Coronavirus (COVID-19) targeted community testing: national evaluation evidence and insights - final report
This report summarises evidence and insights at a national level from evaluation of targeted community testing (TCT). The report covers the period 18 January 2021 to 26 September 2021.
4. Models of delivery and lessons learned
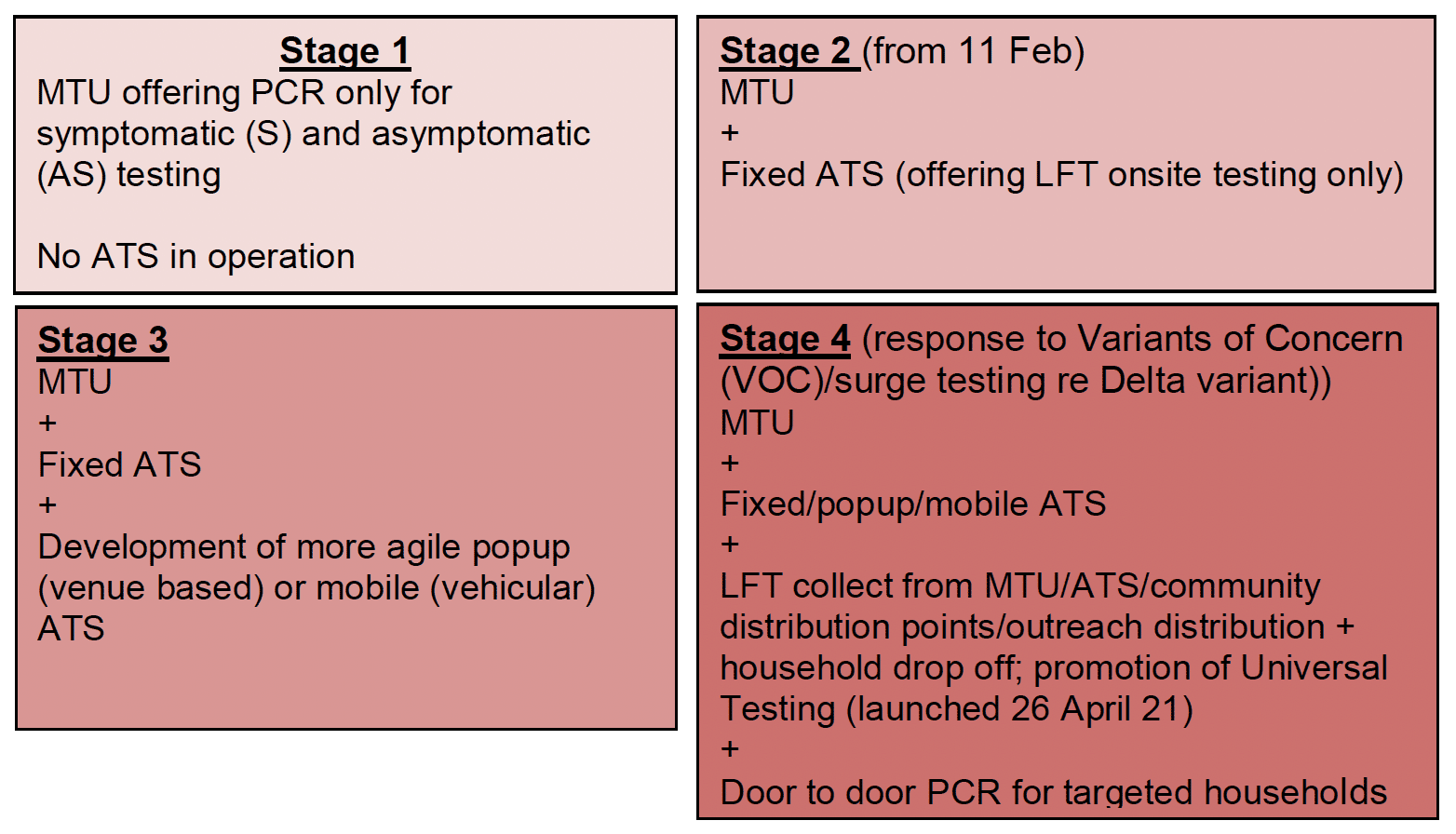
Four evolutions of targeted community testing models have been apparent between 18 January and the end of May 2021, an overview of which is set out in Figure 5 below. Precise dates are not applicable as changes were occurring at different times in different areas. This may not capture all models in operation to the end of May 2021 due to the fast pace of change. Also, it is worth remembering that models have continued to evolve since this point in time.
In addition, home PCR tests kits have been used throughout by some areas, either drop off or posted or given out at sites for those presenting with symptoms or for confirmatory PCR for those testing positive. This is not included in descriptions.
Graphic text below:
Stage 1
MTU offering PCR only for symptomatic (S) and asymptomatic (AS) testing
No ATS in operation
Stage 2 (from 11 Feb)
MTU
+
Fixed ATS (offering LFT onsite testing only)
Stage 3
MTU
+
Fixed ATS
+
Development of more agile popup (venue based) or mobile (vehicular) ATS
Stage 4 (response to Variants of Concern (VOC)/surge testing re Delta variant)) MTU
+
Fixed/popup/mobile ATS
+
LFT collect from MTU/ATS/community distribution points/outreach distribution + household drop off; promotion of Universal Testing (launched 26 April 21)
+
Door to door PCR for targeted households
Models
Each partnership, and even different local authorities within partnerships, developed their own approaches to suit the population, geography and resources of their local area, as well as adapting to what was happening with the pandemic and restrictions more broadly. Some partnerships were more advanced with their proposals than others at the time of this research. Hence, it is challenging to provide a comprehensive picture of the models in place at this time. Instead, three types of models are described in broad terms offering some insights into the setup of TCT at this time.
The hub and spoke model
This was an approach taken by a number of the local areas within and across partnerships. It comprised of a blend of fixed sites with popup and/or mobile options.
The fixed sites tended to be set up and serve more populated areas to ensure good footfall. They were perceived to create a presence, helping to advertise regular community testing, whilst the popup/mobile assets enabled a flexible and adaptable response for rapid deployment to where they were most needed.
The mobile option was seen as addressing issues around a lack of a suitable/available site or venue at locations suggested by data. In addition, the time it takes to set up an ATS not always being responsive enough such that case rates may have declined at that location whilst spiking elsewhere in the intervening period.
Fixed sites using Fire and Rescue Stations
One partnership developed a model which operated from fixed Fire and Rescue station locations. When prevalence was low, testing operated from the sites on a fixed timetable, but with the capability to alter the timetable to target specific stations in high risk areas as data dictated.
The rationale behind this model was to provide broad geographic coverage for a relatively dispersed population in sites that are typically within walking distance. This model was perceived to be effective at targeting those in areas of deprivation, as this is often where Fire and Rescue stations are situated.
Flying Squad – LFT outbreak response
The final model is one described by the local area as the 'Flying Squad'. This involved the rapid deployment of a popup LFT site to a specific place or organisation with an outbreak. It offers LFT tests to non-symptomatic and non-contacts as an adjunct to MTU-based outbreak PCR testing to provide rapid detection of additional cases that may be asymptomatic.
In the case study described, people in the target population were encouraged to test 4 times over a period of 10-11 days. Cases found this way were requested to get PCR confirmation. The partnership that developed this regarded it as very successful and planned to keep this in addition to operating a hub and spoke model.
Balance between MTU and ATS testing
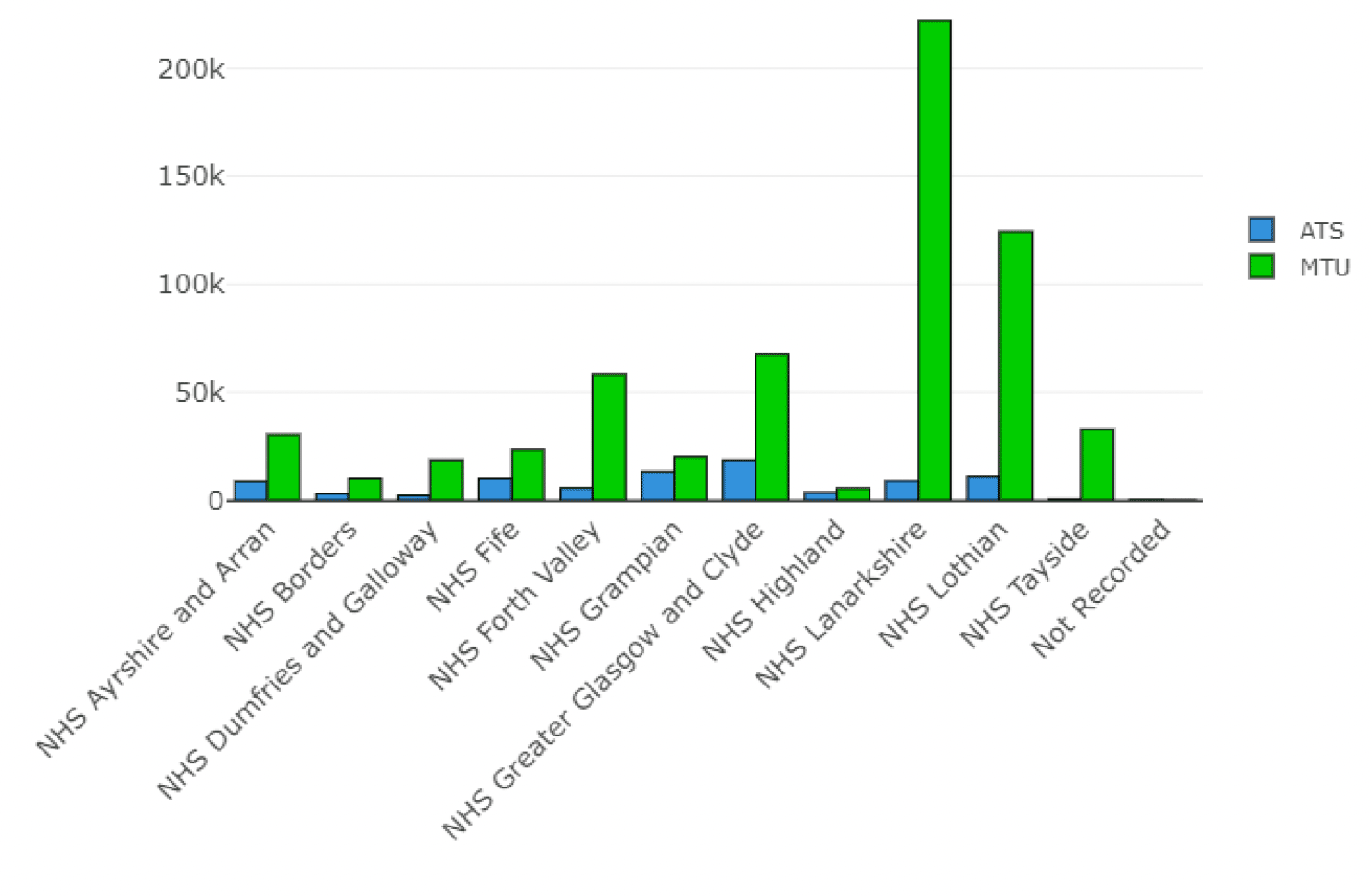
Overall MTU appears to have dominated TCT up to 26 September 2021. Cumulatively, testing via MTUs has seen a total of 613,280 tests (87.7% of total tests classed as via TCT) with 85,939 tests classed as through TCT ATSs (12.3%), also see Figure 6.
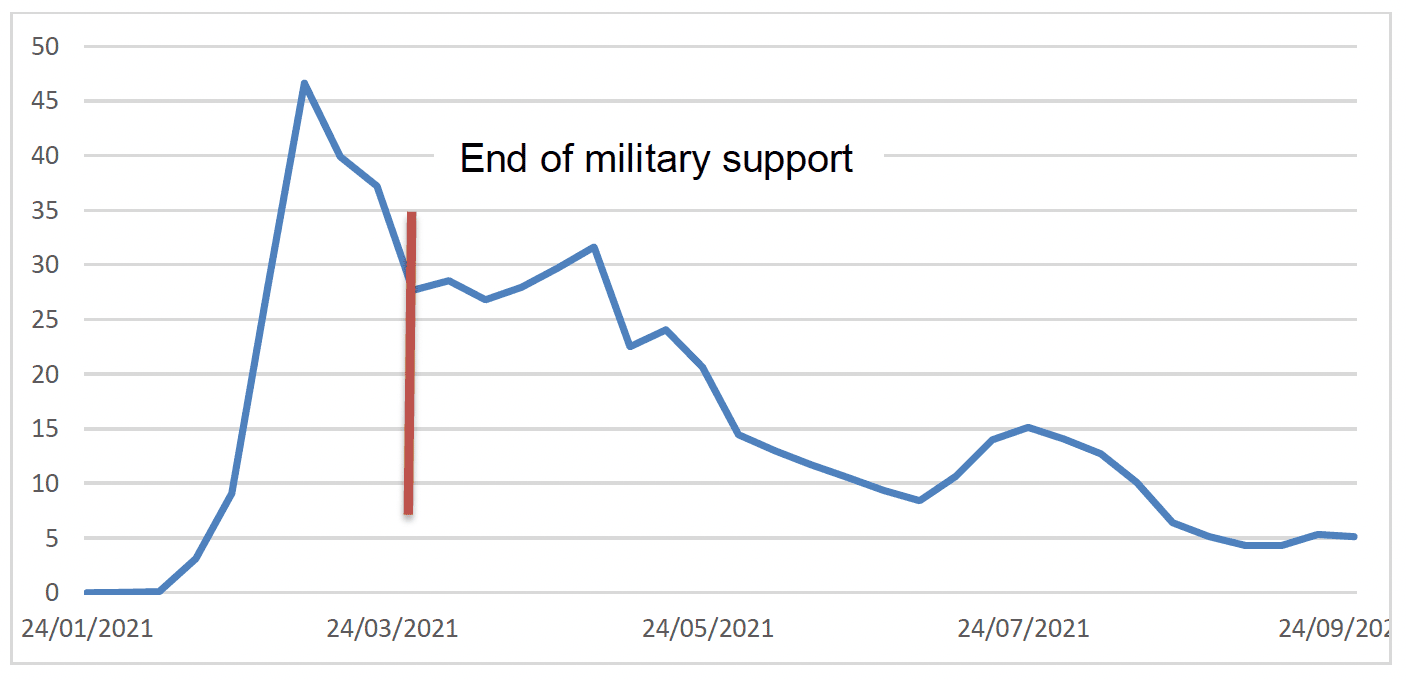
Week by week since early July, the proportion of LFT testing recorded as taking place via ATS has declined so that by 26 September, it was only around 5% of TCT testing taking place (Figure 7) and Annex C for data table. However, with the launch of the Universal Offer and Pharmacy Collect, the opportunity to obtain LFTs by the general public was no longer limited to TCT. TCT itself evolved to incorporate promotion and distribution of the Universal Offer kits as outlined in stage 4 of Figure 5 above. The data from the Universal Offer is not linked back to TCT, hence the true extent of TCT ATS is ultimately unknown. It is clear though that, through the TCT programme, significant capabilities have been developed to conduct locally targeted testing, both for LFT and PCR testing
Operational lessons and suggestions
The final section of this report summarises findings from both Proforma exercises around operational aspects of TCT. The reader is reminded that these cover the first few weeks and early months of implementation.
Setting up and running a site
- There was perceived to have been good collaboration with military colleagues in all areas, with military colleagues providing training and expertise that allowed ATSs to operate successfully. Some areas initially staffed ATS with only military colleagues and trained up local authority staff over time. This allowed for a quick and smooth set up of ATS due to military colleagues having previous setup experience.
- Initially some experienced issues with equipment while setting up ATS, some areas had to build their own booths because those that were delivered were of poor quality. Some areas also reported delays with PPE and testing kits.
- Staff working at the ATS have typically been seasonal workers, temporary employees or redeployed from other areas where the service was paused due to the pandemic (for example, leisure). A key issue for many was the return of these staff to their original duties as restrictions eased. One Health Board suggested targeted recruitment of skilled, long-term unemployed to involve in the TCT programme.
- In one area staff were given the option to train for different site roles, this was perceived to have helped with team building, variety for the staff and meant there was wide ranging competence of site staff.
- Communication was a key theme, and many aspects have been covered elsewhere. The one addition here, based on feedback on the May Proforma was more from an operational perspective highlighting challenges from having multiple sources of information – "There are so many data sets and guidance documents circulating/ being updated - this has made it difficult for everyone to understand the aim of the community testing programme, and has caused juxtapositions, confusion and delay."
Maintenance of TCT over time
A common concern in the March Proformas was the ability to maintain community testing over time for a number of reasons:
- Availability of sites as lockdown starts to ease and centres begin to open for other purposes. This concern was one of the driving forces behind development of mobile ATSs and the establishment of the Mobile Testing Working Group. One area described attempting to use non-Council venues but experienced longer lead-in times and planned to explore co-location with vaccination venues.
- Staffing and maintaining a service with many staff currently used being furloughed and redeployed staff who will return to other duties. One area described using bank staff and creating contingency plans with volunteer services.
- An opinion was expressed that dedicated staff are required rather than this being an add on to existing day jobs. One area carried out rapid recruitment of temporary staff from the local community due to constraints on using staff from elsewhere. The majority were on full-time temporary contracts, however, a risk was highlighted of attrition of such staff.
- The buy in of public going forward to continue to attend ATS centres.
- The cost-benefit balance if prevalence is low.
Test site user experience
- On Proformas, partnerships reported high satisfaction with their experience across areas from test site attendees (>90% for those areas reporting exit survey results).
- Improvement suggestions from the public included: improving the registration process on UK Gov website and a suggestion to enable creation of a profile to simplify getting tested repeatedly; more publicity about the sites, signage (directing people to the site and better/bigger signs at the test site) and parking.
- While most people said they found the test easy to do themselves, some areas reported higher numbers of people who struggled with tests and worried they might not have done the test right or were surprised they were not supervised during taking the test and thought they may had done this incorrectly.
General Practical Suggestions
- Have a paper backup system for when IT systems are down
- Consider a waiting room for those without a mobile phone to wait for results (or provide a phone and topup, as was implemented in one area)
- Display site code and guidance in queuing area to facilitate self-registration
- Make sure iPads & phones can connect to the internet
- If staff are working outside in the dark, they should have high-visibility vests and a radio and preferably work in pairs
- Check the communications are accurate, some areas reported issues with incorrect ATS opening times advertised on social media.
Models and Reach
- Co-locating an MTU with an ATS enables convenient and rapid access to confirmatory PCR. Experience was reported of confirmatory PCR not always being done when home tests kits are supplied or people are directed to other PCR sites
- It was suggested that sites should be able to offer the spectrum of testing choices to improve access, effectiveness and cost–effectiveness
- One Health Board reported that their rural communities have been difficult to target due to lack of suitable accommodation, the deployment of a full ATS squad for small population numbers and the time which is required to set up an ATS with little return.