Miscarriage care in Scotland: delivery framework
The delivery framework for Miscarriage Care in Scotland outlines a plan for introducing a graded model of miscarriage care. The Framework sets out 34 actions to help NHS Boards prioritise change locally and move to a ‘One Scotland’ approach.
Accessing Early Pregnancy Care
Considerations
Care
Organisation and provision of miscarriage care should be by clinical nurse or midwifery specialists, and medical staff specifically trained in early pregnancy care, within self-contained early pregnancy units where possible. The model of care within rural and island services will be different but the care should always be patient-centred with support from a regional early pregnancy network. Formal training should be provided for sonographers, specialist nurses/midwives and clinicians responsible for early pregnancy ultrasound to ensure: individualised communication and care; diagnostic accuracy; robust reporting; inclusivity and cultural competency, and; consistent and accessible information provision for women/couples. Where possible, regional EPU/EPAS should arrange to share training opportunities with smaller NHS Boards and island units.
Referral
Referrals to early pregnancy services are made by self-referral, referral by health care professionals such as a GP, NHS 24, or Midwife; or via the Emergency Department. Self-referral to the nearest EPU/EPAS is the optimal pathway recommended in this framework; this reduces the burden on all other services, offers the best patient-centred referral pathway and ensures access to specialist advice.
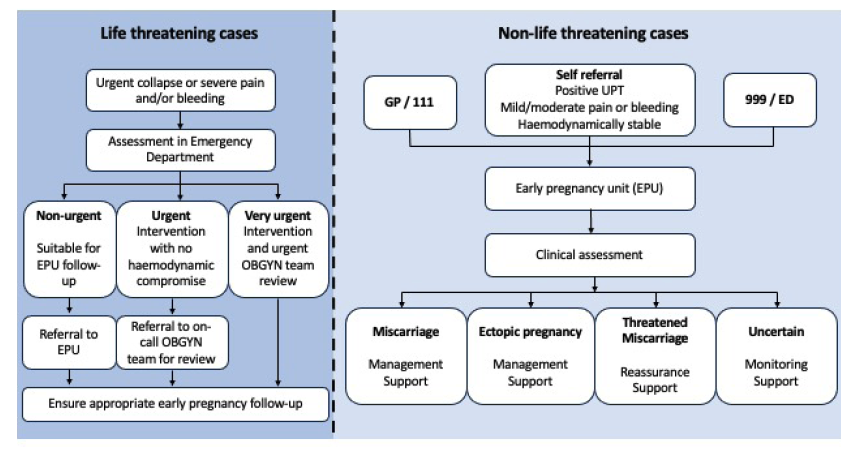
Emergency care
Emergency early pregnancy care should be delivered in line with the latest NICE guideline (NG126) (Figure 2). This framework recommends that a same-day emergency care plan is established with 111 and 999 services referring women directly to EPU/EPAS or local obstetrics and gynaecology department rather than to the ambulance and Emergency Department services. This means appropriate information must be available for 111 and 999 call handlers. A clear referral pathway should exist to the EPU/EPAS, in the local area that can provide a call-back service to women with early pregnancy complications, to arrange any appropriate further management and triage. NICE recommends that this should be within 24 hours.
If the EPU/EPAS is unavailable, and urgent care is required, treatment should be managed in the Emergency Department as a last resort. Where possible, women should be able to directly access out of hours care in specialist obstetrics and gynaecology departments and receive telephone advice and face-to-face review as necessary, instead of being referred to the Emergency Department. The exception to this is where a woman is haemodynamically unstable with severe abdominal pain, or major haemorrhage, where local policy may be to attend the Emergency Department directly in those circumstances. Triage within an obstetrics and gynaecology department for all other scenarios would be most appropriate.
Outside of normal working hours, regional teams and integrated care systems could combine to provide a cover service whereby women could access advice and care 24/7 without needing a referral from another healthcare provider. A directory of services that signposts women to the correct EPU/EPAS has been developed NHS inform - early pregnancy units.
Regional centres
Consideration should be given to the development of regional centres within NHS Board areas to ensure that out of hours provision of early pregnancy care can be established, and smaller units can refer patients and seek second opinions.
Separate spaces
All hospital settings treating those who are experiencing pregnancy complications should provide an appropriate separate private space for breaking bad or unexpected news and managing miscarriage care. All EPU/EPAS and out of hours services should ensure that there are cold storage facilities available to receive or store pregnancy remains. This might be for the investigation of recurrent miscarriage or to access sensitive disposal care pathways with staff trained in bereavement care.
The Scottish Government Programme for Government commitment is clear that NHS Boards should provide separate spaces for people who suffer a miscarriage (or other type of pregnancy and baby loss). This framework recommends that the most appropriate setting should be offered to assess and manage women with pain, bleeding or where risk of fetal loss and miscarriage is very high. This may be within a maternity triage setting where no other option exists, but boards should consider and explore the most appropriate, private and dignified space to assess and manage such women. Appropriate settings include early pregnancy units, bereavement suites or appropriate single-room facilities within obstetrics and gynaecology wards.
Bereavement care
Compassionate, culturally competent and high-quality sensitive care, bereavement care and trauma-informed care is fundamental. All staff involved with the care of women in early pregnancy should have bereavement care training specific to early pregnancy, in line with the National Bereavement Care Pathway NBCP Scotland (Annex C).
Key Actions
3. Ensure patients are made aware that clear, easily accessible and translatable information is available on NHS inform about managing concerns in early pregnancy which includes details on accessing care within each NHS Board. Provide patient leaflets for additional support I think I'm having a miscarriage: leaflet and After a miscarriage and Miscarriage: dads and partners.
4. NHS Boards to ensure that information about their early pregnancy service is up to date, effectively communicated, and easily available, to women, as highlighted in the Refreshed Framework for Maternity Services in Scotland (2011).
5. NHS Boards to ensure that those experiencing complications in early pregnancy are able to self-refer to their nearest Early Pregnancy Unit /Assessment Service (EPU/EPAS) within opening hours.
6. Women, who are clinically stable, with pain and/or bleeding and a positive pregnancy test who contact the Scottish Ambulance Service, 111, their GP or the Emergency Department should be directed to their nearest EPU/EPAS within opening hours.
7. Outside EPU/EPAS opening hours it is important that women have access to advice to prevent unnecessary attendance at the out of hours service or Emergency Department. Each NHS Board should ensure that women have access to someone who can speak to them over the telephone 24-hours-a-day, 7-days-a-week, including via an interpreter in their preferred language if required. Clinically stable women should be directed to the EPU/EPAS service when the service opens. In-person assessment should be available to those who require to be seen urgently because of clinical concern no matter what time of day or night.
8. Wherever possible NHS Boards to build access to a seven-day early pregnancy assessment service with a same-day approach. Women with pain or bleeding in early pregnancy should be able to speak to someone with expertise in early pregnancy every day and be triaged for in-person assessment in the EPU/EPAS as required. All patients should be managed through EPU/EPAS within 24 hours of initial presentation as per MBRRACE-UK 2024 recommendations. MBRRACE-UK Maternal MAIN Report 2024
9. NHS Boards that cannot provide a seven-day EPU/EPAS service within their Board should have agreements in place with neighbouring NHS Boards with clear lines of referral pathways. A networked approach within and between NHS Boards will ensure that patients and local non-specialist providers, including in primary care, are able to speak to someone with expertise in early pregnancy every day who can advise and arrange access to in-person assessment as required.