National cancer plan: progress report - August 2022
Scotland's national cancer plan comes to completion in March 2023. This report uses insights from the available evidence to update on progress against all 68 actions in the plan as at 31 August 2022.
Cancer Plan Progress Updates: Detection and Diagnosis
Data on Detection and Diagnosis
Scottish Breast Screening Programme
The latest release of data by Public Health Scotland provides an update of breast screening statistics to 31 March 2021. These data include: Scottish Breast Screening Programme performance standards, attendance figures, cancer detection rates, biopsy results and screening outcomes. The reporting period (2018/19 - 2020/21) includes the pause to the programme between March and August 2020 when no individuals were invited to breast screenings.
Screening invitations and uptake in three-year period 2018/19 - 2020/21
- For the three year period from 2018/19 to 2020/21, 675,381 women aged 50-70 were invited to attend a routine breast screening appointment. This number is lower than expected due to the pause to screening.
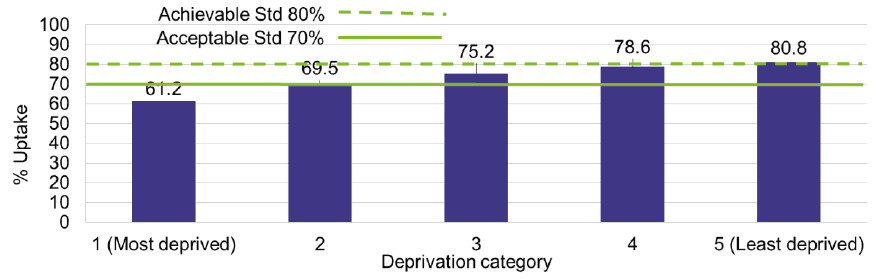
- More than seven in ten women (73%) took up their invitations from 2018/19 to 2020/21. This is a slight increase from the previous three-year period (72%).
- For the one-year period of 2020/21, Scotland had an uptake rate of 75.1%.
- There was a 20 percentage point uptake gap between the most (61%) and least (81%) deprived areas, a trend similar to the previous period. See Figure 6 below.
Screening invitations in 2020/21 compared to the yearly average
- In 2020/21, 151,977 women aged 50-70 were invited for screening. This number is lower than the yearly average of 259,940 reported since 2017.
Invasive breast cancer detection rates and breast cancer registrations
NHS Inform provides information about breast cancer in females and in males. The most common form of breast cancer is invasive ductal breast cancer, which develops in the cells that line the breast ducts. Invasive ductal breast cancer accounts for about 80% of all breast cancer cases and is sometimes called 'no special type'. Invasive cancer has the ability to spread outside the breast, although this does not necessarily mean it has spread. The phrase ‘breast cancer registrations’ refers to new cases of breast cancer registered in the three-year period reported here.
- Invasive breast cancer detection rates remained relatively stable across the three-year period (2018/19 - 2020/21).
- In 2020/21, invasive breast cancer detection rates rose across age groups when compared to the previous year.
- For the last 10 years, 53% of breast cancer registrations in women aged 50-69 were detected through the programme, but this dropped to 39% in 2020, as referenced in Public Health Scotland’s latest report on cancer incidence in Scotland (April 2022).
* The Scottish Index of Multiple Deprivation is a tool to identify places in Scotland where people are experiencing multiple disadvantage.
Summary of key points
Capacity within the breast screening programme continues to be challenging due to COVID-19 and the pause to the programme in 2020. However, uptake for breast screening has increased in the most recent three-year period (2018/19 - 2020/21), with invasive cancer detection rates remaining relatively stable across this period. The latest annual programme statistics published in April 2022 showed that uptake has risen from 72% to 75.1% between 2019/20 and 2020/21. In 2020/21, invasive cancer detection rates rose when compared to the previous year. However, in 2020 there was a reduction in the percentage of breast cancer registrations in women aged 50-69 that were detected through the screening programme. This decrease is likely to be due to the pause in screening. Uptake rates are highest in areas of lowest socioeconomic deprivation, reflecting persisting health inequalities.
Scottish Bowel Screening Programme
NHS Inform provides information about bowel cancer. The latest release of data by Public Health Scotland provides an update of bowel screening statistics in relation to key performance indicators for the Scottish Bowel Screening Programme to April 2021. These data include: uptake, laboratory and clinical outcomes of screened individuals. The reporting period (for those invited from 1 May 2019 to 30 April 2021) includes the pause to the programme between March and October 2020 when no individuals were invited to participate in bowel screenings.
Screening invitations and uptake, 1 May 2019 to 31 April 2021
- For the two-year period from 1 May 2019 to 30 April 2021, 1.4 million people were invited to participate in routine bowel screening. This number is lower than the previous two-year period (1.8 million) due to the pause to screening. Eligible people were posted a screening kit that is completed at home. Since 1 April 2013, those aged over 74 can self-refer and opt in to bowel screening.
- More than six in ten people (65%) took up their invitations, which is the highest uptake rate in the programme's history.
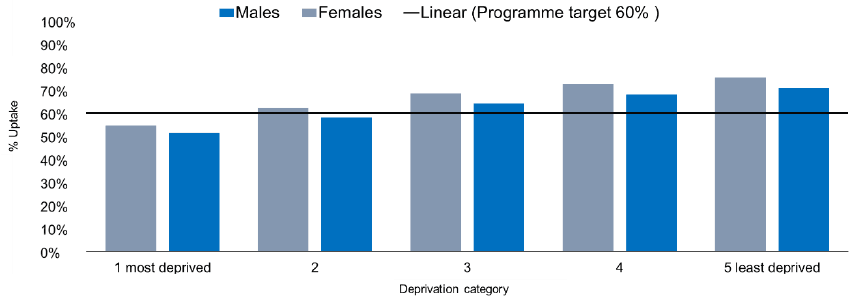
- Uptake was higher in females (67%) than males (63%), though both were above the Health Improvement Scotland standard of 60%.
- There was a large (20%) uptake gap between the most (53%) and least (73%) deprived quintiles, which is a slight decrease from the figure in 2018 (23%). See Figure 7 below.
* The Scottish Index of Multiple Deprivation is a tool to identify places in Scotland where people are experiencing multiple disadvantage.
Colonoscopies performed after positive referral, 1 May 2019 to 31 April 2021
The proportion of colonoscopies performed within four weeks of a positive referral was 39%, an increase of 11 percentage points compared to the previous report. 34% were seen in four to eight weeks, and 27% in more than eight weeks.
- 72% of those with a positive referral went on to receive a colonoscopy within the time period, a reduction of 1% versus the previous report. This was slightly higher in males (73%) than females (72%).
Summary of key points
There was a reduction in overall numbers screened for bowel cancer due to the pause to the programme in 2020. Uptake for bowel screening was the highest in the programme’s history. Uptake rates are highest in women and in areas of lowest deprivation. There was a slight decrease in the overall proportion of those with a positive referral who went on to receive a colonoscopy, although there was an increase in the proportion performed within four weeks of a positive referral.
Scottish Cervical Screening Programme
NHS Inform provides information about cervical cancer. The latest release of data by Public Health Scotland provides an update of cervical screening statistics to 31 March 2021. This release provides annual and quarterly statistics on uptake by age group, NHS board, deprivation and human papillomavirus (HPV) immunisation status. In addition, data are presented on laboratory turnaround times, number of screening tests and results of tests by NHS board and laboratory. For the period reported, cervical screening was routinely offered to women aged 25-64 in Scotland: those aged 25-49 every three years and those aged 50-64 every five years. The reporting period (from 1 April 2020 to 31 March 2021) includes the pause to the programme between March and June 2020 when no individuals were invited to cervical screenings.
Uptake for screening, 1 April 2020 to 31 March 2021
- The population offered cervical screening comprised eligible women aged 25-49 plus eligible women aged 50-64, reflecting the different frequency of the screening offer by age group.
- Uptake of cervical screening is the percentage of eligible women who were screened adequately within the specified period. The uptake rate in 2020-21 was 69.3%, with just over one million eligible women having participated.
- Uptake has declined in recent years. The 2020-21 rate is down 1.9 percentage points when compared to the previous year.
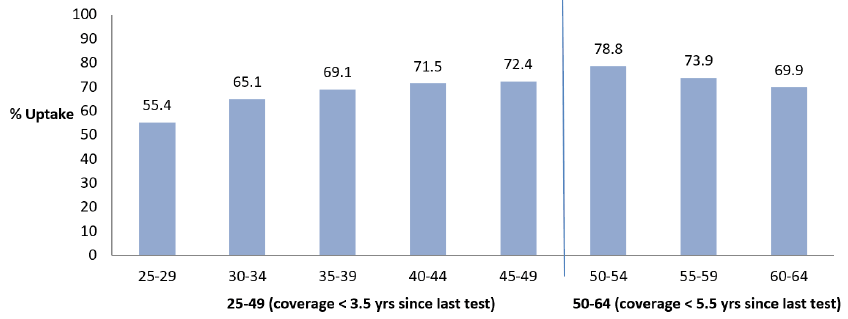
- Uptake increased with age: from 55% for ages 25 to 29, to a peak of 79% in those 50 to 54 years, before reducing in the oldest invited age groups. See Figure 8 below.
- There was an 11 percentage point uptake gap between the most (63%) and least (74%) deprived areas.
- Cervical screening uptake is higher in HPV-vaccinated women aged 24-29 (68%) when compared to non-vaccinated women in this age group (32%). The majority of cervical cancers are caused by HPV infection.
Results for those testing positive for HPV, 1 April 2020 to 31 March 2021
- Of those testing positive for HPV, around two thirds (65%) were negative with no sign of abnormal change in cells, 30% identified low grade cell changes and 5% of these women were identified as having high grade cell changes, including cervical cancer.
Cervical Screening Processing, 1 April 2020 to 31 March 2021
- There were 174,299 cervical screening tests processed within the programme. This is noticeably lower than previous years and is at least in part due to the pausing of the screening programme in response to the COVID-19 pandemic, and due to changes in the programme age range.
Summary of key points
The pandemic resulted in a temporary pause to screening from March to June 2020. The impact of this pause can be seen in the laboratory samples processed, and is likely to have influenced uptake figures. Uptake for cervical screening has declined in recent years. Uptake rates are highest in women aged 50 to 54 years, amongst HPV-vaccinated women in the 24-29 age group and in areas of lowest deprivation.
Diagnostic Demand and Waiting Times
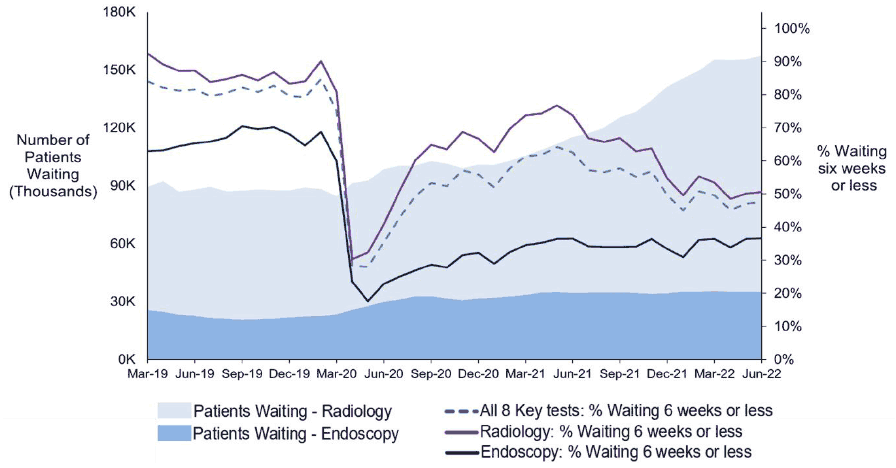
Quarterly releases by Public Health Scotland provide data on the number of patients waiting for one of eight key diagnostics tests and investigations and the time they have waited. The eight key tests and investigations are upper endoscopy, lower endoscopy (excluding colonoscopy), colonoscopy, cystoscopy, Computerised Tomography (CT) scan, Magnetic Resonance Imaging (MRI) scan, barium studies and non-obstetric ultrasound. These statistics provide information about diagnostic demand and waiting times for endoscopy and radiology tests which can affect patients referred to services for suspected cancer. Figure 9 below shows the trend across time in the number of patients waiting and the percentage of patients waiting six weeks or less at month-end, for endoscopy and radiology tests. Patients with an urgent suspicion of cancer continue to be prioritised within these overall referrals (see below information about Waiting Times for Cancer Treatment: 62-day standard from urgent referral on suspicion of cancer to treatment).
At 30 June 2022, for all referrals, including cancer patients:
- 157,289 patients were waiting to be seen for one of the eight key diagnostic tests, an increase of 1.2% from 31 March 2022 and 77.9% from the average in the 12 months prior to the pandemic (from March 2019 to February 2020).
- Of those waiting, 47.5% had been waiting six weeks or less (42 days), a decrease from 49.6% reported at 31 March 2022.
- 34,935 patients were waiting for an endoscopy, a decrease of 0.9% from 31 March 2022 but still 56.3% higher than the pre-pandemic average.
- Of those waiting, 36.6% had been waiting six weeks or less, which remains similar to the 36.4% reported at 31 March 2022 but is markedly down on the 66.7% 12-month average prior to the onset of the pandemic.
- The percentage of patients waiting 52 weeks or over for an endoscopy test increased slightly from 15.2% at 31 March 2022, to 15.5% at 30 June 2022.
- 122,354 patients were waiting for a radiology test, an increase of 1.8% from 31 March 2022 and 85.2% from the average in the 12 months prior to the pandemic.
- Of those waiting, 50.6% had been waiting six weeks or less (42 days), lower than both 53.5% at 31 March 2022 and the pre-pandemic average of 86.6%.
- The percentage of patients waiting 26 weeks or over for a radiology test increased from 4.1% at 31 March 2022 to 5.2% at 30 June 2022.
Summary of key points
The latest quarterly figures for waiting times (as at 30 June 2022) for all patients, including cancer patients, show an overall increase in the number of patients waiting for the eight key diagnostic tests, compared to previous quarterly figures. Services continue to be affected by the impact of the pandemic, such as reduced services due to increased staff absences. The number of patients on the waiting list for endoscopy and radiology tests remain above pre-pandemic levels. In addition, the proportion of patients waiting six weeks or less is higher for radiology tests compared to endoscopy tests.
Waiting Times for Cancer Treatment
Public Health Scotland releases the quarterly update of cancer waiting times statistics, reporting two National Standards on how long patients waited for their first cancer treatment. These statistics cover patients who started their first treatment by quarter ending 31 March 2022. Figure 10 below shows performance against the 62 and 31-day standards over the previous decade.
The 62-day standard states that 95% of eligible patients should wait a maximum of 62 days from urgent suspicion of cancer referral to first cancer treatment. Eligible patients for this standard are those urgently referred with a suspicion of cancer by a primary care clinician, general dental physician, patients referred by one of the national cancer screening programmes, and direct referrals to hospital where the signs and symptoms are consistent with the cancer diagnosed, as per the Scottish Referral Guidelines e.g., self-referral to Accident and Emergency.
The 31-day standard states that 95% of all patients should wait no more than 31 days from decision to treat to first cancer treatment. This standard applies to all patients, regardless of the route of referral.
Performance on 62-day standard: from urgent referral to treatment, quarter ending 31 March 2022 (Quarter 1, 2022)
- There were 3,861 eligible referrals for the 62-day standard (Quarter 1, 2022), a decrease of 6.8% from the previous quarter (Quarter 4, 2021), but a 7.6% increase compared with quarter ending 31 March 2021.
- 76.9% of patients started treatment within the 62-day standard, compared with 79.1% in the previous quarter and 83.0% for quarter ending 31 March 2021.
As shown in Figure 10 below, the 62-day standard was last met in 2012 Q4.
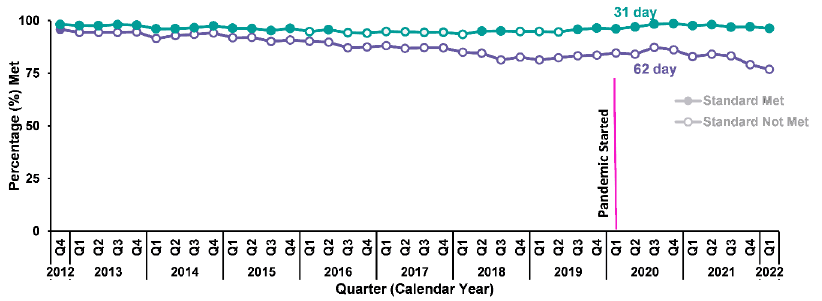
Performance on 31-day standard: from decision to treat to treatment, quarter ending 31 March 2022 (Quarter 1, 2022)
- There were 5,996 eligible referrals within the 31-day standard (Quarter 1, 2022), a decrease of 6.2% from the previous quarter (Quarter 4, 2021), but a 3.5% increase compared with quarter ending 31 March 2021.
- 96.3% of patients started treatment within the 31-day standard, compared with 97.1% in the previous quarter and 97.7% for quarter ending 31 March 2021.
Actions for Screening and Surveillance
Action 9 – Deliver the Screening Inequalities Fund
Commitment: We will tackle inequalities, including those that have been exacerbated by the COVID-19 pandemic, in the uptake and access to national population screening programmes. The Scottish Government committed £2 million over 2021-23 for this work.
Progress: The Scottish Government is investing a further £2 million over 2021/22 and 2022/23 to build a programme of evidence-based, sustainable and scalable projects that tackle inequalities in a systemic way. It also recognises that the pandemic is likely to have exacerbated screening inequalities. This includes dedicated screening inequalities resource in National Screening Oversight and funding being allocated directly to all health boards. This is intended to be recurring funding subject to future budget approvals. Additionally, in response to declining uptake rates for cervical screening, cervical marketing campaigns have run in October 2021 and March 2022, and funding has been provided to Jo’s Cervical Cancer Trust, to tackle barriers and improve uptake rates for cervical screening.
Action 10 – Develop a programme of work and pilot approaches to vaginal self-sampling
Commitment: To broaden the reach of the cervical screening programme and address inequalities, we will develop a programme of work and pilot approaches to vaginal self-sampling. This will enable us to explore and determine the potential for the use of self-sampling at national level.
Progress: To date, there has been insufficient evidence for the UK National Screening Committee to recommend the implementation of self-sampling; they recommended that further work is needed to consider how best to achieve this. A Dumfries and Galloway study will inform this, along with other projects from across the UK and review of international findings. The Dumfries and Galloway study was undertaken in NHS Dumfries and Galloway, sending a vaginal self-sampling kit to all screening participants aged 25-64 years of age who have either i) never attended for cervical screening or ii) who have not attended their most recent appointment. Timescales for reporting results were extended due to the impacts of COVID-19. However, the interim findings were encouraging, and the final report is awaited.
A Short Life Working Group has been established to lead a wider project to contribute to the evidence base for national rollout. Once developed, this evidence base will be shared with the UK National Screening Committee and will inform their future decisions on whether to rollout this approach across the UK.
Action 11 – Develop guidance for surveillance of at risk patients
Commitment: To develop guidance for monitoring surveillance and follow-up services for individuals with either specific gene mutations or otherwise increased clinical risk of developing cancer.
Progress: Since the start of the pandemic, the Scottish Government has worked with Health Boards and relevant stakeholders to identify if national guidance is needed on the delivery of services for high risk cancer surveillance and follow-up screening checks. To date there have been no areas of concern highlighted so guidance is unchanged.
Actions for Diagnostic Testing
Flagship Action
Action 12 – Improving the diagnostic experience – Rapid Cancer Diagnostic Services (formerly known as Early Cancer Diagnostic Centres)
Commitment: To invest up to £3 million into Scotland’s first Rapid Cancer Diagnostic Services (formerly known as Early Cancer Diagnostic Centres), which will provide primary care with access to a new timely, person-centred fast-track diagnostic pathway. The Services – established within existing NHS infrastructure - will enable patients with non-specific but concerning symptoms to be assessed and, if appropriate, tested by a team of specialists in a coordinated manner, to help find cancer earlier.
The Services also aim to reduce variation in how cancer patients that present with non-specific symptoms access and move through NHS Scotland, compared to those with symptoms that meet the Scottish Referral Guidelines for Suspected Cancer. In Phase 1, we committed to establishing at least two sites within the first 100 days of the new parliament (Spring 2021). This will be accompanied by a robust evaluation to embed learning and support equitable access to a Service across Scotland.
Progress: A multi-disciplinary Rapid Cancer Diagnostic Service (RCDS – formerly known as Early Cancer Diagnostic Centres) Oversight Group was formed in October 2020 and met for the first time in December 2020. Three early adopter sites were established in NHS Ayrshire & Arran, NHS Fife and NHS Dumfries & Galloway by June 2021.
As a result of service user feedback (clinical and patients), the name was reviewed and changed to Rapid Cancer Diagnostic Services (RCDS) in September 2022. A two-year evaluation of RCDSs was commissioned to the University of Strathclyde and is expected early October 2023, with an interim report in October 2022.
The following unvalidated data was shared at the NHS Scotland Conference 2022 covering the first nine months of the Services:
- Over 720 referrals have been received (over 500 accepted).
- Around 16% conversion rate to cancer.
- Around 20% conversion to non-cancer conditions.
- The most common symptom at the point of referral is unexplained weight loss (58%).
- Around 64% of patients present with two or more non-specific symptoms at the point of referral.
Service users’ (patients and primary care clinicians) experiences of the RCDSs are being constantly monitored via an independent anonymous system to allow the Services to adapt and evolve over time, ensuring they deliver a truly person-centred pathway. To date, satisfaction rates have been high with positive anecdotal feedback emerging from Health Boards.
“I would have struggled – I had already referred to several specialties.”
GP, NHS Fife
“The diagnosis turned out to be rare. There is no way that I could have figured out which department to send him to without lots of trial and error.”
GP, NHS D&G
“This might have been tricky – some ref Care of the elderly or a medical speciality – this service is brilliant though and really appreciated. I have referred five patients and three had cancer – one not but she needed that wider investigation, and one pending.”
GP, NHS Fife
A nationally agreed dataset ensures the same data points and milestones are captured across RCDSs for evaluation purposes. The National Oversight Group continues to meet quarterly to share best practice, explore common challenges and work towards equitable access to the Services.
Boards that do not host an early adopter site were invited to submit expressions of interest in establishing a RCDS in Spring 2022, with fuller proposals then developed to enable clinical consultation. Ensuring that learning from the three early adopter sites is embedded in any future models is key.
Action 13 – Scanners
Commitment: Radiology investigations for suspected cancer patients have continued to be prioritised throughout the COVID-19 pandemic. However, as other services begin to re-mobilise, additional capacity will be required. This will be supported by the addition of six mobile Magnetic Resonance Imaging (MRI) and three mobile Computerised Tomography (CT) scanners.
Progress: All mobile MRI and mobile CT scanners committed were supplied within the first year of the National Cancer Plan. As of this financial year, six mobile MRI scanners and five CT scanners are in place across NHS Scotland to reduce backlogs and waiting times, with urgent suspicion of cancer (USC) referrals continuing to be prioritised.
Action 14 – Every Health Board in Scotland will have a GP direct access to Computerised Tomography pathway
Commitment: To continue to work with, and encourage, Health Boards to increase GP direct access to CT scans for people with symptoms potentially indicative of cancer, helping more people be tested more quickly.
Progress: Few Health Boards remain with no established direct access to CT pathway but work is underway to develop a national protocol to help reduce variation in access. This is a collaborative effort across primary and secondary care, cancer and imaging teams. Progress is monitored through regular performance management meetings with Boards and updates provided to the National Cancer Recovery Group.
Action 15 – Evaluate the efficiency of Cytosponge™ & Colon Capsule Endoscopy
Commitment: We will introduce Colon Capsule Endoscopy and Cytosponge™
across Scotland, and evaluate their efficacy and impact on patient outcomes. Combined with early detection, these innovative endoscopy solutions have the potential to reduce demand on traditional, more invasive, endoscopy techniques, improve patient experience, and increase screening capacity.
Progress: Colon Capsule Endoscopy (CCE) has been adopted by ten territorial Health Boards. Adoption work is underway with the remaining four Health Boards. There have been over 2800 procedures (post-evaluation study) carried out up to August 2022.
Patients who underwent CCE and who completed a survey about their experience have indicated high levels of satisfaction. 1499 patient responses were received across the 10 operational Health Boards for the period to August 2022 (return rate of 58.2%). 1203 (80%) responses indicated a “Very Good” experience during the procedure.
Cytosponge™ has been implemented in 11 out of 14 territorial Health Boards. By August 2022, over 4600 procedures have taken place. Following implementation in mainland Health Boards, the procedure will be implemented in the island Health Boards. As at August 2022, 39 Cytosponge trained nurses have been trained across 11 Health Boards.
A Cytosponge IT platform (SCOTIA) went live in September 2022. Work is ongoing to integrate the SCOTIA platform with mainland Health Board IT systems. A Cytosponge Registry (RedCap) is being developed to capture information on all patients across Scotland. The Registry will be live by November 2022. Data from the Registry will in due course provide information on patient demographics, procedure data, and long-term outcomes from all NHS Scotland Health Boards.
Action 16 – Convene the oversight group to develop the Endoscopy Renewal Plan
Commitment: To ensure patients have timely access to key diagnostic tests, we will support the creation of an Endoscopy Renewal Plan with the oversight group due to meet in early December. The role of Quantitative Faecal Immunochemical Test (qFIT), a simple test used to detect small amounts of blood in stool samples, in risk-stratifying those for endoscopy will be reflected in the Plan. The possibility of utilising the private sector to increase capacity, Health Boards supporting each other through mutual aid, ongoing clinical prioritisation and national guidance on COVID-19 testing patients pre-procedure, will also be considered in the Plan.
Progress: The Endoscopy and Urology Diagnostic Elective Care Group was convened in December 2020 to provide oversight. The group has since had oversight for the development of the Endoscopy and Urology Diagnostic Recovery and Renewal Plan that was published with a delivery plan in November 2021. Additional capacity continues to be provided for endoscopy via a range of options.
The following guidance and pathways have been published:
- qFIT guidance (Primary and Secondary Care) for patients with colorectal symptoms now published on the Scottish Government website and Turas (NHS Education for Scotland's digital platform).
- New Scottish urgent suspicion of colorectal cancer referral guideline published
- Haematuria pathway revised and SCRG Bladder and Kidney section of the referral guidance has been updated.
The Plan continues to deliver on its actions and will run until March 2025, overseen by the Endoscopy and Urology Diagnostic Programme Board.
Action 17 – Gallium scanner roll-out
Commitment: We will invest an initial £2 million in Gallium services to detect advanced prostate cancer across four Health Boards. Two services will go live in 2020 and the remaining two early in 2021.
Progress: Gallium scanners are up and running in three Health Boards. The remaining scanner has been delayed to provide Gallium Positron Emission Tomography (PET) scanning but has been able to use Prostate-specific membrane antigen (PSMA) PET scanning for prostate cancer since January 2021. Where Gallium PET scanning is required for a small number of patients, the Board is able to refer to neighbouring Health Boards.
Action 18 – National Cancer Diagnosis Audit
Commitment: To continue to support the National Cancer Diagnosis Audit to enable reflection, learning and quality improvement within primary care. This will improve patient outcomes and support earlier diagnosis.
Progress: The National Cancer Diagnosis Audit (NCDA) was completed and published on 3 August 2021. The audit covered a total of 2,318 patients diagnosed with cancer in Scotland during the year 1 October 2018 to 30 September 2019.
Ninety GP practices in Scotland (almost 10%) participated in NCDA 2019/20. This compares with 73 Scottish practices in the previous NCDA 2016/17. The Audit has resulted in a series of direct, tailored feedback reports to participating GP practices, who volunteered to take part.
The University of Aberdeen has been funded through the Detect Cancer Early (DCE) Programme to undertake an analysis of audit data to better understand referral patterns and the symptom profile of those diagnosed with lung cancer and those who experienced non-specific symptoms. Results of this study are due in late 2022 and will be shared with the RCDS Oversight Group and other interested groups.
Actions for Pre-Treatment
Action 19 – Audit of Scottish Referral Guidelines for Suspected Cancer
Commitment: An audit of the adoption of the Scottish Referral Guidelines for Suspected Cancer (refreshed in 2018, published in 2019) will be undertaken in Spring 2021, to understand any differing referral trends following the refresh.
Progress: The University of Aberdeen has been funded to undertake an analysis of National Cancer Diagnosis Audit data. This analysis will provide insights into primary care referral patterns pre and post the Guidelines refresh. A report is expected late 2022, with delays due to access to the safe haven (a secure environment for NHS electronic data).
Urgent suspicion of cancer (USC) referrals continue to be monitored through weekly cancer waiting times data collection with Health Boards. Public Health Scotland currently collect these data and plan to publish referral data alongside cancer waiting times in 2023 to show the true demand coming into the system (not just the numbers diagnosed with cancer).
More recently, the Guidelines have been updated for lower GI cancers to include the use of Quantitative Faecal Immunochemical Testing (qFIT) in clinical triage, and Urological cancer guidelines have been updated to include reference to the new haematuria guidance produced nationally.
Action 20 – Refresh of the Framework for Effective Cancer Management
Commitment: To undertake a refresh of the Framework for Effective Cancer Management by Summer 2021. This will help Boards incorporate new ways of managing cancer pathways and services across NHS Scotland that have emerged as a result of COVID-19.
Progress: The Framework for Effective Cancer Management has been refreshed and was published 3 December 2021. Health Boards have since developed action plans outlining how each element of the Framework will be adopted. Face-to-face visits with the National Framework Consultant have started, with six Boards undertaken so far. These visits provide Health Boards with hands on support and recommendations to improve patient experience and cancer waiting times. Further tailored visits are expected in 2022/23 and beyond to fully embed the Framework. The Chief Operating Officer of NHS Scotland wrote to Health Board Chief Executives in July 2022 to reinforce cancer as a priority and request monthly progress updates, to ensure action plans are on track. Implementation is also monitored through monthly and Quarterly Cancer Waiting Times as the aim is to ultimately improve and sustain performance.
Action 21 – Increased oversight of Cancer Waiting Times
Commitment: Alongside responding to any new COVID-19 peaks, we will continue increased oversight of patients moving through the 31 and 62 day cancer pathways through weekly monitoring with Boards. This involves tracking referral numbers, sharing best practice across Board Cancer Teams, challenging any emerging backlogs and supporting innovative solutions where appropriate.
Progress: Weekly calls continue with mainland Health Boards’ Cancer Teams (monthly for Island Boards). This equates to over 800 calls a year, tracking urgent suspicion of cancer (USC) referrals, collectively exploring solutions to service challenges and sharing best practice across boundaries. In 2021/22, £10 million was released to support Cancer Waiting Time improvements, with the same level of investment confirmed in 2022/23. This investment focuses on the most challenged pathways, in particular, urology and colorectal. The Cancer Delivery Board, which reports to the Integrated Planned Care Programme Board, established in 2022, provides national governance for cancer performance.
Action 22 – Review and redesign patient pathways
Commitment: We will analyse whether new pathways for specific cancers would benefit patients. A focus will be placed on less survivable cancers. Our first priority will be to work with the Scottish Hepatobiliary Network and support clinical consensus on redesign of pancreatic and liver cancer pathways.
Progress: The Pancreatic & Hepatocellular Cancer – Pathway Improvement Project (PHCC-PIP) was launched at the NHS Scotland Event in May 2022. A new cancer care team, comprising 2 Nurse Specialists and 3 Care Co-ordinators, are in post. A high level plan has been agreed for the daily pancreatic consultant rota. A retrospective baseline audit of patient experience for those whose treatment began between March-May 2022 is under way. Preparatory work continues and a ‘go-live’ date will be confirmed soon, whereby early specialist review of radiology findings will be flagged by the care team and coordinators will act as a single point of contact for patients.
Action 23 – Form the urology optimal pathway
Commitment: A collaboration of Scottish Government improvement programmes through the Centre for Sustainable Delivery (CfSD) (including Scottish Access Collaborative and Modern Patient Pathways Programme) will explore ways to reduce variation in urology pathways and ensure equitable access from the point of suspicion of cancer to post-treatment follow-up.
Progress: This work was undertaken by the Endoscopy and Urology Programme Board through the Urology Clinical Forum. We have undertaken a clinical review of urology pathways and updated the National Non-Visible and Visible Haematuria pathways. Simultaneously, we have updated the Scottish Cancer Referral Guidelines (SCRG). The pathways have been published on Turas with links to the SCR guidance.
Work is progressing with the review of the National Urinary Tract Infection (UTI) pathways. We have recently opened two new Urology Hubs, providing new pathways to support rapid access to cystoscopy within a ‘One Stop’ clinic model and same day diagnosis.
Flagship Action:
Action 24 – Cancer Prehabilitation – Testing and evaluating
Commitment: The Scottish Government aims to spearhead prehabilitation, which helps patients prepare for cancer treatment. It will invest up to £1.15 million to implement a programme of work in a number of cancer types, to test and evaluate the concept for delivery across Scotland. The evaluation will focus on implementation of prehabilitation within existing pathways with access to timely treatment remaining a priority.
Progress: A Cancer Prehabilitation Implementation Steering Group (CPISG) is in place and is leading on developing and supporting the effective national roll-out of cancer prehabilitation across Scotland. It has developed the Key Principles for Implementing Cancer Prehabilitation across Scotland which are now available online (see Action 25). They include a principle that prehabilitation should be multi-modal including exercise/activity, nutrition and psychological support.
The Health and Social Care Alliance used the findings of four focus groups undertaken in 2021 with people affected by cancer to inform recommendations to the Scottish Government on proposed cancer prehabilitation services. Recommendations included the need for continued engagement with people affected by cancer; for those people to have access to flexible, person-centred nutritional, physical and psychological support; and for careful messaging to promote the benefits of such interventions. In its response, the Scottish Government committed to addressing those recommendations, which have informed its approach to developing prehabilitation services.
The CPISG has undertaken a survey of service providers whose work contributes or is relevant to cancer prehabilitation. The findings will help CPISG understand the current and planned prehabilitation position within Scotland and identify future requirements, thereby also informing Scotland's new Cancer Strategy. This survey builds on a similar one undertaken in 2019 and seeks to understand the impact of the COVID-19 pandemic on prehabilitation in Scotland.
Maggie’s Workshops
Maggie's have been funded to deliver pilot projects in eight centres across Scotland, offering prehabilitation workshops to people who have been diagnosed with cancer. The workshops are open to all those recently diagnosed and people can self-refer or be referred by their clinical team. An evaluation of the pilot projects is under way. Between 1 November 2021 and 30 June 2022, 515 individuals attended the centres. Evaluation using the Patient Activation Measure showed that prehabilitation was having a positive impact on patients, including increasing their engagement with their own health. Maggie’s have also developed a film 'Getting ready for treatment', which explains how people in Scotland can ‘get ready’ for what’s ahead after a cancer diagnosis.
Action 25 – Develop digital resource to raise awareness of prehabilitation
Commitment: We will develop a digital resource to raise awareness of the benefits of prehabilitation among the public and professionals.
Progress: The website Prehabilitation for Scotland was launched in May 2022. It includes information for the public about prehabilitation, including the three key components of nutrition, physical activity/exercise and psychological support. Information for professionals includes the Key Principles publication and links to education and training resources. It is designed to support everyone affected by cancer by providing access to first-line information and to highlight wider support available. The website will continue to develop over time in response to feedback.
Action 26 – Convene a Nutritional Cancer Care Advisory Group
Commitment: We will convene a Nutritional Cancer Care Advisory Group to develop a framework for nutritional care to be used across cancer prehabilitation in Scotland.
Progress: The Advisory Group has been established. This multi-disciplinary, collaborative group comprises representatives from NHS Boards and third sector organisations. Collectively, they have been working to develop the framework for nutritional care and publication, which is expected in Autumn 2022. Once developed, the ‘Nutrition Framework for People Affected by Cancer’ will define the level of nutritional care that should be available to all adults affected by cancer in Scotland (ages 16 years and above) and provide a structure for delivery of care.
Action 27 – Identify ‘best learnings’ from the West of Scotland’s Psychological Therapies and Support Framework
Commitment: To ensure consistency of support across Scotland, we will look to the well-established West of Scotland’s Psychological Therapies and Support Framework to identify potential learning which can be adopted across the country.
Progress: Using the West of Scotland framework as a starting point, the new national Psychological Therapies and Support Framework for people affected by cancer was developed by a multi-disciplinary group, which included representatives from Health Boards, Third Sector organisations and Social Care organisations. The Framework was published in April 2022.
The overall aim is to bring existing services together in a collaborative manner and illustrate a good practice model thereby providing equitable and efficient access to the appropriate services for people affected by cancer. In addition to setting out best practice, practical steps to facilitate person-centred psychologically-informed care are included alongside a new tool to help audit and demonstrate the quality of service.
Contact
Email: CancerPolicyTeam@gov.scot