Trauma-informed practice: toolkit
This trauma-informed practice toolkit (2021) has now been replaced by the Roadmap for Creating Trauma-Informed and Responsive Change: Guidance for Organisations, Systems and Workforces in Scotland (2023), supported by the National Trauma Transformation Program
Key Principle 5: Empowerment
Efforts are made by the organisation to share power and to give clients and staff a strong voice in decision-making, at both individual and organisational levels. Each level of the organisation, including management, operations, service delivery and staff training, is designed to be empowering for both staff and service users. Staff are empowered by mechanisms of organisational support, and clients are empowered by services that are person-centred, and based on belief in the resilience of individuals and their ability to heal and recover from trauma.
Toolkit
? How does organisation leadership communicate its support for implementing a trauma-informed approach?
? What is the plan for training provision in TIP to be provided to senior management? This should include examples on how to be a trauma-informed leader – including role modelling.
Using Trauma sensitive language
? How do the organisation's mission statement and/or written policies and procedures include a commitment to providing trauma-informed services and supports?
Governance and Leadership
Two key themes emerged from the interviews: the importance of senior management support; and having trauma-informed leaders who could model trauma-informed behaviour and language, and ensure successful implementation.
Case study services referred to the importance of establishing an implementation group and/or identifying a trauma champion within the organisation. Where there was regular movement within an organisation of staff members from one post to another, interviewees said that they had found it helpful to identify several trauma champions to ensure sustainability of the role.
A common barrier in terms of implementing plans for trauma-informed practice was the trauma champion's lack of seniority within the organisation. One case study service found that it had been useful for their trauma champion to be given a seat at senior management meetings, as they had been able to provide regular updates in the form of a standing item on the agenda. Another case study service confirmed the importance of feeding into a high level strategic management group.
"I needed them to want to become trauma-informed leaders in order to take it forward, which translated into practices which would turn into improved outcomes for service users." (CJSW)
"I think it's really important that we look at the way that services are designed to enable staff to be trauma-informed. You need time and space around you, your caseload can't be too big. Again, some of the things that we see are caseloads creeping up in all sorts of different services. I suppose it's then buying into all of the principles to embed into their own organisation." (Police)
"..And we created this role, but we still don't have the best name for it, but it's been called Model Holder…[someone] who understands and has got all the knowledge and skills anyway, that they can help and act as an implementation driver, if you like, and ensures that every bit that we try to operationalise is actually happening." (Residential)
Implementation groups and trauma champions often took the lead in conducting a preliminary assessment of their organisation's current trauma-informed practice. One case study service found it useful to conduct this assessment as a team exercise, adapting the forms in the toolkit to the needs of their own organisation.
Case study services also described the importance of supporting and taking part in a "Trauma-informed Lens" workshop or a trauma-informed service "walkthrough". Interviewees described the need for staff and clients to come together to look at how the service is designed, and to place the service in the context of the wider system. They also highlighted the need to make a clear plan to take trauma-informed practice forward, identifying "SMARTER" objectives and clear lines of accountability based on the results of the preliminary assessment and service walkthrough. It was emphasised that implementation groups should meet regularly to review this process and should feed any updates into senior leadership groups.
A manager from one of the case study services recognised that management support needed to be highly visible in order to drive the agenda forward. In most cases, staff described making presentations to senior managers and leaders, in which they would define the concept of trauma-informed practice and link it to tangible outcomes.
Toolkit
? What preliminary assessment of the organisation's current TIP is taking place? Are toolkits being used? Who is accountable for this?
Other toolkits for Organisational change
? How will a Service Walkthrough be completed, and how will the findings from this be built into the plan to help the service become trauma responsive?
? How does organisation leadership communicate its support for implementing a trauma-informed approach?
Other toolkits for organisational change
"I started to ask them to do an assessment of their team and their service…I asked them to fill out forms – a group exercise…..I adapted the forms for X in Scotland from the Homelessness Toolkit. Very, very detailed stuff about what do you do when a client walks through the door? What is your signage like?" (CJSW)
"When the new building opened the Justice Secretary came to come and cut our ribbon for us, the Chief Social Work Officer from Edinburgh City Council and the NHS….so senior figures in council and NHS – part of that was saying… look what we can bring you with trauma-informed care …the service users were there. I wanted them to hear from service users. I have been through a million services and this is the only one which has really helped me." (CJSW)
Clients were often involved in these events and the voice of service users was seen to have a particularly powerful impact. In several of the case studies, the people leading the drive towards trauma-informed practice were staff working directly with service users, some of whom had lengthy experience of working in their field, coupled with a good understanding of the ways in which trauma-informed practice could improve their services.
Staff talked about the importance of finding 'like-minded' individuals within their organisation and the need to gain 'buy-in' from these individuals. This was commonly done on an informal basis. Several case study services held "kick off" events, which they found were a useful way of meeting like-minded individuals and facilitating wider system change.
Leadership also played an important role in empowering staff to look after themselves, especially in the modelling of self-care, for example by attendance at reflective practice sessions or group supervision. Staff clearly valued attempts by their organisation to actively monitor their wellbeing or to prioritise supervision or reflective practice, and they described a sense of empowerment created by leaders who collaborated closely with staff to produce collective problem-solving.
"…[it's] borne out of 30 years of frustration of seeing things not change." (Addictions)
"… it was all very much bringing together people who had shared interest in this and trying to coordinate efforts….." (CJSW)
"…with each individual house, there were lots of staff development days, there were lots of buy-in days, there was, let's all get behind this. We brought in ex-care experienced young people and other people to all try and get this momentum. We did plenty of presentations, lots of training. Yeah, loads of stuff actually." (Residential)
"Well, we had an event… a town hall event two years ago…or almost two years ago now, which we pulled together about 120 people into the town hall. That followed up a previous trauma-informed event the year before…we had one which was much more around, let's share the trauma-informedmessage right across a community, let's try and get buy-in for the trauma-informed thinking, as it were, right across community planning...Then we agreed that at that point there needs to be a leadershipcommitment. So from the first conferencewe had a paper going to the [x], which was the top level of decision making was well-recognised by interviewees, progress in this area had been problematic across most of the case study services." (Local Authority/ Police)
Toolkit
Setting up a Trauma-Informed event
? Does your organisation have a survivor involvement policy, outlining your mission and what you want to achieve by involving survivors? Have staff been involved in discussions on how this will work/barriers to implementation?
Getting Lived Experience on Board
One organisation described the establishment of a service user reference group as a key part of its governance structure, however the reference group had been discontinued due to the organisation's inability to secure sustainable funding. Three other case study organisations described different ways that they had established service user involvement. These had initially been set up through informal discussions with service users who had completed their own journey through the service and had expressed an interest in continued involvement. Their motivation was usually described as a wish to help others and a desire to feel part of the service community.
Staff reported a number of barriers relating to the inclusion of the service user voice. These included perceived and actual difficulties in finding "suitable" trauma survivors; the lack of financial remuneration; access issues relating to disability; and mental health related problems such as anxiety, social isolation, lack of confidence and low self-esteem. "Red tape" was identified as another factor that impeded attempts to integrate service user groups into governance structures. Some interviewees also suggested that professionals generally occupy the expert role and that they might feel uncomfortable sharing this role with service users in the context of service governance.
One case study service partnered with a group of people with lived experience and felt that this had been pivotal in gaining the level of lived experience necessary for taking forward this agenda. Paid lived experience representatives had been involved in service planning, training and service delivery. This was the only case study service that had people with lived experience who were paid and were embedded in the team, delivering support to people affected by gender-based violence.
"I think the biggest barrier is that that part of the work is never resourced properly. People think, oh we can get that for free, and in reality, what then happens is, because they're not paying for it, they don't value it." (Police)
"This was one of the first principles we were defining with [X], is that people with lived experience deserve to get paid for their contributions as experts of lived experience, because they have something more valuable to offer than anybody else does in a lot of respects." (Police)

Lived experience representatives from Resilience Learning Partnership
"…start by looking at where there's good engagement. In [X] we have a mental health user group. We've got an active recovery community for substance misuse. We've got [Lived Experience expert group]. … I think the more of these groups that you have, the better, by and large...I think it's that whole process of ensuring that individuals are empowered at every stage of the process. The danger is sometimes I think that professionals start to pay lip service to it or they sometimes look at it as a tick-box thing rather than something that they really need to embed in absolutely everything that they do." (Police)
Toolkit
? How can staff and clients be involved with developing a plan for improving engagement and involvement of survivors in service planning and delivery? Has budget been considered to support this?
? What can be done to improve trust and transparency in staff, for survivors who do become involved in service planning and delivery? How has their role been collaboratively identified and clearly outlined to avoid any confusion?
Getting Lived Experience on Board
Policy
As a matter of policy, one case study service routinely involved service users in the recruitment of staff. Staff described the process by which service users would meet candidates prior to the interview and would then represent service users' voices by being a member of the interview panel.
Toolkit
Hiring a Trauma-Informed Workforce
? What strategies are used to reduce the power differentials among staff and clients?
Getting Live Experience on board
Staff from another organisation described how they changed their main method of written communication with the aim of empowering their clients. In place of traditional letters to the professional who had made the referral, staff addressed their letters directly to the client and wrote in a jargon-free, accessible format. In a collaborative process, prior consent was sought from the client to copy the correspondence to any professionals involved in their care. Clients were also asked to identify material that they wished to keep confidential and this was omitted from the correspondence. Clients were then encouraged to check the content of correspondence to ensure that the information and decisions reached were accurately represented. Based on client feedback, any misunderstandings were corrected in the formal medical record.
Dear [first name of client]
Thank you for coming to [name of service] on 26th August 2019.
As promised, I'm writing with a brief summary of our discussion.
You said that a few things have happened recently that have brought back memories from your childhood and you're finding it hard to deal with this. You told me that ... All of these things have made life very difficult for you at the moment.
In terms of a plan, we agreed the following next steps:
- I am registering you with...
- I will ask [name of link worker] to help you engage with...
- I plan to stay in the picture and will arrange to meet up with you again in two months time to see where things are up to for you. We can discuss further options at that point if appropriate.
In the meantime I hope that our meeting was helpful and I'll keep in touch with [name of link worker] to hear how you're getting on.
With best wishes [Name of staff member]
Engagement and involvement
One organisation described their use of focus groups, satisfaction questionnaires, feedback boxes and a "happy-or-not" system to create a direct and ongoing dialogue between the organisation and its service users.
Other case study areas described efforts to engage clients by building a sense of community. They invited service users to contribute to the physical environment, decorating community areas using photos, artwork made by service users, or potted plants.
Toolkit
Getting Lived Experience on Board
Specific challenges were described with regard to the empowerment of children and young people, particularly in the context of educational or residential settings. In some cases, however, staff described a shift in focus towards ensuring that children have hope in their future.
"We are continually evolving how the Nurture Room works by engaging the children. Maybe they want some different role play costumes or want to make a specific good. So they are involved to some extent." (Teacher)

"How did our staff do today?"
"we get women's stories, we get their versions of what their experience of our service has been, and then we try to use that to kind of create a kind of service improvement plan." (CJSW)

Patchwork of empowerment by service users (CJSW)
Service user artwork (Addictions)
"I think it makes it easier for them to like kind of build a relationship with me, if that makes sense, because like, well, she's been in and done it, and she's managed to change, so there's hope for me." (CJSW)
A key part of engagement was the development of peer support groups and/or peer buddying. These were particularly important groups in terms of helping people to normalise their reactions, and empowering people to build corrective relationships.
"I suppose it was a really good way of having a transition out of one-to-one and still have an environment to talk about…how you're doing and different people have lots of different ideas and we'd chat." (Addictions)
"…every Wednesday 12 o'clock, this is my time. And I look forward to it because I can go for days…days and don't speak to anyone." (Addictions)
One peer support forum had developed into a group that campaigned to change the criminal justice system by sharing lived experience with professionals and strategists. This group had been successful in applying for additional funding for group advocacy activities.
"...the thing is, it's like people want to hear our stories, they don't want to like push us away and that any longer, and I think it's important that people hear like with help and that and support, you can change your life" (CJSW)

Cross sector collaboration
To find 'like-minded' people who would collaborate on leading the development of trauma-informed practice, some case study services looked outside of their own organisation and approached professional colleagues in other sectors. Interviewees described various methods of facilitating this process, including the setting up of workshops, conferences and events where people across sectors could meet up. Delegates typically included representatives from healthcare, social work, police, education and third sector organisations.
"…we had a couple of those meetings, and it took a little while for everybody to kind of work out what we were doing, but then we started getting into, what are we doing, what do we all do, what's different, where are the gaps." (Mental Health)
Photographic work by service users (CJSW)
One case study service worked in collaboration with a range of cross sector organisations to enable service users to create images that explored their identity. Photos were taken of objects with a personal value to the client and these became emblems of self and belonging.
Another case study service employed link workers as core members of the staff team. The link workers focused on social connection, enabling clients to engage with community resources that would further their recovery, including access to education facilities and employment schemes, leisure and recreational activities.
Screening, assessment and treatment services
Staff in the case study areas described themselves as being "facilitators" rather than "controllers" of recovery. They viewed their clients as experts by experience and emphasised the importance of supporting trauma survivors to cultivate self-advocacy skills. This positioning of service users in the expert role was acknowledged by survivors.
Working collaboratively in a person-centred way was common to all of the case studies. A strengths-based approach was used by most services, with staff and clients highlighting the importance of safety and stabilisation skills due to the ability of these practical tools to empower clients.
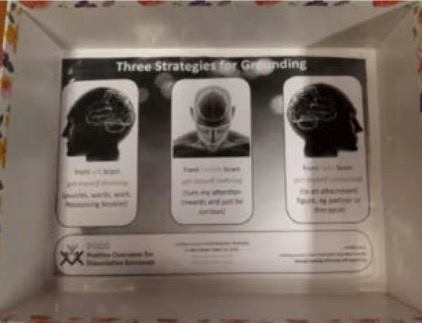
Self-soothing box used for safety and stabilisation
"It's so important, because we didn't want a fixer. How are we going to learn from our mistakes and how are we going to get on with life? We need to figure things out for ourselves. It's alright to ask for help and that, but people can't make the decisions for you, you're the only one that can make the decisions." (CJSW)
"The big difference for me out of the whole thing was [being] given the practical tools because that's stuff that you could take with you for the rest of your life, you know. I've never had that kind of help before." (Addictions)
Training and workforce development
The degree to which staff feel that they have a sense of agency, control and preparedness in performing their roles is key to their perception of empowerment. Interviewees emphasised the need for training to be readily available to staff, enabling them to update their knowledge and skills, particularly with regard to trauma and its impact. The need for training in a range of psycho-education and self help resources was identified, including information on normal reactions to trauma, resilience, and the importance of self-care. Strategies emphasising the role of social connection, routine, exercise, relaxation and good sleep were commonly mentioned. One case study area involved lived experience in their training and workforce development sessions.
Most case study organisations described clear channels for regular communication, such as daily huddles, weekly team meetings or operational debriefs, providing opportunities for staff to voice their opinions and have open and honest discussions.
Staff also described input and feedback mechanisms such as listening groups, email suggestion boxes or visits to services by leaders. Some organisations had processes that clearly demonstrated the ways that working practices had been changed in direct response to staff input and feedback.
Toolkit
Getting lived experience on board
? How do staff members help people to identify strategies to feeling comforted and empowered?
Contact
Email: sharon.glen@gov.scot