Trauma-informed practice: toolkit
This trauma-informed practice toolkit (2021) has now been replaced by the Roadmap for Creating Trauma-Informed and Responsive Change: Guidance for Organisations, Systems and Workforces in Scotland (2023), supported by the National Trauma Transformation Program
Key Principle 1: Safety
Efforts are made throughout the organisation to ensure that staff and the people they serve feel physically and psychologically safe. Staff and clients should experience the setting and the interpersonal interactions taking place within the setting as safe, inviting, and not a risk to their physical or psychological safety.
Physical Environment
All of the case studies demonstrated an understanding that safety was a priority for their clients. Each case study organisation had taken steps to ensure the physical environment promoted a sense of safety and protection, and created a welcoming and domestic atmosphere. Considerable effort had been made by staff to create waiting rooms and consulting rooms with a 'living room' ambience, where people could feel comfortable and at ease.
Opaque screening and sound proofing were used where possible, to reinforce a sense of privacy and confidentiality. Furnishings were chosen specifically for their non-institutional qualities, and attention was paid to detail such as the selection of neutral pictures for the walls, ambient music instead of a radio playing, and the availability of reading materials that were non-triggering. In police stations, a living room style was created in interview rooms for victims and/or vulnerable people to try to promote a sense of safety.

A waiting room (Mental Health), a treatment room (Addictions) and a nurture room (Education).
Toolkit
? How does the physical environment promote a sense of safety, calming and de-escalation for clients and staff?
? In what ways do staff members recognise and address aspects of the physical environment that may be retraumatising, and work with either a) improving the environment and/or b) with people on developing strategies to deal with this?
? How do the organisation's written policies and procedures include a focus on trauma and issues of safety and confidentiality?
? How has the organisation provided space/opportunities that both staff and people receiving services can use to practise self-care?
In some cases, areas were zoned to maximise a feeling of protection. In the waiting room of one service, this was created using seating clusters and high-backed curved-carcass chairs. In one case study area, this was created using panel boards. In the context of residential care, the needs of children and young people were addressed through the creation of calm areas or communal zones. In most cases, lighting was usually intentionally kept subdued and colour schemes neutral to avoid overstimulation.

A classroom using "zoning"
Toolkit
? How is a gender differential taken into account in site selection (if possible) and recruitment?
? How has the organisation developed mechanisms to address gender-related physical and emotional safety concerns (e.g. gender specific spaces, gender specific activities)?
? How will a Service Walkthrough be completed, and how will the findings from this be built into the plan to help the service become trauma responsive?
Interviewees described conducting a 'trauma-informed walk through' of their respective premises to inform the establishment of a physically and emotionally safe environment for service users and staff.
"…a really simple example is we did a walk round and thought, what is potentially scary here? And an example were there was a smashed window that nobody had noticed for like six months, just a tiny one. There was burglar-proofing, like barbed wire stuff on a drainpipe. Loads of things like that, and it was like, why are these still here? It was just asking that question and we made some good changes to that." (Residential care).
Several case study areas described the importance of taking into account gender differentials when choosing a site, ensuring there are waiting rooms with enough space to provide distance when needed, especially for people who have experienced gender-based violence.
"For these kids, it was about having different areas for different moods or needs, if you like. So, a play area, a calm area, a communal area, lots of outside area." Residential setting.
"It's a female only, and I know that sounds horrible, but we're not men haters or that, but it's just easier, like to sit and like talk and that, if that makes sense…. Just because a lot of women have been hurt or been in like domestic abuse relationships and that, so it's not really good or handy like to have a man around, much better and easier for women to open up to women." (CJSW)
The premises of some case studies had kitchen areas connected to the reception, adding to an atmosphere of domesticity, where people were encouraged to prepare their own tea or coffee on arrival. Alternatively, welcoming reception staff offered drinks to visitors, or a water cooler was available.
"They also offered to make you a cup of coffee and all that... I thought that was... That's a nice touch, you know what I mean? That is a nice thing… because that makes you feel like a human." (Addictions)
The importance of the environment was highlighted by interviewees with lived experience.
"It just makes you feel like you're not in a threatening place, and for me anyway, somewhere…clinical places can often be a bit, because they remind you of police cells or police stations or hospitals or, for me, care, like secure units." (Police)
Interviewees regularly highlighted that staff working with trauma survivors should be empathetic, compassionate,
non-judgemental and have good listening skills. In every case study area, these qualities and skills were clearly prioritised, and were reflected by recruitment processes in the form of person specifications and job descriptions. In one case study area, the reception staff were mentioned in every interview as being central to the creation of an emotionally safe environment for both staff and service users.
"…you come in, and [receptionist], she's amazing, she's like the most friendliest like receptionist I've ever known in my life, and she just makes you so welcome, and like do you want a cup of tea, coffee, so then you'll sign in and you'll say who you're here to see. And then you might sit in the like…the sitting area with [receptionist]." (Criminal Justice Social Work)
It was also acknowledged that a balance had to be struck between attempts to create an atmosphere of domesticity and the need for appropriate security measures, such as door buzzers and secure entry systems, to help service users and staff feel safe.

Toolkit
? How has the organisation specifically recruited for individuals who have the skills and qualities necessary to be trauma-informed, e.g. empathetic, welcoming and caring?
Hiring a Trauma-Informed Workforce
Getting Lived Experience on Board
? How will the organisation ensure all workers respond to survivors in a way which is emotionally safe? For example, providing training to staff at all levels.
? How does the organisation ensure that all staff (direct care, supervisors, front desk, etc) receive basic training on trauma, its impact, and strategies for trauma-informed approaches across the agency and across personnel functions?
Screening, assessment and treatment services
Trauma screening has been described in the literature as: "a brief, focused inquiry to determine whether an individual has experienced specific traumatic events" (Harris & Fallot, 2001).
In most case study areas, universal trauma screening was not considered appropriate for the organisation. In these sectors, creating the milieu which made people feel at ease to maximise disclosure, and directly asking the person if they had experienced a traumatic event were deemed more appropriate.
Universal screening for trauma was adopted in three case study areas, using psychometric tools such as the International Trauma Questionnaire (ITQ), ACEs and BCEs. Most services also screened for socio-demographic factors, employment status and life skills.
One case study area described working alongside healthcare services to develop their own tailored screening tool called the Trauma and Mental Health Screener (TAMHS). Staff received specific training in how to use this, as well as additional mental health training which was particularly important to their sector.
"one section of the TAMHS is a kind of summary / formulation of the findings, and that summary / formulation often goes into the report ... with quite a strong caveat that this…so it's a screening tool, rather than a thorough mental health assessment or trauma and mental health assessment." (Criminal Justice Social Work)
In most of the other case study areas, staff would screen for trauma histories at the assessment stage, or when they felt it was appropriate.
"the first time you meet somebody, that rapport isn't there, they maybe don't feel safe coming to a service. And then if you're asking these questions on a questionnaire, that really, it could put the fear into them, and you might never see them again. So it was very much, gauging when the right time is to do that." (Addictions)
Toolkit
? Is timely trauma-informed screening and assessment suitable for your service? If so, is it available and accessible to individuals receiving services?
? How does the organisation address gender-based needs in the context of trauma screening, assessment, and treatment? Do they offer gender specific services? Can they refer to someone who does?
? If suitable, how do staff still ask the difficult questions which need to be asked to identify trauma and how are they supported to do this? How confident are they in doing this? So they need further training?
Asking about trauma
? Is there an organisational policy on how screening should be completed and/or how service users should be asked about trauma? Should there be?
Training
Staff Wellbeing
Trauma-specific models and therapeutic modalities
There should be an agreed format to follow (an agreed screener/questionnaires for the team to use, as well as a clear format for assessment). Trauma training provided to staff should include an element focusing on these issues as workers responses are important when a disclosure is made, as they can reduce the risk of traumatisation or retraumatisation.
Most of the case study areas used an appropriate model to underpin their service delivery, as this was deemed important for the congruence of practice. The most commonly used trauma-informed models were based on the work of Harris & Fallot or SAMHSA. Two case study areas had adapted existing models to meet their own requirements.
Trauma-specific models included Judith Herman's phased-based trauma model and the Seeking Safety model developed by Lisa Najavits (2002).
Case study organisations that were involved in the delivery of treatment services confirmed that their clinicians and practitioners were trained in the use of evidence-based interventions and adhered to the recommendations of treatment guidelines and guidance documents, such as the NICE guidelines for PTSD or the Matrix.
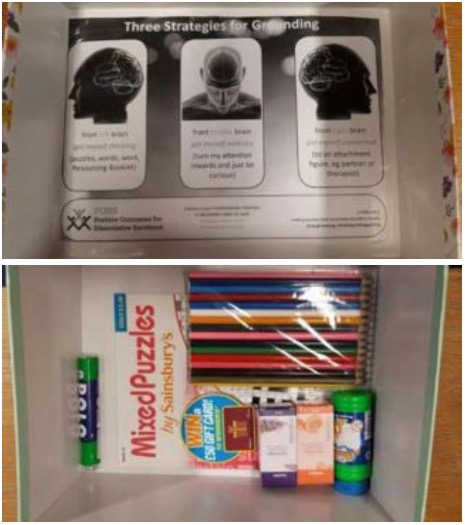
Staff commonly described the importance of having tools they could use to help stabilise their clients. Interviewees emphasised the need for staff to be trained in the delivery of safety and stabilisation interventions in particular, given the role of these self-management skills in increasing a sense of emotional safety for clients. Highlighted interventions included grounding techniques, breathing exercises and mindfulness.
"The big difference for me out of the whole thing was given the practical tools because that's stuff that you could take with you for the rest of your life, you know. I've never had that kind of help before." (Addictions)
Toolkit
? What is the specific model underpinning the organisation's trauma-informed work? Their trauma-specific work?
? Does the organisation have the capacity to provide trauma treatment or refer to appropriate trauma treatment services? Is there a wait for these? If so, is there an alternative way of providing this service?
Trauma-specific models and therapeutic modalities
? Do staff members talk with people about the range of trauma reactions and work to minimise feelings of fear or shame and to increase self-understanding? Can/should they be completing safety and stabilisation work with the client?
Background materials for explaining effects of trauma
Advice on how to use trauma-sensitive language
? How are these trauma-specific practices incorporated into the organisation's ongoing operations?
In one case study area, a specific safety and stabilisation training programme was routinely provided to a sub-group of clinical staff.
The training introduced staff to the concept of the 'window of tolerance' and referred to various methods of emotion regulation. The programme was being evaluated with a view to rolling it out to other staff groups. Another case study area provided 'calming boxes' to trauma survivors. Others offered 'fidget' objects that supported the safety and stabilisation work delivered in the course of psychological treatment.
To support staff in the delivery of such interventions, interviewees highlighted the importance of self-care, supervision and opportunities for reflection.
"About self-care, so when you first come to [name of service], everybody has a self-care plan which…it's mandatory to kind of create in a collaborative way." (CJSW)
"we have group supervision weekly, a reflection space where we can bring difficult exchanges…it's about kind of the emotional impact of the work." (CJSW)

Toolkit
? How does ongoing workforce development/staff training provide staff supports in developing the knowledge and skills to work sensitively and effectively with trauma survivors?
? What types of training and resources are provided to staff and supervisors on incorporating supervision in their work?
? Would creating a specific policy in accessing supervision in your service create more service congruency?
? Are staff given the opportunities to come together and reflect?
In a police setting, the inherent stigma which can be attached to selfcare was raised as a barrier, although it was recognised this has changed in recent years and the mental health and safety of officers and staff is now better recognised. There is now a range of tools and networks to support wellbeing and resilience (including Lifelines Scotland).
Training and workforce development
Some staff talked about an inherent tension between the trauma-informed principle of safety and practices that related to the core function of their organisations. Some practices, staff suggested, would inevitably compromise a trauma survivor's sense of safety and would potentially cause retraumatisation. For example, being held in police custody, receiving a custodial sentence, being detained under the Mental Health Act, or having children removed by Children and Families Social Work, were all seen as potentially re-traumatising processes.
In these circumstances, it was suggested that an awareness of a client's trauma history and the diverse ways that traumatic experience can manifest itself can help staff to reframe complex behaviours as a response to relational triggers. Hostility, manipulative behaviour, lack of motivation, or resistance to services can be reframed as survival mechanisms that are triggered in the face of perceived threat. Through the consistent communication of empathy, warmth, respect and hope, staff maintained that they could provide powerful corrective relational experiences, challenging a client's working models of self and others, and enabling them to update these models in the context of new relational experiences.
"The more cynical officers are the ones that have been exposed to more things, you know, or potentially been really assaulted or had really traumatic experiences at the hands of certain people and we're trying to change their viewpoint a bit in how we can help these people not behave the way they've behaved to them before." (Police)
"Understanding distressing behaviour amongst pupils means a calmer school. More compassionate staff. Better behaved children. More emotionally stable children." (Education)
"…we would be really breaking down barriers of perceptions that police officers already had, you know, just a kind of good/bad thing – people are bad, they're on drugs, if they do this then that's it, they're going to be that way – then fine, we'll just lock them up." (Police)
Toolkit
? How do the organisations written policies and procedures recognise the pervasiveness of trauma in the lives of people (using the services and working in them), and express a commitment to reducing retraumatisation and promoting well-being and recovery?
? How does workforce development/staff training address the ways identity, culture, community, and oppressions can affect a person's experience of trauma, access to supports and resources and opportunities for safety?
Background materials for explaining effects of trauma
? How do the organisation's written policies and procedures recognise the pervasiveness of trauma in the lives of people (using the services and working in them), and express a commitment to reducing retraumatisation and promoting well-being and recovery?
? How do the organisation's staffing policies demonstrate a commitment to staff training on providing services and support that are culturally relevant and trauma-informed?
Pressures on staff time were also highlighted as a potential barrier which could get in the way of a welcoming or engaging approach. However, staff acknowledged that training and the experience of delivering trauma-informed practice would highlight the importance of these methods of informal engagement.
"So if a person's waiting outside and I'm coming in, I'll always say, hello, how are you, …so I understand the reasons why sometimes professionals will ignore patients, it is because they don't want to be asked something. They don't want to be interrupted as they're on the move from…and…yeah. And…very occasionally that then does happen. But I think that's okay 'cause that balances out all other many, many times when people are just pleased that person's saying hello to them." (GP).
Trauma training was considered to be a key method of facilitating a raised awareness in this respect and interviewees consistently commented that one outcome of such training was an increased empathy towards clients. It was also reported that training helped staff understand the importance of providing a safe and nurturing environment for the growth and healing of trauma survivors.
"I think one of the key benefits is about creating more empathy within staff. For some reason it just really hits a note with people…it seems like quite a powerful way to help staff make sense of people's presentation." (Mental Health)
"I mean, I think all healthcare professionals should have it, from… if anything just from a professional wellbeing point of view, it means if you understand why some of those difficult consultations that don't seem to make sense happen…if you're able to understand what that is, then that reduces burnout, increases professional wellbeing, all of those things." (GP)
The importance of staff wellbeing was emphasised by interviewees from each case study area, along with the need to incorporate trauma-informed staff wellbeing policies throughout the organisation's human resource systems. Staff identified the need for training in secondary traumatic stress and vicarious traumatisation, and called for procedures to be put in place to support staff who had their own trauma histories or who may have been affected by working with trauma survivors.
Toolkit
? How does on-going workforce development/staff training provide staff supports in developing the knowledge and skills to work sensitively and effectively with trauma survivors?
Hiring a Trauma-Informed Workforce
? How does the organisation help staff deal with the emotional stress that can arise when working with individuals who have had traumatic experiences?
? How is the emotional safety of staff considered by the organisation? Promoting self care, ensuring staff are adequately supported, staff are involved in feeding into the organisation how this should happen?
Progress monitoring and quality assurance
Mechanisms to monitor trauma-informed principles
Toolkit
Progress monitoring and quality assurance
? How does the organisation conduct a trauma-informed organisational assessment or have measures or indicators that show their level of trauma-informed approach?
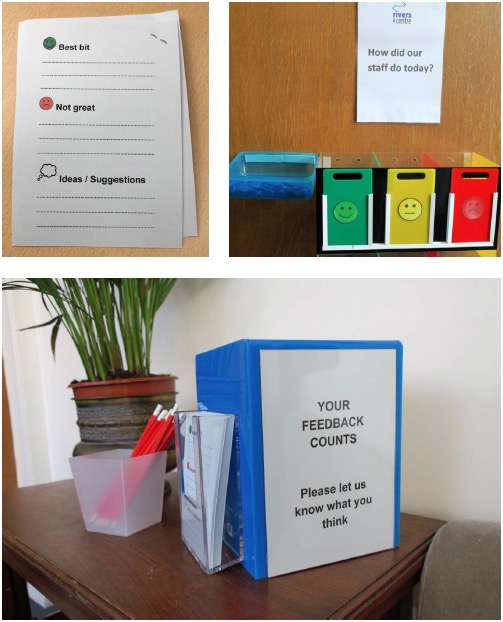
? How does the perspective of people who have experienced trauma inform the agency performance beyond using a service user survey?
Getting Lived Experience on Board
? What processes are in place to gather feedback from people who use services and ensure anonymity and confidentiality?
? What measures or indicators are used to assess the organisation's progress in becoming trauma-informed?
All case study areas were collecting some form of data from service users and staff on the implementation of trauma-informed practice (Appendix 7) shows which elements of trauma-informed practice were being evaluated, how the data were collected, which measurements were used and how findings were reported. Other case study areas assessed, tracked, or monitored trauma-informed principles by gathering data specifically relating to trauma training, most often using pre- and post-measures.
Key barriers to the effective assessment and monitoring of trauma-informed principles included the complexity of evaluation systems, a lack of analysis frameworks, and restrictions on time and resources (Purtle, 2018).
Financing
Interviewees emphasised that many changes can be done with minimal cost, and even small changes can make a big difference to trauma survivors. In many of the case study areas, changes to the physical environment had been made as a result of donations from staff, service users or the wider community.
Staff highlighted the need to conduct robust evaluations of any changes, using direct feedback from service users to build a case for additional funding. In this respect applications to local sources of funding, such as health foundations or small grant awarding bodies can be particularly fruitful. Several of the case study services had also secured funding for their work from Scottish Government innovation grants or funds aimed at reducing the poverty gap.
There was widespread acknowledgement that large-scale measures that might greatly improve the physical and emotional safety of staff and clients, such as the relocation of service premises or the upgrading of furnishings and facilities, are usually not possible without additional sources of funding. However, Domino et al. (2005) highlighted they found trauma-informed, integrated services to be cost-effective, improving outcomes but not costing more than 'standard programming".
Toolkit
? How does the budget support provision of a safe physical environment?
? How does the organisation's budget include funding support for ongoing training on trauma and trauma-informed approaches for leadership and staff development?
? What funding exists for cross sector training on trauma and trauma-informed approaches?
? What funding exists for peer specialists?
? What mechanisms are in place for information collected to be incorporated into service delivery?
Evaluation
Problems with the evaluation of trauma-informed practice have been identified in the literature: "…an amorphous concept that has been defined in a number of ways, making it difficult to evaluate initiatives" (Hanson & Lang, 2014). There was evidence that several of the case study organisations were using appropriate trauma-oriented research instruments to evaluate the effectiveness of their services.
Only three case study areas were conducting evaluations involving a control group or theory of change model. The evaluative approaches used in each case study area are shown in Appendix 7.
Toolkit
? Does the organisation gather feedback from both staff and individuals receiving services?
Getting Lived Experience on Board
? What strategies and processes does the organisation use to evaluate whether staff members feel safe and valued at the organisation?
? How does the organisation include cultural factors in monitoring and quality assurance?
? What mechanisms are in place for information collected to be incorporated into the organisation's quality assurance processes and how well do those mechanisms address creating accessible, culturally relevant, trauma-informed services and supports?
Contact
Email: sharon.glen@gov.scot