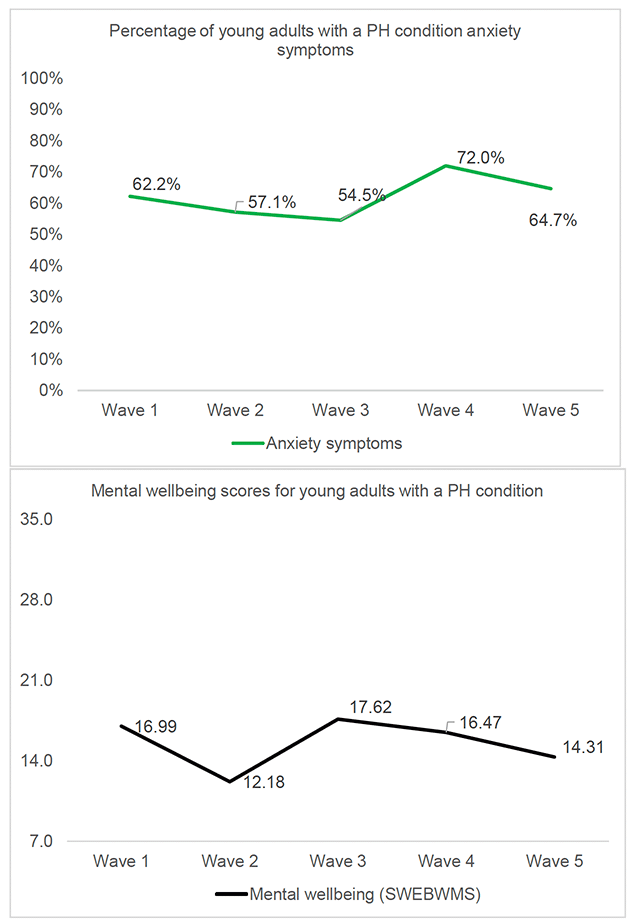
Findings from Wave 1 to Wave 5 of the SCOVID study suggest that young people with pre-existing physical health conditions are at higher risk of mental health problems than young adults with no pre-existing physical health condition. For example, at Wave 5 33.2% of young adults with no pre-existing physical health condition reported depressive symptoms, compared with 85.3% of young adults with a health condition. Additionally, at all waves, young adults with a physical health condition reported higher rates of suicidal thoughts, depressive symptoms, anxiety symptoms, and lower mental wellbeing, than their age group counterparts (30-59 years, 60+ years) who also had a pre-existing physical health condition.
Figure A2.1 illustrates mental health outcome trends (suicidal thoughts, depressive symptoms, anxiety symptoms, and the SWEMWBS wellbeing scores) for young adults with a pre-existing physical health condition across the SCOVID study. Looking at these trends across the waves in context of changes in pandemic restrictions, young adults with a pre-existing physical health condition reported the highest rates of suicidal thoughts and lowest levels of mental wellbeing at Wave 2 (July – August 2020), a time that coincided with the reduction of restrictions in Scotland. Additionally, the highest rates of depressive symptoms were found at Wave 5 (June - July 2021), when restrictions had also been eased. This suggests that this group reported poorer mental health when restrictions were eased in Scotland. As a booster sample was added at Wave 5, this finding should be interpreted with caution as this is a sample is made up of different participants than at the previous waves.
A2.2 Women with a pre-existing physical health condition
Women appear to be at higher risk for poor mental health during the COVID-19 pandemic, and there is evidence in the UK of a disproportionate effect on women's mental wellbeing than men (Etheridge & Spantig, 2020). Further, when it comes to the impact of COVID-19 upon health, there is evidence that women may be at higher risk for longer term symptoms due to the increased rates of inflammatory conditions in women compared men (Torjesen, 2021).
Looking at the background and health of women with a pre-existing physical health condition, 44.4% were in the lower SEG, 75.3% reported that their working status had changed (i.e., furloughed, lost job), and 10.8% were key workers. 2.8% had dependents under 5 years and 23.6% reported having unpaid caring responsibilities. 35.1% also had a pre-existing mental health condition. Compared with women with no physical health condition, those with a health condition were more likely to be in the lower SEG, report a change to working status, have caring responsibilities, and have a mental health condition, factors which may make them more vulnerable to poorer mental health.
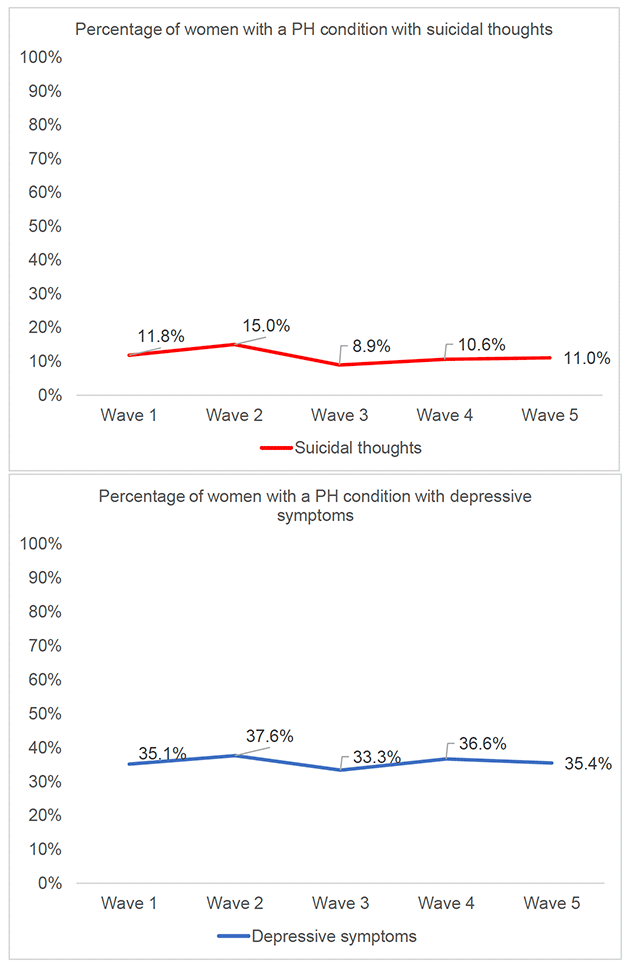
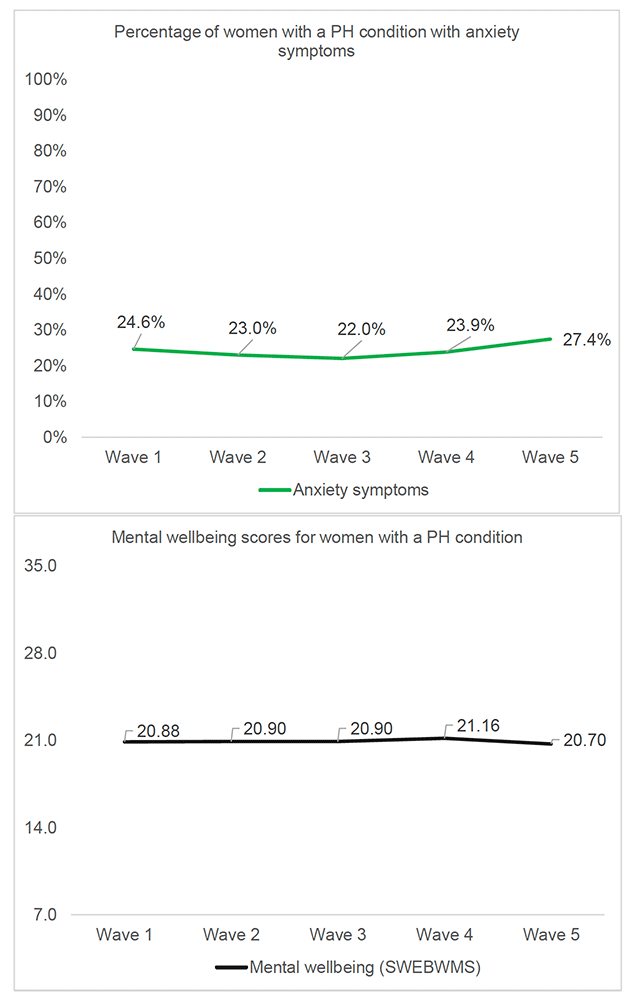
Looking across the study waves, mental health outcomes for women with a pre-existing physical health condition were consistently worse than for women without a pre-existing physical health condition. For example, at Wave 5, 18.8% of women with no pre-existing health condition reported depressive symptoms, compared with 35.4% of women with a pre-existing health condition, and this trend is seen for each outcome across the waves (see Annex 4 Table F). Compared with men with a pre-existing physical health condition, women in this group tended to report higher rates of depressive symptoms and anxiety symptoms across the waves, although overall men reported higher rates of suicidal thoughts and lower levels of mental wellbeing.
Figure A2.2 illustrates mental health outcome trends (suicidal thoughts, depressive symptoms, anxiety symptoms, and the SWEMWBS wellbeing scores) for women with a pre-existing physical health condition across the SCOVID study. Looking at these trends across the waves in context of changes in pandemic restrictions, women with a pre-existing physical health condition reported the highest rates of suicidal thoughts and depressive symptoms at Wave 2 (July – August 2020), a time that coincided with the easing of restrictions in Scotland. The highest rates of anxiety symptoms and lowest mental wellbeing was found at Wave 5 (June - July 2021), when restrictions had also been eased. As a booster sample was added at Wave 5, this finding should be interpreted with caution as this is a sample is made up of different participants than at the previous waves. Additionally, the lowest rates of suicidal thoughts, depressive symptoms and anxiety symptoms were reported at Wave 3 (October 2020), when restrictions were being gradually increased.
A2.3 Men with a pre-existing physical health condition
Looking at the background and health of men with a pre-existing physical health condition, 45.7% were in the lower SEG, 75.2% reported that their working status had changed (i.e., furloughed, lost job), and 13.8% were key workers. 1.0% had dependents under 5 years at home and 23.8% reported having additional caring responsibilities. 39.2% also had a pre-existing mental health condition. Compared with men with no physical health condition, those with a health condition were more likely to be in the lower SEG, report a change to working status, have caring responsibilities, and have a mental health condition, factors which may make them more vulnerable to poorer mental health.
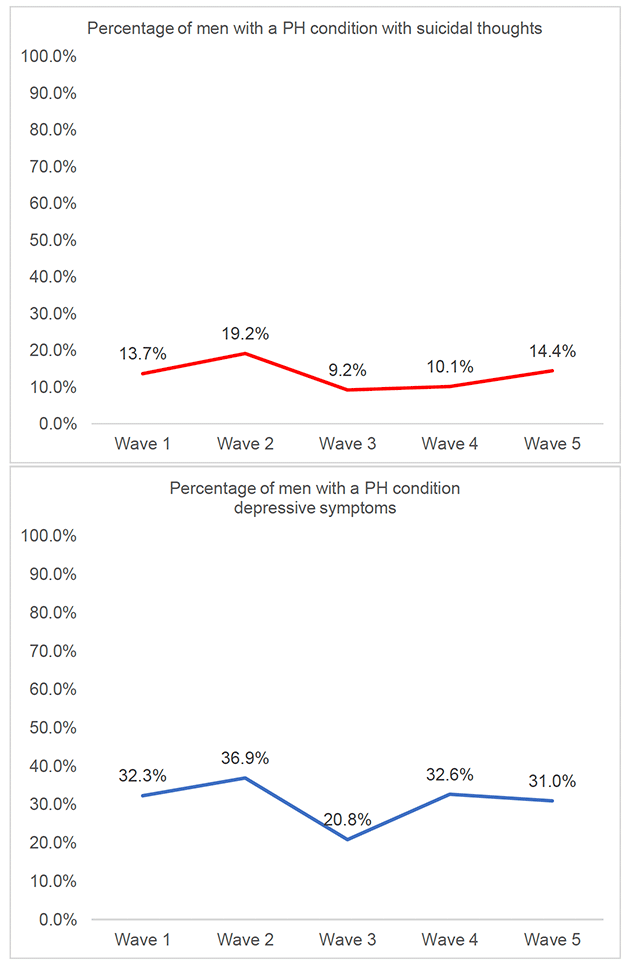
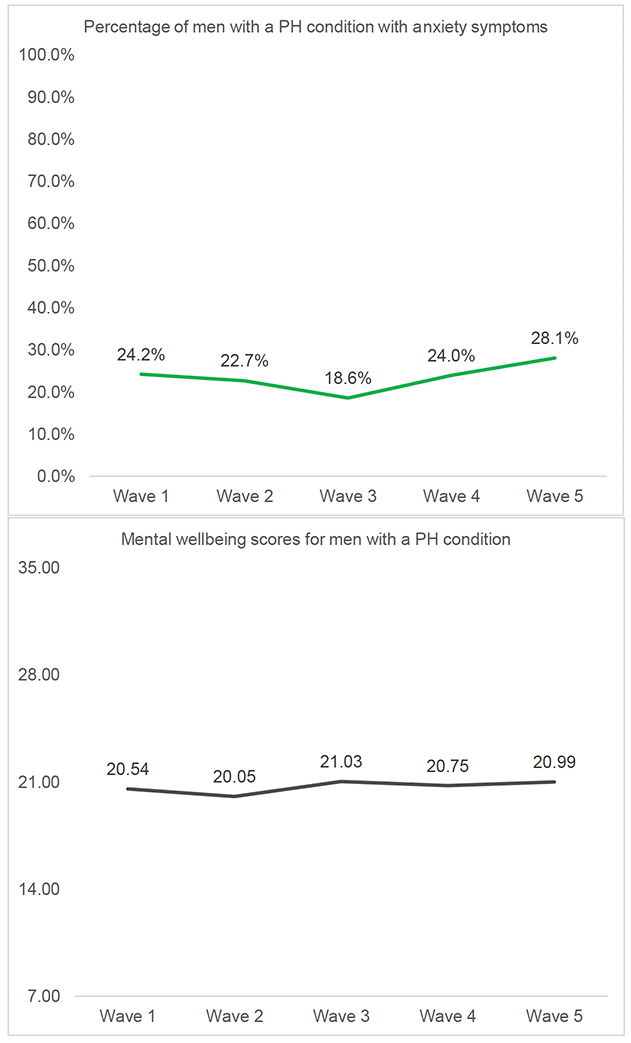
Looking across the study waves, mental health outcomes for men with a pre-existing physical health condition was consistently worse than for men without a pre-existing physical health condition. For example, at Wave 5, 14.3% of men with no pre-existing health condition reported anxiety symptoms, compared with 28.1% of men with a pre-existing health condition, and this trend is seen for each outcome across the waves (see Annex 4 Table F). Compared with women with a pre-existing physical health condition, men in this group tended to reported higher rates of suicidal thoughts and lower levels of mental wellbeing across the waves, although women reported higher rates of depressive and anxiety symptoms.
Figure A2.3 illustrates mental health outcome trends (suicidal thoughts, depressive symptoms, anxiety symptoms, and the SWEMWBS wellbeing scores) for men with a pre-existing physical health condition across the SCOVID study. Looking at these trends across the waves in context of changes in pandemic restrictions, men with a pre-existing physical health condition reported the highest rates of suicidal thoughts, depressive symptoms and lowest mental wellbeing at Wave 2 (July – August 2020), a time that coincided with the reduction of restrictions in Scotland. The highest rates of anxiety symptoms were found at Wave 5 (June - July 2021), when restrictions had also been eased. As a booster sample was added at Wave 5, this finding should be interpreted with caution as this is a sample is made up of different participants than at the previous waves. Similar to women with a physical health condition, the lowest rates of suicidal thoughts, depressive symptoms, and anxiety symptoms where at Wave 3 (October 2020), when restrictions were being increased in Scotland.
A3. Mental health of people with unpaid caring responsibilities
Pre-pandemic evidence suggests that carers report poorer mental health than non-carers, including high levels of stress, anxiety and depression (Carers UK, 2015). Research conducted in the UK during the COVID-19 pandemic suggested that carers of those with intellectual disabilities had significantly greater levels of anxiety, depression, and feelings of defeat and entrapment, with evidence that differences higher than pre-pandemic levels (Willner et al., 2020).
Across Waves 1 to 5 of the SCOVID study, people who had unpaid caring responsibilities reported higher rates of suicidal thoughts, depressive symptoms, anxiety symptoms, and lower levels of mental wellbeing, than people with no caring responsibilities.
Wave 5 data for those with unpaid caring responsibilities indicates that:
- 17.1% reported suicidal thoughts,
- 33.9% reported moderate to severe depressive symptoms, and
- 25.5% reported moderate to severe anxiety symptoms.
Overall trends suggest specific subgroups may be at higher risk of poorer mental health:
- young adults with caring responsibilities
- women with caring responsibilities
A3.1 Young adults with unpaid caring responsibilities
As noted in previous sections, young adults appear to be at higher risk of poor mental health and wellbeing during the pandemic. In the UK, the Carers Trust conducted a survey into the impact of COVID-19 upon young adult carers. They found that 59% of young adult carers say their mental health is worse since the pandemic, 78% are more worried about the future, 74% are feeling more stressed (Carers Trust, 2020).
Looking at the background and health of young adults with unpaid caring responsibilities, 50.0% were in the lower SEG, 25.6% reported that their working status had changed (i.e., furloughed, lost job), and 46.2% were key workers. 9% had dependents under 5 years at home. 37.2% had a pre-existing mental health condition and 16.7% had a pre-existing physical health condition. Compared with young adults with no unpaid caring responsibilities, young carers were more likely to be in the lower SEG, report a change to working status, be a key worker, and have a mental health condition; these factors may make them more vulnerable to poorer mental health.
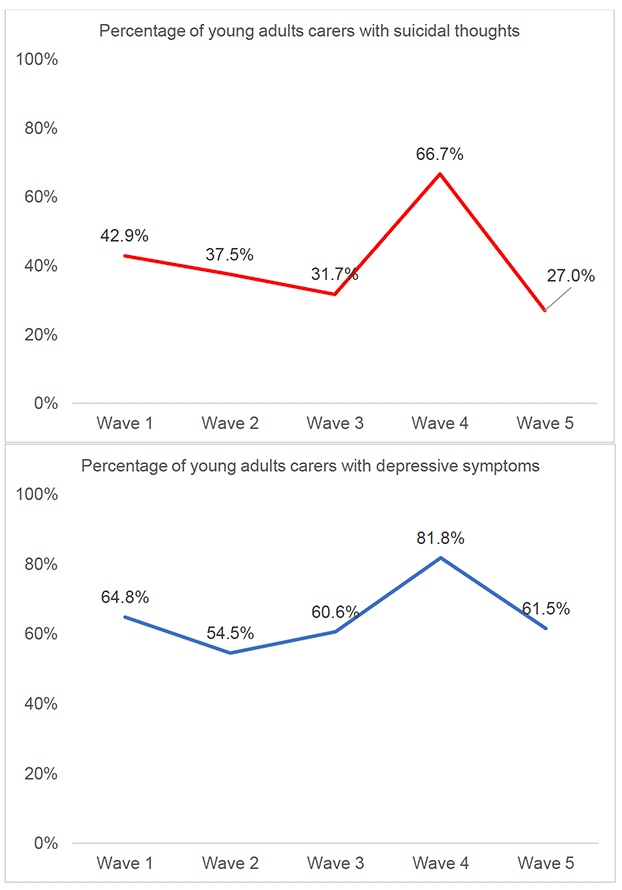
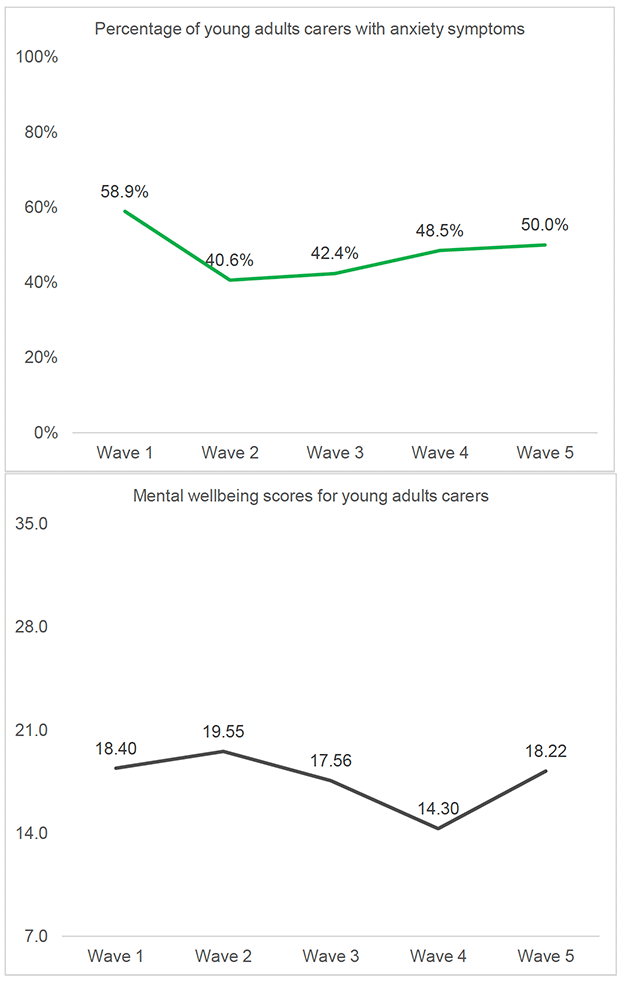
Findings from Wave 1 to Wave 5 of the SCOVID study suggest that young people with caring responsibilities are at higher risk of mental health problems than young adults with no caring responsibilities. For example, at Wave 5 32.3% of young adults with no caring responsibilities reported depressive symptoms, compared with 61.5% of young adults with caring responsibilities (see Annex 4 Table F). Additionally, at all waves, young adults with caring responsibilities reported higher rates of suicidal thoughts, depressive symptoms, anxiety symptoms, and lower mental wellbeing, than their age group counterparts (30-59 years, 60+ years) who also had caring responsibilities.
Figure A3.1 illustrates mental health outcome trends (suicidal thoughts, depressive symptoms, anxiety symptoms, and the SWEMWBS wellbeing scores) for young adults with caring responsibilities across the SCOVID study. Looking at these trends across the waves in context of changes in pandemic restrictions, young adults with caring responsibilities reported the highest rates of suicidal thoughts, depressive symptoms, and lowest levels of mental wellbeing at Wave 4 (February 2021), a time that coincided with a national lockdown. Additionally, the highest rates of anxiety symptoms were found at Wave 1 (May - June 2020), when restrictions were beginning to be eased from the first lockdown. The lowest rates of poor mental health were reported at Wave 2 (July 2020) and Wave 5 (June - July 2021), both periods with eased restrictions. Therefore, it appears the mental health of young carers was worst during periods of lockdown and higher restrictions, and better during periods of eased restrictions.
A3.2 Women with unpaid caring responsibilities
Overall, in the UK women were more likely to take on caring roles than men before the pandemic (Carers UK). Emerging research worldwide suggests that the crisis and its subsequent shutdown response have resulted in an increase in this burden (Power, 2020). Therefore, women carers may be at risk of worse mental health and wellbeing during the COVID-19 pandemic.
Looking at the background and health of women with unpaid caring responsibilities, 41.1% were in the lower SEG, 55.6% reported that their working status had changed (i.e., furloughed, lost job), and 28.8% were key workers. 7.9% had dependents under 5 years at home. 23.2% had a pre-existing mental health condition and 27.3% had a pre-existing physical health condition. Compared with women with no unpaid caring responsibilities, women carers were more likely to be a key worker, have a mental health condition, and have a physical health condition, factors which may make them more vulnerable to poorer mental health.
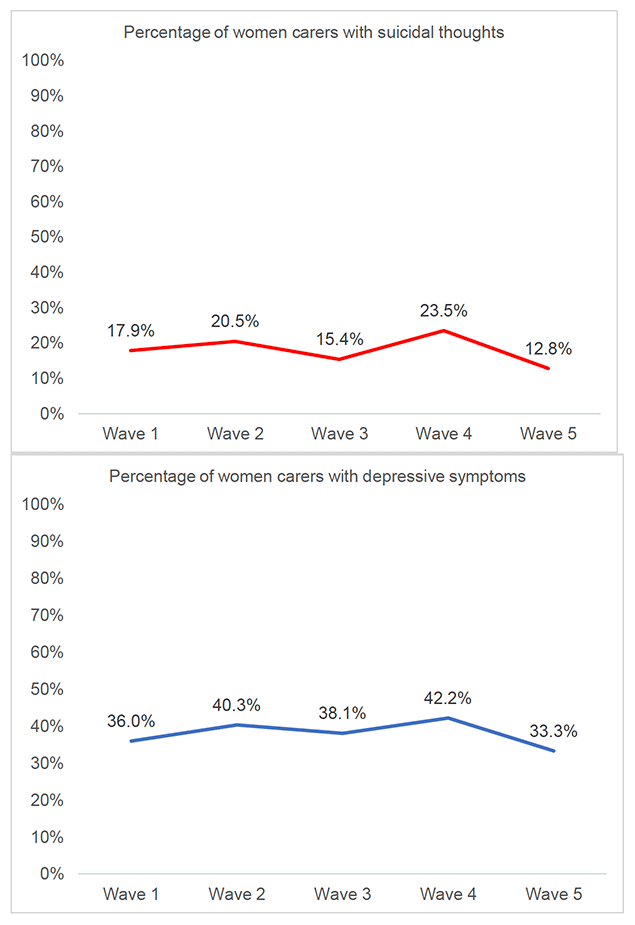
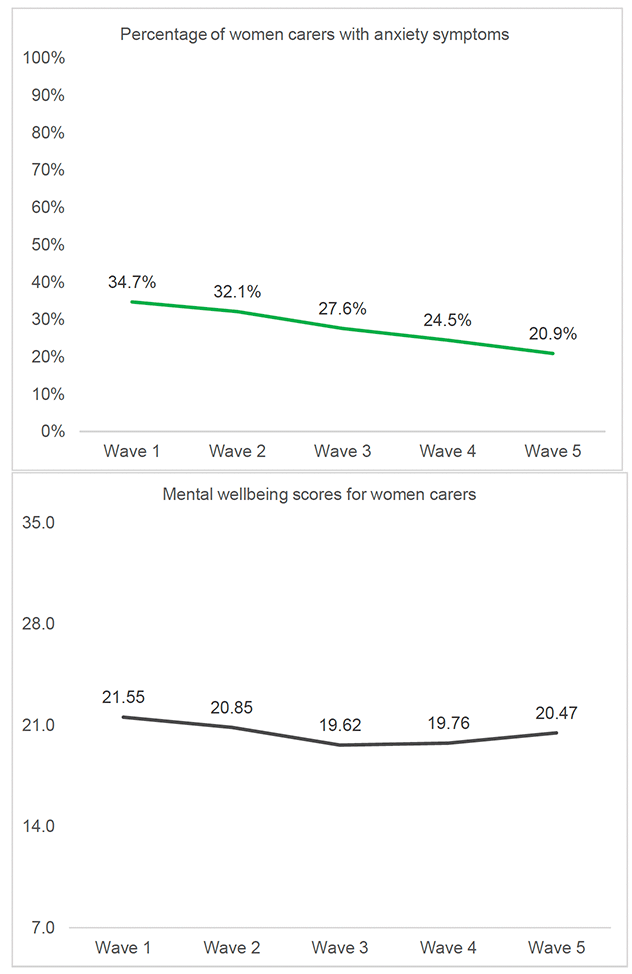
Findings from Wave 1 to Wave 5 of the SCOVID study suggest that women with unpaid caring responsibilities are at higher risk of mental health problems than women with no unpaid caring responsibilities. For example, at Wave 5, 19.9% of women with no caring responsibilities reported depressive symptoms, compared with 33.3% of women with caring responsibilities (see Annex 4 Table F). Additionally, at most waves women with caring responsibilities reported higher rates of suicidal thoughts, depressive symptoms, anxiety symptoms, and lower mental wellbeing, than men who also had caring responsibilities. The main exception was at Wave 5, when men with caring responsibilities reported higher suicidal thoughts, depressive symptoms, and anxiety symptoms.
Figure A3.2 illustrates mental health outcome trends (suicidal thoughts, depressive symptoms, anxiety symptoms, and the SWEMWBS wellbeing scores) for young adults with caring responsibilities across the SCOVID study. Looking at these trends across the waves in context of changes in pandemic restrictions, women with caring responsibilities reported the highest rates of suicidal thoughts and depressive symptoms at Wave 4 (February 2021), a time that coincided with a national lockdown. Additionally, the highest rates of anxiety symptoms were found at Wave 1 (May - June 2020), when restrictions were beginning to be eased from the first lockdown. The lowest rates of poor mental health tended to be reported at Wave 5 (June - July 2021), a period with eased restrictions. Therefore, it appears the mental health of women carers was worst during periods of lockdown and higher restrictions, and better during a period of eased restrictions. As a booster sample was added at Wave 5, this finding should be interpreted with caution as this is a sample is made up of different participants than at the previous waves.
A4. Mental health of people with dependents under 5 years old
A survey in the UK by Young Minds found that 66% of parents said that the COVID-19 pandemic had had a negative impact on their own mental health (Young Minds, 2020). Evidence from the Co-Space study in the UK found that parents who had younger children living in the home reported high levels of stress symptoms during the first lockdown and around a third were stressed by their children's behaviour at that time (Shum et al., 2021).
Across Waves 1 to 5 of the SCOVID study, people who had dependents under 5 years tended to report higher rates of suicidal thoughts, depressive symptoms, anxiety symptoms, and lower levels of mental wellbeing, than people with no dependents under 5 years.
Wave 5 data for those with young dependents (under 5 years) indicates that:
- 11.9% reported suicidal thoughts,
- 27.4% reported moderate to severe depressive symptoms, and
- 18.8% reported moderate to severe anxiety symptoms.
As the sample sizes for young adults with young dependents were small, it was not possible to explore trends for young adults over the waves. For the sex subgroups, trends suggest women with dependents under 5 years were at risk of poorer mental health.
A4.1 Women with dependents under 5 years
In the UK, evidence suggests that women carried out more daily childcare duties than men during lockdown, as women averaged more than three hours a day compared with two hours for men (ONS, 2020). Therefore, women with young dependents may be at risk of worse mental health and wellbeing during the COVID-19 pandemic.
Looking at the background and health of women with young dependents, 42.5% were in the lower SEG, 62.3% reported that their working status had changed (i.e., furloughed, lost job), and 36.8% were key workers. 17.9% had unpaid caring responsibilities. 19.6% had a pre-existing mental health condition and 7.5% had a pre-existing physical health condition. Compared with women with no dependents under 5 years, women with young dependents were more likely to be in the lower SEG, be a key worker, and have a mental health condition; these factors may make them more vulnerable to poorer mental health.
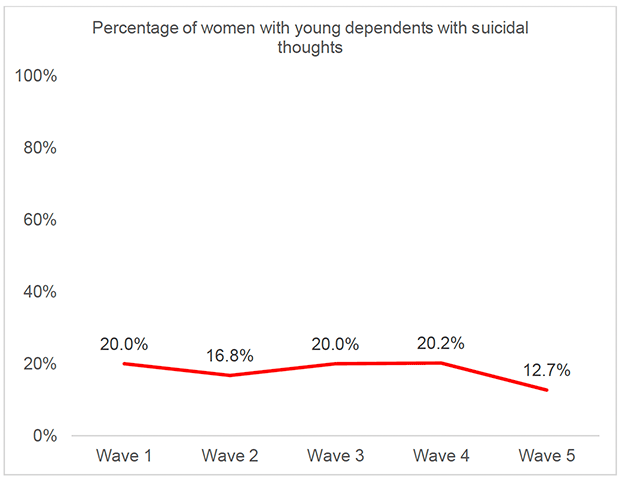
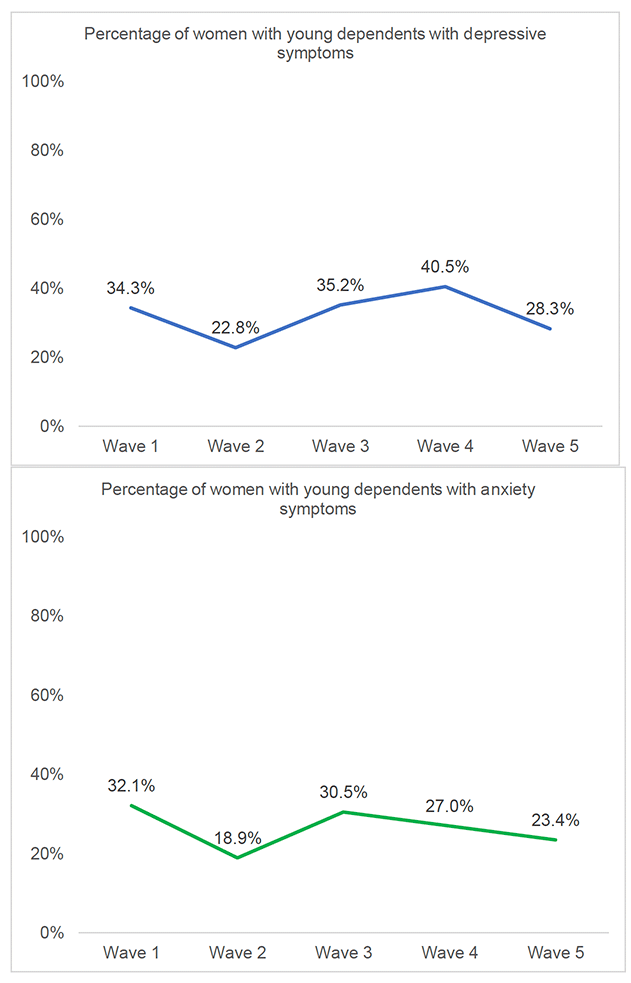
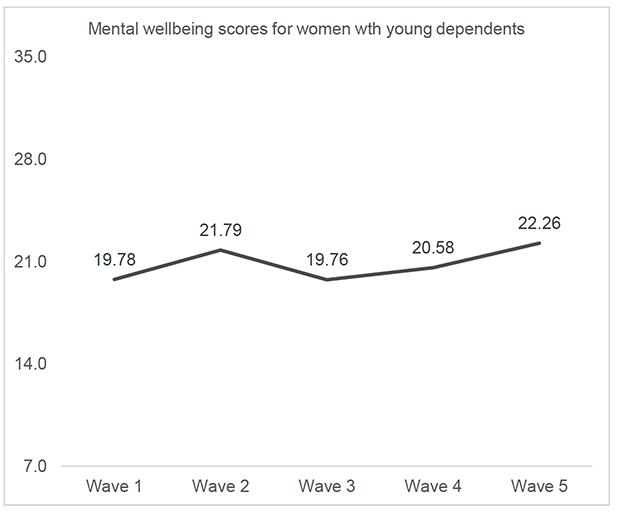
Findings from Wave 1 to Wave 5 of the SCOVID study suggest that women with young dependents tended to be at higher risk of mental health problems than women with no young dependents. For example, at Wave 5, 21.9% of women with no young dependents reported depressive symptoms, compared with 28.3% of women with young dependents (see Annex 4, Table F). Additionally, at most waves women with young dependents reported higher rates of suicidal thoughts, depressive symptoms, anxiety symptoms, and lower mental wellbeing, than men who also had young dependents.
Figure A4.1 illustrates mental health outcome trends (suicidal thoughts, depressive symptoms, anxiety symptoms, and the SWEMWBS wellbeing scores) for women with dependents under 5 years across the SCOVID study. Looking at these trends across the waves in context of changes in pandemic restrictions, women with young dependents reported the highest rates of suicidal thoughts and depressive symptoms at Wave 4 (February 2021), a time that coincided with a national lockdown. Additionally, the highest rates of anxiety symptoms were found at Wave 1 (May - June 2020), when restrictions were beginning to be eased from the first lockdown. The lowest rates of poor mental health tended to be reported at Wave 5 (June - July 2021), a period with eased restrictions. Therefore, it appears the mental health of women with young dependents was worst during periods of lockdown and higher restrictions, and better during a period of eased restrictions. As a booster sample was added at Wave 5, this finding should be interpreted with caution as this is a sample is made up of different participants than at the previous waves.
A5. Mental health of people with vaccine hesitancy
Vaccine hesitancy is described as behavioural delay in acceptance or refusal of vaccines despite availability of vaccine services (SAGE, 2014). The development of effective vaccines against COVID-19 were heralded as a turning point in the pandemic, despite this the accelerated development and relative novelty of the COVID-19 vaccines have led to public uncertainty (Hrynick et al., 2020). There is some evidence that vaccine hesitancy may be higher in vulnerable groups, such as those with mental health problems (Lorenz et al., 2013).
Questions about vaccine uptake and hesitancy were asked at Wave 4 and Wave 5 of the SCOVID study. At both waves, people who had hesitancy in taking the COVID-19 vaccine reported higher rates of suicidal thoughts, depressive symptoms, anxiety symptoms, and lower levels of mental wellbeing, than people who had, or planned to take, the vaccine.
Wave 5 data for those with vaccine hesitancy indicates that:
- 30.7% reported suicidal thoughts,
- 33.2% reported moderate to severe depressive symptoms, and
- 30.4% reported moderate to severe anxiety symptoms.
Overall trends suggest specific subgroups may be at higher risk of poorer mental health:
- young adults with vaccine hesitancy
- women with vaccine hesitancy
A5.1 Young adults with vaccine hesitancy
Research by the Office for National Statistics (ONS) in the UK suggest hesitancy towards the COVID-19 vaccine was highest in 16- to 29-year-olds, compared with those aged 30 to 49 years, and over 50s respectively (ONS, 2021). Reasons for hesitancy included distrust of the safety and content of the vaccine, distrust of government, concern about known and unknown side effects, and belief it was unnecessary for those at low risk of harm from the virus.
At Wave 5 of the SCOVID study, 12.3% of young adults reported vaccine hesitancy, compared with 8.8% of 30-59 year olds, and 1.7% of 60+ year olds.
Looking at the background and health of young adults with vaccine hesitancy, at Wave 5 34.3% were in the lower SEG, 19.4% reported that their working status had changed (i.e., furloughed, lost job), and 47.8% were key workers. 21.2% had caring responsibilities and 19.7% had dependents under 5 years at home. 22.7% had a pre-existing mental health condition and 6.0% had a pre-existing physical health condition. Compared with young adults with no vaccine hesitancy, young adults with vaccine hesitancy were more likely to be a key worker, have caring responsibilities and have a mental health condition, factors which may make them more vulnerable to poorer mental health.
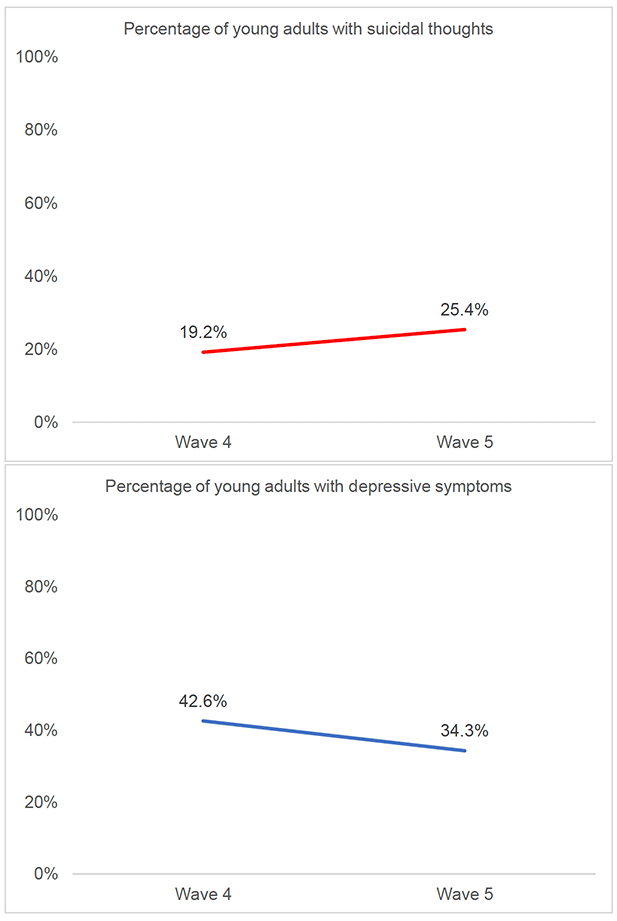
Findings from Wave 4 and Wave 5 of the SCOVID study suggest that young adults with vaccine hesitancy tended to be at higher risk of mental health problems than young adults with no vaccine hesitancy. For example, at Wave 5 11.8% of young adults with no vaccine hesitancy reported suicidal thoughts, compared with 25.4% of young adults with vaccine hesitancy (see Annex 4, Table F). Additionally, young adults with vaccine hesitancy tended to report higher rates of depressive symptoms and anxiety symptoms, than their age group counterparts (30-59 years, 60+ years) who also had vaccine hesitancy.
Figure A4.1 illustrates mental health outcome trends (suicidal thoughts, depressive symptoms, anxiety symptoms, and the SWEMWBS wellbeing scores) for young adults with caring responsibilities at Wave 4 and Wave 5 of the SCOVID study. Looking at these trends in context of changes in pandemic restrictions, young adults with vaccine hesitancy reported the highest rates of depressive symptoms and lowest mental wellbeing at Wave 4 (February 2021), a time that coincided with a national lockdown. In contrast, the highest rates of anxiety symptoms and suicidal thoughts were found at Wave 5 (June – July 2021), when restrictions were eased. Therefore, it appears the mental health of young adults who were vaccine hesitant fluctuated from Wave 4 to Wave 5. As a booster sample was added at Wave 5, this finding should be interpreted with caution as this is a sample is made up of different participants than at the previous waves.
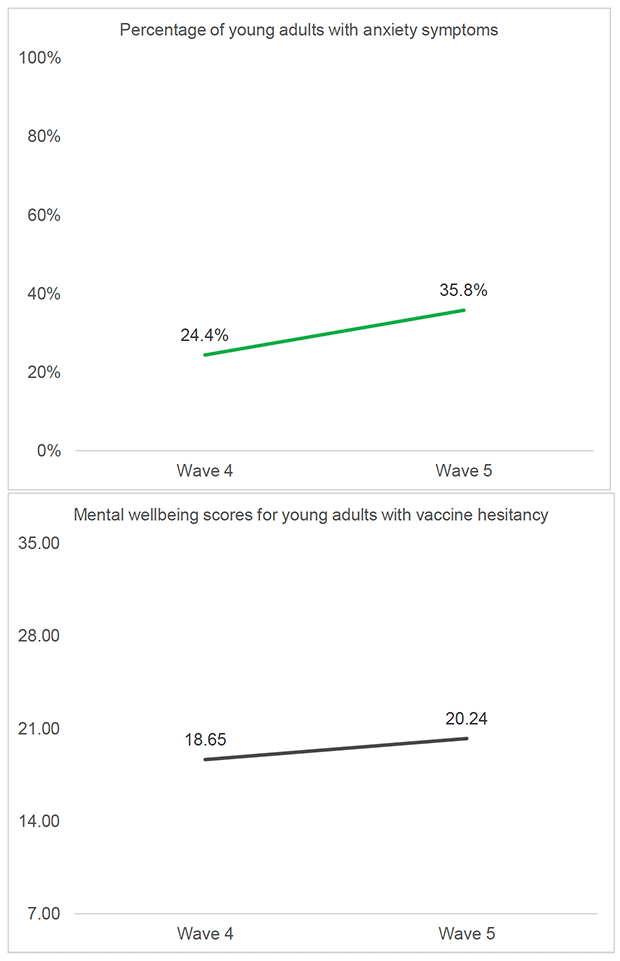
A5.2 Women with vaccine hesitancy
Evidence from the UCL COVID-19 Social Study in the UK suggests that women evidenced slightly lower intentions to get the COVID-19 vaccination than men (Paul et al., 2021). Additionally, a survey of pregnant women in the UK found that 58% of those offered the vaccine had declined it, because they were worried that it would harm the baby and were waiting on more information about the safety of COVID-19 vaccines in pregnancy (Royal College of Obstetricians and Gynaecologists, 2021).
At Wave 5 of the SCOVID study, 7.1% of women reported vaccine hesitancy, and 7.6% of men.
Looking at the background and health of women with vaccine hesitancy, at Wave 5 39.1% were in the lower SEG, 27.2% reported that their working status had changed (i.e., furloughed, lost job), and 23.9% were key workers. 29.3% had caring responsibilities and 26.9% had dependents under 5 years at home. 22.8% had a pre-existing mental health condition and 28.3% had a pre-existing physical health condition. Compared with women with no vaccine hesitancy, women with vaccine hesitancy were more likely to be having caring responsibilities, have young dependents and have a mental health condition, factors which may make them more vulnerable to poorer mental health.
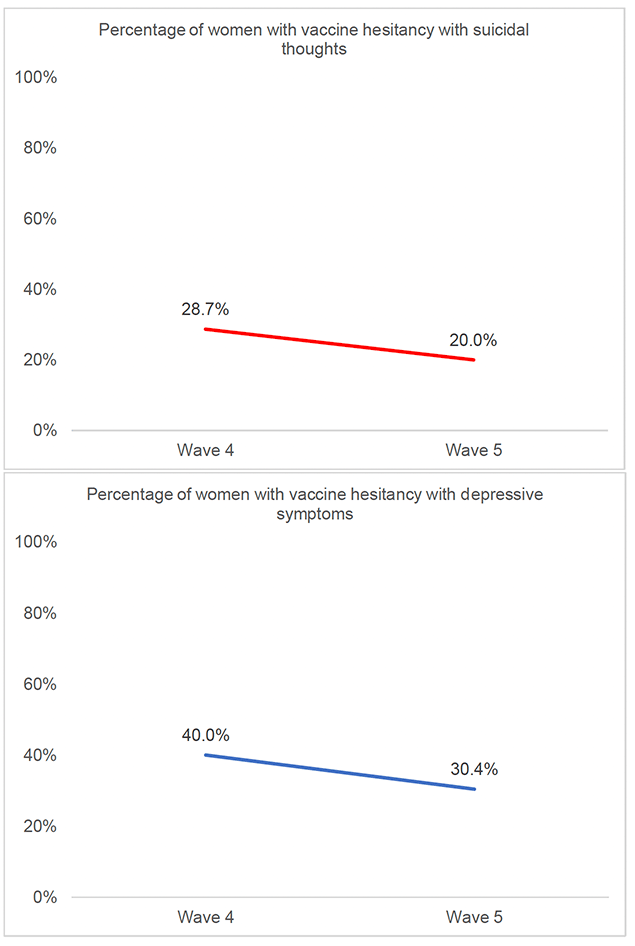
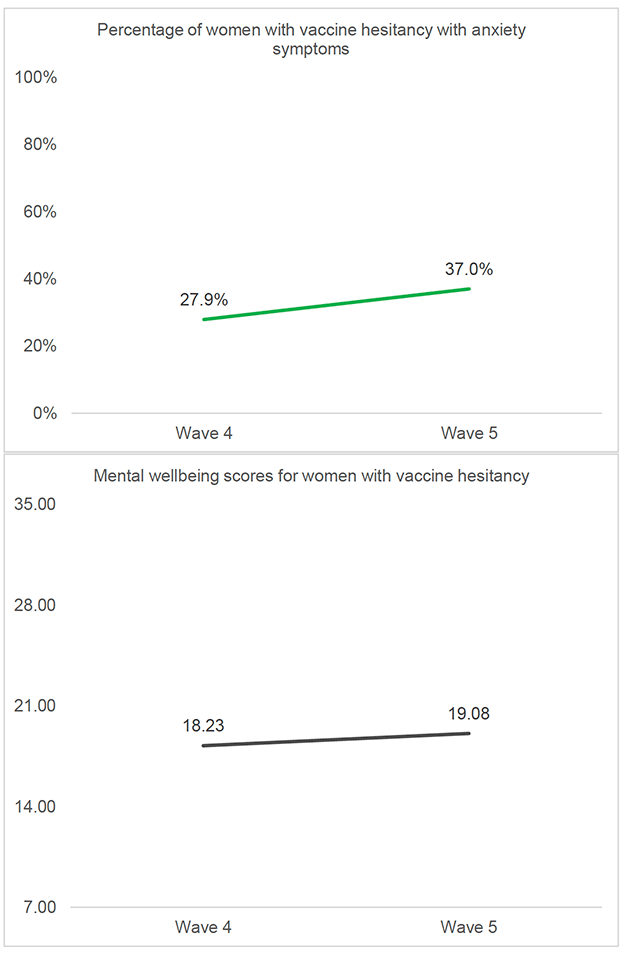
Findings from Wave 4 and Wave 5 of the SCOVID study suggest that women with vaccine hesitancy tended to be at higher risk of mental health problems than women with no vaccine hesitancy. For example, at Wave 5, 18.3% of women with no vaccine hesitancy reported anxiety symptoms, compared with 37.0% of women with vaccine hesitancy (see Annex 4, Table F). Additionally, women with vaccine hesitancy tended to report higher rates of anxiety symptoms and lower mental wellbeing than men who also had vaccine hesitancy.
Figure A4.2 illustrates mental health outcome trends (suicidal thoughts, depressive symptoms, anxiety symptoms, and the SWEMWBS wellbeing scores) for women with vaccine hesitancy at Wave 4 and Wave 5 of the SCOVID study. Looking at these trends in context of changes in pandemic restrictions, women with vaccine hesitancy reported the highest rates of suicidal thoughts, depressive symptoms and lowest mental wellbeing at Wave 4 (February 2021), a time that coincided with a national lockdown. In contrast, the highest rates of anxiety symptoms were found at Wave 5 (June - July 2021), when restrictions were eased. Therefore, it appears the mental health of women who were vaccine hesitant overall was poorer when restrictions were in place. As a booster sample was added at Wave 5, this finding should be interpreted with caution as this is a sample is made up of different participants than at the previous waves.
A5.3 Men with vaccine hesitancy
Evidence suggests that younger men may be less likely to come forward for the COVID-19 vaccination, according to NHS England there is a clear gender divide, with two thirds of men aged 18 to 24 having had a COVID-19 vaccine compared with nearly three quarters of women (NHS England, 2021).
Looking at the background and health of men with vaccine hesitancy, at Wave 5 44.6% were in the lower SEG, 53.8% reported that their working status had changed (i.e., furloughed, lost job), and 33.0% were key workers. 22.8% had caring responsibilities and 4.3% had dependents under 5 years at home. 21.7% had a pre-existing mental health condition and 7.6% had a pre-existing physical health condition. Compared with men with no vaccine hesitancy, men with vaccine hesitancy were more likely to be in the lower SEG, having caring responsibilities, and have a mental health condition, factors which may make them more vulnerable to poorer mental health.
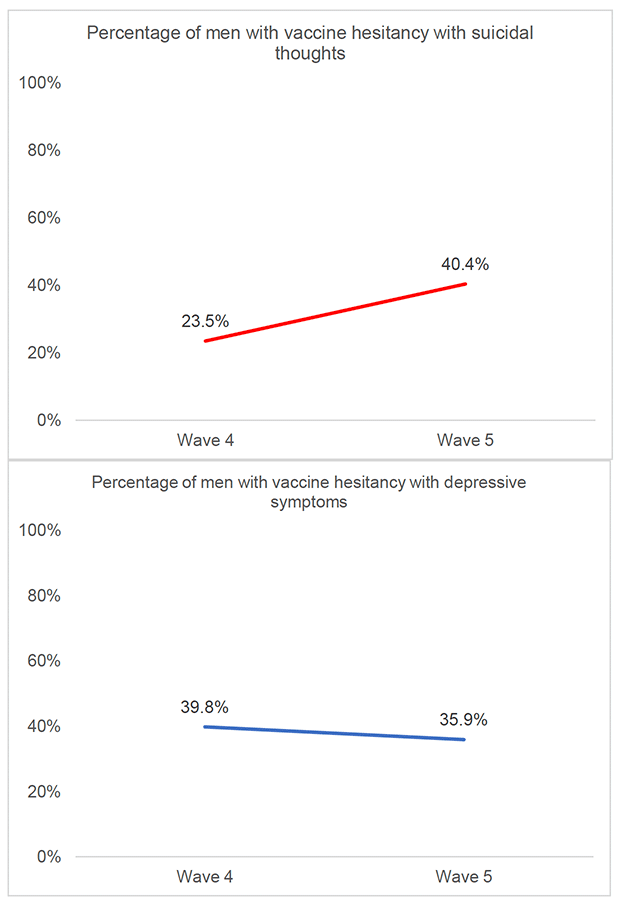
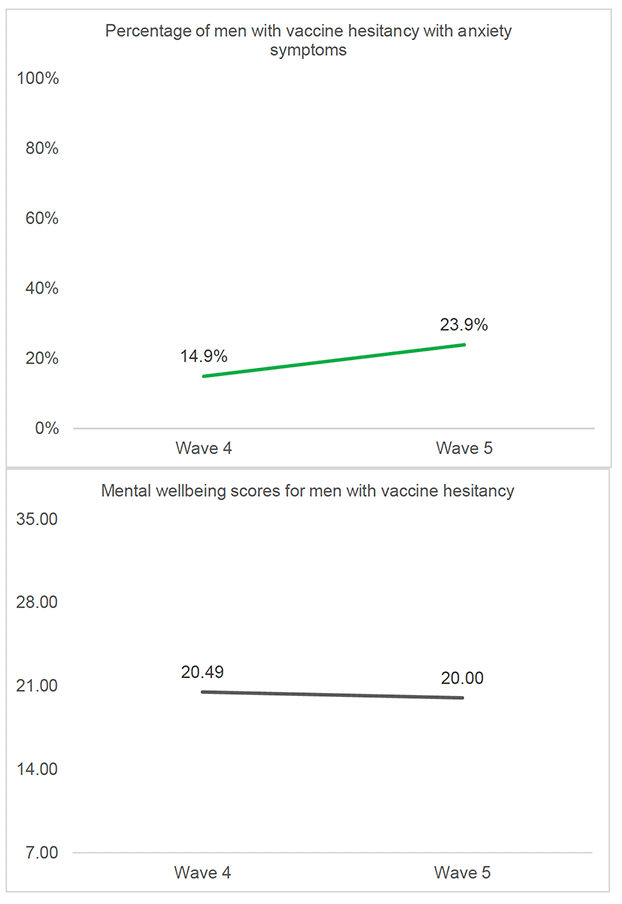
Findings from Wave 4 and Wave 5 of the SCOVID study suggest that men with vaccine hesitancy tended to be at higher risk of mental health problems than men with no vaccine hesitancy. For example, at Wave 5, 18.0% of men with no vaccine hesitancy reported depressive symptoms, compared with 39.8% of men with vaccine hesitancy (see Annex 4, Table F). Additionally, men with vaccine hesitancy reported higher rates of suicidal thoughts and depressive symptoms at Wave 5 compared with women who also had vaccine hesitancy.
Figure A4.3 illustrates mental health outcome trends (suicidal thoughts, depressive symptoms, anxiety symptoms, and the SWEMWBS wellbeing scores) for men with vaccine hesitancy at Wave 4 and Wave 5 of the SCOVID study. Looking at these trends in context of changes in pandemic restrictions, men with vaccine hesitancy reported the highest rates of suicidal thoughts, anxiety symptoms and lowest mental wellbeing at Wave 5 (June - July 2021), a time that coincided with restrictions being eased. Therefore, it appears the mental health of men who were vaccine hesitant overall was poorer when restrictions were not in place. As a booster sample was added at Wave 5, this finding should be interpreted with caution as this is a sample is made up of different participants than at the previous waves.
Contact
Email: socialresearch@gov.scot