Coronavirus (COVID-19) domestic vaccine certification: children's rights and wellbeing impact assessment
Children's rights and wellbeing impact assessment (CRWIA) considering the ways which the domestic Covid vaccine certification scheme may engage the rights of children and young people protected under the United Nation's Convention on the Rights of the Child.
Scope of the CRWIA, identifying the children and young people affected by the policy, and summarising the evidence base
Scope and summary of impacts
The UN Convention on the Rights of the Child (UNCRC) defines a child as anyone under the age of 18. The child wellbeing indicators under the Children and Young People (Scotland) Act 2014 reflect the principles within the UNCRC and also apply to all children up to the age of 18 and so all children are within the scope of this CRWIA.
All children would benefit from a reduction in the transmission of Covid-19. Children would also benefit from an increase in vaccination within the adult population, as this would increase overall community protection. As demonstrated in the summary of evidence below, disabled children and children from minority ethnic (ME) communities are most likely to positively benefit from a reduction in transmission and increased vaccine uptake, as evidence shows that these children have poorer health outcomes if they contract the virus.
All children would positively benefit from allowing higher risk settings to continue to operate as an alternative to closure or more restrictive measures, as evidence shows that their mental health and wellbeing declined during lockdowns and gradually improved as restrictions eased. Evidence within summary of evidence shows that the mental health and wellbeing of disabled children, minority ethnic (ME) children, young carers, LGBT youth and those from lower socio-economic backgrounds are most negatively impacted by restrictions and lockdowns. Therefore, it is likely that they would benefit most if Certification allows higher risk settings to continue to operate as an alternative to closure or more restrictive measures.
There could potentially be some unintended negative impacts on children and some groups of children may be impacted more than others, for example children who look 18 or older or those who do not have proof of age. Also, in the event that the policy exceeds the intention and children are denied access to spaces, services, products, employment or education because they do not have Certification. Finally, the impact on children of a parent, guardian or relevant adult who does not have certification.
While children are exempt from the requirement to prove vaccination status for domestic purposes, 12-17 year olds who have been vaccinated may choose to access their record of vaccination by downloading a PDF via NHS Inform or requesting a paper Certificate by calling the Covid-19 Status Helpline. The Privacy Notice is already online and can be found on NHS Inform: Personal information we process, How we use your data, Your Rights. The Easy Read Version can be found online.
More detail on each of the potential impacts can be found in the key findings section.
Summary of the evidence base
The direct and indirect harms of Covid-19 have also affected children. The summary of evidence below sets out the ways in which Covid-19 has both direct and indirect negative impacts on their health and wellbeing.
Direct harm from Covid
Evidence on the original Covid-19 strain suggested that children are less susceptible and at a lower risk of severe illness compared to adults.[8] [9] [10] Children of all ages are susceptible and able to transmit the Delta strain (B.1.617) of Covid-19, with transmissibility in 5-11 year olds most noticeably increasing.[11] It is still suggested that younger children transmit Covid-19 at a lower rate.[12] Data has also shown children aged between 1-18 years have lower rates of hospitalisation, severe disease requiring intensive hospital care, and death than all other age groups.[13]
Since the emergence of the Delta strain, we have seen an increase in cases and hospital admissions of children. In July, 12,000 new infections were recorded in children in the US, increasing to 94,000 by the first week of August with a record number of 1,902 children being admitted to hospital as of 14 August.[14] Figure 1 shows the % of children for total cases of Covid-19, hospitalisations and mortality in the US.[15] A British Medical Journal paper suggests that the same has not been seen in the UK, with the majority of children in hospital who are positive for Covid-19 actually being sick from a different illness.[16] However, since this report was published on 16 August 2021, the number of cases in children in Scotland, particularly aged 5-11 and 12-15, has increased along with hospitalisations (see Figure 2).[17] For people under 20, the percentage of cases made up of children under 12 in the week ending 5 September was just over 43% (7,462 cases) compared to just over 38% (5,344 cases) in the previous week.[18]
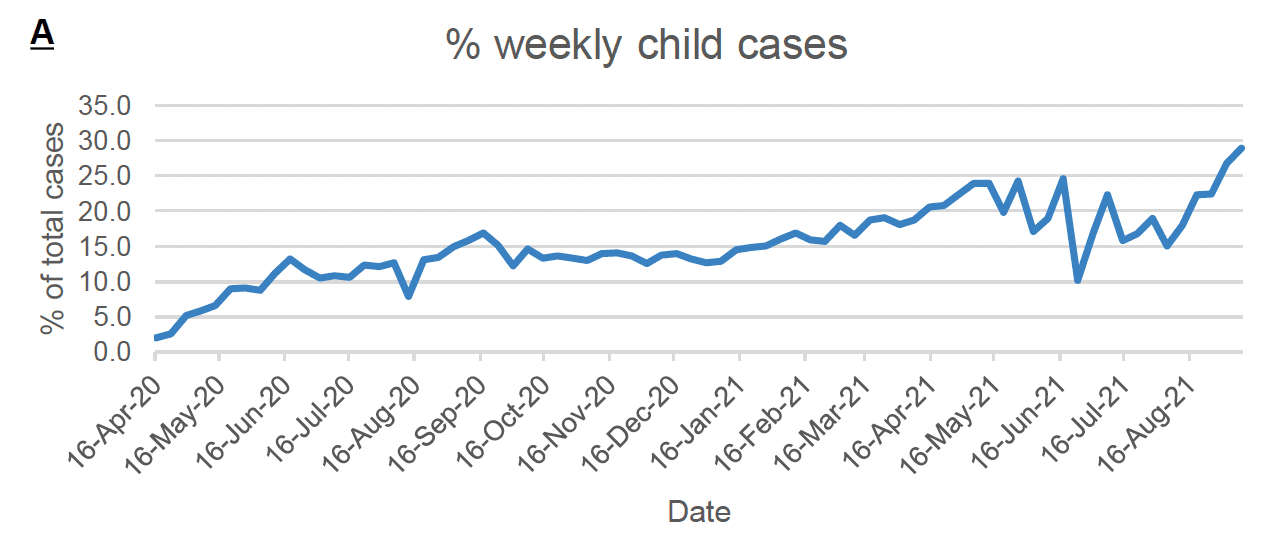
Source: PHS COVID-19 Education report (shinyapps.io).
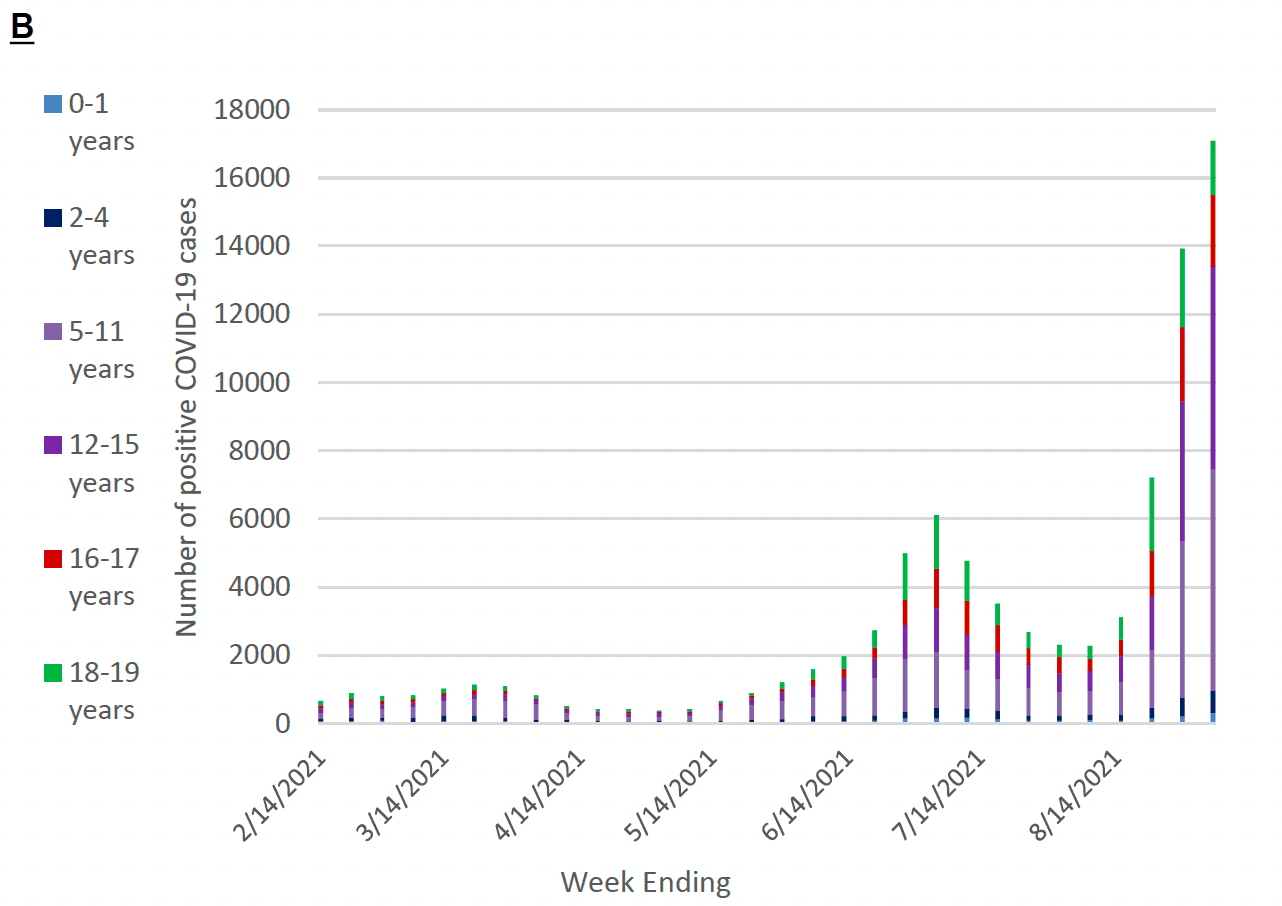
Source: COVID-19 and Age (aap.org)
Even with the recent evidence of an increase in cases and hospitalisations in children, there is high confidence that children are still a minority of all reported Covid-19 cases and moderate confidence that the increase in the share of reported cases among children are due to increased detection of mild cases.[19] Most children do not develop symptoms when infected with the virus, or they develop a very mild form of the disease. However, research has shown that children can become infected, and can spread the virus to other children and adults while they are infectious.[20]
Evidence suggests that adults and children with learning disabilities have markedly increased risks of hospital admission and death from Covid-19, and that this is particularly high for those with Down's syndrome and cerebral palsy.[21] On 3 September 2021 the Joint Committee on Vaccination and Immunisation advised that children aged 12-15 with specific disabilities and health conditions should be offered Covid-19 vaccination.[22]
People from minority ethnic groups in Scotland face significant societal and health inequalities and the pandemic has exacerbated existing health and wider inequalities. They are almost three times as likely than white groups to contract Covid-19 and five times more likely to experience serious outcomes. Evidence suggests this is largely due to social inequalities such as housing, occupational risk and access to healthcare.[23] Black, Asian or mixed-race children had a lower proportion of Covid-19 tests and higher proportion of positive results, Asian children were more likely to be admitted to hospital with confirmed Covid-19 and Black and mix-raced children were more likely to remain in hospital for 36 hours or longer, all relative to white children.[24]
Long Covid
On 22 July 2021 the Office of National Statistics (ONS) developed a short report on long Covid for SAGE. The report states that there is limited data for children, but the data available suggests that long illness duration after Covid-19 infection in school-aged children is uncommon, with around 2% experiencing symptoms at 8 weeks post infection.[25]
A recent report from the Academy of Medical Science (AMS) highlights that, to date, Multisystem Inflammatory Syndrome in Children (MIS-C) is the primary Covid consequence studied in children.[26] The AMS report also shows the results from the ONS survey, dated April to December 2020, which revealed that 12.9% of UK children aged 2 to 11 and 14.5% of children aged 12 to 16 have symptoms five weeks after their first infection. Symptoms include fatigue, muscle and joint pain, headache, insomnia, respiratory problems and palpitations, severe enough to affect daily activities in a high proportion. Studies have also identified immunological differences between children that completely recovered from acute infection and those with long Covid. It is important to note that many of the symptoms of long Covid are also common in the adolescent population (e.g. fatigue, headache). The degree to which long Covid will have longer-term implications for children's health and wellbeing remains unclear.[27]
Data from another study conducted by University College London and Public Health England (PHE) in September 2021 found that 14% of children who caught Covid-19 had symptoms linked to the virus 15 weeks later (unusual tiredness, symptoms of ill health and headaches) while 7% had 5 or more symptoms.[28]
Mental health and wellbeing
At the UK level, a PHE evidence report on mental health and wellbeing, drawing on data from the beginning of the pandemic up to January 2021, found that Covid-19 and associated interventions have likely had an adverse effect on the mental health and wellbeing of children and young people.[29] There is also increasing evidence that many children and young people are coping well overall and some have reported improvements in their mental health following the reopening of schools. Experiences vary by children and young people's characteristics, with those from Black, Asian and Minority Ethnic backgrounds, those with existing mental health conditions, those with Special Educational Needs and Disabilities, and those from low-income families more likely to have been negatively affected.
In terms of differential impact by age, a survey of 11 – 25 year olds carried out between the end of March and beginning of June 2021 found that 40% of respondents agreed that they felt good about their mental health and wellbeing, while 35% disagreed.[30] In a later survey of the same age group carried out between September and November 2020 many young people discussed the mental wellbeing benefits of being able to meet up with their friends again and not being confined to their homes.[31]
Another survey and focus group with 14 – 20 year olds undertaken between August and September 2020 found that 9% of young people responding to the survey met clinical threshold levels for depression, 7% for anxiety, and 28% were categorised as having elevated avoidance and intrusive thoughts and behaviours in relation to the Covid-19 pandemic. The survey also found that while returning to school generally had a positive impact on wellbeing, this was also coupled with anxiety about Covid-19 related risks.[32]
The Scottish Children's Parliament survey of 8 - 14 year olds carried out in September 2020 found that respondents generally felt cheerful and in a good mood (64%); the largest increase in positive responses came from 12 to 14 year olds. There were significant improvements in children reporting that they often felt lonely (from 26% to 20%).[33] This was particularly so for the group of children who had reported highest levels of loneliness during lockdown 1, girls aged 12 to 14 (from 34% to 20%). Rates of worry across a range of topics including school work and 'the future' remained constant and worry about child and family health, money and exams increased post lockdown. Girls aged 12 to 14 were consistently most likely to agree that there were lots of things to worry about in their lives, whilst children aged 8 to 11 were more likely to report worrying about multiple areas than in previous surveys.
The second Covid-19 Early Years Resilience and Impact Survey of parents of 2 – 7 year olds carried out in November and December 2020 found that almost half (39%) of 2-3 year olds and over a third (31%) of 4-7 year olds had a slightly raised, high, or very high Strength and Difficulty Score, indicating the presence of behavioural or emotional difficulties. Just under half (46%) of parents said that their child's mood was the same as during the initial lockdown, just over a third (33%) felt that it had improved, while a firth (21%) felt that it had got worse. [34]