Coronavirus (COVID-19) targeted community testing: national evaluation evidence and insights - final report
This report summarises evidence and insights at a national level from evaluation of targeted community testing (TCT). The report covers the period 18 January 2021 to 26 September 2021.
2. The Public Health Impact of Community Testing
Positive cases identified through Community Testing
Since its launch on 18 January and up until 26 September 2021, the TCT programme has detected a substantial number of positive COVID-19 cases – 93,466. Of these, almost a third (31%) were in those classed as without symptoms. These are cases that may not otherwise have been detected in the absence of symptoms, or were identified earlier than they otherwise would have been via PCR-based testing once symptomatic, see Table 1.
| Total tests | 699,219 |
|---|---|
| Total positive cases | 93,466 – of which 29,387 (31%) were in those without symptoms |
| Percent positive | 13.4% (combined symptomatic and asymptomatic) |
A small majority of tests conducted were in those without symptoms, with a sizeable proportion of symptomatic tests carried out within the TCT programme, see Figure 1.
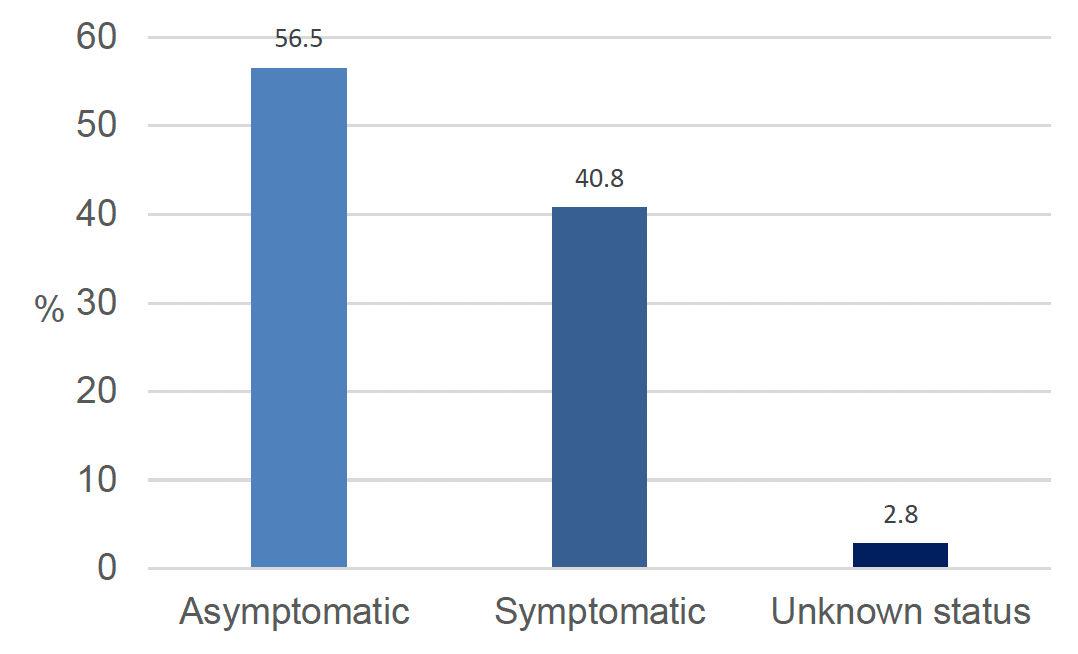
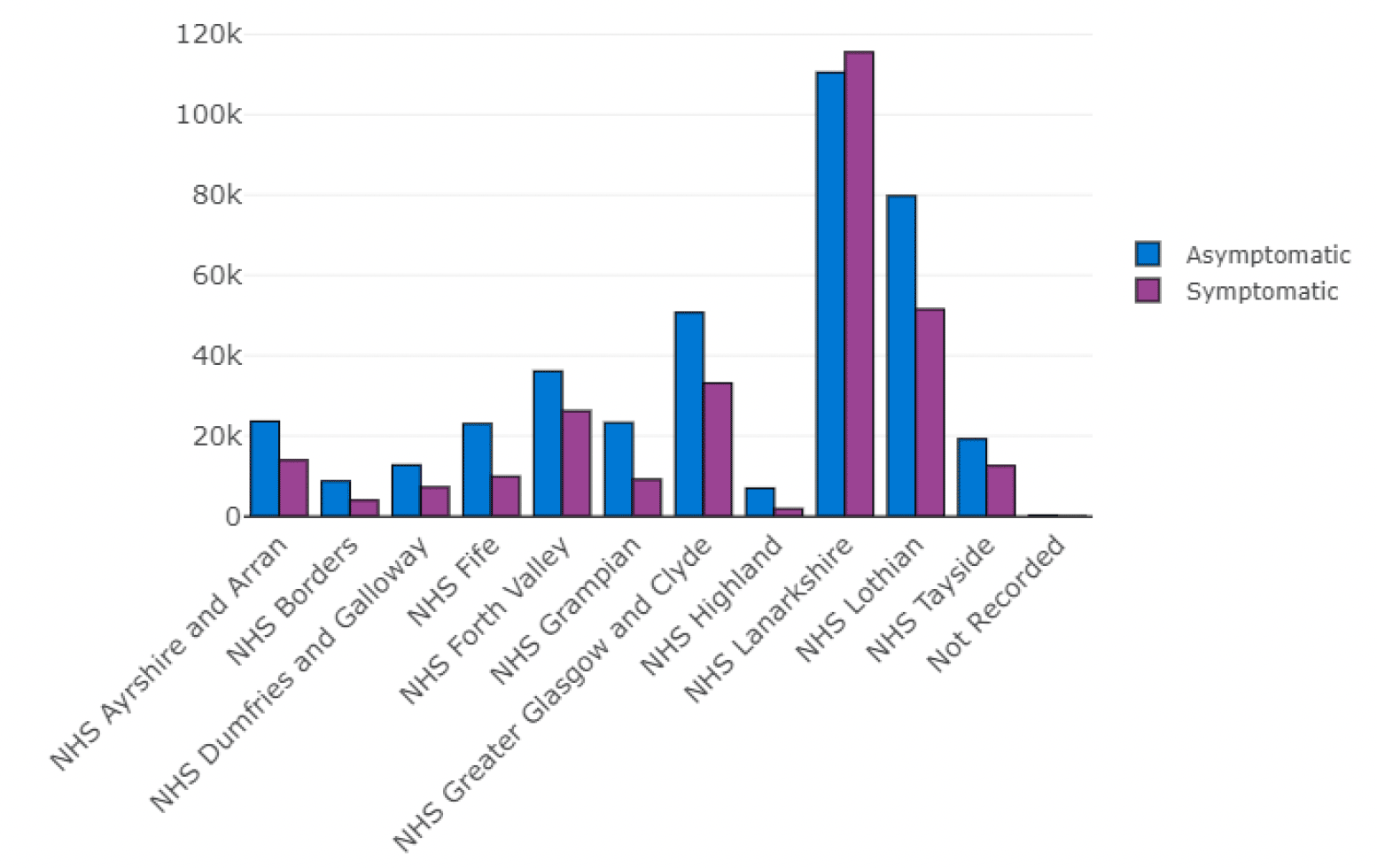
Figure 2 shows that asymptomatic testing was dominant to varying degrees in all partnership TCT programmes, with the exception of Lanarkshire.
Although symptomatic testing has been available via local and regional testing sites outwith the TCT programme, the sizeable proportion of symptomatic testing within the overall TCT programme is indicative of how the programme has likely broadened (as intended) access to testing for some communities that may have found accessing local and regional test sites challenging.
In addition, the data covers a period when several local partnerships were implementing surge testing. Although LFT testing contributed substantially, the surge testing was mainly focused on PCR testing for symptomatic and asymptomatic people, particularly when the new Delta variant was starting to increase in prevalence with the associated requirement to track the variant.
Uptake of testing and change over time
The trend for overall TCT testing uptake, as indicated by weekly number of TCT tests conducted, has generally tracked a similar pattern to testing across Scotland[8], reflective of the changing incidence of COVID-19 and relaxation of restrictions, see Figure 3.
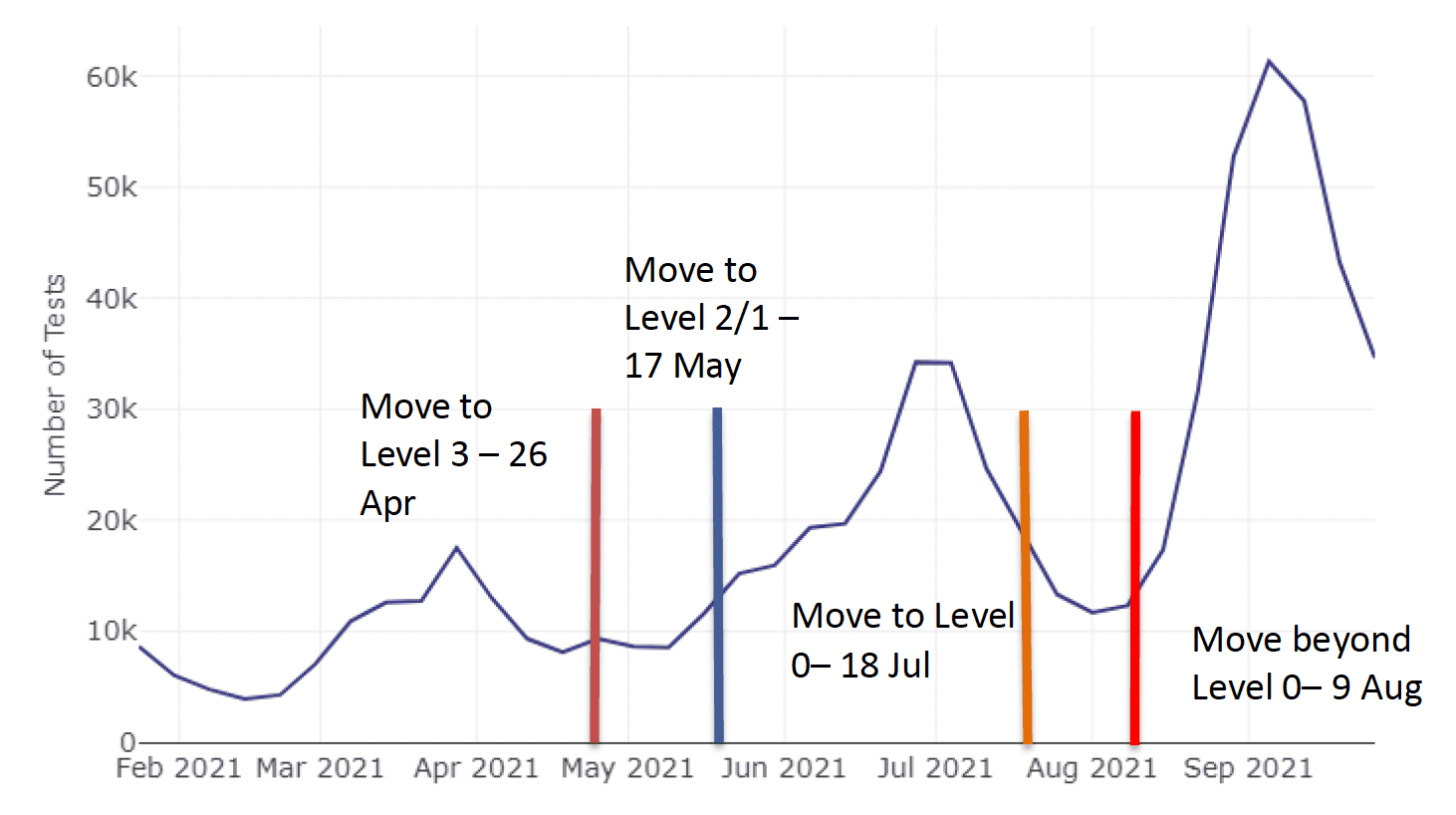
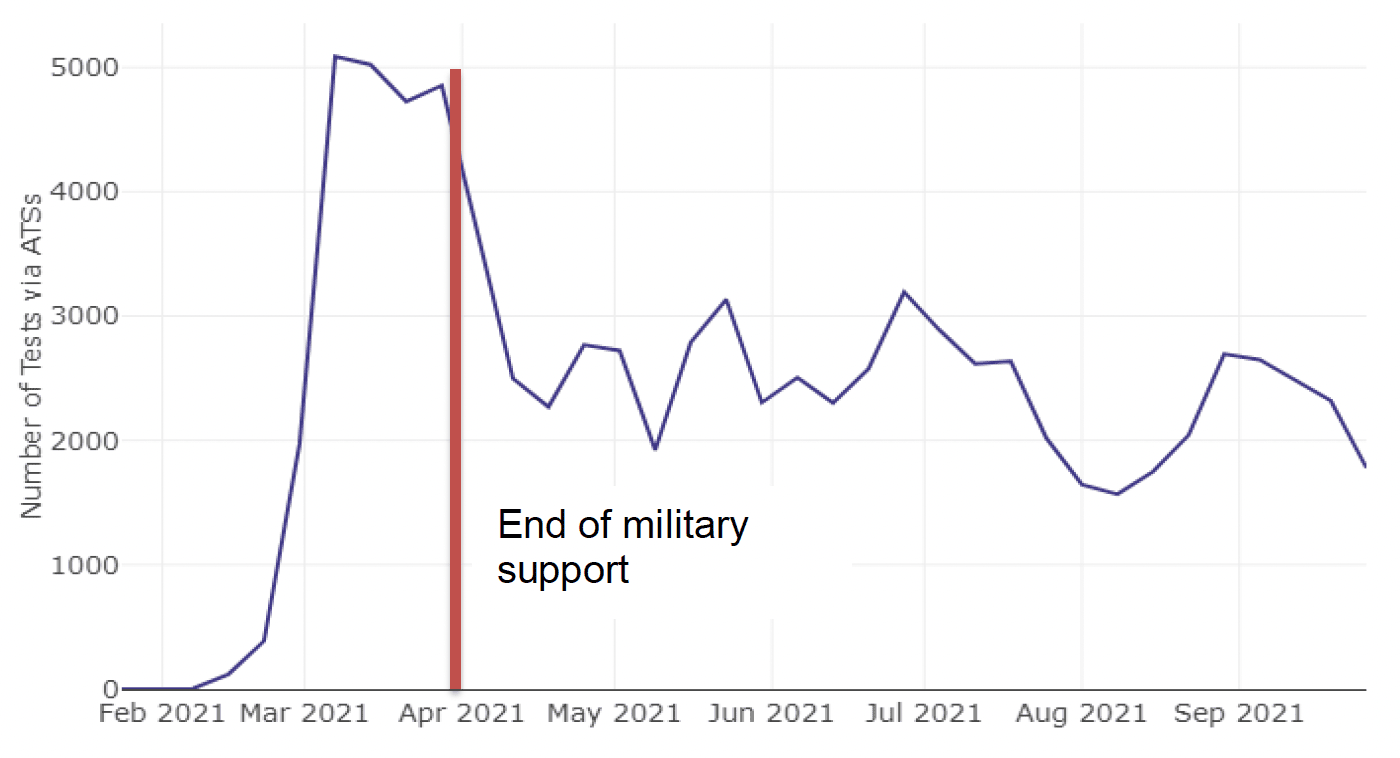
The one exception is the peak in early April for TCT testing which is not so evident for all Scotland testing. A possible explanation for this is an initial push to get the community asymptomatic test sites (ATS) operational, supported by military assistance. Figure 4 shows how the weekly number of targeted community tests that were conducted via ATS (ie LFT testing) grew sharply, peaking at just over 5000 by 7th March. There was a sharp decline after the end of March coinciding with the cessation of military support, and tests then became universally available from 26th April through the Universal Offer.
Qualitative evidence from both Proforma returns, and a common theme at times during Reference Group discussions, indicated a sense from local partnerships that footfall through ATSs was overall lower than expected. The overall capacity of the sites in the early stages was felt to be much under-utilised despite substantial communications and engagement efforts. This was even the case for partnerships who regarded their TCT programmes as successful. In part, this may be a reflection of the stage of the pandemic at that time with cases declining.
From Proformas, a wide range of communication methods were described to encourage attendance at TCT sites: social media, radio campaigns, leaflets, posters, message boards at transport links, letter drops, targeted communication with community and faith leaders and local businesses and schools local to test sites. This also included translations of some of these resources in several languages in some areas.
One partnership planned to employ a community links worker to develop grassroots connections, another had developed a group of COVID-19 Empowerment Champions to reach non-engaged communities. Another area was working with 'community influencers', community leaders and groups, whilst another was using local 'celebrities' and 'well kent'[9] faces to publicise the test centre. There was also reported use of Council Environmental Health, Education, Communications teams and the voluntary sector.
Feedback reported in Proformas indicated social media, word of mouth, letters to households and AA route signage have been particularly effective, demonstrated via responses to test site Exit Interviews, or from increased attendance at sites after certain communications activity. More on targeting, communications and engagement is presented below.
Targeted testing – effective case finding
One of the intentions behind community testing has been for testing capabilities to be targeted, particularly to areas with persistent high cases or where the cases are spiking, through use of data and local intelligence. In theory this should be more effective at finding positive asymptomatic cases than untargeted or general population testing. In addition, there is assistance at community test sites to support taking the test correctly and to ensure the results are recorded.
PHS publishes data on the number of LFT tests, number of positive results and test positivity for a wide range of the pathways using LFT testing, including for the LFTs carried out through TCT[10]. This allows a degree of comparison between the different pathways to indicate how effective they are at identifying positive asymptomatic cases. However, some caution is advised in interpreting this data as the different pathways are not directly comparable. In some pathways tests are administered, whilst in others they are self-test which could affect the sensitivity of the test. Also, not all pathways will have similar reporting of positive and negative results, with lower likelihood of recording negative results (negative recording bias) for self-test which will tend to inflate the percent LFT positive. Finally, LFT is a small part of the testing conducted via TCT. A large number of asymptomatic tests are carried out using PCR so this comparison is only of part of the TCT programme.
Between 19 November 2020 and 21 September 2021[11], a total of 85,837 LFT tests were conducted via TCT sites. Cumulatively, a total of 780 positive cases were identified with a percent LFT positive rate of 0.9%. For comparison to LFT tests via all pathways see Table 2.
| Total no. of LFT tests | 11,555,190 |
|---|---|
| Total no. positive | 71,192 |
| Total percent positive | 0.6% |
Challenges with the data notwithstanding, TCT had a percent LFT positive of 0.9% up to 21 September 2021 and was one of the highest of the LFT pathways and above the 0.6% for all pathways combined, suggesting tentatively that the targeted approach has been effective.
This is also likely to be an underestimate of the contribution of TCT because ATS and MTU sites have promoted the use of the Universal Offer and Pharmacy Collect and distributed Universal Offer packs as part of the TCT programme. The data are not linked back to TCT, but instead recorded as Universal Offer. Thus TCT efforts will also be reflected in the data for the Universal Offer, which had the highest percent LFT positive at 2.6%.
Targeted testing – reaching the right groups
Another feature of targeting is to reach groups that may be more challenging to engage with testing. For example, Liverpool and Welsh pilots of mass testing indicated that younger people, men and those from more deprived area were less likely to get tested[12]. Scottish Government commissioned polling, which included questions around general testing attitudes and behaviours. This also indicated men and lower occupation grades reported being less likely to have a test, order or use Universal Test kits[13]. Funding was provided as part of the programme to improve understanding of local communities to improve reach.
A robust assessment of reach to different groups has not been possible for a variety of reasons, including that many TCT sites are typically transient and it is difficult to describe a precise population that is being targeted in each area. This is in part due to multiple other pathways in operation to which many in a geographical area will have access. Some of the models of the TCT programme also included promotion and drop off of Universal Offer LFT kits where the data is not linked back to TCT.
There is greater understanding with respect to age, gender and level of deprivation (as indicated by SIMD) because this data is requested when recording a test result (although not always completed). However, there is no good quality data on other population characteristics and a wide variety of population groups have been identified as at risk or likely to be less engaged with testing eg migrant populations; those whose first language is not English; ethnic minority groups; gypsy and other traveller groups.
Although there is no robust evidence around effectiveness of reach for this report, qualitative data collected from partnerships via the Proformas enable reporting on their experiences and perceptions around efforts to engage with a range of population groups.
Targeted testing – features of success, challenges and suggestions for improvement
In the May 2021 Proforma, local partnerships were asked their views on features that supported and challenged targeted testing and suggestions for how to improve targeting. Presented below is a summary of key messages which includes supplementary evidence from March Proformas.
Overall, partnerships reported data driven location of sites and communications and engagement as key elements of success for targeted testing, as well as flexible and responsive models of operation.
Key challenges mirrored aspects of success and included issues around communications and engagement, and lack of flexible testing models. The issue of multiple testing pathways was also raised, mainly in relation to adding to confusion.
Communications and engagement key messages (see also earlier entry)
Communications need to be clear, locally relevant, wide-ranging with engagement through multiple channels; Also, constant and dynamic. One partnership response encapsulated this by stating:
"Good communication via a range of media channels with clear messaging about the local context and reasons for getting tested, as well clear instructions on how to access and book for both symptomatic and asymptomatic testing."
Social media appears as consistently one of the main sources for public awareness - based mainly on exit surveys of attendees, but also social media analytics and site staff feedback. However, it is worth highlighting that this should be interpreted as the main sources of information for those engaging or attending. This may not be the same as for those not attending.
Communication was highlighted as a key to success, but also one of the main challenges to success if it was not done well. Some issues with communication highlighted within Proforma returns include:
- Conflicting messaging of national 'stay at home' advice versus local 'come and get tested'
- Inaccurate and non-user friendly Government websites
- Challenges around engaging the disengaged and understanding who they are
- Confusion for the public (and professionals) on understanding the multiple pathways available for testing, where and when you can or should get a test; also changing expectations around what should happen at a TCT site as a result of the introduction of the Universal Offer and expectation to just be able to walk away with a kit rather than test there and then. There was some concern that confusion impacted on footfall.
- Tackling misinformation, such as on social media
Suggestions for improvement
- Increased local and targeted communications and use of more communication channels (eg outdoor advertising; advertise community drop off at high rise flats where residents may have mobility problems, and at social housing)
- Engagement - build stakeholder relationships, wider community outreach and use of outreach teams
- Scottish Government website to take a triage approach with users answering a series of Y/N questions to reach correct site information
- National campaigns about the benefits of testing
- Promotion of testing at the point of vaccination
- Conduct seasonal campaigns (eg at Halloween and Christmas)
- Create videos for social media to target specific groups (several have already done this with reported success)
Use of data and local intelligence key messages
A wide range of data and local intelligence has been, and continues to be, used to effectively target key areas of concern through regular intelligence discussions and reviews in the local partnerships.
The range of data used varies between areas but can include:
- Public health monitoring data such as total number and trends for cases and positivity rates
- Public demand/footfall – eg tests per day per site
- Cases per site
- Indicators of 'community vulnerability' or 'community of interest' assessment
- Availability of centres to site testing
- Wastewater virus analysis
- Car access and rurality considerations
- Contact management system (CMS) to locate and support a local outbreak
- Scorecard ratings that combine testing rate and incidence with social/clinical and demographic vulnerability (highest rating of 5 indicating lowest comparative rates of testing and highest incidence signalling an issue)
- Colorado social distancing index to identify at risk communities
Important aspects to note around the use of data, that came through from Proformas, are:
- Local intelligence is key and data alone is insufficient, the data needs to be placed in context
- Sites can't always be located according to data due to the lack of an available site
- Setting up of local monitoring systems has helped mitigate shortfalls in UKGov data
Local knowledge came through as key to placing any of the data in context to deploy test sites appropriately. For example knowing that a rapid rise in cases is associated with either a school or care home. This knowledge is important to understand if an observed spike is a real issue or not and understanding that they have other routes for testing. In some geographical areas testing uptake may appear low but this is due to many people living in this geographical area having access to testing through workplace programmes such as NHS or Education
Testing systems were established to track tests taken and results specific to TCT. However, in some areas the set-up of local monitoring systems was felt to have helped mitigate shortfalls in the UKGov testing data and the availability of this data. This approach was only possible in areas where the analytical resource to support this was available.
Wastewater testing
Wastewater testing involves collecting samples of wastewater at various locations and analysing them to detect levels of COVID-19 RNA. This can give an indication of the level of virus circulating in the population of the area served by the wastewater sampling site[14]. Early on in the TCT programme, views from local partnerships using it were that it was a useful adjunct to other public health monitoring data, primarily to confirm suspicions. It has also shown value in early warning of an area of concern when public health data had not yet shown any issues. Some pros and cons expressed by partnerships are set out in Table 3.
Table 3: Wastewater pros and cons based on partnership feedback March 2021
Pros: confirms suspicions based on positivity results
Cons: variability in results
Pros: insight independent of testing strategy
Cons: infrequency of sampling
Pros: may be useful as warning signal when case numbers/testing low
Cons: timing of availability - results lag or run in parallel to positivity results,
geographies for testing do not match those required,
uncertain value in addition to standard surveillance methods (cases)
Pros: Partnership example - confirmed case rates were not high and testing uptake was average. "Alerted by SEPA to levels being amongst the highest they had ever seen. Two MTUs deployed and, for both, people came forward for testing and cases were found."
Cons: Partnership comment - "Local data so far doesn't suggest that WW RNA levels have risen before a signal is seen in case numbers"
Approaches to testing
Pros and cons were raised around both mobile and fixed models of operation.
Observations were made that fixed sites could have significant lead in times to set up and start operations, and may also end up located where they are not necessarily most required due to availability of suitable sites. Mobile testing was seen to address many of these drawbacks by being more responsive and flexible.
However, there were recognised challenges for the mobile model as well in terms of effective and timely communications to the public; the transient nature for anyone wishing to access them repeatedly; and the challenge of rapid identification of suitable sites.
Suggestions to improve targeting and uptake
- Offer testing at community based events (could help reach young males)
- Target holiday spots
- Work with local businesses/employers to encourage staff testing (where not already available)
- Dual testing capability (PCR and LFT) in all types of mobile units to enable flexibility of what can be offered at sites
- Explore co-location with vaccination centres
- Offer incentives to get tested (eg local business vouchers)